Embed Size (px)
Citation preview

Recent Advances in Neonatology
Jonathan Fanaroff, MD, JDAssistant Professor of PediatricsCase School of Medicine
DirectorRainbow Center for Pediatric EthicsRainbow Babies & Children's HospitalCleveland, Ohio
34th Annual Perinatal SymposiumAdvocate Christ Medical CenterHope Children’s HospitalNovember 17-18, 2010Oak Lawn, Illinois

I have no conflicts of interest to disclose
I will not be discussing off label uses of any drugs or devices
All pictures were obtained from public sources


NEONATAL REPORT CARD
• Prevent prematurity – MINIMAL PROGRESS• Reduce asphyxia - HYPOTHERMIA
EFFECTIVE BUT ADJUNCTIVE RX NEEDED• Eliminate GBS and nosocomial infections – GBS
reduced; nosocomial infections – PROGRESS.• Reduce NEC – PROBIOTICS?• Prevent barotrauma- BPD- CPAP >
SURFACTANT/MECHANICAL VENTILATION• Prevent retinopathy - LOWER OXYGEN
SATURATION?• Avoid iatrogenesis/medication errors- HIGH
PRIORITY- STILL TOO MANY MISTAKES

Courtesy of Linda deVries


FETAL TREATMENTESTABLISHED
• Twin-twin transfusion• CCAM with hydrops• Sacrococcygeal teratoma• Posterior Urethral Valves• Fetal arrhythmias• Airway compromise

FETAL TREATMENT FUTURE
• Stem cell transplantation• Gene therapy• Correction of birth defects• Wound healing without scars

BENEFITS OF DELAYED CORD CLAMPING IN PRETERM INFANTS
• Increased blood volume• Improved circulatory and
respiratory function including higher BP
• Improved cerebral oxygenation• Reduced intraventricular
hemorrhage• Increased urine output

BENEFITS OF DELAYED CORD CLAMPING IN PRETERM INFANTS
• Higher hematocrit• Acquisition of progenitor cells- this facilitates
red blood cell production and enhances the immune system
• Reduced need for blood transfusions• Reduced NEC• Reduced Late Onset Sepsis

HARM OF DELAYED CORD CLAMPING IN PRETERM INFANTS
• No adverse effects of delayed cord clamping for preterm infants have been identified except higher peak serum bilirubin concentration (Reynolds, 2008).
• Delayed cord clamping does not effect survival of preterm infants (Rabe et al, 2004; Rabe et al, 2008).
• There has been only one report examining the impact of delayed cord clamping on neurodevelopmental outcome (Mercer et al, 2010). The investigators found evidence of improved motor scores at 7 months corrected age in preterm infants who had received delayed cord clamping at birth.

DELAYED CORD CLAMPING
• Despite knowledge since the 1960s that delayed clamping of the umbilical cord increases the volume of placental transfusion in both term and preterm infants and continued studies which show benefits and little, if any, risk in preterm infants, it has not gained wide acceptance

Baby girl, Twin B, 24 weeks GA, BW 585 g, No ANS; Vaginal delivery; 2 days old, RDS;MECHANICAL VENTILATION;Grade I IVH, BRUISED,hyperbilirubinemia, phototherapy
PREVENT PREMATURITY

PREMATURITY
• The frequency of preterm births is about 12-13% in the USA and 5-9% in many other developed countries;
• The rate of preterm birth has increased in many locations, predominantly because of increasing indicated preterm births and preterm delivery of artificially conceived multiple pregnancies.
• Common reasons for indicated preterm births include pre-eclampsia or eclampsia, and intrauterine growth restriction.

HOT TOPICS • PREVENTING/REDUCING LATE PRETERM BIRTHS• Late Preterm infants represent almost three-
fourths of all premature births in the United States.
• The identification of late preterm infants as a high-risk group of infants has been an important public health breakthrough.
• Before the recognition that late preterm infants have unique physiology and risks, they constituted a relative 'silent morbidity and mortality'

LATE PRETERM BIRTH : PREVENTION
OSHIRO – Concerted system and multidisciplinary team effort changed culture and reduced deliveries before
39 weeks from 28% to 3%OHIO PERINATAL COLLABORATIVE
Document G.A. and reason for delivery= RESULTED IN INDUCTIONS WITHOUT
INDICATIONS DECREASING FROM 13%-8%

PREMATURITY –FACTORS AFFECTING SURVIVAL
• Approach to and changing borders of viability? Importance of– Birth weight; – gestational age– gender– antenatal steroids– site and time of delivery – mode of delivery
Born at home at 25 weeks gestation. Male,600g, Temp. 33oC on arrival in peripheral hospital. .

