Embed Size (px)
Citation preview

Recent Advances in the Provision of Value-Based Care Models in Oncology
August 17, 2017
Debbie Stern, RPh, Senior Vice President, Medical Oncology and Specialty Drug Management, eviCore healthcare
Gergana Zlateva, Vice President, Oncology Market Access, Pfizer, Inc.

Agenda
2
Overview of Current Oncology Landscape Payer/Provider Value models Payer/Pharma Value Models Impact on Patient What’s Next?

Since 1975, the chances that a cancer patient will live 5 years or more have increased by 41% across cancers.
3
5 year survival is increasing for many cancer types
https://www.imshealth.com/files/web/IMSH%20Institute/Reports/Global_Oncology_Trends_2017/QIIHI_Oncology_Trend_Report_2017_Advances_Complexity_Cost_Exhibits.pdf

2017 APPROVALS
4
BREASTKisqali (ribociclib)
OVARIANZejula (niraparib)
NSCLCAlunbrig (brigatinib)Tagrisso (osimertinib)Keytruda (pembrolizumab)*+
Zykadia (ceritinib)*Tafinlar/Mekinest (dabrafenib/trametinib)*
MERKEL CELLBavencio (avelumab)+
ALLRydapt (midostaurin)
Urothelial/BladderImfinzi (durvalumab) +
Opdivo (nivolumab)*+
Bavencio (avelumab)*+
Keytruda (pembrolizumab)*+
NHLRituxan Hyclea (rituximab/hyalur)
HODGKIN LYMPHOMAKeytruda (pembrolizumab)*+
HEPATOCELLULAR Stivarga (regorafenib)*
Supportive therapyXermelo (telotristat ethyl)
MSI-H or dMMR solid tumorsKeytruda (pembrolizumab)*+* Approved for expanded indications
+ IV administration
2017/2018 PIPELINE- 87% are targeted therapies
Breast• Abemaciclib• Buparlisib• Neratinib• Talazoparib• Entinostat• Glembatumumab• Veliparib
NSCLC• Durvalumab*• Epacadostat• Olmutinib
Hematologic • Volsertib• Inotuzumab• Duvelisib• Momelotinib
Melanoma• Binimetinib• Encorafenib
Medical oncology new approvals and pipeline continue to grow
Since 2011, 68 new cancer drugs have been approved for 22 indications

Two-thirds of the growth in the United States oncology costs in the last five years can be attributed to the uptake of innovative medicines launched since 2011.
5
The total cost of oncology medicines rose by $20.7Bn to $44.1Bn in the United States between 2011 and 2016.
https://www.imshealth.com/files/web/IMSH%20Institute/Reports/Global_Oncology_Trends_2017/QIIHI_Oncology_Trend_Report_2017_Advances_Complexity_Cost_Exhibits.pdf

New drug therapies, lifestyle changes and improvements in screening and early disease detection are driving increased survival
6
Introduction of novel cancer drugs associated with survival increases
https://www.imshealth.com/files/web/IMSH%20Institute/Reports/Global_Oncology_Trends_2017/QIIHI_Oncology_Trend_Report_2017_Advances_Complexity_Cost_Exhibits.pdf

Cancer drug costs exceeded only by inpatient costs
7
Drug therapy represents about 20% of total cancer care spend
https://www.imshealth.com/files/web/IMSH%20Institute/Reports/Global_Oncology_Trends_2017/QIIHI_Oncology_Trend_Report_2017_Advances_Complexity_Cost_Exhibits.pdf

8
Market trends are causing disruption in oncology management
Changes create opportunity and incentives for new approaches
8
New treatments
Precision medicine
Advanced analytics
New business models / APM
Value-based care
Government mandates /regulations
Non-integrated providers and
vendors

Choosing Wisely includes recommendations for achieving the best quality care across a wide range of modalities
9
Nonevidence-based practices creates higher costs and lower quality
Key initiatives impacting cancer care:• Screening• Imaging• RT• Drugs• Genetic Testing• Surgery• Palliative Care• Survivorship
Choosing Wisely is an initiative of the ABIM/American Board of Internal Medicine) Foundation in partnership with Consumer Reports that seeks to advance a national dialogue on avoiding wasteful or unnecessary medical tests, treatments and procedures

Most common drivers of nonevidence-based prescribing:
10
• Use beyond recommended lines of therapy
• Inappropriate drug combinations within a regimen
• Genetic testing not done when indicated
• Poor performance status doesn’t support aggressive therapy
Keeping treatment consistent with the evidence
treated with chemo do not receive a treatment plan consistent with current ASCO Choosing Wisely
recommendations
Up to 40% of patients
1 Journal of Oncology Practice. 11:4. 20153 http://www.valuebasedcancer.com/vbcc-issues/2014/november-2014-vol-5-no-9/257863 eviCore, Data on File
Lack of treatment coordination and highly variable nonevidence-based practice patterns
are contributing to unnecessary costs and avoidable toxicities

