Embed Size (px)
Citation preview

Recent structural and functional imaging findingsin schizophreniaMargaret A. Niznikiewicz, Marek Kubicki and Martha E. Shenton
Purpose of review
Schizophrenia is a severe mental disorder that affects nearly
1% of the general population and has long been a challenge for
both clinicians and researchers in terms of treatment and
etiology. More recently, evidence has amassed that suggests
that schizophrenia is a brain disorder, and that some aspects of
this disorder appear to be genetic. It has only been in the past
decade, however, that adequate neuroimaging tools have
become available to study brain abnormalities in schizophrenia.
These technologic advances have led to a much better
understanding of both structural and functional brain
abnormalities in schizophrenia, and allowed construction of
comprehensive theories regarding the neural underpinnings of
schizophrenia. The present review provides an account of
research activities in the fields of structural magnetic resonance
imaging (MRI), functional MRI, and diffusion tensor imaging
during the past year, dating from August 2001 to August 2002.
Recent findings
In the review we discuss MRI findings in chronic schizophrenia
and in first episode schizophrenia, and we include information
on family studies. We note that the two major hypotheses
regarding schizophrenia (neurodevelopmental and/or
neurodegenerative) provide a theoretical framework for most
studies. For the functional MRI studies, we note that questions
focus on identifying networks of brain regions that are abnormal
and contribute to functional abnormalities.
Summary
Jointly, MRI, functional MRI, and diffusion tensor imaging
research suggests that schizophrenia is a disorder that impacts
on several brain regions, leading most notably to abnormalities
in both frontal and temporal lobes, as well as to abnormal
connections between those two major structures.
Keywords
brain abnormalities, diffusion tensor imaging, functional
magnetic resonance imaging, neuroimaging, schizophrenia
Curr Opin Psychiatry 16:123–147. # 2003 Lippincott Williams & Wilkins.
Boston Veterans Affairs Healthcare System, Clinical Neuroscience Division,Laboratory of Neuroscience, Department of Psychiatry, Harvard Medical School,Boston, Massachusetts, USA
Correspondence to Margaret A. Niznikiewicz, PhD, Department of Psychiatry-116A,Boston VA Healthcare System, 940 Belmont Street, Brockton, MA 02301, USAFax: +1 508 580 0059; e-mail: [email protected]
Current Opinion in Psychiatry 2003, 16:123–147
Abbreviations
ACC anterior cingulate cortexCSP cavum septi pellucidiDLPFC dorsolateral prefrontal cortexDTI diffusion tensor imaging(f)MRI (functional) magnetic resonance imagingPTSD post-traumatic stress disorderSTG superior temporal gyrusVBM voxel-based morphometry
# 2003 Lippincott Williams & Wilkins0951-7367
IntroductionInterest in elucidating the structural and functional brain
abnormalities that occur in schizophrenia has a long
history, dating back to Kraepelin’s [1] and Bleuler’s [2]
early descriptions of schizophrenia. For Kraepelin, the
disorder, which he described as ‘dementia praecox’, or
early dementia, was defined primarily by the course or
outcome. For Bleuler the disorder was defined more by
the marked cognitive and emotional dysfunctions, and
by a split between emotions and cognition, or what he
described as ‘schizophrenia’. However, both of those
seminal thinkers believed that, ultimately, schizophrenia
would be linked to a brain disorder. Early work in this
field was thus particularly discouraging because there
were no tools available that allowed investigators to
discern subtle brain abnormalities. With the advent of
neuroimaging techniques, beginning with computer-
assisted tomography findings in 1976 [3] and the first
magnetic resonance imaging (MRI) scan of a schizo-
phrenic brain in 1984 [4], we now know more about
brain abnormalities in schizophrenia than at any other
time in the history of schizophrenia research.
In the present review we highlight important recent
structural and functional findings [i.e. MRI, functional
(f)MRI, and diffusion tensor imaging (DTI)] in schizo-
phrenia. Structurally, those findings suggest predomi-
nantly enlarged lateral ventricles and temporal lobe
abnormalities, but functionally, they suggest more
temporal–frontal connectivity abnormalities. We frame
these findings within the context of research findings
reported during the past 15 years. We highlight structural
MRI studies that address neurodevelopmental and/or
neuroprogressive hypotheses of brain abnormalities, and
functional studies that address specific hypotheses
regarding several domains of cognitive dysfunction in
schizophrenia. We end with a brief review of DTI
findings that demonstrate connectivity abnormalities in
DOI: 10.1097/01.yco.0000058610.61505.6b 123

schizophrenia, followed by a summary and discussion of
future directions in neuroimaging studies in schizophre-
nia.
It is increasingly recognized that schizophrenia is a
disease of the brain that profoundly affects most aspects
of human function. Although the exact nature of the
dysfunction and its etiology remain unknown, substan-
tial progress has been made in identifying brain
abnormalities in schizophrenia and in mapping abnormal
cognitive functions onto brain structures. One reason for
this progress is that the quality of in-vivo images using
MRI has increased dramatically over the past 15 years.
We are now able to acquire and evaluate 1 mm slices
through the entire brain, a spatial resolution that was
previously impossible [5..]. Advances in fMRI have also
made it possible to go beyond examining isolated brain
regions to examining interconnected neural networks
that are probably implicated in schizophrenia [6–9].
Additionally, the recent advent of DTI renders possible
the investigation of abnormal connectivity among brain
areas because it is well suited to examining white matter
in the brain (for review [10..]).
In this review we present the most recent findings in
schizophrenia from structural MRI, fMRI, and DTI
studies reported between 1 August 2001 and August
2002. We begin with a review of MRI structural findings
in chronic schizophrenia and in first episode schizo-
phrenia. This is then followed by a review of fMRI and
DTI findings in schizophrenia. We frame these recent
findings within the context of MRI findings over the past
15 years.
Magnetic resonance imaging: structuralfindings in chronic schizophreniaMagnetic resonance imaging has continued to provide
important information regarding the brain structure in
schizophrenia, with most studies motivated by a keen
interest in pursuing the possible causes of schizophrenia
and in identifying regions affected by the disease
process.
Overview and context
Two reviews of MRI structural findings in schizophrenia
have recently been published, one by Shenton et al. [5..]
and the other by Kasai et al. [11 .], that are quite
comprehensive. The review by Shenton et al. spans the
time period from 1988 to 2000, and reviews more than
190 MRI studies. In patients with schizophrenia, as
compared with normal control individuals, it documents
the following: lateral ventricular enlargement (80% of
studies); third ventricle enlargement (73% of studies);
medial temporal lobe volume reductions (74% of
studies), including amygdala, hippocampus, and para-
hippocampal gyrus; and neocortical superior temporal
gyrus (STG) volume reductions (100% of studies),
particularly on the left, with the percentage decreasing
to 67% of studies when STG gray and white matter are
combined. There is also moderate evidence for frontal
lobe volume reduction in schizophrenia (59% of studies),
particularly prefrontal and orbitofrontal regions, and
parietal lobe abnormalities (60% of studies), including
both supramarginal and angular gyri abnormalities; the
latter regions are important in language processing.
Finally, enlarged cavum septi pellucidi (CSP; 92% of
studies), basal ganglia abnormalities (68% of studies),
corpus callosum abnormalities (63% of studies), thalamus
abnormalities (42% of studies), and cerebellar abnorm-
alities (31% of studies) are also evident in schizophrenia.
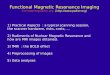
Figure 1 [12] provides a lateral view of the brain that
depicts the locations of the frontal, parietal, temporal,
and occipital lobes, as well as major gyri in the brain,
including STG.
Previous MRI findings thus highlight the importance of
temporal lobe abnormalities in schizophrenia. However,
this is not to suggest that the temporal lobe is the only
brain region that is abnormal in schizophrenia. In fact,
the temporal lobe is highly interconnected with other
brain regions, including the frontal lobe [13–19], and
normal brain function depends on such interconnectiv-
ity. In the present review of fMRI and DTI findings in
schizophrenia, the role of neural connectivity in schizo-
phrenia is further highlighted.
Neurodegenerative hypothesis
There are two prevailing hypotheses concerning the
etiology of brain abnormalities in schizophrenia: neuro-
developmental and neurodegenerative. Shenton et al.[5..], as well as Weinberger and McClure [20 .],
discussed the merits of these two theoretical approaches,
and a review paper by Okubo et al. [21] focused primarily
on evidence for progressive changes in schizophrenia.
Although these approaches are not described in detail
here, it is important to point out that neurodevelop-
mental and neurodegenerative approaches have a long
history in schizophrenia. They are often viewed as
mutually exclusive, but are increasingly recognized as
complementary [20.], with the suggestion that schizo-
phrenia (like many neurologic diseases) may be
characterized by both neurodevelopmental and neuro-
degenerative processes. Several, if not most, of the
studies discussed here adopt those two perspectives as
their theoretical anchor points.
Evidence for progressive changes in gray matter in
chronic schizophrenia has been reported in separate
studies conducted by Velakoulis et al. [22], Hulshoff etal. [23], and Convit et al. [24]. Velakoulis et al. [22]
used a voxel-based morphometry (VBM) approach to
Schizophrenia124

study gray matter changes across all brain regions, as a
function of illness duration. This approach offers a
quick way to evaluate multiple brain regions at once,
across many individuals. Negative correlations (unre-
lated to the age of onset) with illness duration were
found for right medial temporal, medial cerebellar and
bilateral anterior cingulate, and white matter volume in
the right posterior limb of the internal capsule. Positive
correlations were noted for globus pallidus (Table 1),
suggesting the role for medication in the latter
volumetric changes. Evidence for progressive changes
was also reported by Hulshoff et al. [23]. In their cross-
sectional study of gray and white matter changes in
159 schizophrenic patients and 158 normal control
individuals (Table 1), a steeper regression for gray
matter volume changes as a function of age was found
in the schizophrenia group.
These findings support an earlier, important longitudinal
study conducted by Mathalon et al. [43..]. In patients
with schizophrenia as compared with control individuals,
those investigators reported progressive volume decline
from baseline to rescan 4 years later both in frontal and
temporal gray matter, as well as expansions in sulci and
lateral ventricles. Moreover, Mathalon et al. observed
that cortical gray matter in these brain regions showed an
accelerated decline over time in those patients with the
most severe symptoms. These observations were inter-
preted as suggesting that a progressive pathologic
process is evident in at least some patients with
schizophrenia.
A different strategy was adopted by Convit et al. [24],
who parcellated the frontal lobes into subregions and
compared the volumes of the subregions between young
normal control individuals, old normal control indivi-
duals, and young schizophrenia patients (Table 1).
Patients with schizophrenia and older normal control
individuals both showed smaller volumes in the superior
frontal gyrus and orbitofrontal regions, suggesting that
both older control individuals and younger patients with
schizophrenia exhibit frontal lobe volume reduction as
compared with younger control individuals. However,
these similarities in volume reduction do not necessarily
suggest similar mechanisms. Moreover, differences in
education between groups may have also influenced the
findings.
In another study, Lawrie et al. [44] evaluated change
over time in magnetic resonance volume of the temporal
lobe and amygdala–hippocampal complex in control
individuals and in relatives of patients with schizophre-
nia (defined as being in a family in which there were at
least two first-degree or second-degree relatives diag-
nosed with schizophrenia; Table 2). Previous results
showed a reduction in the amygdala–hippocampal
complex at baseline in relatives of patients with
schizophrenia. A subset of those people was then
followed up over time, and results revealed no changes
in temporal lobe or in the amygdala–hippocampal
complex in relatives at risk for schizophrenia (i.e. volume
reductions noted at baseline were stable and did not
change over time). However, when psychotic relatives
Inf. frontalsulcus
Sup. frontal sulcus
Percentral sulcus
Central sulcus Postcentral sulcus
Sup. parietal lobule
Intraparietal sulcus
Inf. parietal lobule
Parieto-occipitalsulcus
Preoccipital notch
Horizontal fissure
Medulla oblongataLateral sulcus
Orbital gyri
Figure 1. Lateral view of the human brain
From Carpenter and Sutin [12]; reprinted withpermission from Williams & Wilkins, New York,USA. Inf., inferior; Sup., superior.
Structural and functional imaging in schizophrenia Niznikiewicz et al. 125

Table 1. Magnetic resonance imaging structural findings in chronic schizophrenia
ReferenceMagnet/slicethickness
Participants(n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Ananth [25..] 2 Tesla/1.5 mm(contiguous)
SZ 20NC 20
SZ 37.8NC 38.6
SZ 10/10NC 10/10
Voxel-based morphometry was used to measure globaland regional gray matter. Global gray matter differenceswere observed, but more importantly regional graymatter differences were observed, particularly in the leftmediodorsal thalamus. Other differences betweengroups involved the occipitoparietal cortex; premotor,medial, and orbital prefrontal cortices; and inferolateraltemporal lobe. White matter differences were observedbetween groups in the lateral optic radiation of theoccipital cortex. Of note, abnormalities in ventral andmedial prefrontal cortices correlated with a positivefamily history of SZ. There was no proportionalreduction in gray matter with age in SZ.
Chemerinski[26]
1.5 Tesla/1.5 mmand 3–4 mm(contiguous)
SZ 45NC 45
SZ 30.0NC 30.5
Males only Total cerebral gray matter and total cerebral surfacearea, as well as ventral frontal cortex (comprised oforbitofrontal and straight gyrus) were measured. Find-ings showed no group differences for total cerebral graymatter, total cerebral surface area, or ventral frontalcortex or orbitofrontal cortex, but right straight gyrusshowed smaller volume and shape in SZ. The volume ofventral frontal cortex was negatively correlated withsocial dysfunction in SZ.
Chow [27.] 1.5 Tesla/1.5 mm(contiguous)
SZ 14NC 14(Note: 22q11deletionsyndromeand SZ)
SZ 27.5NC 28.2
SZ 7/7NC 7/7
Total gray and white matter, lateral ventricles, as well asfrontal, temporal, and parietal gray and white matterwere measured. Findings showed that total gray matter,and frontal, temporal and left parietal lobe gray matterwere significantly reduced in SZ. This was mostprominent in the frontal and temporal lobes. There wasalso an observed increase in the lateral ventricles in SZ.
Convit [24] 1.5 Tesla/1.2 mm(contiguous)
SZ 9NC young 9NC old 9
SZ 35NC young37.4NC old 69.8
Males only Smaller volumes of superior and orbital frontal gyri wereobserved in both old NC and in SZ as compared withyounger NC. Old NC and SZ thus did not differ. Thissuggests similarities between the SZ and aging NC infrontal lobe abnormalities. (There were both age andeducation differences between groups).
Erbagci [28] 1.0 Tesla/3 mm(5-mm interslicegap)
SZ 26NC 29
SZ 34.7NC 28.6
SZ 11/15NC 11/18
Third ventricle and adhesio interthalamica were mea-sured. Results showed that the adhesio interthalamicawas more often absent in SZ than in NC. Third ventriclewas not correlated with presence or absence of adhesiointerthalamica, as predicted.
Falkai [29] 1.5 Tesla/1.2 mm(contiguous)
SZ(MA) 14SZ(U) 12NC 10
SZ(MA) 33.6SZ(U) 29.8NC 24.4(NC wereyounger)
SZ(MA) 8/6SZ(U) 8/4NC 5/5
Sylvian fissure and amygdala–hippocampal complexwere measured. Results showed that amygdala–hippo-campus volume was reduced, and there was anabnormal asymmetry in SZ(U). Sylvian fissure did notshow differences among groups. The authors sug-gested that brain abnormalities involving medial tem-poral lobe structures are not familial.
Goldstein[30..]
1.5 Tesla/3.1 mm(contiguous)
SZ 40NC 48
SZ male 46.6SZ female41.4NC male 41.6NC female39.0
SZ 27/13NC 27/13
22 regions of interest were evaluated. Relative to maleNC, male SZ were characterized by reductions infrontomedial cortex, middle frontal cortex, cingulate gyri,paracingulate gyri, Heschl’s gyrus, and Broca’s area,but with increased volume in posterior cingulate andbasal forebrain. Planum temporale was also smaller onthe right in male SZ, but larger on the right in female SZ.Relative to female NC, female SZ were characterized byreductions in fronto-orbital gyri, basal forebrain, anteriorcingulate gyri, and posterior supramarginal gyri, butexhibited increases in volume in cingulate gyri and rightplanum temporale. No differences were noted forsubcortical gray matter or for CSF.
Hagino [31] 1.5 Tesla/1 mm(contiguous)
SZ 86NC 79
SZ 29.3NC 24
SZ 46/40NC 44/35
Cavum septum pellucidum (the membrane separatingthe lateral ventricles) was measured. Findings showedno group differences in the prevalence of large cavumseptum pellucidi (74.4% in SZ; 74.7% in NC), andthere were also no sex-mediated differences. Suchlarge cavum in NC is unusual, with most other studiesreporting prevalence between 5 and 13%.
(continued opposite )
Schizophrenia126