SURVIVAL -NICHD -NRN 1998 – 2003 (n = 4165) JAPAN and LITERATURE
GA SURVIVAL JAPAN DANI
22 wk 5 % 40 % 2%
23 wk 26 % 60 % 13%
24 wk 56 % 80 % 35%
25 wk 76 % 85 % 56%
• Tyson 2008; Itabashi 2009 Dani 2009

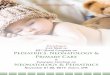
Copyright ©2010 American Academy of Pediatrics
Stoll, B. J. et al. Pediatrics 2010;126:443-456
FIGURE 1 Survival to discharge according to GA among 9575 VLBW infants born in NICHD NRN centers between January 1, 2003, and December 31, 2007

NICHD Neonatal Network 1998 – 2003 (n = 4165)
GA survival NDI survival w/o NDI
22 wk 5 % 80 % 1 %
23 wk 26 % 65 % 9 %
24 wk 56 % 50 % 28 %
25 wk 76 % 39 % 46 %

THE MYTH OF OXYGEN
200 years after its discovery we do not know • The optimal oxygen concentration or oxygen
saturation during resuscitation of the newly born.
• The optimal oxygen saturation in treating extremely low birth weight infants.
• Short and long term effects on morbidity and mortality, growth and development of using oxygen in the newborn period.

How much Oxygen is needed?• What is the evidence to lower initial FiO2 ?
– Clinical data have demonstrated that pure oxygen:• Increases neonatal mortality (~ 40%, also in developed
countries).• Increases oxidative stress at least 4 weeks after birth.• Increases myocardial and kidney injury.• Delays recovery (significantly lower 5 min Apgar score
and heart rate; prolonged time to first breath and first cry)
• Increases time of resuscitation needed and oxygen.• Is associated with higher risk of childhood leukemia
and cancer.(Saugstad OD, Ramji S, Vento M. Pediatrics 2006; )

01
02
03
04
05
06
07
08
09
01
00O
xyge
n sa
tura
tion
(%)
1 2 3 4 5 6 7 8 9 10minutes from birth
10-90th centile median
Term Neonates > 37 weeks gestation
Dawson Ja et al Pediatrics 2010

01
02
03
04
05
06
07
08
09
01
00O
xyge
n sa
tura
tion
(%)
1 2 3 4 5 6 7 8 9 10minutes from birth
10-90th centile median
Preterm < 37 weeks gestation
Dawson Ja et al Pediatrics 2010

0
200
400
600
800
1000
ml O2 / kg
Oxygen load in ELBW infants resuscitated initially with 30% or 90% FiO2.
Lox group Hox group
Lox group 465
Hox group 864
1
Escrig R et al Pediatrics 2008

Copyright ©2010 American Academy of Pediatrics
Kattwinkel, J. et al. Pediatrics 2010;126:e1400-e1413
2010 AHA Neonatal Resuscitation Guidelines



Pulse Ox in the Delivery Room
• Use when resuscitation can be anticipated• Use when PPV is given for more than a
few breaths• Use when cyanosis is persistent• Use when supplementary oxygen is
administered• Measure preductal sat (Right UE)

Oxygen in the Delivery Room
• Can start with room air or blended O2
• Goal is an oxygen saturation value in the interquartile range of preductal sats in healthy term babies born via vaginal delivery at sea level
• If blended oxygen is not available, resuscitation should be initiated with room air

1930’s-1950’s: Oxygen Rx, no Mechanical Ventilation

“We have no proof that the regular type of respiration, which we are accustomed to consider “normal,” is better for a premature infant than the periodic type of breathing described. Likewise, we have no convincing evidence that an increased oxygen content of arterial blood is beneficial or necessarily of importance. It is evident, however, that these healthy premature infants breathed in a more normal manner in an oxygen-enriched atmosphere.”
Wilson JL et al. Am J Dis Child 1942;63:1080-5

Oxygen & RLF
Singleton RLF
Mutliples RLF
Singleton Scarring
RLF
Multiples Scarring
RLF
0
10
20
30
40
50
60
70
80
90
70
83
17
67
31
42
5
14
Routine OxygenCurtailed Oxygen

Deaths on day of birth /1000 live births
Mortality on the first day of life in the United States and in England and Wales before (open circles and squares) and after (closed circles and squares) oxygen restriction. (Redrawn from Bolton and Cross, 1974).

