Embed Size (px)
Citation preview

Recent Advances in Diabetes
2017
Enrico Cagliero, MD
MGH Diabetes Center
Harvard Medical School

Conflict of Interest Disclosure
Enrico Cagliero, MD
has no significant relationships with industry to report

Recent Advances in Diabetes
Rationale
Current guidelines
Cases
Therapies
CVD reduction

Goals of Treatment
Avoid acute complications of diabetes
Prevent micro and macrovascular
complications
Minimize hypoglycemia
Minimize weight gain
Increase quality of life
Individualize A1c goals !

Type 2 diabetes is a progressive disease Secondary Failure of Metformin Monotherapy
Diabetes Care 2010; 33:501-506

Standards of Medical Care in
Diabetes - 2017
Pharmacologic Approaches to
Glycemic Management
Diabetes Care 2017;40 (Suppl. 1):S64-S74

Antihyperglycemic therapy in type 2 diabetes: general recommendations
Diabetes Care 2017;40 (supplement1):S64-S74

Diabetes Care 2017;40 (supplement1):S64-S74
Combination injectable therapy for type 2 diabetes

Start with monotherapy with Metformin unless A1c > 9% (consider starting with dual therapy), or A1c > 10% (consider injectable therapy)
If monotherapy not effective after 3 months, proceed to dual therapy
If dual therapy not effective after 3 months, proceed to triple therapy
If triple therapy not effective after 3 months, proceed to basal insulin or GLP-1 analogs
Summary

How to choose among the new
therapies?

Why do we need more oral agents and not start
insulin therapy sooner?
Insulin associated with more hypoglycemia
Weight gain
Insulin still “refused” by many patients
Worse adherence to insulin injections
Some agents seem to provide CVD protection in
patient with pre-existing CVD disease

Novel Therapies for Type 2 Diabetes
GLP-1 Agonists
DPP-IV Inhibitors
Bile acid sequestrant
Bromocriptine
Sodium Glucose Co-Transporter 2 Inhibitors

Case 1
56 year old patient with type 2 diabetes referred by PCP
Presented with polyuria and polydipsia 2 years ago, random glucose ~ 400 mg/dl (22 mmol/l), HbA1c 11%
PMH: type 2 diabetes, HTN, hyperlipidemia
Patient started on Glipizide 20 mg qd, then titrated to 20 mg bid

Case 1
Patient started on insulin, NPH 30 units qHS,
titrated up to 78 units qHS
A1c down to 7.6
Lispro insulin then added at biggest meal of the
day
With insulin therapy A1c down to 7.2, weight up
by 22 pounds (10 kg)
What is the next step?

240
250
260
270
280
4
5
6
7
8
9
10
A1c
lb
1 2 3 4 5 6 7 8 9
Start NPH at bedtime
Exenatide added
years
Case 1
Lispro added at dinner