Table 1. (continued )
ReferenceMagnet/slicethickness
Participants(n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Hulshoff [23] 1.5 Tesla/1.2 and1.6 mm (contigu-ous)
SZ 159NC 158
SZ 35.6NC 37.7(Age range16.3–76.9)
SZ 112/47NC 106/52
Total volume of cerebral and cereballar gray and whitematter, and lateral and third ventricles were measured.Total brain volume, total cerebral gray matter, and bothprefrontal gray and white matter were reduced in SZ,and lateral ventricles and third ventricles were increasedin SZ. Results also showed steeper regression slopesfor age and gray matter volume in SZ as compared withNC.
Meisenzahl[32]
1.5 Tesla/3 mm(contiguous)
SZ 30NC 30
SZ 29.4NC 29.1
Males only 3-mm slices were reformatted and resliced into 1.5-mm.Planum temporale was measured. No volumetric orasymmetry differences were observed, regardless ofplanum temporale definitions used.
Meisenzahl[33]
1.5 Tesla/3 mm(contiguous)
SZ 44NC 48
SZ 30.2NC 30.3
Males only 3-mm slices were reformatted and resliced into 1.5-mm.Bifrontal temporal gray matter volume and generalizedwhite matter volume deficits associated with allele 2carriers.
Okugawa [34] 1.5 Tesla/1.5 mm(contiguous)
SZ 32NC 32
SZ 39.3NC 38.6
Males only Gray matter, white matter, and CSF were measured inthe frontal, temporal, parietal, and occipital lobes.Results showed gray and white matter reduction in thetemporal region in SZ, as well as white matter reductionthat was more widespread, and increased CSF inwhole brain and in the frontal and temporal lobes in SZ.
Rajarethinam[35]
1.5 Tesla/3 mm(contiguous)
SZ 20NC 20
SZ 33.5NC 33.9
Males only The amygdala–hippocampus complex (both amygdalaand hippocampus) was evaluated on 1-mm reformatted3-mm slices. Results showed no group differences forthe amygdala–hippocampal complex, but negativecorrelations were observed between left amygdala andthought disorder, between left hippocampus andnegative symptoms, and between left anterior andposterior hippocampus and both negative and positivesymptoms in SZ.
Suzuki [36.] 1.5 Tesla/1 mm(contiguous)
SZ 45NC 42
SZ 26.4NC 26.1
SZ 23/22NC 22/20
A new method, adapted from fMRI, namely statisticalprobability mapping (SPM), was used to measure graymatter and white matter of the brain.Gray matter in males: gray matter was decreased in leftsuperior temporal and middle frontal gyrus, and bilateralanterior cingulate gyrus. Gray matter in females: graymatter was decreased in right anterior cingulate gyrus,the medial part of the right superior frontal gyrus, andright middle frontal gyrus. Gray matter was increased inright precuneus, postcentral gyrus, left cuneus andprecuneus, and right cerebellumWhite matter: both males and females exhibiteddecreases in the bilateral anterior limb of the internalcapsule and superior occipitofrontal fasciculus.Females also exhibited increased bilateral parietallobes.
Takahashi [37] 1.5 Tesla/1 mm(contiguous)
SZ 40NC 40
SZ: male 26.4;female 25.9NC male 25.5;female 24.8
SZ 20/20NC 20/20
The volume of whole brain gray and white matter, andanterior cingulate gray and white matter was evaluated.Results showed that right anterior cingulate (ACG) graymatter is reduced in female SZ, and there is a lack ofright4left asymmetry in female SZ. ACG white matterin female SZ also lacked normal right4left asymmetry.
Velakoulis [22] 1.5 Tesla/3 mm(contiguous)
SZ 39(Illness dura-tion: 2–31years)
SZ 36(Range19–60)
34/5 Voxel-based morphometry was used to measuretemporal, cingulate, and cerebellar abnormalities.Findings showed that right medial temporal, cerebellar,and bilateral anterior cingulate gray matter volumescorrelated negatively with illness duration, and rightglobus pallidus volume correlated positively with illnessduration.
Velakoulis [38] 1.5 Tesla/1.5 mm(contiguous)
SZ 45NC 139
SZ 34.1NC 30.05
87.7%/59.% Both two-dimensional measure of shape (volume loss inthe head of the hippocampus) and volume distinguishedbetween the two groups.
Wang [39.] 1.5 Tesla/1.25 mm(contiguous)
SZ 15NC 15
SZ 32.9NC 30.9
Males only Principal components analysis based on left–rightasymmetry vector fields was used; group differenceswere reported in the subiculum.
(continued overleaf )
Structural and functional imaging in schizophrenia Niznikiewicz et al. 127

were examined separately, there was a reduction in
temporal lobe volume over time. Lawrie et al. suggested
that there are abnormalities in temporal lobe structures
in relatives at risk for schizophrenia, but that no changes
occur in those structures over time; In contrast, such
changes are seen in individuals who develop psychotic
features, further suggesting that changes over time are
observed only when psychosis is evident.
One negative finding among reports of progressive
changes was reported by Ananth et al. [25 ..], who did
not find proportional gray matter reduction with age in
patients with schizophrenia. However, they did report
left mediodorsal thalamus abnormalities using VBM, as
well as differences in occipitoparietal cortex, premotor,
medial, orbital prefrontal cortices, and inferolateral
temporal lobe in patients with schizophrenia as com-
pared with control individuals (Table 1). VBM is a
relatively new and promising technique, but it needs
further refinement, including comparison with manual
measurements of brain regions of interest (which are the
standard for comparison), before it can widely be
accepted as an accurate measure of brain regions of
interest.
Neurodevelopmental hypothesis
Support for a neurodevelopmental origin of schizophre-
nia is often sought by studying brain structures in which
perinatal maturation coincides with increased risk for
schizophrenia (i.e. second and third trimester). These
include midline structures that are proposed to mediate
attention and information processing [57], including CSP
(two thin leaflets that fuse together as the corpus
callosum and hippocampus develop; for more extensive
review [5..]). Other midline structures include the
adhesio interthalamica (single or multiple connections
between the medial surfaces of the two thalami), the
corpus callosum, and the hippocampus. Finally, other
structures that may be affected by adverse perinatal
event(s) include: the sulcal–gyral pattern of the brain, as
well as regions of the brain that are lateralized for
specialized functions such as language, including STG
and a component of that gyrus, namely the planum
temporale (for review [5..]).
Midline structures
Evidence emerging from studies of midline structures
suggests subtle neurodevelopmental abnormalities af-
fecting these brain areas. Erbagci et al. [28], for example,
examined the adhesio interthalamica to determine
whether they were present or absent (abnormal) in
schizophrenia. They found adhesio interthalamica to be
absent more often in patients with schizophrenia than in
normal control subject individuals, suggesting a neuro-
developmental abnormality in at least a subset of
patients diagnosed with schizophrenia (Table 1).
Hagino et al. [31] examined CSP, another brain anomaly
that is believed to be neurodevelopmental in origin.
They did not find group differences in the prevalence
of large CSP in a group of 86 schizophrenia patients
and 79 normal control individuals. However, this
finding is not consistent with 92% of studies showing
enlarged CSP in patients with schizophrenia (for review
[5 ..]). Moreover, those investigators reported that
74.7% of control individuals showed abnormal CSP.
This figure is much higher than the range 5–13% that
was generally reported for control individuals in
previous studies.
Narr et al. [47] examined the genetic contributions to
altered shape of the corpus callosum in a study of
dizygotic and monozygotic twins discordant for schizo-
phrenia (Table 2). No group volume differences were
found between affected and nonaffected individuals, but
both affected and unaffected monozygotic twins shared
an upward bowing of the callosum, which is suggestive
of volumetric enlargement of the ventricles and is
consistent with genetic rather than environmental
influences on corpus callosum anatomy.
Table 1. (continued )
ReferenceMagnet/slicethickness
Participants(n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Wible [40] 1.5 Tesla/1.5 mm(contiguous)
SZ 17NC 17
SZ 44NC 40
Males only No group differences were observed for prefrontal graymatter, but right prefrontal white matter was reduced inSZ and this was also correlated with right hippocampalvolume.
Zuffante [41] 1.5 Tesla/1.25 mm(contiguous)
SZ 23NC 23
SZ 43.3NC 46.5
Males only No group differences were observed between groupsfor volume of area 46 (middle frontal gyrus), althoughdeficits were noted in SZ in both spatial and nonspatialworking memory tasks.
Yucel [42] 1.5 Tesla/1.5 mm(contiguous)
SZ 55NC 75
SZ 35.99NC 29.08
Males only Reduced folding of the left anterior cingulate cortex wasfound in SZ.
CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; NC, normal control; SZ, chronic schizophrenia; SZ(MA), multiply affected family (in whichthere is more than one member with SZ); SZ(U), uni-affected family (in which only one member is diagnosed with SZ).
Schizophrenia128

Table 2. Magnetic resonance imaging structural findings in childhood/adolescent onset schizophrenia or in relatives of patients diagnosedwith schizophrenia
ReferenceMagnet/slicethickness
Participants(n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Relatives of SZ
Cannon [45.] 1.5 Tesla/5 mm(contiguous)
SZ 64SZSIBS 51NC 54
SZ 40.5SZSIBS 40.3NC 40.7(SZ = SZ orSZAFF;SZSIBS = SZor SZAFFSIB)
SZ 32/32SZSIBS 22/29NC 23/31
FH predicted gray matter volume loss in the patient andsibling groups, most strongly in the temporal lobe. Anincrease in CSF and sulcal enlargement was associatedwith hypoxia in patients only, whereas FH and sulcalenlargement in the temporal lobe were observed insiblings only. The authors concluded that FH wasassociated with increased brain abnormalities in SZ andin their nonpsychotic siblings, but not in NC.
Harris [46] 1.5 Tesla/1.5 or1.7 mm (contigu-ous)
SZ 6UP 12NC 6
SZ 38UP 69NC 38
SZ 5/1UP: positive history4/2; negativehistory 2/4NC 5/1
Whole brain and hippocampus were measured. Resultsshowed that positive history parents had a largerhippocampus volume than did SZ. The authorsspeculated that positive history parents have somecompensatory mechanisms or protective factors thatresult in larger hippocampi than in their affectedchildren.
Lawrie [44] 1.0 Tesla/1.88 mm(contiguous)
RELSZ 66NC 20
RELSZ 23.1NC 22.9(RELSZ = atleast two 1stor 2nd degreerelatives withSZ)
RELSZ 34/32NC 13/7
Previously these investigators reported reducedamygdala–hippocampal complex volume in people atrisk for SZ. In this study, a subset of these patients,along with healthy NC, were rescanned on average 2years later. Results showed that there was not areduction in temporal lobe and amygdala–hippocampalcomplex over time for all high-risk relatives. Instead,there was volume reduction in the right temporal lobe inhigh-risk individuals with psychotic features. This findingsuggests that brain structures may change over timewith psychotic symptoms, but may remain stable (i.e.reduced but no progression) in individuals at risk for SZwho do not evince psychotic symptoms.
Narr [47] 1.0 Tesla/1.2 mm(contiguous)
Discordantcotwins: MZ20; DZ 20Control cot-wins: MZ 20;DZ 20
Discordantcotwins: MZ48.3; DZ 49Control cot-wins: MZ 48.3;DZ 47.9
Discordant cotwins:MZ 10/10;DZ 10/10Control cotwins:MZ 10/10;DZ 10/10
Lateral ventricle and third ventricle volume wereevaluated, as well as corpus callosum area and verticaldisplacement (upward bowing). Results showed thatboth affected and unaffected MZ cotwins hadsignificant callosal displacements. There were nodifferences among groups in corpus callosum areameasures. Of note, lateral and third ventricle volumewere associated with corpus callosum displacement.The authors suggested that upward bowing of thecorpus callosum may be a useful developmental markerfor screening for SZ.
O’Driscoll[48.]
1.5 Tesla/1 mm(contiguous)
RELSZ 20NC 14
RELSZ 35.4NC 36.2
RELSZ 9/11NC 5/ 9
Amygdala–anterior hippocampus and posteriorhippocampus were evaluated. Results showed reducedvolume of amydgala–anterior hippocampal volume aswell as poor delayed verbal memory in RELSZ ascompared with NC. Across all participants there was acorrelation between delayed verbal memory andamygdala–anterior hippocampus. The data provide anempiric link between verbal memory deficits andvolumetric abnormalities in the amygdala–anteriorhippocampus in RELSZ.
Seidman[49..]
1.5 Tesla/3 mm(contiguous)
RELSZ 45SZ 18NC 48(RELSZ =families withone or two1st degreerelatives withSZ)
RELSZ 44.6SZ 43.2NC 40.1(Group differ-ences in sex,education, andIQ)
RELSZ 17/28SZ 10/8NC 27/21
Volumes of total cerebrum and of hippocampi weremeasured. Results showed significantly smaller lefthippocampus volumes in RELSZ, particularly formultiplex families (i.e. those with more than one personwith SZ), but no differences were found in hippocampalvolumes between SZ and their relatives. Additionally,verbal memory and left hippocampal volume werepositively correlated, particularly in the multiplex RELSZ.The authors suggested that reduced hippocampalvolumes and verbal declarative memory deficits reflect avulnerability to SZ.
(continued overleaf )
Structural and functional imaging in schizophrenia Niznikiewicz et al. 129