History of Perinatology
1940 -
1960
Respiratory distress
Blindness from ROP
Liberal O2
Restricted O2
ROP
Death & CP
Year Problem Treatment Iatroepidemic

Bill Silverman
Teach thy tongue to say I do not know and thou shalt progress.

SUPPORT Trial
SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Target ranges of oxygen saturation in extremely preterm infants. N Engl J Med 2010;362:1959-1969

PRIMARY OUTCOME
Lower Saturation
GroupN=654
Higher Saturation
GroupN=662
Adjusted Relative Risk
(95% CI)
Severe ROP/death 28.3% 32.1% 0.90 (0.76,
1.06)Severe ROP 8.6% 17.9% 0.52 (0.37,
0.73) NNT=11
Death 19.9% 16.2% 1.27 (1.01, 1.60) NNH=27
Carlo NICHD- Support Trial NEJM 2010

Feasibility of Automated Regulation ofInspired O2 in Ventilated Preterm Infants
Perc
en
t of
Tim
e
O2 Saturation (SpO2)
Claure, (Pediatrics)
*
*p<0.02
*
0
10
20
30
40
50
60
88-95% >95%
Automated Routine



GBS
• Recommendations for universal screening were rapidly adopted and GBS disease has declined.
• Improved management of preterm deliveries and improved collection, processing, and reporting of culture results may prevent additional cases of early-onset group B streptococcal disease.

GBS GUIDELINES 2010still in final reviews
• GBS remains the leading cause of EOS• Antenatal GBS screening and intrapartum
antibiotic prophylaxis (IAP) for culture- +ve and high risk remain foundation
• ? New features address preterm labor, mothers with penicillin allergy and culture techniques.

Advances in Nutrition
Denne and P
oindexter, Sem
Perinatol 2007

Protein Intake for VLBW Infants• TPN – usually 3.5 g/kg/d. Closer to 3.0
g/kg/d at term.• Up to 4.0 g/kg/d in some very small
infants.• Provide 2 – 3 g/kg/d from birth when
possible,• advance to full protein in 3-4 days.• Monitor BUN (what is too high/low?), little
benefit to monitoring albumin/pre-albumin
S. Abrams, MD

PROBIOTICS• Probiotics investigated
extensively but not in the USA• No approved product• Debate on best bacilli, dose,
duration of therapy, • Potential risks?-sepsis;allergy

Preventive Probiotic Trials in Preterm Infants
Study Hoyos 1999
Dani 2002
Lin 2005
Bin-Nun 2005
Lin 2008
Samanta 2008
Probiotic species
L. acidophilus B. infantis (Infloran®)
L. GG L. acidophilus B. infantis (Infloran®)
ABCdophilus® S. Thermophilus
B. infantis
B. bifidum
L. Acidophilus B. bifidum (Infloran®)
B. Infantis B. bifidum B. longum L. acidophilus
Effect Decreased NEC vs historic controls
1.4% vs 2.7%, NS
1.1% vs 5.3%, p < 0.05
1% vs 14%, p < 0.05
1.8% vs 6.5%, p = 0.02
5.5% vs 15.8%, p = 0.04
Probiotics: 53/2093 (2.5%) vs Control: 142/2143 (6.6%) p<0.01, NNT=24

Copyright ©2010 American Academy of Pediatrics
Deshpande, G. et al. Pediatrics 2010;125:921-930
FIGURE 2 Effect of probiotics on NEC

Copyright ©2010 American Academy of Pediatrics
Deshpande, G. et al. Pediatrics 2010;125:921-930
FIGURE 3 Effect of probiotics on blood culture-positive sepsis

Copyright ©2010 American Academy of Pediatrics
Deshpande, G. et al. Pediatrics 2010;125:921-930
FIGURE 4 Effect of probiotics on all-cause mortality

DESHPANDE ET AL
• The results of our update confirm those of the previous systematic reviews while improving their precision and further reducing the role of chance alone.
• The dramatic benefits in terms of reduced risk for all-cause mortality and definite NEC are sustained; however, despite the addition of 4 new trials (N = 783) to the existing data, there is still no evidence that probiotic supplementation reduces the risk for LATE ONSET SEPSIS.