Case 1
Patient was switched from basal insulin plus
prandial to basal and Exenatide
Total insulin daily dose decreased from 95 units
to 75 units
Weight down 36 pounds (16 kg) on Exenatide
and kept off for > 9 years
A1c has remained < 7% for > 9 years
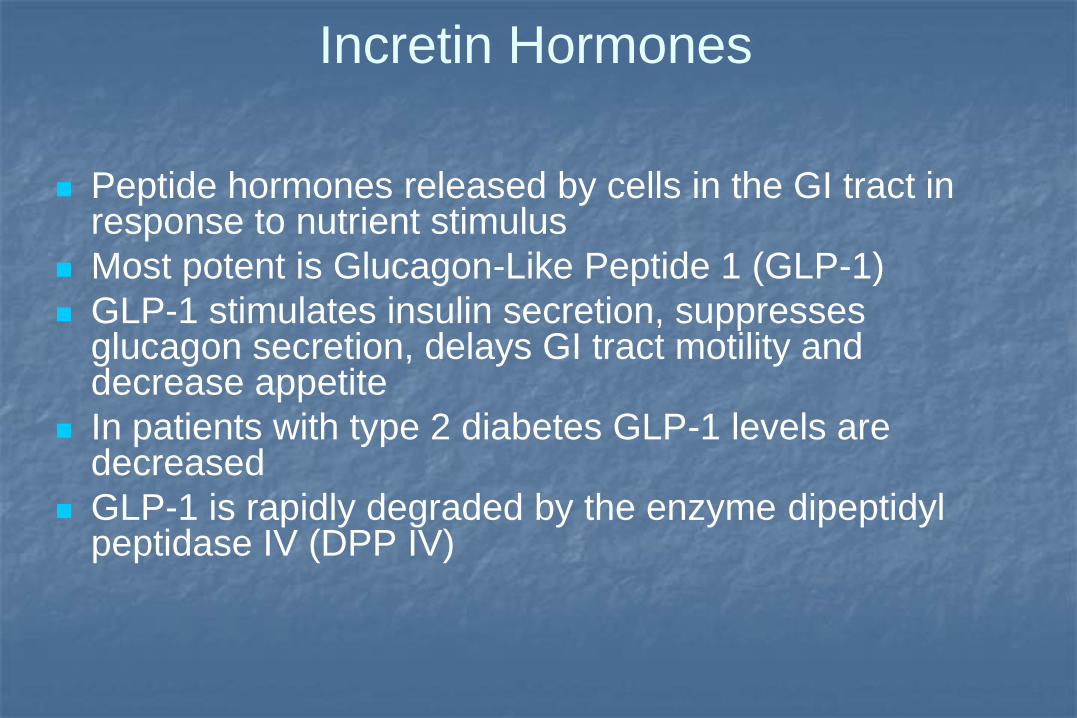
Incretin Hormones
Peptide hormones released by cells in the GI tract in response to nutrient stimulus
Most potent is Glucagon-Like Peptide 1 (GLP-1)
GLP-1 stimulates insulin secretion, suppresses glucagon secretion, delays GI tract motility and decrease appetite
In patients with type 2 diabetes GLP-1 levels are decreased
GLP-1 is rapidly degraded by the enzyme dipeptidyl peptidase IV (DPP IV)

Strategies To Prolong GLP-1 Action
GLP-1
(active) GLP-1
(inactive)
DPP-4
1. GLP-1 Agonists • Exenatide (Byetta®)
• Liraglutide (Victoza®)
• Exenatide ER (Bydureon®)
• Albiglutide (Tanzeum®)
• Dulaglutide (Trulicity®)
• Lixisenatide (Adlyxin®)
2. DPP-4 Inhibitors • Sitagliptin (Januvia®)
• Saxagliptin (Onglyza®)
• Linagliptin (Tradjenta®)
• Alogliptin (Nesina®)

Effects of Exenatide versus Aspart Insulin in Type 2 Diabetes
Nauck et al, Diabetologia 50:259-267, 2007
5 kg

Glucagon-Like Peptide 1 Receptor Agonist or Bolus Insulin with
Optimized Basal Insulin in Type 2 diabetes
Diabetes Care 2014;37:2763-2773

Comparison of adding weekly GLP-1 agonist
versus 3 daily Lispro injections
Diabetes Care 2014;37:2317-25