Table 2. (continued )
ReferenceMagnet/slicethickness
Participants(n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Steel [50] 1.0 Tesla/1.5 mm(contiguous)Some sectionstested onanother 1.0 Teslascanner/1.5 mm(contiguous)
6 sibships(n = 18)[SIBSHIP = 1patient withSZ, oneobligate carrier(inheritedgenetic risk, noSZ), one non-carrier and noSZ]
SZ sibships46.2Obligate 49Noncarrier45.2
7/11 Whole brain, prefrontal and temporal lobes, caudate,lentiform and thalamic nuclei, as well as amygdala–hippocampal complex, lateral, third and fourth ventricleswere measured. Results showed overall reduction incortical gray matter in SZ siblings (5%) withpronounced loss in the amygdala–hippocampus (12%).Obligate carriers were similar to SZ siblings in exhibitingamygdala–hippocampal complex volume reduction, andwere similar to unaffected noncarriers in exhibitingwhole brain gray matter volume reduction. Obligatecarriers had smaller ventricles than did SZ siblings. Theauthors concluded that reduced cortical gray matterwas associated with phenotypic SZ, whereasreductions in medial temporal lobe structures such asthe amygdala–hippocampus were associated with agenetic risk for SZ.
Van Erp [51.] 1.5 Tesla/1.3 mm(contiguous)
SZ 72 (60 SZ/12 SZAFF)US 58NC 53
SZ 40.2US 40.7NC 40.9
Males only Hippocampus was measured and smaller hippocampusvolume was found in SZ with FH, followed by SZwithout hypoxia, their siblings, and NC. There was noassociation between hypoxia and hippocampal volumein NC. Of note, smaller hippocampus correlated withearlier age of onset in SZ.
Childhood/adolescent onset of SZ
James [52] 1.5 Tesla/5 mm(contiguous)
AOSZ 16NC 16
AOSZ 16.6NC 16.0(Mean age atbaseline MRIscan differedbetweengroups)
AOSZ 9/7NC 9/7
Whole brain, lateral ventricles, third ventricle, temporallobe, and medial temporal lobe structures (amygdalaand hippocampus) were measured in adolescents withSZ and in NC. SZ had follow-up scans on average 2.7years later, and NC had follow-up scans on average 1.7years later. Results showed generalized ventricularenlargement (lateral and third ventricle), particularly inmale SZ, which was most prominent on the left, as wellas left amygdala volume reduction in SZ, and a trendtoward left hippocampal volume reduction in SZ. Therewas no progression of tissue loss in brain volumes or inlateral and third ventricular volumes over time.
Levitt [53] 1.5 Tesla/1.4 mm(contiguous)
COSZ 13NC 20
COSZ 14.2NC 12.0 (IQdifferencesbetweenCOSZand NC)
Children Total brain, temporal lobe volume, amygdala, andhippocampus volume were measured. Results showedthat amygdala volume, especially on the left, was largerin the COSZ group than in NC. There was also a trendfinding for a reversal of the normal right4left amygdalaasymmetry in COSZ.
Matsumoto[54]
1.5 Tesla/1.5 mm(contiguous)
AOSZ 40NC 40
AOSZ 15.5NC 15.7
AOSZ 20/20NC 20/20
Total gray and white matter of the superior temporalgyrus was measured in early onset SZ. Total brainvolume was also measured. Results showed that totalgray and white matter volume of the right superiortemporal gyrus was smaller in AOSZ than in NC.Bilateral volumes in AOSZ were correlated with age atonset of psychosis, whereas severity of thoughtdisorder and hallucinations were inversely related toright superior temporal gyrus volume. The authorssuggested that these findings may reflect aneurodevelopmental disruption.
Thompson[55..]
1.5 Tesla/1.5 mm(contiguous)
COSZ 12NC 12
COSZ 13.9NC 13.5(Onset byage 12)
COSZ 6/6NC 6/6
This study followed individuals over 5 years with threeseparate MRI scans. Results showed that deficitsprogress from parietal areas, to temporal lobes, andsensorimotor and dorsolateral prefrontal cortices inpatients with COSZ.
(continued overleaf )
Schizophrenia130

Amygdala–hippocampal complex
Three recent studies examined the amygdala–hippo-
campal complex in schizophrenia. Velakoulis et al. [38]
used both traditional volumetric measures and shape
measures to evaluate the hippocampus in schizophrenia.
Both shape-based and volume-based analyses suggested
reduced hippocampal volume in the patient group.
Specifically, the shape-based analysis indicated volu-
metric loss in the posterior portion of the hippocampus
(Table 1). Those researchers suggested that abnormal
receptor distribution in early development could lead to
altered hippocampal development in terms both of
shape and connectivity. Figure 2 provides MRI images
that depict the amygdala–hippocampal complex, as well
as the temporal lobe, frontal lobe, lateral ventricles, and
STG.
Although amygdala and hippocampal volume reductions
in schizophrenia are among the more robust findings, not
all studies report volume reductions. For example, in a
recent study conducted by Rajarethinam et al. [35], no
group differences were found in hippocampus and
amygdala volumes, although left amygdala volume
correlated negatively with the severity of thought
disorder in the patient group, and left hippocampal
volume was correlated with negative symptoms in the
patient group. Of note, in that study 3-mm slices were
used, as compared with use of 1.5-mm slices by
Velakoulis et al. [38]. This difference in spatial resolution
may explain the negative finding because differences in
spatial resolution can adversely effect the ability to
detect differences between groups. Of further note, that
reductions in left amygdala volume were correlated with
increased formal thought disorder confirms several
earlier studies that showed similar correlations (for
review [5..]).
Falkai et al. [29] were interested in evaluating families in
which only the proband had schizophrenia versus
families in which multiple family members were affected
with schizophrenia. They found more reduction as well
as abnormal asymmetry in the amygdala–hippocampal
complex in families in which only the proband was
diagnosed with schizophrenia, as compared with control
individuals and with probands from families with mul-
tiple diagnoses of schizophrenia. Those investigators
interpreted this finding as suggesting that brain abnorm-
alities in medial temporal lobe regions are not familial.
The question of how genetic transmission might impact
on reduction in hippocampal volume was also addressed
in a familial MRI study conducted by Harris et al. [46].
Hippocampal volumes were studied in patients with
schizophrenia, in their parents (families in which only
one parent had an ancestral history of schizophrenia),
and in normal control individuals. Unaffected parents
with an ancestral history of schizophrenia had larger
hippocampal volumes than did their affected offspring
(Table 2). Those authors concluded that reduced
hippocampal volume is not a genetically transmitted
risk factor. In addition, the unaffected parents with
ancestral history of schizophrenia had the largest
hippocampal volumes among the three groups, suggest-
ing that such increases in volume may represent a
protective or compensatory factor in a person at genetic
risk for schizophrenia. Of note, however, the proportion
of males and females in the positive and negative history
groups and in the control group was not equal, and this
in itself might have affected the findings.
The findings reported by Harris et al. [46] are not
consistent with findings from a study conducted by
Seidman et al. [49..]. Those investigators examined
Table 2. (continued )
ReferenceMagnet/slicethickness
Participants(n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Other
McCreadie[56]
0.5 Tesla/3 mm(contiguous)
SZDYS 31SZNDYS 31NC 31
SZDYS 43SZNDYS 44NC 43(Nevermedicated SZfrom SouthIndia, with andwithout DYS)
SZDYS 18/13SZNDYS 18/13NC 18/13
Cerebral hemisphere and lateral ventricles were mea-sured on two contiguous slices. Caudate and lentiformnucleus were measured. Results showed that leftlentiform gyrus was larger in SZDYS whereas rightventricle : hemisphere ratio was larger in SZNDYS thanin NC. When volume of lentiform nucleus was correctedfor hemisphere in a smaller group of patients, volumedifferences between groups were not present. Theauthors suggested that SZDYS may have striatalpathology that may represent a subset of SZ.
AOSZ, adolescent onset schizophrenia; COSZ, childhood onset schizophrenia; CSF, cerebrospinal fluid; DYS, dyskinesia; DZ, dyzygotic twin; FH,fetal hypoxia; IQ, intelligence quotient; MRI, magnetic resonance imaging; MZ, monozygotic twin; NC, normal control; RELSZ, relative ofschizophrenia; SZ, schizophrenia; SZAFF, schizoaffective disorder; SZDYS, schizophrenia with dyskinesia; SZNDYS, schizophrenia withoutdyskinesia; UP, unaffected parents; US, unaffected siblings.
Structural and functional imaging in schizophrenia Niznikiewicz et al. 131

hippocampal volume as a marker of vulnerability for
schizophrenia in both simplex (one person in the family
with schizophrenia) and multiplex (two people in the
family with schizophrenia) unaffected relatives of
schizophrenic patients, patients with schizophrenia, and
normal control individuals (Table 2). Using this genetic
sampling approach, left hippocampus was found to be
reduced in the unaffected relatives, especially those
from the multiplex families. Moreover, the volume
found in the unaffected relatives was not significantly
different from that found in patients with schizophrenia.
Seidman et al. also reported a correlation between
deficits in verbal memory performance and reduced left
hippocampal volume. This association is similar to that
reported in previous structural MRI studies (for review
[5..]) and to that reported by O’Driscoll et al. [48.], who
found reduced anterior amygdala–hippocampus in rela-
tives of patients with schizophrenia as compared with
control individuals, which was correlated with impair-
ments in verbal memory. These data thus provide an
empiric link between verbal memory deficits and brain
abnormalities in the amygdala–hippocampal complex
both in schizophrenia and in relatives of patients with
schizophrenia.
Similar findings were also reported by Van Erp et al.[51 .]. They found the smallest hippocampal volume in
patients with schizophrenia, followed by their full
siblings, and normal control individuals. In addition,
the smallest hippocampal volumes were observed in
schizophrenic patients with fetal hypoxia, a relationship
not noted in any other group.
The effect of fetal hypoxia on cortical gray matter loss
and on volume of cerebrospinal fluid was also assessed
in a study conducted by Cannon et al. [45 .] in a group
of patients with schizophrenia, full siblings of schizo-
phrenic patients, and matched normal control indivi-
duals (Table 2). Fetal hypoxia predicted reductions in
gray matter volume and increased levels of cerebro-
spinal fluid in patients and their siblings, but not in
control individuals. Of note, hypoxia did not correlate
with white matter changes in any group. These findings
point to a scenario in which genetic vulnerability and
environmental factors may interact in the development
of schizophrenia, because brain regions particularly
vulnerable to hypoxia, such as the hippocampus, were
especially impacted in at least a subset of patients
diagnosed with schizophrenia.
Finally, Steel et al. [50] compared volumes of specific
brain regions, including the amygdala–hippocampal
complex, in sibships with either one patient with
schizophrenia, one obligate carrier without the disorder
but with affected offspring, and one nonaffected
‘noncarrier’. Obligate carriers shared reduced amygda-
la–hippocampal volumes with schizophrenic patients,
but not the whole brain, or frontal or temporal lobe
reductions found in schizophrenic patients. Those
findings suggest that reduced cortical structures are
associated with the phenotype of schizophrenia, whereas
the reduction in the amygdala–hippocampal complex is
associated with genetic risk for schizophrenia in the
absence of the disorder. Of note in this regard, a recent
twin study was conducted in post-traumatic stress
Figure 2. Coronal 1.5 mm view of the brain
Coronal view
Right Left
Sagittal view
Anterior Posterior
Sagittal view
Front Back
Frontallobe
Lateralventricle
Superiortenporalgyrus
Amygdala-hippocampalcomplex
Temporallobe
Coronal 1.5 mm view of the brain shows the temporal lobe, frontal lobe,superior temporal gyrus, amygdala–hippocampal complex, and thelateral ventricles. The location of the coronal slice is depicted in thesagittal view. (Courtesy of Susan Demeo, Magdalena Hale Spencer,and Anders Brun.)
Schizophrenia132

disorder (PTSD) monozygotic twins discordant for
PTSD [58]. It found that the unaffected twin also
showed reduced amygdala–hippocampal volume as
compared with monozygotic twins without PTSD,
suggesting that such volume reduction may reflect a
genetic vulnerability or predisposition to PTSD.
Cortical and subcortical sex differences
The role of sex differences in mediating gene expres-
sion in schizophrenia was examined by Goldstein et al.[30 ..]. They assessed a range of cortical and subcortical
brain volumes, and hypothesized that sex-mediated
brain differences in men and women with schizophrenia
are present in cortical but not in subcortical regions.
Indeed, differential patterns of cortical brain abnormal-
ities were found in schizophrenic men and women
relative to their control groups (Table 1). No sex
differences were found in asymmetry, with the excep-
tion of the planum temporale, in which male patients
exhibited smaller planum temporale on the right and
female patients showed larger planum temporale on the
right, resulting in greater planum temporale symmetry
in women. This finding is not consistent with that of
Meisenzahl et al. [32], who reported no asymmetry
differences in males using three different methods of
planum temporale definition. As expected, however,
Goldstein et al. found no sex-mediated group differ-
ences in subcortical regions, despite normally existing
sex dimorphisms in these areas. The authors inter-
preted their findings as supporting the role of
neurodevelopmental factors in schizophrenia, especially
because they relate to timing of the release of gonadal
hormones and their relative distribution between
cortical and subcortical brain regions.
Cingulate cortex and schizophrenia
The anterior cingulate cortex (ACC) was examined in
three studies. Yucel et al. [42] studied the morphology of
the ACC in a group of 55 male patients and 75 normal
control individuals. The surface morphology of the ACC
was used to classify paracingulate sulcus either as
prominent, present, or absent. The results suggest that
patients had less leftward folding of the anterior
cingulate than did control individuals, and these
differences existed over and above those found in the
entire left hemisphere. The results were viewed as
supporting evidence for the role of neurodevelopmental
factors in the etiology of schizophrenia because cortical
folding is established in the second and third trimesters
of pregnancy, remains stable throughout life, and is not
influenced by environmental factors such as alcohol
abuse, neuroleptic exposure, or age.
In contrast to Yucel et al. [42], two other studies [30..,37]
found group differences in ACC to be sex related (i.e.,
observed only in women). Additionally, Takahashi et al.
[37] found reduced gray and white matter in the ACC,
along with reduced asymmetry in women, in a study that
examined ACC gray and white matter using high-
resolution three dimensional MRI.
Frontal cortex and schizophrenia
Three studies evaluated the role of frontal cortex in
schizophrenia. In the first of those, Chemerinski et al.[26] looked at the relationship between social function in
male patients with schizophrenia and the morphology of
the ventral frontal cortex, parcellated into orbitofrontal
gyrus and straight gyrus. Both volume and surface
measures were completed (Table 1). Only the volume
of the straight gyrus was found to be smaller in the
patient group and, in agreement with the study
hypothesis, was correlated with measures of social
adjustment, both before and after illness onset. This
relationship became especially clear when negative
symptoms were controlled for, suggesting that negative
symptomatology and poor social function may represent
two distinct features of the illness. These data are
consistent with previous findings suggesting that pre-
morbid functioning, particularly poor premorbid social
functioning, may be related to more frontal lobe
abnormalities in schizophrenia (for review [5..]).
In the second study, Wible et al. [40] analyzed the
relative volumes of gray and white matter of the
prefrontal cortex and its correlations with clinical
variables. Although no differences were found in gray
matter, white matter was reduced in the right hemi-
sphere in the patient group, and it correlated with
volume of the right hippocampus in the patients only.
Also, patients with high negative symptom scores had
lower white matter volumes than did those with low
negative scores. The fact that the patients in the study
were characterized by more negative symptoms suggests
the importance of evaluating more homogeneous patient
groups, because this may make a large difference with
respect to which brain regions are most affected.
Differences in genetic loading may also be important
because there is some indication that patients with more
negative symptoms may have more neurodevelopmental
abnormalities and an earlier age of onset (for review
[5 ..]).
Finally, in the third study, that conducted by Zuffante etal. [41], a lack of volumetric changes in the frontal lobes
(area 46) was noted, despite the presence of deficits on
tasks of both spatial and nonspatial working memory.
Schizophrenia and gene expression
More direct studies of genetic factors that might be
associated with schizophrenia include those by Chow etal. [27 .] and Meisenzahl et al. [33]. The latter
investigators [33] examined the relationship between
Structural and functional imaging in schizophrenia Niznikiewicz et al. 133