• Ten different probiotics used in 11 studies• None of the studies were done in the U.S.• No FDA approved probiotics for preemies• Quality control in manufacturing a concern• We don’t know which products in which
population of at-risk neonates

S. Abrams, MD

LACTOFERRIN
• Lactoferrin, an iron-binding protein with multiple physiological functions –anti-microbial, –anti-inflammatory– immunomodulatory,
is one of the most important proteins present in mammalian milk.

Bovine Lactoferrin supplementation for prevention of late-onset sepsis in very low-birth-weight neonates: a randomized trial.
• INTERVENTION: Infants were randomly assigned to receive orally administered Bovine Lactoferrin (BLF) (100 mg/d) alone (n = 153), BLF plus Lactobacillus GG (6 x 10(9) colony-forming units/d) (n = 151), or placebo (n = 168) from birth until day 30 of life (day 45 for neonates <1000 g at birth).
Manzoni et al JAMA. 2009; 302:1421-8.

Bovine Lactoferrin supplementation for prevention of late-onset sepsis in very low-birth-weight neonates: a
randomized trial.
• MAIN OUTCOME MEASURE: • First episode of late-onset sepsis, ie,
sepsis occurring more than 72 hours after birth with isolation of any pathogen from blood or from peritoneal or cerebrospinal fluid.
Manzoni et al JAMA. 2009; 302:1421-8.

Results :
LactoFerrin+LactobacillusGG vs. PLACEBOLF + LGG
(n=137)PLACEBO (n=153)
R.R. 95% C.I.
p-value
Late-Onset sepsis (all agents)
11/137(8.0%)
37/153(24.2%)
0.23 0.13-0.56
0.001
Total IFI (%) 3/137(2.2%)
12/153(7.8%)
0.33 0.08-0.78
0.02
NEC 0/137(0%)
10/153(6.5%)
0.11 0.18-0.54
0.002
Overall Mortality
6/137(4.4%)
13/153(8.5%)
0.41 0.08-1.09
0.09

LF combinedn =(139+137) = 276
PLACEBO n = 153
R.R. 95% C.I.
p-value
Late-Onset sepsis (all agents)
23/276(8.3%)
37/153(24.2%)
0.28 0.16-0.50
<0.001
LOS by Gram-Positive 1.8% 7.8% 0.21 0.07-0.62 0.002
LOS by Gram-Negative 5.4% 10.5% 0.48 0.35-0.98 0.05
LOS by Candida spp 1.8% 7.8% 0.21 0.07-0.62 0.002
NEC 2/276(0.7%)
10/153(6.5%)
0.10 0.02-0.48 <0.001
Mortality (all causes prior to discharge)
3.3% 8.5% 0.36 0.15-0.87
0.02
Death OR NEC 4.7% 12.4% 0.34 0.16-0.72
0.004
RESULTS : LF combined (alone or with LGG) vs. PLACEBO
Power calculations: 0.95 for LOS, 0.74 for NEC, 0.65 for IFI, 0.45 for mortality

Bovine Lactoferrin supplementation for prevention of late-onset sepsis in very low-birth-weight neonates: a randomized trial.
• CONCLUSION: • Compared with placebo, Bovine
Lactoferrin supplementation alone or in combination with Lactobacillus rhamnosus GG (LGG) reduced the incidence of a first episode of late-onset sepsis in VLBW neonates.
Manzoni et al JAMA. 2009; 302:1421-8.


NEURO-DEVELOPMENTAL OUTCOME
• “Long term neuro-developmental consequences of extreme prematurity are mediated not only by acute destructive events but also by disruptive effects on subsequent brain development in regions adjacent to and remote from the original injury.”
• Volpe JJ Lancet Neurol 2009;8;110-124

CEREBELLAR INJURY
• Cerebellar injury is a previously under recognized form of prematurity related brain injury
• Cerebellar injury in the preterm infant is associated with impaired growth of the uninjured contralateral cerebral hemisphere with significant impairment evident as early as term equivalent

CEREBELLAR INJURY (CI)
• Limperopolous measured volumes of cortical and subcortical gray matter and white matter in 38 preterm infants with MRI evidence of cerebellar injury.
• Unilateral CI was associated with significantly smaller volumes of cortical gray and cerebral white matter incontralateral cerebral hemisphere.
• Limperopoulos Pediatr Res 68;145-150,2010

CEREBELLAR INJURY (CI)
• Regions affected were dorso-lateral prefrontal, premotor, sensorimotor and mid temporal regions.
• With bilateral CI –no significant inter hemispheric differences
• Hence regional cerebral growth impairment results from interruption of cerebrocerebral connectivity and loss of neuronal activation critical for development
• Limperopoulos Pediatr Res 68;145-150,2010


COOLING BLANKET FOR HIE

Epidemiology of Perinatal Asphyxia
• Of ~ 130 million annual births world-wide, 4 million have evidence of birth asphyxia (30 per thousand). Of these 1 million die and 1 million develop neurologic sequelae.