Exenatide once weekly versus twice daily
for the treatment of type 2 diabetes
Drucker et al. Lancet 372;1240-1250, 2008
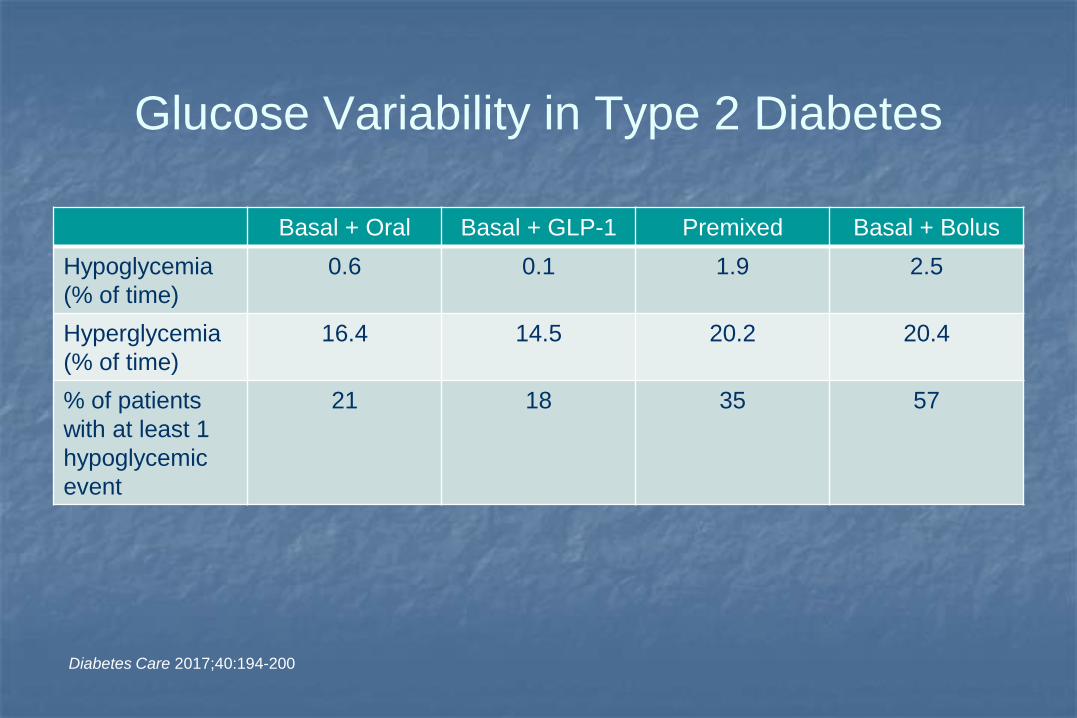
Glucose Variability in Type 2 Diabetes
Basal + Oral Basal + GLP-1 Premixed Basal + Bolus
Hypoglycemia
(% of time)
0.6 0.1 1.9 2.5
Hyperglycemia
(% of time)
16.4 14.5 20.2 20.4
% of patients
with at least 1
hypoglycemic
event
21 18 35 57
Diabetes Care 2017;40:194-200

Risk of pancreatitis in patients treated with incretin-based therapies
Diabetologia 2014; 57:1320-24

GI adverse events of Liraglutide
Liraglutide Placebo Difference
Nausea 40 15 25%
Diarrhea 21 9 12
Constipation 20 9 11
Vomiting 16 4 12
Dyspepsia 9 3 6
Abdominal Pain 5 3 2
N Engl J Med 2015;373:11-22

GLP-1 Receptor Agonists
Exenatide (Byetta®)
Twice/day sc. Injections
Start with 5 mcg bid within 60 minutes of a meal and after 1 month increase the
dose to 10 mcg bid if eGFR > 30 ml/min
Liraglutide (Victoza®)
Once day sc injection, “use with caution in renal impairment”
Start with 0.6 mg qd for 1 week, then increase to 1.2 mg qd; may go to 1.8 mg qd
Exenatide ER (Bydureon®)
Once per week injection 2 mg, do not use if eGFR < 30 ml/min
Albiglutide (Tanzeum®)
Once per week injection, 30 mg, can increase to 50 mg if eGFR> 15 ml/min
Lixisenatide (Adlyxin®)
Once per day, start at 10 mcg per day and increase to 20 mcg/day after 2 weeks
Dulaglutide (Trulicity®)
Once per week, start 0.75 mg, can increase to 1.5 mg. No renal dose adjustement
needed

Case 2
78 year old patient with 12 years history of type 2 diabetes
Very physically active, competitive snowboarder
PMH: type 2 diabetes, HTN, hyperlipidemia, hypothyroidism, benign prostatic hypertrophy
Patient on Metformin 1000 mg bid, Aspirin 81 mg qd, Atorvastatin 10 mg qd, Levo-thryoxine 100 mcg qd, Lisinopril 20 mg qd
Normal renal function, A1c 8.3
What is the next step?