brain volumetric measures and individual genotypes.
Specifically, because higher plasma levels of interleukin-
1b are found in blood samples of schizophrenic patients,
they examined the relationship between interleukin-1ballele 2 carriers and volumetric brain abnormalities.
Schizophrenic patients who were carriers had smaller
volumes in the frontal and temporal gray matter and a
generalized deficit in white matter volume. There was
no association between the interleukin-1b polymorphism
at position –511 and schizophrenia.
Chow et al. [27.], in a preliminary study of 14 adults with
schizophrenia who also suffered from 22q deletion
syndrome (a disorder associated with increased risk for
schizophrenia) and 14 age-matched and sex-matched
control individuals, found that the patient group
exhibited smaller total gray matter volumes in the
temporal and frontal lobes. White matter did not show
volumetric differences between groups.
Taken together, these results suggest a scenario of how
genetically mediated risk for schizophrenia might inter-
act with other genetic and environmental vulnerability
factors to result in schizophrenia.
Summary
MRI structural findings in schizophrenia over the past
year are generally in agreement with previous structural
MRI findings in schizophrenia. Multiple brain regions
appear to be affected in schizophrenia, although rather
than generalized deficits these abnormalities are pre-
dominantly in temporal lobe, including medial temporal
lobe (e.g. amygdala–hippocampal complex) and neocor-
tical temporal lobe (i.e. STG, which includes planum
temporale and Heschl’s gyrus; see Goldstein et al.[30 ..]), followed by frontal, parietal [27 .,30..], and
occipital lobe abnormalities [34]. In addition, family
members of patients with schizophrenia appear also to
evince brain abnormalities, including amygdala–hippo-
campal volume anomalies [44,46,48.,49..] and corpus
callosum anomalies [47].
The recent and growing interest in studies of families
and relatives is particularly important; such investiga-
tions provide crucial information because brain abnorm-
alities observed in nonpsychotic relatives of patients with
schizophrenia provide the best indicator of potential
vulnerability markers of schizophrenia, independent of
psychosis. Such studies also provide important clues to
possible early neurodevelopmental anomalies that reflect
both liability or vulnerability to schizophrenia, and relate
to the expression of schizophrenia.
Finally, we note new methodologic advances, such as
the use of VBM [22,25..,36.], which offer a quick way
to evaluate multiple brain areas across many indivi-
duals, in contrast to the usual labor intensive manual
tracing of brain regions of interest. Additionally, a more
sophisticated method of asymmetry definition based on
a vector field [39 .] offers what may represent a better
assessment of asymmetry in such structures as hippo-
campus. These methods, which need further refine-
ment, will probably offer new possibilities for
generating hypotheses that can then be followed up
in more carefully delineated manual region of interest
investigations.
Magnetic resonance imaging studies: firstepisode schizophreniaThe extent to which brain abnormalities found in
chronic schizophrenia are also present in first episode
schizophrenia is the focus of a number of MRI studies.
Individuals with a first episode of schizophrenia provide
a unique opportunity to examine the effects of a
psychiatric process without the confounding factors of
chronicity and exposure to chronic neuroleptic medica-
tions. Additionally, studying first episode schizophrenia
patients, as well as childhood and adolescent onset
schizophrenia, and at-risk populations such as relatives of
schizophrenic patients (see previous section) and in-
dividuals with schizotypal personality disorder is a
fruitful strategy to elucidate the etiology of schizophre-
nia and its cognitive correlates [5..,59,60]. Again, as with
the MRI studies of chronic schizophrenia, both neuro-
developmental and neurodegenerative models of schizo-
phrenia provide a theoretical framework for many of the
studies.
Initial abnormalities
The majority of studies document that brain abnormal-
ities exist at the onset of the illness.
Multiple brain areas approach
Two studies examined multiple brain areas to look for
evidence of an initial insult [61,62]. Cahn et al. [61] (see
Table 3 for brain regions studied) found enlargement of
the third ventricle only, suggesting to these investigators
that other brain abnormalities reported in schizophrenia
may appear later in the course of illness and also may be
medication related.
Using the strategy of comparing volumetric changes
across different clinical populations, Salokangas et al. [62]
examined differences in several brain areas (Table 3) in
first episode schizophrenia, and in depression, with and
without psychotic features. First episode patients
evinced reduced left frontal lobe volumes, whereas
depressive patients with psychosis evinced enlarged
ventricular and posterior sulcal cerebrospinal fluid
volumes. Patients with depression without psychotic
features only evinced larger white matter volumes than
other clinical groups.
Schizophrenia134

Table 3. Magnetic resonance imaging structural findings in first episode schizophrenia
ReferenceMagnet/slicethickness Participants (n)
Mean age(years)
Sex[male/female (n/n)] MRI measures and major findings
Cahn [61] 1.5 Tesla/1.6 mm(contiguous)
SZ 20NC 20
SZ 27.63NC 27.24(Neurolepticnaı̈ve)
SZ 16/4NC 16/4
ICC, total brain, frontal lobe (gray and white matter),cerebellum, hippocampus, parahippocampal gyrus,thalamus, caudate nucleus, and lateral and third ventricleswere measured. Only third ventricle differed in SZ ascompared with NC, with enlarged third ventricle in SZ.The investigators concluded that this paucity of findings infirst episode SZ suggests that brain abnormalities developover time as seen in chronic SZ, which may therefore berelated to a progression of the illness or to the effects ofneuroleptic medications over time. (There weredifferences in education between groups).
Frumin [63] 1.5 Tesla/1.5 mm(contiguous)
SZ 14AFF 19NC 18
SZ 28.1AFF 25.8NC 24.5(Minimal neuro-leptic expo-sure)
SZ 11/3AFF 14/5NC 16/2
Corpus callosum area and shape measures werecompleted. Group differences were noted in shape for SZversus NC, but no differences between groups wereobserved for area measures of the corpus callosum.
Gunduz [64] 1.5 Tesla/5 mm (contigu-ous), 1 mm inplane resolution
SZ = 51(SZAFF 4,SZPHRE13)NC 28
SZ 24.5NC 25.8(Neurolepticnaı̈ve and mini-mal exposure)
SZ 37/14NC 17/11
Total brain volume, caudate nucleus, putamen, nucleusaccumbens volume, and subcommissural limbic forebrainvolume were measured. Findings showed no groupdifferences in volumes of the basal ganglia, although agewas correlated with volumes of caudate and putamen inNC. (There were differences in education and parentalsocioeconomic status between groups).
Joyal [65] 1.5 Tesla/1.5 mm(contiguous)
SZ 18NC 22
SZ 28NC 30(Neurolepticnaı̈ve)
SZ 11/7NC 14/8
Entorhinal cortex and whole brain volume were measured.Findings showed smaller entorhinal cortex volume in SZversus NC.
Keshavan [66] 1.5 Tesla/5 mm(1-mm inter-slice gap)
SZ 31Non-SZP 12NC 31
SZ 24.20Non-SZP22.83NC 25.09
SZ 20/11Non-SZP 6/6NC 20/11
Area measures of the corpus callosum were completed.Findings showed smaller area of corpus callosum, itsanterior genu, anterior body, isthmus, and anteriorsplenium in SZ as compared with NC and non-SZP. Age-related increases in corpus callosum size observed in NCwere not seen in patients, suggesting neuro-developmental abnormalities.
McCarley[67..]
1.5 Tesla/1.5 mm(contiguous)
SZ 15AFF 18NC 18
SZ 27.6AFF 23.5NC 24.9
SZ 12/3AFF 15/3NC 15/3
ICC, total gray and white matter, planum temporale, andHeschl’s gyrus were measured. Findings showed smallergray matter volume of the left planum temporale andsmaller Heschl’s total gray matter volume in SZ, whichdiffered from AFF and NC.
Salokangas[62]
1.5 Tesla/5.4 mm(contiguous)
SZ 11PD 20Non-PD 17NC 19
SZ 36.6PD 34.0Non-PD 38.4NC 30.5
SZ 3/8PD 8/12Non-PD 8/9NC 12/7
Frontal and temporal lobe gray and white matter weremeasured, as well as lateral ventricles and sulci. Findingsshowed reduced gray matter volume in left frontal lobe inSZ group as well as larger ventricular and posterior sulcalcerebrospinal fluid volumes in the PD group, and largerwhite matter volumes in the non-PD group.
Sumich [68] 1.5 Tesla/1.5 mm(contiguous)
SZ 25NC 16
SZ 24.0NC 27.0(Minimallytreated withneuroleptics)
All male Whole brain, Heschl’s gyrus, planum temporale,hippocampus, and amygdala were measured. Findingsshowed smaller hippocampus volumes and smaller leftplanum temporale volumes in the SZ group.
Szesko [69] 1.0 Tesla/3.1 mm(contiguous)
SZ 75NC 36
SZ 24.7SZ 27.3NC = 25.3
SZ 43/32NC 24/12
Hippocampal volume and ICC were measured. Findingsshowed that anterior hippocampal volume was correlatedwith motor and executive functions in men with SZ.
Lee [70.] 1.5 Tesla/1.5 mm(contiguous)
SZ 22AFF 20NC 24
SZ 26.0AFF 22.6NC 24.0
SZ 17/5AFF 15/5NC 21/3
Whole brain gray and white matter and CSF weremeasured. Findings showed smaller volume of leftfusiform gyrus in SZ versus NC and AFF. Right fusiformgyrus volume was also smaller in SZ as compared withthe NC group only.
Wood [71] 1.5 Tesla/1.5 mm(contiguous)
SZ 30CHRSZ 12NC 26
SZ 21.8CHRSZ 33.6NC 23.8
SZ 19/11CHRSZ 11/1NC 14/12
ICC, temporal lobe, hippocampus, and whole brain weremeasured in a follow-up study averaging 2.2 yearsfollowing the first MRI scan. Findings showed whole brainvolume loss in both chronic and first episode SZ at followup.
AFF, affective disorder with psychosis; CHRSZ, chronic schizophrenia; CSF, cerebrospinal fluid; ICC, intracranial contents (brain, ventricular system,and subarachnoidal CSF); MRI, magnetic resonance imaging; NC, normal control; non-SZP, nonschizophrenic psychotic; PD, psychotic depression;SZ, first episode schizophrenia; SZAFF, schizoaffective; SZPHRE, schizophreniform.
Structural and functional imaging in schizophrenia Niznikiewicz et al. 135

Temporal lobe structures (amygdala–hippocampal complex,
entorhinal cortex, and superior temporal gyrus)
Four studies looked directly at STG volumetric
abnormalities [53,54,67..,68]. [The study conducted
by Levitt et al. [53] is discussed in detail under Change
over time (see below).] A study conducted by
McCarley et al. [67 ..] focused on gray matter in STG,
amygdala–hippocampal complex, and parahippocampal
gyrus in first episode schizophrenia, patients with a first
episode of affective psychosis (mainly manic), and in
normal control subject individuals (Fig. 2). Patients
with first episode schizophrenia had smaller gray matter
volumes of left posterior STG, left planum temporale,
and total Heschl’s gyrus volume relative to control
individuals and to affective patients. Similar conclusions
were drawn in a study conducted by Sumich et al. [68],
in which first episode schizophrenic patients were
found to have smaller volumes of hippocampus
bilaterally and smaller left planum temporale relative
to control individuals.
In a study of adolescent persons with early onset
schizophrenia, Matsumoto et al. [54] found reduced
right rather than left superior temporal gyrus, and
severity of thought disorder and hallucinations were
inversely correlated with volume of the right superior
temporal gyrus, suggesting that this pattern of
abnormalities may be characteristic of early onset
schizophrenia. Of note, this asymmetry finding is the
reverse of that reported in adult onset schizophrenia,
in which left STG is frequently reported to be
reduced [67 ..].
The relationship between hippocampal volume and
neuropsychological function was evaluated by Szeszko
et al. [69] in 43 men and 32 women with first episode
schizophrenia. Anterior hippocampus was correlated
with both executive and motor functions in men,
although no significant correlations emerged for
women. These results further suggest that medial
temporal lobe abnormalities are present at first
episode and that such abnormalities are associated
with what are considered frontal lobe functions,
therefore further suggesting an abnormality in fron-
to–temporal neural circuitry in schizophrenia. These
findings also suggest a role for sex in mediating both
structural and functional abnormalities in schizophre-
nia.
Joyal et al. [65] measured the entorhinal cortex in
neuroleptic naı̈ve patients with schizophrenia and
control individuals. Those investigators reported re-
duced entorhinal cortical volume in the patient group.
This finding is consistent with previous reports of
entorhinal cortical volume reduction in schizophrenia
(for review [5 ..]).
Fusiform gyrus
Lee et al. [70.] reported reduced left fusiform gyrus in
first episode patients with schizophrenia relative to first
episode patients with affective psychosis (mainly manic)
and normal control individuals. The fusiform gyrus
volume on the right was smaller in schizophrenic
patients as compared with controls but not smaller than
in the affective group. This gyrus is important in the
identification of human faces, and volume reduction here
may be relevant to problems that patients with schizo-
phrenia experience with respect to social cues.
Midline structures
Keshavan et al. [66] measured the area of the corpus
callosum in neuroleptic naı̈ve first episode patients,
nonpsychotic patients, and normal control individuals.
Reduced area was found in the anterior genu, body,
isthmus, and splenium subdivisions of the corpus
callosum, which connect heteromodal association areas,
but not in those areas that connect primary cortices, in
first episode schizophrenia patients, followed by non-
schizophrenic, and psychotic patients. In addition, age-
related growth in the size of the corpus callosum was
present in normal persons but not in first episode
schizophrenia patients. The authors viewed these results
as supporting a neurodevelopmental abnormality, which
impacts primarily on association cortices. Frumin et al.[63] also reported abnormal shape but not volume in first
episode schizophrenia patients, but not in affective
psychosis patients.
Subcortical structures
Gunduz et al. [64] examined the integrity of parts of
the basal ganglia (caudate nucleus, nucleus accum-
bens, putamen, subcommissural limbic forebrain) in
first episode, medication naı̈ve schizophrenia patients.
No volumetric differences were found in basal ganglia
structures between neuroleptic naı̈ve first episode
schizophrenic patients (n = 53) and normal controls
(n = 28). Of note also is the study conducted by
McCreadie et al. [56], in which gray matter volume in
components of the basal ganglia (putamen and caudate
nucleus), as well as volume of the lateral ventricles,
were measured in never medicated patients in rural
India, who were estimated to have been ill for
approximately 10 years. One group of patients
suffered from dyskinesia whereas the other did not.
Results showed larger left putamen in the dyskinesia
patients; the patients without dyskinesia evinced a
higher lateral ventricle : hemisphere ratio, especially on
the right side. The authors concluded that schizo-
phrenic pathology may interfere with normal, age-
related changes in the basal ganglia, which are
independent of medication effects (Table 2). Several
methodologic limitations preclude clear-cut interpreta-
tion of the findings.
Schizophrenia136