Reduces avoidable ER visits and hospitalization
11
Evidence-based guidelines focus on the most appropriate treatment
Prevents/manages
side effects
Reduces toxicity
Monitors for appropriate use of G-CSF for patients on chemotherapy regimen with high risk for febrile neutropenia
Provides alternative treatment options for patients with advanced disease and poor performance status
1~30% of G-CSF use is not warranted based on regimen risk of febrile neutropenia*
1 http://www.valuebasedcancer.com/vbcc-issues/2014/november-2014-vol-5-no-9/257862Journal of Oncology Practice. 11:4. 2015
240% patients with advanced solid tumor cancers who are unlikely to benefit from therapy continue to be prescribed aggressive therapy

Physicians currently have to endure intense complexity while making treatment decisions for metastatic NSCLC.
Treatment Landscape for a Newly Diagnosed Metastatic NSCLC Patient
12
Translating clinical practice guideline into a treatment decision
https://www.imshealth.com/files/web/IMSH%20Institute/Reports/Global_Oncology_Trends_2017/QIIHI_Oncology_Trend_Report_2017_Advances_Complexity_Cost_Exhibits.pdf
NCCN compendia has > 160 Regimens for treatment of NSCLC

13
Pathway program differentiators
• Clinical source for pathways• Limitation of treatment options• Incentives for use• Ease of use/MD acceptance• Authorization capabilities• Integrated RX and Medical benefit mgt.• Ownership/potential conflicts of interest• Inclusion of multiple treatment modalities
• Lab/Genetic Testing• Radiation Therapy• Surgery• Advanced Imaging• Palliative Care• End-of-live Care

Author, Publication Title FindingsJackson, DM, et al.DOI: 10.1200/JOP.2017.021741;published online ahead of print atjop.ascopubs.org on March 4, 2017.
(Dana Farber)
Cost and Survival Analysis Before and AfterImplementation of Dana-Farber Clinical Pathways forPatients With Stage IV Non–Small-Cell Lung Cancer
22% decrease in total cost of care with no impact on clinical outcomes, primarily from chemo costs
Adeboyeje, G, et alDOI: 10.1200/JOP.2017.020867;published online ahead of print atjop.ascopubs.org on March 4, 2017.
(Anthem/Aim)
Reducing Overuse of Colony-Stimulating Factors inPatients With Lung Cancer Receiving Chemotherapy:Evidence From a Decision Support–Enabled Program
9% decrease in use of CSF with no change in the incidence of FN
Newcomer, LN, et alDOI: 10.1200/JOP.2016.015198;published online ahead of print atascopubs.org/journal/jop onOctober 18, 2016.
(United/eviCore/NCCN)
Transforming Prior Authorization to Decision Support
20% difference in chemotherapy drug cost trends for the pilotsite compared to the rest of the nation during the trial period without need for reducing therapy options or limiting provider network.
14
Do guideline adherence and pathways work?

Value means different things for different stakeholders
Outcome and cost measures need to be mutually agreed upon
Is Value Measurement the Answer?
OUTCOMECOST
VALUE
ProvidersPayers
Patients
• Improved outcomes (survival)
• Improve quality of life• Lower toxicities
Value-based contracting• Payment is tied to achievement
of goals, objectives, or performance benchmarks
• Avoid hospital days / ED visits
• Increased efficiencies• Minimize unnecessary
care

Market challenges are driving a need for better cost and appropriate use management
As value-based methodology matures, there will be more blending between UM and Cost Management
16
Payer strategies to manage medical oncology costs and utilization
$
Optimal Cancer Care
Value Based UM:Pathways/Guidelines
Indication-based formularies
Integrated patient management
Value Based Cost Management: APM• Bundle/episode of care
model• OCM Model• Outcomes based
contracts (Pharma)• Provider risk contracts

OCM is a bundled payment model where providers accept financial risk for the totality of a patient’s care over a predefined period of time
17
•.
•Goal:
•Achieve better health, improved care, and smarter spending for cancer patients through appropriately alighted financial incentives and practice redesign activities (e.g. HER technology, 24/7access to clinician, patient navigator)
•Methodology:• Launched July 1, 2016, and runs through June 30, 2021
• 6 mo episode is triggered by the initiation of chemotherapy (most cancer types)
• Medicare patient with Parts A and B coverage
• Episodes of cancer care: payment model targets chemotherapy and related care during a 6-month period following the initiation of chemotherapy treatment
• If requisite quality thresholds are met, and aggregate payments fall below the target, OCM practices will receive a performance-based payment (PBP).
•Challenges:• Infrastructure investment
• Pricing methodology that includes appropriate risk adjustments
• Reporting requirements
CMS OCM (Oncology Care Model): a test case for alternative payment model
Results not yet documented

VALUE-BASED AGREEMENTSCBI Market Access Conference,August 16-17, 2017, Philadelphia
Gergana Zlateva, VP, Oncology Market Access Pfizer

Disclaimer
The speaker is an employee of Pfizer Inc. Views and opinions expressed are the speaker’s own and do not
necessarily reflect those of the company.