Case 2
Years
Sitagliptin added

Case 2
A1c levels came back to goal and remained at
goal for > 2 years
DPP-4 Inhibitors well tolerated with minimal side
effects
Low risk of hypoglycemia, important in elderly
patients
No weight gain

Efficacy of sitagliptin in patients with type 2
diabetes
J Diabetes 2013; 5:68-79

Diabetes Medications for Adults With Type 2 Diabetes: An Update
Agency for Healthcare Research and Quality (US); 2016 Apr.Report No.: 16-EHC013-EF

Agency for Healthcare Research and Quality (US); 2016 Apr.Report No.: 16-EHC013-EF
Diabetes Medications for Adults With Type 2 Diabetes: An Update

Saxagliptin and Cardiovascular Outcomes in
Patients with Type 2 Diabetes Mellitus
N Engl J Med 2013;369:1317-26

Diabetes Care 2016 May; 39(5): 735-737
FDA warning: saxagliptin and alogliptin may increase the risk of heart failure,
particularly in patients who already have heart or kidney disease
DPP-4 Inhibitors and Heart Failure

Risk of pancreatitis in patients treated with incretin-based therapies
Diabetes Care 2017; 40:164-70

DPP-IV Inhibitors
Sitagliptin (Januvia®) 2006
100 mg po qd (reduce dose in renal insufficiency)
Saxagliptin (Onglyza®) 2009
2.5 or 5 mg po qd (reduce dose in renal insufficiency)
Linagliptin (Tradjenta®) 2011
2.5 mg po qd (no renal adjustment)
Alogliptin (Nesina®) 2013
25 mg po qd (reduce dose in renal insufficiency)

DPP-4 Inhibitors
Less powerful than sulfonylureas
Minimal risk of hypoglycemia
Less weight gain than sulfonylureas
Easy to use and tolerate
Neutral effects on cardiovascular disease
Risk of heart failure?
Risk of pancreatitis?

Case 3
57 year old woman with type 2 diabetes referred by PCP
Diagnosed with diabetes in 2010, A1c was 8.2, started on Metformin at the time. Now A1c 8.1
PMH: type 2 diabetes, HTN, hyperlipidemia, obesity, hypothyroidism, OSA, GERD
Medications: Metformin 1000 mg bid, aspirin 81 mg qd, Levothyroxine 100 mcg qd, Losartan 100 mg qd, Nifedipine ER 60 mg qd, Omeprazole 40mg qd, Simvastatin 20 mg qd
What is the next step?

Case 3
Years
Case 3
Significant improvement in A1c (at goal for 1
year)
Weight loss of 8 pounds
Developed 1 episode of UTI (? drug related?)
CVD benefit?

Sodium-Glucose Co-Transporter 2 Inhibition

Effects of Canaglifozin in Patients with Type 2 Diabetes
Diabetes, Obesity and
Metabolism 15:372-382,
2013

Lancet Diabetes Endocrinol 2014;2:691-700
Comparison of Empagliflozin and Glimepiride as add-on to Metformin in patients with
type 2 diabetes: a 104 week randomized, active controlled, double-blind, phase 3 trial
Glimepiride
Empagliflozin

Long-term glycaemic response and tolerability of dapagliflozin versus a sulphonylurea
as add-on therapy to metformin in patients with type 2 diabetes: 4-year data
Diabetes, Obesity and Metabolism 2015;17:581-90

SGLT2-associated “euglycemic” DKA
DKA occurred in 12 of 17,596
patients in canagliflozin program <1
per 1000 patient-years
Most were insulin-treated or, in
retrospect, had LADA
Other triggers are carbohydrate
restriction, insulin cessation,
illness, alcohol
Hyperglycemia may be absent
A predicatable occurrence in type 1
DM
Peters AL. Diabetes Care 2015; Erondu. Diabetes Care 2015; Rosenstock J. Diabetes Care 2016; Ogawa W. JDI 2016
SGLT2
↓Blood glucose
↑ ↑ Glycosuria
↓Insulin/glucagon
ratiofavorable to
ketogenesis
Trigger plus ↑ ↑ Glycosuria
Euglycemic DKA