Change over time
Change over time was explicitly addressed in four
studies [52,53,55..,71]. In the study conducted by Levitt
et al. [53], volumetric changes in medial temporal lobe
regions were evaluated in a group of early psychosis
schizophrenic patients (mean age 14 years; mean time of
onset to scan time 4.2 years). Although childhood onset
schizophrenia patients are different from first episode
populations, in this group no volumetric changes were
observed in the hippocampus, but the amygdala was
enlarged in the patient group, with the group difference
more pronounced on the left side. There was also a trend
toward left greater than right asymmetry in the amygdala
volume in the patient group (Table 2).
Both the study by Thompson et al. [55..] and that by
Wood et al. [71] found evidence of ongoing neuro-
degenerative processes, whereas James et al. [52] did
not. Using a new method for evaluating the brain,
Thompson et al. [55..] tracked the rate of progression
of gray matter loss in children with childhood onset
schizophrenia (aged 13–18 years). Results suggest an
age-dependent loss of gray matter, which is progressive
and most pervasive in the parietal lobe early, with
progression to superior frontal and motor areas, and
lateral temporal and dorsolateral prefrontal cortex. Of
particular note, the rate of progression in this group
surpassed normal gray matter loss observed in normal
control individuals.
Furthermore, to examine progressive changes over time,
Wood et al. [71] conducted a study of first episode and
chronic patients with a 2.2-year time interval between
MRI scans. No time-related changes were observed in
the hippocampus or in the temporal lobe in the first
episode group. However, whole brain volumetric loss
was observed in both first episode and chronic groups,
and the rates did not differ between the two patient
groups.
In contrast, James et al. [52], in their study of
adolescent onset schizophrenia cases, demonstrated
enlarged lateral and third ventricles and reduced left
amygdala, and a trend toward left hippocampal volume
reduction at baseline as compared with control
individuals (Table 2). Scans taken at an average of
1.7 years later for control individuals and 2.7 years later
for the adolescent onset group revealed no reduction
over time. The authors interpreted these findings as
suggesting a nonprogressive neurodevelopmental dis-
order that impacts on brain structures before the onset
of clinical symptoms. However, the small sample, the
different time intervals between scans for patient and
control groups, and the relatively thick 3-mm slices all
limit the generalizability of these findings. It is also
quite likely that early onset schizophrenia constitutes a
subtype of schizophrenia that is unrelated to adult
onset schizophrenia.
Summary
First episode patients evince brain abnormalities, most
notably in medial temporal lobe (amygdala–hippocampal
complex, entorhinal cortex), STG, corpus callosum, left
planum temporale and left Heschl’s gyrus, left frontal
gray matter, and left fusiform gyrus. They also generally
have larger lateral ventricles than do control individuals.
These findings are similar to those reported in chronic
schizophrenia. In addition, there is some indication that
initial brain abnormalities are present at the onset of
illness, suggesting neurodevelopmental influences.
Furthermore, there is some indication that certain brain
regions may show progressive changes over time,
although far more research work following a large
number of first episode patients over time is needed
before conclusions can be drawn regarding brain changes
over time.
Functional brain imaging studiesfMRI has been increasingly used to study abnormal
cognitive processes in schizophrenia because it is less
invasive and costly than positron emission tomography
and because it promises better localization of function
than does positron emission tomography. Because the
fMRI signal reflects, indirectly, the relationship between
neural activity in response to a stimulus and blood flow
levels within brain regions, it can, at least in principle,
aid in identifying brain regions that exhibit abnormal
response to cognitive task requirements. As such, fMRI
can complement other imaging techniques such as
structural MRI, which offers an excellent spatial resolu-
tion, and event-related potentials, which offer excellent
temporal resolution, to provide information on where in
the brain cognitive operations are disturbed. However,
its ultimate success crucially depends upon appropriate
experimental designs and data analysis techniques
[72,73].
Most recent fMRI studies focused on deficits identified
by neuropsychologic and clinical research as central to
schizophrenia, including working memory, language
function, and thought disorder and auditory hallucina-
tions, as well as social cognition and correlates of
abnormal saccadic eye movements. More recently, fMRI
has also been used to ascertain the impact of medication
and behavioral therapy treatments. In addition, studies
have examined abnormal motor function [74,75] and
some have focused on face and affect processing [76,77].
In most studies, the focus has been on identifying a
network of brain regions that exhibit abnormal activation
and that are involved in the cognitive processes under
investigation. Figure 3 provides an illustration of fMRI
activation differences between normal control indivi-
Structural and functional imaging in schizophrenia Niznikiewicz et al. 137

duals and patients with schizophrenia, in the inferior
frontal lobe as a result of semantic encoding operations.
Of note, the activation observed in control individuals
was lacking in patients with schizophrenia. Below, we
review relevant fMRI studies conducted over the past
year; the studies are grouped according to the type of
cognitive operation investigated.
Executive function
Prefrontal cortex is involved in various aspects of
executive functioning and has been studied extensively
in schizophrenia. Weinberger et al. [78 ..], for example,
viewed prefrontal dysfunction and its association with
impaired working memory function as central to the
pathophysiology of schizophrenia. Those investigators
suggested that the catechol-O-methyl-transferase gene is
involved in regulation of frontal lobe function, especially
with respect to working memory tasks, and as such may
represent a candidate genetic risk factor for schizophre-
nia.
Two central objectives regarding the role of prefrontal
cortex in schizophrenia are to identify whether the
conditions that lead to abnormal dorsolateral prefrontal
cortex (DLPFC) response are manifested as either
hypoactivation or hyperactivation, and to identify the
network of functional connections between brain areas
that are involved in supporting specific cognitive
operations. With regard to the latter, the connections
between DLPFC and temporal cortex are especially
relevant to our understanding of functional abnormalities
in schizophrenia.
Barch et al. [79..] looked at the role of prefrontal
cortex in working and long-term memory deficits in
schizophrenia during the processing of verbal and
nonverbal stimuli. Those investigators found that right
DLPFC showed decreased activation in both working
memory and long-term memory tasks in patients with
schizophrenia (Table 4), as well as decreased activa-
tion in hippocampal regions, basal ganglia, thalamus,
and parietal cortex. This suggests that in schizophre-
nia there are impairments in the neural circuits that
are necessary to perform cognitive routines common
to both working memory and long-term memory
tasks, rather than impairments in discrete functional
areas.
However, in a study of logical reasoning conducted by
Ramsey et al. [81], prefrontal activation was normal in
medicated patients, after correcting for performance
between patients and normal control individuals. This
result is consistent with some previous studies [96,97]
that did not find ‘hypofrontality’ in patients, when
both patients and control individuals performed equally
well on a task (Table 4). In the same design,
nonmedicated patients showed activation levels that
were higher than those in normal control individuals.
These results suggest that performance levels across
groups may be an important factor in interpreting the
results of activation studies. Additionally, the result
found in unmedicated patients suggests that efficiency
of neural communication may be compromised in
schizophrenia.
Similarly, no group differences in the DLPFC were
found by Paulus et al. [82] in a study of decision making
(Table 4). However, abnormal activation was found
within the fronto-parietal network in patients with
schizophrenia (i.e. less activation in the inferior, medial
prefrontal, and right superior temporal cortex, and more
activation in the postcentral and inferior parietal cortex).
However, interpretation of these results is difficult
because, in addition to the complexity of the process
studied, nonmedicated patients as well as patients
medicated with typical and atypical neuroleptics were
included in the study.
An indication of abnormal fronto-parietal connection in
schizophrenia was also found by Honey et al. [83]. In the
working memory study, in which no group differences
were found in performance accuracy, a correlation was
found between increased reaction time and activation in
parietal cortex in the normal control group, whereas no
such correlation was detected in the patient group
(Table 4).
The functional integrity of prefrontal brain regions in
mediating inhibitory function was investigated by Rubia
et al. [84] using stop and ‘go/no go’ inhibitory motor
tasks. In the stop task there was less activation in the left
dorsolateral superior frontal gyrus and an increase in
subcortical areas in the schizophrenia group, with
equivalent behavioral performances in the patient and
normal control groups, suggesting involvement of an
abnormal neural network in inhibitory function.
The role of ACC in mediating error monitoring was
examined in normal control individuals and schizophre-
nic patients using an event-related fMRI design during a
continuous performance task [85.]. When the target
detection was made more challenging by degrading the
quality of the visual display, more errors were committed
by both groups. Healthy individuals showed a response-
related increase in activation in the anterior cingulate
gyrus related to error detection. Such an increase in
anterior cingulate gyrus activation was not observed in
schizophrenic patients. Moreover, anterior cingulate
gyrus activation was associated with impairments in
performance adjustment, suggesting that abnormal
internal error monitoring in schizophrenia may be related
to functional abnormalities in the cingulate cortex. A
Schizophrenia138

caveat to these results is that all patients were
medicated, which might have contributed to the limited
response in the cingulate.
Kumari et al. [86] examined functional correlates of
procedural learning often found to be abnormal in
schizophrenia. In normal control individuals there was
increased activity in brain regions associated with
procedural learning, including striatum, thalamus, cere-
bellum, precuneus, medial frontal lobe, and cingulate
gyrus. In schizophrenic patients, however, the only
structure activated was the anterior portion of the
inferior gyrus. Importantly, patients with schizophrenia
did not exhibit evidence of procedural learning. Again,
the results indicate a possible role of activated structures
in procedural learning, and abnormal procedural learning
in patients, which may stem from the inadequate
engagement of these structures.
Overall, results of many of the studies involving different
aspects of memory and executive function indicate that
functional abnormalities in schizophrenia are not only a
matter of reduced activation in the same brain region as
in normal control individuals (as demonstrated in some
studies) but also a matter of engaging different regions
or, alternatively, using different strategies mediated by
the same region, as demonstrated by other studies. For
example, Zorrilla et al. [80], using a picture recognition
paradigm, showed that in the patients there was a
positive correlation between recognition memory and
activation in the parahippocampal and hippocampus gyri
during encoding, whereas in normal control individuals
there was a negative correlation between these two
variables.
Saccadic eye movements
Two recent papers discussed neural substrates of
saccadic inhibition deficits in schizophrenia, which are
believed to represent a vulnerability marker for schizo-
phrenia and have been associated with a dysfunction in
the dorsolateral prefrontal cortex [98–100]. However, the
neural bases of the antisaccadic deficit are not well
understood [101,102]. The two studies also provide
nonconvergent results, probably due to different meth-
odologies (Table 4). In one of them, McDowell et al. [87]
analyzed blood oxygenation level dependent signal
change between refixation (fixation baseline) and anti-
saccades (refixation saccade baseline). Under these
conditions, only DLPFC was found to exhibit less
activation in patients with schizophrenia during anti-
saccade generation (Table 4).
In the other study, Raemaekers et al. [88] used an event-
related fMRI design. Brain activity generated during
saccade and antisaccade tasks were compared across
brain regions involved both in the generation of saccades
and in structures involved in the transmission of an
inhibitory signal to brainstem regions. In this design,
group difference existed in the striatum but not in the
DLPFC, suggesting that striatum structures are part of a
network that governs saccadic eye movement.
Language function in schizophrenia
Abnormal language function, in its many manifestations,
including thought disordered speech and verbal halluci-
nations, is a hallmark symptom of schizophrenia. It has
been proposed that abnormal lateralization of language
areas may be an underlying factor.
Functional lateralization for language was examined by
Sommer et al. [89 .]. Those investigators used a
lateralization index that was calculated for several areas
supporting language function (Table 4). Lower scores
on the lateralization index were found in schizophrenic
patients, which was due to increased activation in the
right hemisphere rather than to reduced activation in
the left hemisphere, suggesting an inefficiency in
inhibiting the nondominant hemisphere. The laterali-
zation index was also correlated with the severity of
hallucinations.
Figure 3. Semantic processing functional magnetic resonanceimaging study
z = 8 mm T value
4
3.5
3
2.5
2
1.5
1
0.5
0
Results are shown for a semantic processing functional magneticresonance imaging study. The axial image shows difference in activationin the left inferior prefrontal cortex (area in yellow) between nine controlindividuals and nine schizophrenia patients, which reflects groupdifferences in semantic encoding in a levels of processing paradigm.(Courtesy of Marek Kubicki.)
Structural and functional imaging in schizophrenia Niznikiewicz et al. 139