What Are Value-Based Agreements?• Triple Aim/ Institute For Healthcare Improvement 2008
1. Improving the experience of care 2. Improving the health of populations3. Reduce per capita costs of health care
• Healthcare services• Move from a fee-for-service to a value-based contracts benchmarked
to outcomes and quality of care
• Pharmaceuticals• Looking beyond market-share or volume-based contracts• Insurer pays differential amounts for a drug based on how effective it is• Often value-based agreements = outcomes-based agreements

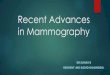
Impact of Oncology Treatments on Outcomes
• Cancer death rates have declined 22% since early 1990s
• Number of cancer survivors has increased from 3 million in 1970 to 14 million in 2014.
• 83% of survival gains in cancer are attributable to new treatments, including medicines
PhRMA, Medicines in Development for Cancer, Sept 2015

Number of Treatment Options over Time: 2006-2016
QuintilesIMS: Global Oncology Trends 2017, June 2017

Launched and Investigational Compounds for NSCLC
IMS: Oncology Trends 2015-2010, May 2016

Immuno-oncology and the promise of combination therapies
Jacob Plieth 7 Edwin Elmhirst, Evaluate: PD-1/ PD_L1 Combination Therapies, May 2017

Value Assessment of Oncology MedicinesOncology Drug Abacus NCCN Evidence Blocks
ASCO Value Framework Evidence Reports

Types of Value-Based Agreements for Pharmaceuticals
Price level or nature of reimbursement is tied to future metrics ultimately related to patient performance, outcomes, efficacy, tolerability, dosing, benefit, outcomes, quality of life, or clinical usage
Reimbursement decision in which approval is conditional on the collection of additional population level studies after launch (with provisional reimbursement) to support coverage or pricing
Price level or nature of reimbursement is based on financial considerations and is not related to clinical performance
DescriptionTerms
Performance-Based Agreements
Coverage with Evidence Development (CED)
Financial-Based Agreements
Price-volume agreementsTotal cost capNon-price discounts/ free goods
Examples
Outcomes guaranteeCompliance monitoringPattern or process of care
Centers for Medicare and Medicaid Services agreements around medical devices

Risk-Share Agreements in US
PhRMA: Barriers to value-Based Contracts for Innovative Medicines, March 2017

Challenges with implementing VBA in US
• Key laws implicated: • Medicaid Best Price• Average Sales Price reporting requirements in Medicare part B• 340B• Anti-kickback statutes

Additional Challenges Specific to Oncology
• Endpoints measured in clinical trials – PFS, OS, HR, CR, etc – not captured in medical claims data
• Patients treated with combination therapies or a combination of medicine and procedure (radiation, surgery) - difficult to attribute causality of outcome to 1 intervention
• Small numbers: > 200 tumor types with many sub-types
• Medically appropriate/ off-label use

Outcomes-Based Agreement in Oncology
Health Affairs Blog: http://healthaffairs.org.proxy1.athensams.net/blog/2017/04/03/overcoming-challenges-of-outcomes-based-contracting-for-pharmaceuticals-early-lessons-from-the-genentech-priority-health-pilot/

Genentech–Priority Health Outcomes-Based Pilot
• Avastin (bevacizumab) in patients with non–small-cell lung cancer
• Rebates tied to PFS, a key endpoint in the phase 3 RCT • The shorter the PFS in a given patient, the greater the rebate to
Priority Health. • If PFS > 6 months (median PFS from ph3 RCT), Priority Health
would not receive a rebate
• Measurement of PFS at the individual level • expedites data capture and increases the timeliness of rebates • methods for verifying PFS from claims, imaging, and EHR data.
• Rebates calculated for each patient
Health Affairs Blog: http://healthaffairs.org.proxy1.athensams.net/blog/2017/04/03/overcoming-challenges-of-outcomes-based-contracting-for-pharmaceuticals-early-lessons-from-the-genentech-priority-health-pilot/

How Do We Understand The Impact on The Patient?
Avalere Health: Patient Perspective Value Frameworkhttp://avalere.com/expertise/life-sciences/insights/avalere-health-and-fastercures-release-version-1.0-of-the-patient-perspecti

Summary
Innovation in oncology medicines is significant driver for survival gains for cancer patients
Oncology treatments are becoming more complex causing high variability in practice
Clinical guidelines are important foundation for value-based care
Providers, Patients and Payers all view value of oncology medicines differently
Outcomes-based agreements for oncology medicines are not very common as they are difficult to execute