Adverse Events in the EMPA-REG
OUTCOME Trial
Placebo Empagliflozin 10 mg Empagliflozin 25 mg
UTI male 9 11 10%
UTI female 41 36 37
Gen. Infection male 2 5 5
Gen Infection female 3 9 11
N Engl J Med 2015;373:2117-28

SGLT-2 Inhibitors
Canagliflozin (Invokana®) 2013
100 mg qd, if eGFR> 60 mg/min can increase to 300
mg qd
Dapagliflozin (Farxiga®) 2014
5 or 10 mg qd, do not use if eGFR< 60 mg/min
Empagliflozin (Jardiance®) 2014
10 to 25 mg qd, do not use if eGFR < 45 mg/min
Side effects: •Polyuria •UTI •Genital infections •Hypovolemia •DKA

FDA Guidance—2008 Goal: to demonstrate
cardiovascular safety
Approach
Blinded central adjudication of
CVD events
Inclusion of high-risk subjects:
advanced CVD, elderly, CKD
Minimum exposure of 2 years in
large CVOT
Approximately 15,000 pt-yrs
Adapted from Inzucchi, SI Yale 2016 and Darren McGuire, UTSW Medical Ctr, 2015
Glucose Lowering Medications and Cardiovascular Disease

Study SAVOR EXAMINE TECOS CAROLINA CARMELINA
DPP4-i saxagliptin alogliptin sitagliptin linagliptin linagliptin
Comparator placebo placebo placebo sulfonylurea placebo
N 16,500 5,400 14,000 6,000 8,300
Results 2013 2013 2015 2017 2017
Study LEADER ELIXA SUSTAIN 6 EXSCEL REWIND
GLP1-RA liraglutide lixisenatide semaglutide exenatide LR dulaglutide
Comparator placebo placebo placebo placebo placebo
N 16,500 14,000 6,000 5,400 8,300
Results 2016 2015 2016 2018 2019
Study EMPA-REG CANVAS DECLARE NCT01986881
SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin
Comparator placebo placebo placebo placebo
N 7300 4300 22,200 3900
Results 2015 2017 2019 2020
Large CV Outcomes Trials in Diabetes post-2008
✓
✓ ✓ ✓
Slide courtesy of Silvio Inzucchi, Yale

Summary of early CVD Outcomes Trials
All cardiovascular disease outcomes trials have enrolled people
at high risk of CVD outcomes
Most trials of new diabetes drugs have shown neither benefit nor
harm
Most have had a small difference in glycemic control between
the intervention and control group
On the order of 0.5% A1C
It seems likely that differences in glycemic control of this
magnitude, in this population, have no impact on cardiovascular
disease risk

EMPA-REG CVD Outcomes
Zinman B et al. N Engl J Med 2015;373:2117-2128
CVD benefit apparent at 3 months… A1C difference ~0.5
Primary outcome (CVD death, non-fatal MI, stroke) HR 0.86 (0.74-0.99)
CVD Death HR 0.62 (0.49-0.77)
All-cause Death HR 0.68 (0.57-0.82)

Study SAVOR EXAMINE TECOS CAROLINA CARMELINA
DPP4-i saxagliptin alogliptin sitagliptin linagliptin linagliptin
Comparator placebo placebo placebo sulfonylurea placebo
N 16,500 5,400 14,000 6,000 8,300
Results 2013 2013 2015 2017 2017
Study LEADER ELIXA SUSTAIN 6 EXSCEL REWIND
GLP1-RA liraglutide lixisenatide semaglutide exenatide LR dulaglutide
Comparator placebo placebo placebo placebo placebo
N 16,500 14,000 6,000 5,400 8,300
Results 2016 2015 2016 2018 2019
Study EMPA-REG CANVAS DECLARE NCT01986881
SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin
Comparator placebo placebo placebo placebo
N 7300 4300 22,200 3900
Results 2015 2017 2019 2020
Large CV Outcomes Trials in Diabetes post-2008
✓
✓ ✓ ✓
✓
Slide courtesy of Silvio Inzucchi, Yale

LEADER Outcomes
Marso SP et al. N Engl J Med 2016.
Benefit apparent at 1 year
Primary outcome (CVD death, non-fatal MI, stroke) HR 0.87 (0.78-0.97)
CVD Death HR 0.78 (0.66-0.93)
All-cause Death HR 0.85 (0.74-0.97)