Table 4. Functional magnetic resonance imaging findings in schizophrenia
ReferenceParticipants(n)
Mean age(years)
Sex[male/female(n/n)] Task design Major findings
Executive and memory function studies
Barch [79..] SZ 38NC 48
SZ 36.3NC 36.5
SZ 24/14NC 23/25
WM and LTM tasks. Bothverbal and nonverbal stimuliwere presented within threetasks: WM-n-back task;encoding task; and recognitiontask. Block design; whole braincoverage
Impaired activation was found in SZ in theright DLPFC and the medial temporal lobefor both WM and LTM tasks. Otherregions found to have impaired activationduring both WM and LTM included basalganglia, thalamus, and parietal cortex.
Zorilla [80] SZ 8NC 10
SZ 54.2NC 61.9
SZ 3/5NC 8/2
Picture encoding andrecognition task
In NC, a negative correlation was foundbetween level of activation inparahippocampal gyrus and hippocampusfor the recognition task. In SZ, a positivecorrelation between the same variableswas found.
Ramsey [81] Exp 1: SZ 10;NC 10Exp 2: SZ (medi-cationnaı̈ve)11; NC 10
Exp 1: SZ 28.9;NC 24.1Exp 2: SZ 27.7;NC 28.4
Exp 1: SZ 9/1;NC 7/3Exp 2: SZ 8/3;NC 7/3
Logical reasoning, a version ofXT-task. Block design; wholebrain coverage
After correcting for performance, brainactivation was not different between NCand medicated SZ. In unmedicated SZ,brain activity was elevated relative to NC.
Paulus [82] SZ 15NC 15
SZ 41.7NC 41.0
All male Two-choice prediction task.Block design; whole braincoverage
No differences in activation were noted inthe right prefrontal cortex in SZ and NC.Less activation was found in inferior,medial prefrontal, and right superiortemporal gyrus in SZ. More activation wasalso found in right prefrontal and bilateralparietal cortex in medicated SZ relative tounmedicated SZ.
Honey [83] SZ 20NC 20
SZ 34.6NC 39.3
All male Verbal n-back task. Blockedperiodic BA design; whole braincoverage
No group difference was found inactivation levels in the prefrontal and parietalregions. A lack of correlation betweenreaction time and level of activation inparietal regions was found in SZ.
Rubia [84] SZ 6NC 7
SZ 40.0NC 40.0
All male Motor response inhibition stopand go/no-go tasks. Blockdesign; whole brain coverage
In both the stop and go/no-go tasks,reduced activation was observed in the leftanterior cingulate in SZ. During the stoptask, increased signal was observed in theright and left dorsomedial andventromedial thalamus, and right putamenin SZ.
Carter [85.] SZ 17NC 16
SZ 33.5NC 34.1
SZ 12/5NC 11/5
Error monitoring task. Subjectsdetected visual cues in eitherclear or degraded displayconditions in alternating blocks.Event-related design; wholebrain coverage
NC activated anterior cingulate, rightmedial frontal, and left posterior parietalcortex during error commission. No error-related increase in brain activity was foundin SZ.
Kumari [86] SZ 6NC 6
SZ 34.67NC 31.38
All male Procedural, sequence learningtask. Block design; whole braincoverage
Procedural learning was associated withactivation in the striatum, thalamus,cerebellum, precuneus, medial frontallobe, and cingulate gyrus in NC. In SZ,only anterior inferior gyrus was activated.
Saccadic eye movement studies
McDowell[87]
SZ 14NC 13
SZ 37.0NC 35.0
SZ 10/4NC 12/1
Refixation saccade and anti-saccade tasks. Block design;whole brain coverage
SZ patients did not show increasedDLPFC activation during the antisaccadetask as was observed in NC.
Raemaekers[88]
SZ 16NC 17
SZ 27.9NC 25.9
SZ 13/3NC 10/7
Occulomotor task: prosaccade,antisaccade, and active fixation.Event-related design; wholebrain coverage
Overall, activation was reduced in SZrelative to NC in all regions. The interactionbetween level of activation during theinhibitory task and illness was significantfor striatum only. SZ did not show theactivity in the striatum, which was presentin NC during antisaccade (inhibitoryactivity).
(continued opposite )
Schizophrenia140

Table 4. (continued )
ReferenceParticipants(n)
Mean age(years)
Sex[male/female(n/n)] Task design Major findings
Language studies
Sommer[89.]
SZ 12NC 12
SZ 27.0NC 28.0
All male Verb generation and semanticdecision reverse read task.Block design; whole braincoverage
Reduced language-laterality activation inthe SZ group was related to increasedactivation in the right hemisphere ratherthan to decreased activity in the lefthemisphere.
Kircher [90] SZ 6NC 6
SZ 34.3NC 34.0
All male Speech generation task.Seven Rorschach cards werepresented on the screenduring scanning and subjectswere asked to describe them.Event-related design; wholebrain coverage
In SZ, severity of thought disorder wascorrelated positively with activity in thecerebellar vermis, right body of caudate,and right precentral gyrus. Severity ofthought disorder was negativelycorrelated with left superior temporalgyrus, and the posterior part of middletemporal gyrus.
Kircher [91.] SZ 6NC 6
SZ 34.3NC 34.0
All male Speech generation task.Seven Rorschach cards werepresented on the screenduring scanning and subjectswere asked to describe them.Event-related design; wholebrain coverage
NC activated more the left, whereas SZactivated more the right middle temporalgyrus.
Lawrie [44] SZ 8NC 10
SZ 28.6NC 26.4
SZ 3/5NC 5/5
Sentence completion task.Block design; whole braincoverage
Bilateral activation of DLPFC and leftmiddle/superior temporal gyrus wasobserved in both groups. Functionalfrontotemporal connectivity wasdiminished in SZ.
Bentaleb [92] SZ 1NC 1
SZ 36NC 36
Female casestudy
Patient with auditoryhallucinations scanned duringhallucinations and whilelistening to external speech.Block design; whole braincoverage
Auditory verbal hallucinations wereassociated with increased activity in theleft primary auditory cortex and the rightmiddle temporal gyrus.
Shegrill [93] SZ 1 SZ 36 Male singlecase study
Single patient imaged duringsomatic and auditory verbalhallucinations. Event-related-likedesign; whole brain coverage
Somatic hallucinations were associatedwith activation in the primarysomatosensory and posterior parietalcortex, and auditory hallucinations wereassociated with middle and superiortemporal cortex activation.
Motor function studies
Kodama [74] SZ 9NC 10
SZ 23.2NC 24.9
SZ 6/3NC 6/4
Finger tapping task. Blockdesign. Slices coveringprefrontal cortex (axial slicesabove the corpus callosum)
Less activation was found in the premotorareas in SZ; after training, the activationlevel increased in the left premotor area inSZ and decreased in NC.
Muller [75] SZ(HA) 10SZ(OL) 10SZ(UN) 10NC 10
SZ(HA) 32.0SZ(OL) 30.2SZ(UN) 32.7NC 32.8
SZ(HA) 10SZ(OL) 10SZ(UN) 7/3NC 10
Finger tapping task. Blockdesign; whole brain coverage
Right premotor cortex, putamen, and leftcerebellum had higher activation inSZ(UN) than in NC. SZ(UN) exhibitedhigher level of activation than other treatedSZ patients across all regions studied.
Face and emotion processing studies
Kosaka [76] SZ 12NC 12
SZ 26.0NC 24.4
SZ 6/6NC 6/6
Facial emotional intensityjudgment task and the size of ageometric shape judgment task.Block design; coronal slicescovering amygdala only
Positive facial emotion identificationactivated the amygdala bilaterally in bothgroups, but greater activation of the rightamygdala was found in SZ relative to NC.Negative face emotion identification didnot produce group differences, butbilateral amygdala activation was found inSZ whereas only right amygdala activationwas found in NC.
Quintana [77] SZ 8NC 8
SZ 35.22NC 29.25
SZ 6/2NC 6/2
Visual-motor task of cue andstimulus matching with either acircle or a facial diagram. Blockdesign; axial slices superior tothe middle temporal lobe
Motor cortical areas involved in therepresentation and execution of facialmovement were activated in SZ onlyduring processing of facial expressions.
(continued overleaf )
Structural and functional imaging in schizophrenia Niznikiewicz et al. 141

Two fMRI studies conducted by Kirscher and coworkers
[90,91 .] focused on thought disorder and its relationship
to brain activation. fMRI was performed while thought
disordered and normal control individuals talked about
Rorschach cards. In the control individuals the amount of
words articulated was positively correlated with activa-
tion in the left STG, whereas in the patients it was
correlated with activation in the right STG. Those
authors interpreted these results as evidence for
abnormal lateralization of areas involved in word retrieval
and speech planning and monitoring. They proposed
that relatively greater activation of the right STG in the
patients may directly contribute to loosening of associa-
tions, because the right STG is presumably involved in
generating broad semantic fields [103,104] whereas the
left STG is involved in maintaining narrow semantic
fields so that contextually inappropriate meanings are
suppressed early.
Functional correlates of auditory hallucinations
The relationship between auditory hallucinations and
functional connectivity between frontal and temporal
structures was examined in an fMRI study conducted by
Lawrie et al. [105 .]. Both patients and control individuals
showed equivalent levels of DLPFC activation in the
sentence completion task, but the functional correlation
coefficient between activity in left DLPFC and left
medial/superior temporal cortex was lower in the patient
group, and this correlation connectivity coefficient was
lower still in patients with hallucinations (Table 4). This
finding of abnormal connectivity between frontal and
temporal areas is in agreement with the findings of a
study conducted by Ford et al. [106].
A direct approach of mapping auditory hallucinations
onto brain regions was taken by Bentaleb et al. [92] in a
single case study. In that study a female patient with
schizophrenia was scanned while experiencing auditory
verbal hallucinations, and while listening to external
speech that eliminated the subjective experience of
auditory hallucinations. Experiencing auditory hallucina-
tions was associated with increased activity in the
primary auditory cortex and medial temporal gyrus.
Another single case was reported by Shegrill et al. [93],
who acquired fMRI signal during somatosensory and
auditory hallucinations. Somatosensory hallucinations
activated primary somatosensory and parietal cortices,
whereas auditory hallucinations activated the middle and
superior temporal cortex. Both of these studies sug-
gested that experiencing hallucinations in a given
modality (auditory or somatosensory) involves activation
of sensory areas that are normally involved in processing
sensory information in that modality.
Functional magnetic resonance imaging: a tool to study
the efficacy of clinical interventions
Wykes et al. [94.] used fMRI to study functional brain
changes after cognitive remediation therapy aimed at
improving information processing during working mem-
ory tasks. All individuals were scanned twice. Decreased
activation was found in normal individuals on repeat
scans, whereas increased activation of the right inferior
frontal gyrus was observed in schizophrenic patients,
especially those who underwent cognitive remediation
therapy (Table 4). Because no other measures such as
medication or symptom severity changed across the two
scanning sessions, the authors suggested that these
Table 4. (continued )
ReferenceParticipants(n)
Mean age(years)
Sex[male/female(n/n)] Task design Major findings
Drug and behavioral therapy efficacy studies
Wykes [94.] SZ(CRT) 6SZ(CT) 6NC 6
SZ(CRT) 35.0SZ(CT) 36.0NC 36.0
All male Two back, working memorytask, a vigilance task. Blockdesign; 10 axial slices in theanterior commissure-posteriorcommissure plane
As a result of cognitive remediationtherapy, increased values of FPQ werefound in SZ in right inferior frontal gyrus,and bilateral occipital cortex, and de-creased values of FPQ were found in NCin the left inferior/middle frontal gyrus, rightfrontal cortex, and right inferior frontalcortex.
Stephan [95.] SZ 6NC 6
SZ 25.8NC 27.5
SZ 5/1NC 5/1
Alternating finger tapping taskof the right and left hand.Subjects were scanned twice,3 weeks apart, with SZ beingmedicated at the 2nd scan.Block design; whole brain cov-erage
This study examined CFC as a function ofolanzapine treatment with seed voxelcorrelational analysis. Results suggest thatthere is a normalization of CFC afterolanzapine treatment.
CFC, cerebellum functional connectivity; DLPFC, dorsolateral prefrontal cortex; Exp, experiment; FPQ, fundamental power quotient; LTM, long-termmemory; NC, Normal control; SZ, schizophrenia; SZ(CT), SZ receiving cognitive therapy; SZ(CRT), SZ receiving cognitive remedial therapy; SZ(HA),SZ receiving haldol; SZ(OL), SZ receiving olanzapine; SZ(UN), untreated SZ; WM, working memory.
Schizophrenia142

results were attributable to practice and remediation
therapy benefits.
An interesting report from Stephan et al. [95 .] discussed
the role of olanzapine in ‘normalizing’ the functional
connectivity between cerebellar activity and thalamic
cortical circuitry during finger tapping in patients with
schizophrenia. Using seed voxel correlation analysis,
which was introduced by Horwitz and coworkers
[107,108], the study explored cerebellar functional
connectivity, and it was concluded that olanzapine
improved cerebellar functional connectivity for the right
but not for the left cerebellum (Table 4).
Summary
Continuing the tradition of more recent reports [109],
most studies reported during the past year used
activation paradigms that employed experimental de-
signs traditionally used in neuropsychology such as the
n-back task, verb generation or finger tapping, along with
clinical tools such as Rorschach cards. The experiments
were designed to identify which brain regions show
abnormal activation in tasks probing executive and
memory processes, language processes, and motor
function. The overwhelming number of studies suggests
that for any given task there is not a single abnormal
brain region that is related to abnormal function, but
instead there is a network of brain regions that are
affected and that, together, contribute to functional
abnormalities in schizophrenia. Abnormal connectivity
between temporal and frontal brain regions continues to
figure prominently in functional abnormalities in schizo-
phrenia. Importantly, some studies indicated that
patients with schizophrenia not only show a nonoptimal
activation in brain regions used by normal control
individuals in a given task, but they also might use
different brain regions, either as part of compensatory
mechanisms or faulty neural connections. Finally, as a
new development, a handful of studies used fMRI as a
tool to look at the efficacy of both medication and
behavior therapy interventions. This latter application of
fMRI will probably figure more prominently in future
studies, particularly in studies testing the efficacy of new
medications in targeting cognitive and clinical symptoms
in schizophrenia.
Diffusion tensor imagingDTI is another promising tool that permits further
examination of abnormal functional connectivity in
schizophrenia, and thus brings us closer to under-
standing schizophrenia as a disease of disconnections,
or disruptions, in important brain areas that work in
concert, and not in isolation, in cognition and behavior.
DTI is a relatively new technique that can be used to
visualize and measure the diffusion of water in brain
tissue, and it is particularly useful for evaluating white
matter abnormalities in the brain. Thus far seven DTI
studies have been conducted in schizophrenia [110–
115,116 ..] to investigate white matter abnormalities in
multiple brain regions, including prefrontal and temporal
white matter, corpus callosum, and uncinate fasciculus
(for review [10 ..]). Figure 4 shows a single coronal slice
of a tensor map (see left image; this map is primarily
used for visualization purposes) and an anisotropy map
(see right image; this map is used for diffusion
quantification), both of which were derived from DTI
data. Figure 5 shows the newest application of DTI,
namely in-vivo white matter fiber tractography, a
method that will render possible both dissection and
quantification of major white matter pathways in the
human brain in vivo.
In a recent study, Kubicki et al. [116..] used DTI to
examine the structural integrity of white matter tracks
(b)(a)
Figure 4. Diffusion tensor imaging
Coronal slices (4-mm thick) are shown that wereacquired on a 3 Tesla magnet using diffusiontensor imaging. These images are from a normalcontrol individual. (a) A diffusion tensor map, inwhich the blue lines represent the in-planecomponent of the diffusion (i.e. white matter fibertracts are traveling parallel to the acquisitionplane). The out-of-plane components of diffusionare color coded (from yellow to dark orange),and represent fibers that are perpendicular to theacquisition plane (i.e. the darker the color, thestronger the out-of-plane diffusion). (b) Afractional anisotropy map – a rotationallyindependent measure that is frequently used forquantifying diffusion. (Courtesy of MarekKubicki.)
Structural and functional imaging in schizophrenia Niznikiewicz et al. 143