BIRTH ASPHXIA -HIE
• HIE is one of the leading causes of neurocognitive and motor delay in the pediatric age.– HIE moderate:
• 10% die• 30% neurocognitive/motor delay
– HIE severe: • 60% die • ~100% neurocognitive/motor delay
• No substantial changes in medical approach for decades.

Epidemiology of Perinatal Asphyxia
• Although the incidence of birth asphyxia is lower in the Western world, the annual rate is still high (3-6 per thousand term births).
• Over the past 20 years, the incidence of birth asphyxia has remained constant, despite major advances in perinatal medicine

Mechanism of Action of Hypothermia
• Reduces cerebral metabolism• Prevents cerebral edema• Preserves ATP levels; decreases energy
utilization• Reduces/suppresses cytotoxic AA accumulation• Reduces NO synthase activity• Suppresses free radical activity• Inhibits apoptosis [cell death]• Prolongs therapeutic window? Shankaran

ENCEPHALOPATHY ENROLLMENT CRITERIA FOR HYPOTHERMIA TRIALS
• A hypoxic-ischemic insult occurring around the time of birth resulting in an encephalopathic state characterized by the need for resuscitation at birth, severe metabolic acidosis, neurological depression, seizures and electroencephalographic abnormalities.
• Enrollment within 6 hours

Induced HypothermiaDeath/Severe Neuromotor Disability
0%
10%
20%
30%
40%
50%
60%
70%
CoolCap* NICHD**
Treated
Control
56%57%
39%46%
*RR 0.81 [0.62, 1.05], p=0.10; **RR 0.72 [0.52, 0.95], p=0.02

Edwards, A D. et al. BMJ 2010;340:c363
Therapeutic hypothermia compared with normothermia
death or disability ("events").

Edwards, A D. et al. BMJ 2010;340:c363
Therapeutic hypothermia compared with normothermiaNormal Neurologic Function ("events").

Edwards, A D. et al. BMJ 2010;340:c363
Therapeutic hypothermia compared with normothermiaMortality ("events").

Edwards, A D. et al. BMJ 2010;340:c363
Therapeutic hypothermia compared with normothermiaDeath or Disability stratified by severity of encephalopathy
("events").

CURRENT STATUS HYPOTHERMIA
WBH/SHC are relatively safe– Reduce mortality due to HIE.
–Increase intact survival at 2 years of age.
–Number needed to treat (NNT) of 6-8.

Cilio MR, Ferriero DM Synergistic neuroprotective therapies with hypothermia.
Semin Fetal Neonatal Med;2010;15;293
• Neuroprotection is a major health care priority, given the enormous burden of human suffering and financial cost caused by perinatal brain damage.
• With hypothermia as therapy for term HIE, there is hope for repair and protection of the brain after a profound neonatal insult.
• However, it is clear from the published clinical trials and animal studies that hypothermia alone will not provide complete protection or stimulate the repair that is necessary for normal neuro developmental outcome.

Cilio MR, Ferriero DM Synergistic neuroprotective therapies with hypothermia.
Semin Fetal Neonatal Med;2010;15;293
• Possible adjunctive and synergistic therapies with hypothermia include xenon, N-acetylcysteine, erythropoietin, melatonin and cannabinoids in addition to anti-convulsive therapy.

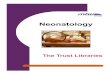
Morriss, F. H. Neoreviews 208;9:e8-e23
Copyright ©2008 American Academy of Pediatrics
Factors contributing to medical errors and the pathway from error to adverse medical event in the neonatal intensive care unit

What Should We Do ?

What Should We Do ?
Ann Intern Med 2010; 153:213-221

Thomas & Zoe Quaid





![NEONATOLOGY TODAY · les F. Simmons Jr.] Fluid and Electrolyte Management. Lippincott Williams & Wilkins. Philadelphia, USA, 2004. • Klaus and Fanaroff. Care of The High Risk Neonate,](https://img.pdfslide.net/doc/110x75/5eceb7d2ac8f391609197dea/neonatology-les-f-simmons-jr-fluid-and-electrolyte-management-lippincott-williams.jpg)