Study SAVOR EXAMINE TECOS CAROLINA CARMELINA
DPP4-i saxagliptin alogliptin sitagliptin linagliptin linagliptin
Comparator placebo placebo placebo sulfonylurea placebo
N 16,500 5,400 14,000 6,000 8,300
Results 2013 2013 2015 2017 2017
Study LEADER ELIXA SUSTAIN 6 EXSCEL REWIND
GLP1-RA liraglutide lixisenatide semaglutide exenatide LR dulaglutide
Comparator placebo placebo placebo placebo placebo
N 16,500 14,000 6,000 5,400 8,300
Results 2016 2015 2016 2018 2019
Study EMPA-REG CANVAS DECLARE NCT01986881
SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin
Comparator placebo placebo placebo placebo
N 7300 4300 22,200 3900
Results 2015 2017 2019 2020
Large CV Outcomes Trials in Diabetes post-2008
✓
✓ ✓ ✓
✓
Slide courtesy of Silvio Inzucchi, Yale
✓

SUSTAIN-6 Outcomes Primary outcome (CVD death, non-fatal MI, stroke) HR 0.74 (0.58-0.95)
CVD Death HR 0.98 (0.65-1.48)
All-cause Death HR 1.05 (0.74-1.50)
Weight and glycemic control improved most with highest dose semaglutide, with treatment difference of 4.3 kg and HbA1c of 1.0%
***Increased risk of retinopathy complications in semaglutide group, though numbers were small.

Study SAVOR EXAMINE TECOS CAROLINA CARMELINA
DPP4-i saxagliptin alogliptin sitagliptin linagliptin linagliptin
Comparator placebo placebo placebo sulfonylurea placebo
N 16,500 5,400 14,000 6,000 8,300
Results 2013 2013 2015 2017 2017
Study LEADER ELIXA SUSTAIN 6 EXSCEL REWIND
GLP1-RA liraglutide lixisenatide semaglutide exenatide LR dulaglutide
Comparator placebo placebo placebo placebo placebo
N 16,500 14,000 6,000 5,400 8,300
Results 2016 2015 2016 2018 2019
Study EMPA-REG CANVAS DECLARE NCT01986881
SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin
Comparator placebo placebo placebo placebo
N 7300 4300 22,200 3900
Results 2015 2017 2019 2020
Large CV Outcomes Trials in Diabetes post-2008
✓
✓ ✓ ✓
✓
Slide courtesy of Silvio Inzucchi, Yale
✓ ✓

•In patients with long standing type 2 diabetes and
established cardiovascualr disease, Empagliflozin or
Liraglutide should be considered as they have been
shown to reduce cardiovascular and all cause mortality
when added to standard care
•FDA approved new indication for Empagliflozin for
reduction of CVD death
Standards of Medical Care in Diabetes – 2017
American Diabetes Association
New Drugs for Type 2 Diabetes
FDA Approved over the last year
Basaglar
Degludec (Tresiba)
Degludec/Aspart (Ryzodeq)
Lixisenatide (Adlyxin)
Glargine/Lixisenatide (Soliqua)
Degludec/Liraglutide(Xulthopy)

Xultophy Dosing:
• Recommended starting dose is
16 units of degludec (and 0.58
mg of liraglutide)
• Maximum daily dosage 50 units
of degludec and 1.8 mg
liraglutide
New combination treatment of basal insulin and
GLP-1 analog

Take Home Messages
GLP-1 Analogs: As effective as prandial insulin but with less hypoglycemia and weight loss
Good post-prandial efficacy
About 25% of patients can not tolerate for GI side effects
Decrease CVD mortality and morbidity
DPP-4 Inhibitors: Less powerful than other oral agents
Easy to use, also in patients with CKD
Minimal risk for hypoglycemia
Consider for elderly, simple regimens, patients unable to tolerate
Metformin
SGLT-2 Inhibitors: Consider as second line agents
Decrease CVD mortality and morbidity
Monitor for risk of DKA