of the uncinate fasciculus, the most prominent fiber
track that connects the frontal and temporal lobes.
Those investigators found a lack of normal left4right
asymmetry in a fractional anisotropy measure (a
measure of water diffusion within the fibers, and thus
an indirect measure of the integrity of the fibers) in
patients with schizophrenia as compared with normal
control individuals. Findings from that study are but
another piece of evidence in support of abnormal
connectivity patterns between the frontal and temporal
lobes in schizophrenia.
ConclusionThe picture emerging from current MRI and fMRI
research, as well as from the small number of DTI
studies thus far conducted, is that schizophrenia is a
brain disorder in which multiple areas are affected not in
a random manner but along the lines of functional
connectivity, with prominent roles played by both frontal
and temporal cortical structures, but also with involve-
ment of relevant subcortical brain regions. As new
experimental designs are informed by advances in
cognitive neuroscience, and new analytic techniques
optimize information that can be gleaned from fMRI
designs and from new advances in structural MRI and
DTI, the field of schizophrenia will be enriched with a
more comprehensive understanding of this devastating
disease. In the domain of fMRI research, advances in
analyzing fMRI data are important for meaningful
interpretation of results. Accordingly, future directions
should include careful experimental designs that afford a
better understanding of the neural connectivity involved
in supporting cognitive tasks. It is also becoming
apparent that medication status of patients is an
important factor, both as a potential confounding factor
and as a variable of interest with respect to the efficacy of
medication on cognitive tasks evaluated by fMRI, as
well as on possible neuroprotective effects with respect
to ameliorating possible changes in brain structure over
time as evaluated by structural MRI and DTI. Finally,
more studies are needed that evaluate relatives of
patients with schizophrenia in order to elucidate further
Figure 5. In-vivo three-dimensional fiber tractography of the human brain
An in-vivo three-dimensional fiber tractography ofthe human brain is shown, which was createdusing diffusion tensor imaging data. The dataused to create this three-dimensional modelwere acquired on a 3 Tesla magnet. (Courtesy ofHae Jong Park.)
Schizophrenia144

markers or genetic risk factors associated with brain
abnormalities in schizophrenia.
AcknowledgementsResearch by the authors and cited in the present review was supportedin part by the National Institute of Mental Health MH R01 50740 (MES),MH K02 01110 (MES), MH 63360 (MAN), by two VeteransAdministration Merit Awards (MES and MAN-Co-PI), and by aNARSAD Young Investigator Award (MK). The authors also wish toacknowledge Lisa Lucia for her assistance in getting the bibliographyand tables together, and Marie Fairbanks for her administrative support.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:. of special interest.. of outstanding interest
1 Kraepelin E. Dementia praecox. 1919/1971. New York: Churchill LivingstoneInc.
2 Bleuler E. Dementia praecox or the group of schizophrenias. 1911/1950.New York: International Universities Press.
3 Johnstone EC, Crow TI, Frith CD, et al. Cerebral ventricular size andcognitive impairment in chronic schizophrenia. Lancet 1976; 2:924–926.
4 Smith RC, Calderon M, Ravichadran GK, et al. Nuclear magnetic resonancestudy in schizophrenia: a preliminary study. Psychiatry Res 1984; 12:137–147.
5. .
Shenton ME, Dickey CC, Frumin M, McCarley RW. A review of MRI findingsin schizophrenia. Schizophr Res 2001; 49:1–52.
This paper is the most comprehensive review of MRI structural findings inschizophrenia to date.
6 Andreasen NC. Linking mind and brain in the study of mental illnesses: aproject for a scientific psychopathology. Science 1997; 275:1586–1593.
7 Andreasen NC. Schizophrenia: the fundamental questions. Brain Res 2000;31:106–112.
8 Weinberger DR. On the plausibility of ‘The Neurodevelopmental Hypothesis’of schizophrenia. Neuropsychopharmacology 1996; 14 (Suppl):1S-11S.
9 Weinberger DR, Mattay V, Callicott J, et al. fMRI applications inschizophrenia research. Neuroimage 1996; 4:S118-S126.
10. .
Kubicki M, Westin CF, Maier C, Mamata F, et al. Diffusion tensor imagingand its application to neuropsychiatric disorders. Harvard Rev Psychiatry2002; 10:324–336.
This paper provides a review of DTI applications in neuropsychiatric disorders andis one of the few reviews on this topic.
11.
Kasai K, Iwanami A, Yamasue H, et al. Neuroanatomy and neurophysiology inschizophrenia. Neurosci Res 2002; 43:93–110.
This paper provides an up-to-date review of neuroanatomical and neurophysiologyin schizophrenia.
12 Carpenter MB, Sutin J. Human neuroanatomy. New York: Williams & Wilkins;1983.
13 Fuster JM. The Prefrontal Cortex. New York: Raven Press; 1989.
14 Goldman-Rakic PS, Selemon LD, Schwartz ML. Dual pathways connectingthe dorsolateral prefrontal cortex with the hippocampal formation andparahippocampal cortex in the rhesus monkey. Neuroscience 1984;12:719–743.
15 Pandya DN, Seltzer B. Association areas of the cerebral cortex. TrendsNeurosci 1982; 5:386–394.
16 Pandya DN, Van Hoesen GW, Mesulam MM. Efferent connections of thecingulate gyrus in the rhesus monkey. Exp Brain Res 1981; 42:319–330.
17 Selemon LD, Rajkowska G, Goldman-Rakic PS. Abnormally high neuronaldensity in the schizophrenic cortex. A morphometric analysis of prefrontalarea 9 and occipital area 17. Arch Gen Psychiatry 1995; 52:805–820.
18 Vogt BA, Pandya DN, Rosene DL. Cingulate cortex of the rhesus monkey: I.Cytoarchitecture and thalamic afferents. J Comp Neurol 1987; 262:256–270.
19 Vogt BA, Pandya DN. Cingulate cortex of the rhesus monkey: II. Corticalafferents. J Comp Neurol 1987; 262:271–289.
20.
Weinberger DR, McClure RK. Neurotoxicity, neuroplasticity, and magneticresonance imaging morphometry: what is happening in the schizophrenicbrain? Arch Gen Psychiatry 2002; 59:553—558.
This paper provides a thoughtful commentary on the interpretation of neurotoxicity,neuroplasticity, and MRI morphometric measures in schizophrenia, and what theyprobably mean.
21 Okubo Y, Saijo T, Oda K. A review of MRI studies of progressive brainchanges in schizophrenia. J Med Dent Sci 2001; 48:61–67.
22 Velakoulis D, Wood SJ, Smith DJ, et al. Increased duration of illness isassociated with reduced volume in right medial temporal/anterior cingulategrey matter in patients with chronic schizophrenia. Schizophr Res 2002;57:43–50.
23 Hulshoff Pol HE, Schnack HG, Bertens MG, et al. Volume changes in graymatter in patients with schizophrenia. Am J Psychiatry 2002; 159:244–250.
24 Convit A, Wolf OT, de Leon MJ, et al. Volumetric analysis of the pre-frontalregions: findings in aging and schizophrenia. Psychiatry Res 2001; 107:61–73.
25. .
Ananth H, Popescu I, Critchley HD, et al. Cortical and subcortical gray matterabnormalities in schizophrenia determined through structural magneticresonance imaging with optimized volumetric voxel-based morphometry. AmJ Psychiatry 2002; 159:1497–1505.
These investigators apply VBM measures to elucidating cortical and subcorticalgray matter abnormalities in schizophrenia. This method will probably be importantin future structural and fMRI studies because it can be completed quickly in a largenumber of cases, in contrast with manual measurements, which are timeconsuming and restrict the number of cases that can be evaluated at any onetime. Moreover, multiple brain regions can be evaluated at once.
26 Chemerinski E, Nopoulos PC, Crespo-Facorro B, et al. Morphology of theventral frontal cortex in schizophrenia: relationship with social dysfunction.Biol Psychiatry 2002; 52:1–8.
27.
Chow EW, Zipursky RB, Mikulis DJ, Bassett AS. Structural brainabnormalities in patients with schizophrenia and 22q11 deletion syndrome.Biol Psychiatry 2002; 51:208–215.
This paper presents a study of patients with schizophrenia and 22q11 deletionsyndrome. By investigating known genetic disorders in which one outcome isschizophrenia-like symptoms, we may learn more about the genetic determinantsof schizophrenia.
28 Erbagci H, Yildirim H, Herken H, Gumusburun E. A magnetic resonanceimaging study of the adhesio interthalamica in schizophrenia. Schizophr Res2002; 55:89–92.
29 Falkai P, Honer WG, Alfter D, et al. The temporal lobe in schizophrenia fromuni- and multiply affected families. Neurosci Lett 2002; 325:25–28.
30. .
Goldstein JM, Seidman LJ, O’Brien LM, et al. Impact of normal sexualdimorphisms on sex differences in structural brain abnormalitiesin schizo-phrenia assessed by magnetic resonance imaging. Arch Gen Psychiatry2002; 59:154–164.
This paper investigates more than 22 brain regions using MRI, and it is a carefuland thoughtful study of the impact of normal sexual dimorphisms on sexdifferences in structural brain abnormalities in schizophrenia.
31 Hagino H, Suzuki M, Kurokawa K, et al. Magnetic resonance imaging studyof the cavum septi pellucidi in patients with schizophrenia. Am J Psychiatry2001; 158:1717–1719.
32 Meisenzahl EM, Zetzsche T, Preuss U, et al. Does the definition of borders ofthe planum temporale influence the results in schizophrenia? Am J Psychiatry2002; 159:1198–1200.
33 Meisenzahl EM, Rujescu D, Kimer A, et al. Association of an interleukin-1beta genetic polymorphism with altered brain structure in patients withschizophrenia. Am J Psychiatry 2001; 158:1316–1319.
34 Okugawa G, Sedvall GC, Agartz I. Reduced grey and white matter volumesin the temporal lobe of male patients with chronic schizophrenia. Eur ArchPsychiatry Clin Neurosci 2002; 252:120–123.
35 Rajarethinam R, DeQuardo JR, Miedler J, et al. Hippocampus and amygdalain schizophrenia: assessment of the relationship of neuroanatomy topsychopathology. Psychiatry Res 2001; 108:79–87.
36.
Suzuki M, Nohara S, Hagino H, et al. Regional changes in brain gray andwhite matter in patients with schizophrenia demonstrated with voxel-basedanalysis of MRI. Schizophr Res 2002; 55:41–54.
This paper uses VBM to evaluate regional changes in the brain in schizophrenia.Such methods will probably become more commonplace in future structural MRIstudies of schizophrenia.
37 Takahashi T, Kawasaki Y, Kurokawa K, et al. Lack of normal structuralasymmetry of the anterior cingulate gyrus in female patients with schizo-phrenia: a volumetric magnetic resonance imaging study. Schizophr Res2002; 55:69–81.
Structural and functional imaging in schizophrenia Niznikiewicz et al. 145

