Embed Size (px)
Citation preview

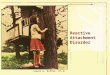
Understanding Attachment

THE ATTACHMENT BEHAVIORAL SYSTEM
IS THE
ATTACHMENT
FIGURE
SUFFICIENTLY
NEAR,
RESPONSIVE,
ATTUNED
YES
NO
ATTACHMENT
BEHAVIORS: VISUAL
CHECKING, SIGNALING
NEED FOR CONTACT,
PLEADING, CLINGING
FEAR,
ANXIETY
DEFENSIVE
FELT SECURITY,
LOVE, SELF-
CONFIDENCE
PLAYFUL,
SMILING,
EXPLORATORY,
SOCIABLE
AVOIDANCE,
WATCHFULNESS
WARY
AMBIVALENCE,
CLINGING,
ANGER

Secure Base
Self-Confidence/Exploration
Perceived Threat
Felt security
Attachment System
Signaling
Proximity Seeking
Safe Haven
Caregiver’s
Signal detection

Secure Base
Perceived Threat
Felt security
Attachment System
Signaling
Safe Haven
Caregiver’s
Signal detection
Sense of Self
Sense of Other
B
a
l
a
n
c
i
n
g


Attachment Styles and Parent
Responsiveness
Inconsistent/Role
reversal
Responsive/Attuned
Avoidant
Ambivalent
Disorganized
Secure
Frightening/
Threatening/
Dissociated
Rejecting/disengaged/
overly Intrusive
Parent Responses Themes Attachment Style

Reactive Attachment Disorder

What is RAD
• Understanding Changes from DSMIV to DSM5 – Elimination of a class of disorders know as “Disorders
That Usually Begin in Infancy and Early Childhood,” included dxs such as: • ADHD
• ODD
• CD
• Separation Anxiety Disorder (SAD)
• Autism
• Reactive Attachment Disorder
• Others

• Redistributed them into other classes (some are whole new classes) – E.g.
– ADHD and Autism Neurodevelopmental (New Class)
– ODD and CD Disruptive, Impulsive, and Conduct Disorder (New Class)
– Separation Anxiety Disorders
– RAD Trauma-Stressor-Related Disorders (New Class)

Trauma-and Stressor-Related Disorders
• A spectrum of disorders in which exposure to a traumatic stressor and or other stressful events is a core feature of the disorder
• These disorders within a developmental framework, beginning with attachment related disorders

Trauma-and Stressor-Related Disorders
• Attachment Related Disorders— – Previously one disorder (reactive attachment
disorder) with two subtypes: (1) emotionally withdrawn/inhibited and (2) indiscriminately social/disinhibited
– Now two distinct disorders • Reactive Attachment Disorder (internalizing) • Disinhibited Social Engagement Disorder (externalizing)
– Rationale is that they represent two different spectrums of responses, internalizing vs externalizing, and they have very different long term outcomes and responses to treatment (reactive > disinhibited)

Diagnostic Tips
• Neglect typically begins early (first two years of life) and often before disorder symptoms are manifested
• Still uncertainty about how this disorder manifest in older children
• Comorbidities are common
• Be cautious when making the diagnosis in children older than five

Important Differential Diagnosis
• Autism Spectrum
– Much lower likelihood of neglect
– Presence of restricted range of interest and ritualized behavior/rigid routines, fixated interests, unusual sensory reactions/profiles
• Both can engage in rocking and flapping motor behaivors
– More specific deficit in social communication (e.g., poor goal-directed, intentional social communication)
– Still maintain selective attachments and attachment behavior

Reactive Attachment Disorder
• Inhibited, socially withdrawn behavior toward adult caregiver
• Persistent social and emotional dysregulation
• Experience patterns of extreme insufficient care

Disinhibited Social Engagement Disorder
• Lack of anxiety or reticence with unfamiliar adults
• Not accounted for by the impulsivity due to ADHD
• Criterion C is the same as for reactive attachment disorder

Disinhibited Social Engagement Disorder
• Comorbidities are frequent, ranging from cognitive and language delays.
• Although it may be distinguished from ADHD, it may also be comorbid with ADHD.

Posttraumatic Stress Disorder
• Expansion of criterion A with more specificity regarding the events that qualify as traumatic Criterion A now allows:
– Learning about the traumatic event of family member) or close friend
– Exposure to aversive details about the traumatic event
• Dropping A2 (intense fear reaction to exposure)

Posttraumatic Stress Disorder
• Expansion from 3 to 4 symptom clusters – DSM-IV avoidant/numbing cluster is divided into two
distinct clusters: • Avoidance—thoughts and memories as well as people places
and events
• Persistent negative alterations in cognition and mood – Memory disturbances regarding event
– Loss of interest
– Negative beliefs or expectations about oneself world and others (shattered assumptions)
– Cognitive distortions about causes and consequences of traumatic event
– Includes negative emotional states

Posttraumatic Stress Disorder
• Arousal and reactivity cluster now includes expression of verbal or physical aggression towards other people and reckless or self-destructive behavior
• Includes specifiers regarding presence of dissociative symptoms and delayed expression of symptoms
• For children 6 and under, separate criteria with lowered threshholds

Useful Instruments for Assessing Attachment and Related Problems

Disturbance of Attachment Interview

Evidenced Based Treatments

Relationship Components—case formulation model
A C
Relationship Specific
Cognitions
interactions
Relationship Specific
Cognitions
IWM of Attachment and Caregiving Based onHx of attachment experiences
IWM of Attachment and Caregiving Based onHx of attachment experiences

Common Features
• Sameroff’s 3 Rs
– Redefine, re-educate, remediate
• Working with Parent
• Working with Child
• Creating safety
• Working with parent-child interactions
• Working with systems: school, teachers, community resources

Evidenced Based Treatments

Evidenced-Based Treatments
• Infancy and Early Childhood
– Attachment and Bio-behavioral Catch-up
• Dozier, Lindhiem, & Ackerman (2005)
– Setting: Home (foster, adoptive, biological)
– Targets: Child dysregulation, Caregiver nurturance, Caregiving parenting


• Ages 1-4 • Targets: child
caregiver interactions, child behavior, parenting stress
• Setting: outpatient

Evidenced Based Treatments
• Ages: 2-21 • Targets: complex
trauma; behavior problems
• Outpatient, home residential

• Targets: Child PTSD, Child Behavior, Secure Attachment, parent PTSD
• Setting: Home, Community Settings

Treatments to Avoid
• Treatments involving: enforced holding and physical constraints, physical domination, provoked catharsis, ventilation of rage, age regression, humiliation, exaggerated control
• However, this does not exclude common behavioral management strategies: time out, rewards, contingency management, grounding, and restraint for safety purposes
• Avoid predictions of psychopathy and other misconceptions • Avoid treatment that portray these children as pervasively
manipulative, deceitful, and without conscience as these views tend to perpetuate negative parent child interactions