Embed Size (px)
Citation preview

RECCURENT MEDULLOBLASTOMA:ROLE OF DIFFUSION WEIGHTED
IMAGING
Dr. Rakhee Gawande M.D and Dr. David Nascene M.D
Department of Radiology
Control# 1638Poster# EP 130

DISCLOSURES
• NONE

INTRODUCTION• Medulloblastoma is the most common malignant
CNS tumor of childhood
• Comprise 15-20% of CNS tumors of children
• 35-40% recurrence rate
• Surveillance imaging important for early detection,
prompt intervention and good outcome
• MRI of the brain and spine remain primary modality
for diagnosis of recurrence
• Since relapse is typically intra-cranial, surveillance
spine MRI has low yield

SURVEILLANCE IMAGING• The reported rate of asymptomatic relapse is 19-
46%
• Multiple studies have shown that surveillance
imaging detected minority of recurrences with no
survival advantage
• Survival advantage limited due to our inability to
successfully treat recurrence.
• Current treatment regimen per the COG Phase II
screening trial (ACNS0821) include combination of
temozolomide, irinotecan, and bevacizumab

SURVEILLANCE IMAGING
• In the ACNS0821, recurrence is defined as tumor
measurable in two perpendicular dimensions on
MRI and histologic verification of malignancy at
original diagnosis, but not necessarily at the time of
recurrence.
• Recurrent disease should be differentiated from
treatment-related changes like radiation necrosis or
pseudoprogression

SITES OF RECCURENT DISEASE• Relapse more common in young children• Isolated local recurrence rare; usually
associated with meningeal dissemination• Local recurrence not associated with
incomplete resection• Risk for local recurrence influenced by
patient age and not by amount of residual tumor
• Frontobasal region predominant site for supratentorial meningeal recurrence

PURPOSE
To compare the rate of detection of recurrent
disease on diffusion weighted imaging (DWI)
with contrast enhanced imaging (CE-MRI)

MATERIAL AND METHODS
• Retrospective review of MRI of patients with
medulloblastoma
• Recurrence defined as an area of hyperintense
signal on DWI with iso-hypointense signal on ADC
(Apparent diffusion coefficient)
• And area of nodular enhancement on CE-MRI

RESULTS• Database search from 2003 to 2013 revealed 45 patients
with medulloblastoma
• 12 patients (26%) suspected to have recurrent disease
• Mean age of patients at recurrence 17.1+/-14.4 yrs (range 4
to 47, median 11 yrs)
• Male: Female 8:4
• Mean time interval from diagnosis to recurrence is 36.3 +/-
32.5 months (range 6 to 113 months)
• Site of recurrence:
Cerebellum:7
Subependymal: 5
Basal cistern:1

RESULTS
COMPARISON OF DWI WITH CE-MRI:
• 9/12 patients with confirmed recurrence had
restricted diffusion signal (100%)
• Only 5/12 patients had contrast enhancement (55%)
• 2/12 patients with radiation necrosis had positive
contrast enhancement and no restricted diffusion
signal
SENSITIVITY SPECIFICITY PPV NPV
DWI 100% 75% 90% 100%
CE MRI 55.56% 33.33% 71.43% 20%

3 monthFollow up
DWI ADC Post gad
38 yr old male with local recurrence 30 months after therapy along the inferomedial right cerebellum. Note restricted diffusion signal on an initial scan without associated enhancement. A close interval follow-up showed enhancement in this region consistent with biopsy proven recurrence
LOCAL RECURRENCE

DWI ADC Post gad
8 yr old male with local recurrence in the right cerebellum seen as an area of restricted diffusion signal with associated enhancement. Note persistent disease on follow up scans
6 mthFollowup
LOCAL RECURRENCE

SUBEPENDYMAL RECURRENCE
13 yr old female with subependymal recurrence 74 months after therapy. Note enhancing nodular lesion in the midline along the septum pellucidum with restricted diffusion signal
DWI ADC Post gad

SUBEPENDYMAL RECCURENCE
DWI ADC Post gad
9 yr old female with subependymal recurrence in the frontal horn of both lateral ventricles, 34 months after therapy. Note absence of contrast enhancement with clear detection of lesion on DWI
SUBEPENDYMAL RECCURENCE
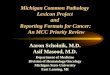
DWI Post gad
5 yr old male with subependymal recurrence seen 16 months after therapy. Note that the lesion is easily identified on DWI due to restricted diffusion signal. Lesion is not clearly apparent on post contrast images.

SUBEPENDYMAL RECCURENCE
DWI ADC Post gad
10 yr old male with subependymal recurrence 56 months after therapy. The lesion is easily identified in the anterior body of the left lateral ventricle on DWI and shows progressive increase in size and restricted diffusion signal over 1 yr period. Note lack of contrast enhancement and difficulty in detection on the post-contrast images. Lesion was missed on several scans performed at an outside facility.

RADIATION NECROSIS
6 MONTHFOLLOW UP
4 yr old female with patchy enhancement in the right cerebellum 9 months following treatment. Note absence of DWI signal abnormality. Follow up imaging showed resolution of enhancement without treatment, consistent with radiation necrosis
DWI ADC Post gad

CONCLUSION
• Restricted diffusion signal is commonly seen in
patients with recurrent medulloblastoma
• It can aid in the early detection of these lesions with
favorable outcome.
• Hence DWI images should be carefully scrutinized
in all patients and suspicious areas carefully
followed.
REFERENCES1. Surveillance imaging in children with malignant CNS tumors: low yield of spine MRI. Perreault S, Lober RM, Carret AS, Zhang G, Hershon L, Décarie JC, Vogel H, Yeom KW, Fisher PG, Partap S. J Neurooncol. 2014 Feb;116(3):617-23
2. Misdiagnosing recurrent medulloblastoma: the danger of examination and imaging without histological confirmation. Weintraub L, Miller T, Friedman I, Abbott R, Levy AS. J Neurosurg Pediatr. 2014 Jan;13(1):33-7.
3. Isolated sensorineural hearing loss as initial presentation of recurrent medulloblastoma: neuroimaging and audiologic correlates. Amene CS, Yeh-Nayre LA, Crawford JR. Clin Neuroradiol. 2013 Dec;23(4):301-3.
4. Recurrence in childhood medulloblastoma. Warmuth-Metz M, Blashofer S, von Bueren AO, von Hoff K, Bison B, Pohl F, Kortmann RD, Pietsch T, Rutkowski S. J Neurooncol. 2011 Jul;103(3):705-11.
5. Cranial magnetic resonance imaging findings of leptomeningeal contrast enhancement after pediatric posterior fossa tumor resection and its significance. Loree J, Mehta V, Bhargava R. J Neurosurg Pediatr. 2010 Jul;6(1):87-91.
6. Diffusion-weighted magnetic resonance imaging of treatment-associated changes in recurrent and residual medulloblastoma: preliminary observations in three children. Schubert MI, Wilke M, Müller-Weihrich S, Auer DP. Acta Radiol. 2006 Dec;47(10):1100-4.