38 Velakoulis D, Stuart GW, Wood SI, et al. Selective bilateral hippocampalvolume loss in chronic schizophrenia. Biol Psychiatry 2001; 50:531–539.
39.
Wang L, Sarang C, Miller MI, Csernansky JG. Statistical analysis ofhippocampal asymmetry in schizophrenia. Neuroimage 2001; 14:531–545.
This paper uses a principal components analysis based on left–right asymmetryvector fields. It is a method that will probably become more commonplace in futurestructural MRI studies of schizophrenia.
40 Wible CG, Anderson J, Shenton ME, et al. Prefrontal cortex, negativesymptoms, and schizophrenia: an MRI study. Psychiatry Res 2001; 108:65–78.
41 Zuffante P, Leonard CM, Kuldau JM, et al. Working memory deficits inschizophrenia are not necessarily specific or associated with MRI-basedestimates of area 46 volumes. Psychiatry Res 2001; 108:187–209.
42 Yucel M, Stuart GW, Maruff P, et al. Paracingulate morphologic differencesin males with established schizophrenia: a magnetic resonance imagingmorphometric study. Biol Psychiatry 2002; 52:15–23.
43. .
Mathalon DH, Sullivan EV, Lim KO, Pfefferbaum A. Progressive brain volumechanges and the clinical course of schizophrenia in men: a longitudinalmagnetic resonance imaging study. Arch Gen Psychiatry 2001; 58:148–157.
This paper, published in February of 2001 and thus covering earlier data thanthose included in the present review (August 2001 to August 2002), presents acompelling finding of accelerated frontotemporal cortical gray matter decline andcortical sulcal and lateral ventricle enlargement in schizophrenia. Of note, severityof illness was associated with more accelerated changes over time. The latter maysuggest neurotoxicity of medication because higher doses of medication are oftenused in patients with more severe symptoms, or it might reflect the neurotoxicity ofpsychosis itself.
44 Lawrie SM, Whalley HC, Abukmeil SS, et al. Temporal lobe volume changesin people at high risk of schizophrenia with psychotic symptoms. Br JPsychiatry 2002; 181:138–143.
45.
Cannon TD, van Erp TG, Rosso IM, et al. Fetal hypoxia and structural brainabnormalities in schizophrenic patients, their siblings, and controls. Arch GenPsychiatry 2002; 59:35–41.
This study provides information concerning the possible effects of fetal hypoxia onstructural abnormalities in schizophrenia, in the siblings of patients withschizophrenia, and control individuals.
46 Harris JG, Young DA, Rojas DC, et al. Increased hippocampal volume inschizophrenics’ parents with ancestral history of schizophrenia. SchizophrRes 2002; 55:11–17.
47 Narr KL, Cannon TD, Woods RP, et al. Genetic contributions to alteredcallosal morphology in schizophrenia. J Neurosci 2002; 22:3720–3729.
48.
O’Driscoll GA, Florencio PS, Gagnon D, et al. Amygdala-hippocampalvolume and verbal memory in first-degree relatives of schizophrenic patients.Psychiatry Res Neuroimaging 2001; 107:75–85.
This paper, similar to that of Seidman et al. [49..], provides important newinformation regarding amygdala–hippocampal volume and deficits in verbalmemory in the first-degree relatives of patients with schizophrenia.
49. .
Seidman LJ, Faraone SV, Goldstein JM, et al. Left hippocampal volume as avulnerability indicator for schizophrenia: a magnetic resonance imagingmorphometric study of nonpsychotic first-degree relatives. Arch GenPsychiatry 2002; 59:839–849.
This paper focuses on MRI findings in the nonpsychotic first-degree relatives ofpatients with schizophrenia. It is one of the first studies to use high spatialresolution MRI to investigate a very understudied but important group of individuals– the relatives of patients with schizophrenia. Of note, the investigators foundreduced hippocampal volume in the relatives, suggesting that hippocampal volumemay be a vulnerability indicator for schizophrenia.
50 Steel RM Whalley HC, Miller P, et al. Structural MRI of the brain in presumedcarriers of genes for schizophrenia, their affected and unaffected siblings. JNeurol Neurosurg Psychiatry 2002; 72:455–458.
51.
Van Erp TGM, Saleh PA, Rosso IM, et al. Contributions of genetic risk andfetal hypoxia to hippocampal volume in patients with schizophrenia orschizoaffective disorder, their unaffected siblings, and healthy unrelatedvolunteers. Am J Psychiatry 2002; 159:1514–1520.
This paper provides important information about genetic risk and fetal hypoxia andits association with hippocampal volume reduction in patients with schizophreniaand their unaffected siblings.
52 James AC, Iavaloyes A, James S, Smith DM. Evidence for non-progressivechanges in adolescent-onset schizophrenia: follow-up magnetic resonanceimaging study. Br J Psychiatry 2002; 180:339–344.
53 Levitt JG, Blanton RE, Rochelle C, et al. Medial temporal lobe in childhood-onset schizophrenia. Psychiatry Res 2001; 108:17–27.
54 Matsumoto H, Simmons A, Williams S, et al. Superior temporal gyrusabnormalities in early-onset schizophrenia: similarities and differences withadult-onset schizophrenia. Am J Psychiatry 2001; 158:1299–1304.
55. .
Thompson PM, Vidal C, Giedd JN, et al. Mapping adolescent brain changereveals dynamic wave of accelerated gray matter loss in very earlyschizophrenia. Proc Natl Acad Sci USA 2001; 98:11651–11655.
This paper presents a new method for mapping brain changes over time andreveals a quite dynamic change of accelerated gray matter loss in very earlyschizophrenia.
56 McCreadie RG, Thara R, Padmavati R, et al. Structural brain differencesbetween never-treated patients with schizophrenia, with and withoutdyskinesia, and normal control subjects: a magnetic resonance imagingstudy. Arch Gen Psychiatry 2002; 59:332–336.
57 Andreasen NC, Arndt S, Swayze V, et al. Thalamic abnormalities inschizophrenia visualized through magnetic resonance image averaging.Science 1994; 266:294–298.
58 Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampalvolume predicts pathologic vulnerability to psychological trauma. NatNeurosci 2002; 5:1242–1247.
59 Dickey CC, McCarley RW, Shenton ME. The brain in schizotypal personalitydisorder: a review of structural MRI and CT findings. Harvard Rev Psychiatry2002; 10:1–15.
60 Mehler C, Warnke A. Structural brain abnormalities specific to childhood-onset schizophrenia identified by neuroimaging techniques. J Neural Transm2002; 109:219–234.
61 Cahn W, Hulshoff Pol HE, Bongers M, et al. Brain morphology inantipsychotic-naive schizophrenia: a study of multiple brain structures. Br JPsychiatry Suppl 2002; 43:S66–S72.
62 Salokangas RKR, Cannon T, Van Erp T, et al. Structural magnetic resonanceimaging in patients with first-episode schizophrenia, psychotic and severenon-psychotic depression and healthy controls: Results of the Schizophreniaand Affective Psychoses (SAP) project. Br J Psychiatry 2002; 181 (suppl43):S58–S65.
63 Frumin M, Golland P, Kikinis R, et al. Shape differences in the corpuscallosum in first-episode schizophrenia and first-episode psychotic affectivedisorder. Am J Psychiatry 2002; 159:866–868.
64 Gunduz H, Wu H, Ashtari M, et al. Basal ganglia volumes in first-episodeschizophrenia and healthy comparison subjects. Biol J Psychiatry 2002;51:801–808.
65 Joyal CC, Laakso MP, Tiihonen J, et al. A volumetric MRI study of theentorhinal cortex in first episode neuroleptic-naive schizophrenia. BiolPsychiatry 2002; 51:1005–1007.
66 Keshavan MS, Diwadkar VA, Harenski K, et al. Abnormalities of the corpuscallosum in first episode, treatment naive schizophrenia. J Neurol NeurosurgPsychiatry 2002; 72:757–760.
67. .
McCarley RW, Salisbury DF, Hirayasu Y, et al. Association between smallerleft posterior superior temporal gyrus volume on magnetic resonance imagingand smaller left temporal P300 amplitude in first-episode schizophrenia. ArchGen Psychiatry 2002; 59:321–331.
This study documents smaller posterior STG volume and smaller left temporalP300 in first episode patients with schizophrenia, which is not evident in firstepisode affective psychotic patients, suggesting that these anomalies are presentat first episode of illness and may be quite specific to schizophrenia.
68 Sumich A, Chitnis XA, Fannon DG, et al. Temporal lobe abnormalities in first-episode psychosis. Am J Psychiatry 2002; 159:1232–1235.
69 Szeszko PR, Strous RD, Goldman RS, et al. Neuropsychological correlatesof hippocampal volumes in patients experiencing a first episode ofschizophrenia. Am J Psychiatry 2002; 159:217–226.
70.
Lee CU, Shenton ME, Salisbury DF, et al. Fusiform gyrus volume reduction infirst-episode schizophrenia: a magnetic resonance imaging study. Arch GenPsychiatry 2002; 59:775–781.
This study is among the first to show fusiform gyrus volume reduction in firstepisode schizophrenia. Because fusiform is related to human face perception, thisfinding may underlie problems that patients with schizophrenia experience withsocial cues and interpreting facial emotions.
71 Wood SJ, Velakoulis D, Smith DJ, et al. A longitudinal study of hippocampalvolume in first episode psychosis and chronic schizophrenia. Schizophr Res2001; 52:37–46.
72 Cohen MS. Parametric analysis of fMRI data using linear systems methods.Neuroimage 1997; 6:93–103.
73 Cohen MS, DuBois RM. Stability, repeatability, and the expression of signalmagnitude in functional magnetic resonance imaging. J Magn Reson Imaging1999; 10:33–40.
74 Kodama S, Fukuzako H, Fukuzako T, et al. Aberrant brain activation followingmotor skill learning in schizophrenic patients as shown by functional magneticresonance imaging. Psychol Med 2001; 31:1079–1088.
Schizophrenia146

75 Muller JL, Roder C, Schuierer G, Klein HE. Subcortical overactivation inuntreated schizophrenic patients: a functional magnetic resonance imagefinger-tapping study. Psychiatry Clin Neurosci 2002; 56:77–84.
76 Kosaka H, Omori M, Murata T, et al. Differential amygdala response duringfacial recognition in patients with schizophrenia: an fMRI study. SchizophrRes 2002; 57:87–96.
77 Quintana J, Davidson T, Kovalik E, et al. A compensatory mirror corticalmechanism for facial affect processing in schizophrenia. Neuropsychophar-macology 2001; 25:915–924.
78. .
Weinberger DR, Egan MF, Bertolino A, et al. Prefrontal neurons and thegenetics of schizophrenia. Biol Psychiatry 2001; 50:825–844.
This paper presents a thorough and persuasive argument for the role of prefrontalcortex, and the role of catechol-O-methyl-transferase val allele in increasing the riskfor schizophrenia.
79. .
Barch DM, Csernansky JG, Conturo T, Snyder AZ. Working and long-termmemory deficits in schizophrenia: Is there a common prefrontal mechanism? JAbnorm Psychol 2002; 111:478–494.
This is a very good study conducted in a large number of individuals that carefullylooked at the contributions of prefrontal and temporal structures in workingmemory and long-term memory task, concluding that both of those structures areinvolved in supporting cognitive subroutines.
80 Zorrilla LTE, Jeste DV, Brown GG. Functional MRI and novel picture-learningamong older patients with chronic schizophrenia: abnormal correlationsbetween recognition memory and medial temporal brain response. Am JGeriatr Psychiatry 2002; 10:52–61.
81 Ramsey NF, Koning HA, Welles P, et al. Excessive recruitment of neuralsystems subserving logical reasoning in schizophrenia. Brain 2002;125:1793–1807.
82 Paulus MP, Hozack NE, Zauscher BE, et al. Parietal dysfunction isassociated with increased outcome-related decision-making in schizophreniapatients. Biol J Psychiatry 2002; 51:995–1004.
83 Honey GD, Bullmore ET, Sharma T. De-coupling of cognitive performanceand cerebral functional response during working memory in schizophrenia.Schizophr Res 2002; 53:45–56.
84 Rubia K, Russell T, Bullmore ET, et al. An fMRI study of reduced leftprefrontal activation in schizophrenia during normal inhibitory function.Schizophr Res 2001; 52:47–55.
85.
Carter CS, MacDonald AW, Ross LL, et al. Anterior cingulate cortex activityand impaired self-monitoring of performance in patients with schizophrenia:an event-related fMRI study. Am J Psychiatry 2001; 158:1423–1428.
This interesting study examined the role of ACC in error monitoring and relatedreduced activation in the ACC to reduced error sensitivity in schizophrenia.
86 Kumari V, Gray JA, Honey GD, et al. Procedural learning in schizophrenia: afunctional magnetic resonance imaging investigation. Schizophr Res 2002;57:97–108.
87 McDowell JE, Brown GG, Paulus M, et al. Neural correlates of refixationsaccades and antisaccades in normal and schizophrenia subjects. BiolPsychiatry 2002; 51:216–223.
88 Raemaekers M, Iansma JM, Cahn W, et al. Neuronal substrate of thesaccadic inhibition deficit in schizophrenia investigated with 3-dimensionalevent-related functional magnetic resonance imaging. Arch Gen Psychiatry2002; 59:313–320.
89.
Sommer IE, Ramsey NF, Kahn RS. Language lateralization in schizophrenia,an fMRI study. Schizophr Res 2001; 52:57–67.
This interesting study addressed the issue of functional laterality in schizophrenia.
90 Kircher TT, Liddle PF, Brammer MJ, et al. Neural correlates of formal thoughtdisorder in schizophrenia: preliminary findings from a functional magneticresonance imaging study. Arch Gen Psychiatry 2001; 58:769–774.
91.
Kircher TT, Liddle PF, Brammer MJ, et al. Reversed lateralization of temporalactivation during speech production in thought disordered patients withschizophrenia. Psychol Med 2002; 32:439–449.
This study, in spite of the small number of individuals studied, offers an interestingexplanation for language associative dysfunction in schizophrenia.
92 Bentaleb LA, Beauregard M, Liddle P, Stip E. Cerebral activity associatedwith auditory verbal hallucinations: a functional magnetic resonance imagingcase study. J Psychiatry Neurosci 2002; 27:110—115.
93 Shegrill SS, Cameron LA, Brammer MI, et al. Modality specific neuralcorrelates of auditory and somatic hallucinations. J Neurol NeurosurgPsychiatry 2001; 71:688–690.
94.
Wykes T, Brammer M, Mellers J, et al. Effects on the brain of a psychologicaltreatment: cognitive remediation therapy: functional magnetic resonanceimaging in schizophrenia. Br J Psychiatry 2002; 181:144–152.
This is an interesting example of using fMRI to study the effects of behavioralcognitive therapy.
95.
Stephan KE, Magnotta VA, White T, et al. Effects of olanzapine on cerebellarfunctional connectivity in schizophrenia measured by fMRI during a simplemotor task. Psychol Med 2001; 31:1065–1078.
This study, in spite of small number of individuals studied, is an interesting exampleof using fMRI to examine the effects of medication.
96 Fletcher PC, McKenna PJ, Frith CD, et al. Brain activations in schizophreniaduring a graded memory task studied with functional neuroimaging. Arch GenPsychiatry 1998; 55:1001–1008.
97 Manoach DS, Press DZ, Thangaraj V, et al. Schizophrenic subjects activatedorsolateral prefrontal cortex during a working memory task, as measured byfMRI. Biol Psychiatry 1999; 45:1128–1137.
98 Weinberger DR, Berman KF, Zec RF. Physiological dysfunction ofdorsolateral prefrontal cortex in schizophrenia, 1: regional cerebral bloodflow evidence. Arch Gen Psychiatry 1986; 43:114–124.
99 Nieman DH, Bour LJ, Linszen DH, et al. Neuropsychological and clinicalcorrelates of antisaccade task performance in schizophrenia. Neurology2000; 54:866–871.
100 Park S, Holzman PS. Association of working memory deficit and eye trackingdysfunction in schizophrenia. Schizophr Res 1993; 11:55–61.
101 Nakashima Y, Momose T, Sano I, et al. Cortical control of saccade in normaland schizophrenic subjects: a PET study using a task-evoked rCBFparadigm. Schizophr Res 1994; 12:259–264.
102 Crawford TJ, Puri BK, Nijran KS, et al. Abnormal saccadic distractability inpatients with schizophrenia: a 99mTc-HMPAO SPET study. Psychol Med1996; 155:1703–1710.
103 Faust M. Chiarello C. Sentence context and lexical ambiguity resolution bythe two hemispheres. Neuropsychologia 1998; 36:827–835.
104 Beeman M, Friedman RB, Grafman J, et al. Summation priming and coarsesemantic coding in the right hemisphere. J Cogn Neurosci 1994; 6:26–45.
105.
Lawrie SM, Buechel C, Whalley HC, et al. Reduced frontotemporalfunctional connectivity in schizophrenia associated with auditory hallucina-tions. Biol Psychiatry 2002; 51:1008–1011.
In spite of the limited number of individuals assessed, this interesting study showsboth lack of hypofrontality in a task in which both groups performed at acomparable level, and evidence for abnormal fronto-temporal connectivity in thepatients, especially in those who were hallucinating.
106 Ford JD, Mathalon DH, Whitfield S, et al. Reduced communication betweenfrontal and temporal lobes during talking in schizophrenia. Biol Psychiatry2002; 51:485–492.
107 Horwitz B, Duara R, Rapoport SI. Inter-correlations of glucose metabolicrates between brain regions: application to healthy males in the state ofreduced sensory input. J Cereb Blood Flow Metab 1984; 4:484–499.
108 Horwitz B, Rumsey JM, Donohue BC. Functional connectivity of angulargyrus in normal reading and dyslexia. Proc Natl Acad Sci USA 1998;95:8939–8944.
109 Hofer A, Weiss EM. Advances in the neuroimaging of cognitive functions inschizophrenia. Curr Opin Psychiatry 2002; 15:3–7.
110 Buchsbaum MS, Tang CY, Peled S, et al. MRI white matter diffusionanisotropy and PET metabolic rate in schizophrenia. NeuroReport 1998;9:425–430.
111 Lim KO, Hedehus M, Moseley M, et al. Compromised white matter tractintegrity in schizophrenia inferred from diffusion tensor imaging. Arch GenPsychiatry 1999; 56:367–374.
112 Foong J, Maier M, Clark CA, et al. Neuropathological abnormalities of thecorpus callosum in schizophrenia: a diffusion tensor imaging study. J NeurolNeurosurg Psychiatry 2000; 68:242–244.
113 Foong MR, Symms GJ, Barker M, et al. Investigating regional white matter inschizophrenia using diffusion tensor imaging. NeuroReport 2002; 13:333–336.
114 Agartz I, Andersson JL, Skare S. Abnormal brain white matter inschizophrenia: a diffusion tensor imaging study. NeuroReport 2001;12:2251–2254.
115 Steel RM, Bastin ME, McConnell S, et al. Diffusion tensor imaging (DTI) andproton magnetic resonance spectroscopy (1H MRS) in schizophrenicsubjects and normal controls. Psychiatry Res 2001; 106:161–170.
116. .
Kubicki M, Westin CF, Maier S, et al. Uncinate fasciculus findings inschizophrenia: a magnetic resonance diffusion tensor imaging study. Am JPsychiatry 2002; 159:813–820.
This interesting study used DTI to examine the largest white matter fiber tractconnecting the frontal and temporal lobe, namely the uncinate fasciculus. Findingsof abnormal asymmetry suggest that fronto-temporal connections may bedisrupted in schizophrenia.
Structural and functional imaging in schizophrenia Niznikiewicz et al. 147