Embed Size (px)
Citation preview

Realities in the fieldRealities in the field

FEVER
Differential Diagnosis
not possible
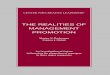
What happens in practice when a child presents with fever
Where malaria risk is high
Fever or history of fever?
Treated with antimalarial
Child survives
Classified as malaria
Artemisinin based Combination Therapy (ACT)
is recommended by WHO

What happens/could happen when a child presents with danger signs
DANGER SIGNS
Basic treatment started with
Artesunate suppository
Signs of a child requiring urgent
attention
Typical case:TC5022-2 – mother's description .. fever 3 days prior to death. at home for 2 days without treatment.
third day of illness, the fever intensified, and the child became very weak. Did not go to hospital. Day3 child had laboured breathing and died.
Lethargy?- baby conscious but not responding to sounds or movementUnable to feed? why – too weak, shortness of breath, disturbed consciousness, inability to swallow
Is child vomiting everything? Sign of an illness to be identified, child can become dehydratedDoes child have convulsions with illness? – Febrile seizures? But meningitis, malaria, pneumonia cannot be ruled out
If unable to eat, drink or suckUnable to sit, stand or walk unaided
Lethargy/ altered consciousnessRepeated convulsions
Repeated vomiting
REFERRED to
HOSPITAL
Classified as severe malariaWith added symptoms of chest in-drawing
+ rapid breathing classified as malaria +pneumonia

Because it was late at night, they did not go to hospital. The fever intensified and the child started having
difficulty breathing (deep breathing) .. Child dies on the 3rd day of illness at home
On return to per os status, child given oral
antimalarial
Child survives
Did not go to hospital. But the child improved and
could eat and play
NOT KNOWNWhat proportion of children treated early with
rectal artesunate are at risk of death without hospital intervention?
NOT KNOWNWhat proportion of children treated early might
safely be given a suppository plus oral ACT treatment
HIGH risk of death
Child does not respond
Child responds
What happens/could happen when a child presents with danger signs
Referral advice not
followed
REFERRED to
HOSPITAL

NOT KNOWNProportion of children treated with rectal artesunate
are at risk of death without hospital intervention?
NOT KNOWNWhat proportion of children treated early might
safely be given a suppository plus oral ACT treatment and not need hospitalisation
Should rectal artesunate be made availableOnly with ACTs?
RISK- BENEFIT
INFORMATION NEEDEDHow to really scale up rectal artesunate + ACTs?
What packagingHealth Information/Education
Pricing Supply Logisticswill be necessary
To make the intervention work at national level?
INFORMATION NEEDEDProportion of children treated with rectal artesunate
that need hospital management because they(i)Progress to severe malaria
(ii) Have anaemia, dehydration, malnutrition (iii) Have pneumonia co-infection or just pneumonia
Chest Indrawing
Strange Sounds
Fast Breathing
SOLUTION UNICEF main implementing Agency
for Child Survival(i) Make part of UNICEF – community based IMCI
(ii) Target countries & GFATM(iii) Produce product, package with ACTs(iv) Introduce Health Education, Deploy(v) Develop mechanisms for scale up

Community Integrated Management of Community Integrated Management of Childhood Illness, C-IMCIChildhood Illness, C-IMCI
C-IMCI = an integrated child care approach to improve key family and community practices likely to have greatest impact on child survival, growth and development
Practices include: breastfeeding and complementary feeding, hygiene and helping to prevent malaria - consistent use of treated nets, home management of fever episodes, and through recognizing symptoms and promptly referring severe fever cases to a health facility.
UNICEF advocates with governments to improve health systems, including ensuring that essential drugs, supplies and equipment are available.
UNICEF helps to buy and distribute these items, including vaccinations for routine immunization, Vitamin A supplements, insecticide-treated nets in malaria-affected areas, and malaria home management kits (pre-packaged anti-malarial medications).

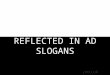
Countries with child health
related community
interventions
IMCI Unit AFRO
Countries with Community-IMCI in more than 3 Districts
Community IMCI : Implementation Status

IMCI Unit AFRO
COUNTRIES WITH PLAN FOR C-IMCI
•Planning at national and district levels
•Partners collaborating in planning

SummarySummary
Children who obtain rectal artesunate by reason of their acute disease are likely to benefit
However, in providing the drug, we need to discourage complacency that the drug will solve all problems
The probability is high that most (>75%) children will return to per os status
For these children –co-packaging with oral ACTs makes sense; hospitalisation may not be necessary
But, there is a small, critical, risk that some children will not respond because they have same symptoms but another infection
Need to identify the non-responders quickly