Embed Size (px)
DESCRIPTION
The benefits of reducing health inequalities are economic as well as social. As the Marmot Report shows, the costs of health inequalities can be quantified in human terms, years of life lost and years of active life lost; and in economic terms, by the cost to the economy of additional illness. Karsten Stampa, team member of Clear Village Charitable Trust, met Ms. Ilaria Geddes who is part of the Marmot Review research team and responsible for observing the operationalisation of suggested policy recommendations.
Citation preview

DNA FOR 21ST CENTURY DWELLING
RECODE
INEQUALITIES
HEALTH
A CLEAR VILLAGE DISCUSSION WITH THE UNIVERSITY COLLEGE LONDON,ILARIA GEDDES, DPT. OF PROF SIR MICHAEL MARMOT LONDON, 18-20 MAY 2010
PUT CAUSES OF HEALTH INEQUALITIES IN FOCUS, NOT THEIR SYPTOMS!

©C
LEA
R V
ILLA
GE
2010
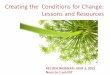
figure 2: Populations living in areas with, in relative terms, the least favourable environmental conditions, 2001-6
‘Inequalities are a matter of life and death, of health and sickness, of well-being and misery. The fact that in England today people in different social circumstances experience avoidable differences in health, well-being and length of life is, quite simply, unfair. Creating a fairer society is fundamental to improving the health of the whole population and ensuring a fairer distribution of good health.’ states Prof Sir Michael Marmot, chair of the Strategic Review of Health Inequalities in England Post-2010, in his Review Report*.
THE CONTEXTThe Marmot Review - in 2008, Professor Sir Michael Marmot was asked by the former Secretary of State for Health to chair an independent review to propose the most effective evidence-based strategies for reducing health inequalities in England from 2010, incl. following tasks (shortened):• identify the evidence most relevant to
underpinning future policy and action• show how this evidence could be
translated into practice• advise on possible objectives and
measures• publish a report of the Review’s work.
SOCIAL GRADIENT IN HEALTH The Marmot Review clearly shows that the lower one’s social position, the worse his health. To cite the report it can be stated that in ‘England, people living in the poorest neighbourhoods, will, on average, die seven years earlier than people living in the richest neighbourhoods’ as following figure shows:
figure 1: Life expectancy and disability-free life expectancy (DFLE) at birth, persons by neighbourhood income level, England, 1999-2003
In turn we can say that health inequalities result from social inequalities, e.g. from early child development & education, employment & working conditions, housing & neighbour-hood conditions, standards of living and lack of freedom to participate equally in benefits of society.
HEALTH & WELL-BEINGHealth inequalities, as described above, do not arise by chance. Bad as those factors might be, inequalities can not be attributed simply to genetic makeup, bad and unhealthy behaviour (smoking, junk food) or people’s access to medical care. Social and economic differences in health status reflect and are caused by social and economic inequalities in our society. These inequalitites are influenced by a range of interacting factors that shape health & well-being, e.g. material circumstances, the social environment, psychosocial factors, behaviours and biological factors; which are,
in turn, shaped by people’s social position which is grown by education, occupation, income, gender, ethnicity and race. All these influences are set in a socio-political, cultural and social framework.To pick just one example, there is empirical evidence that the more deprived areas are that people live in, the more environmental conditions can be found in those areas that might influence inhabitant’s health.
As a recommendation, the Review states that to focus solely on the most disadvantaged will not reduce health inequalities. Actions must be universal with a scale and intensity that is proportionate to the level of disadvantage.
*Information, pictures and visualisations sourced from: The Marmot Review - Strategic Review of Health Inequalities in England Post-2010
THE MARMOT REVIEW -a clear village discussion

©C
LEA
R V
ILLA
GE
2010
Figure 10 Populations living in areas with, in relative terms, the least favourable environmental conditions, 2001–6
executive summary — 1
photo: Gary Sludden/Getty Images
Least favorable conditions100
90
80
70
60
50
40
30
20
10
0
Least deprived areasLevel of deprivation
Percentage of the population
Most deprived areas
No conditions
1 condition
2 conditions
3 or more conditions
Least favorable conditions100
90
80
70
60
50
40
30
20
10
0
Least deprived areasLevel of deprivation
Percentage of the population
Most deprived areas
No conditions
1 condition
2 conditions
3 or more conditions
Least favorable conditions100
90
80
70
60
50
40
30
20
10
0
Least deprived areasLevel of deprivation
Percentage of the population
Most deprived areas
No conditions
1 condition
2 conditions
3 or more conditions
Least favorable conditions100
90
80
70
60
50
40
30
20
10
0
Least deprived areasLevel of deprivation
Percentage of the population
Most deprived areas
No conditions
1 condition
2 conditions
3 or more conditions
Least favorable conditions100
90
80
70
60
50
40
30
20
10
0
Least deprived areasLevel of deprivation
Percentage of the population
Most deprived areas
No conditions
1 condition
2 conditions
3 or more conditions
Environmental conditions: river water quality, air quality, green space, habitat favourable to bio-diversity, flood risk, litter, detritus, housing conditions, road accidents, regulated sites (e.g. landfill)
Source: Department for Environment, Food and Rural Affairs23
Low Q at 22m0
10
20
30
40
50
60
70
80
90
100
22 26 30 34 38 42 46 50 54 58 62 66 70 74 78 82 86 90 94 98 102 106 110 114 118
Months
Average position in distribution
High Q at 22mHigh socioeconomic statusLow socioeconomic status
Note: Q = cognitive score Source: 1970 British Cohort Study17
Figure 6 Inequality in early cognitive development of children in the 1970 British Cohort Study, at ages 22 months to 10 years
executive summary —
photo: Bromley by Bow Centre
Low Q at 22m0
10
20
30
40
50
60
70
80
90
100
22 26 30 34 38 42 46 50 54 58 62 66 70 74 78 82 86 90 94 98 102 106 110 114 118
Months
Average position in distribution
High Q at 22mHigh socioeconomic statusLow socioeconomic status
WELL-BEING & ECONOMYThe benefits of reducing health inequalities are economic as well as social. As the report utters, costs of health inequalities can be quantified in human terms, years of life lost and years of active life lost; and in economic terms, by the cost to the economy of additional illness. Referring back to fig. 1 and the DFLE curve and its levels of disability shown, more than three-quarters of the population do not have disability-free life expectancy as far as the age of 68, which is currently discussed as the prospective pension age in England. The Marmot review argues that ‘if society wishes to have a healthy population, working until 68 years, it is essential to take action to both raise the general level of health and flatten the social gradient.’
BEYOND ECONOMIC GROWTH We agree with the Review in another point: it is indeed time to move beyond economic growth as the sole measure of social success; a holisticly observed well-being should be a more important societal goal than simply more economic growth. Climate change and all actions taken against it have the worst effects on the poorest and most vulnerable
people globally. The Marmot team thinks that action to reduce health inqualities is completely compatible with action to create sustainable futures. Fostering sustainable local communities, active transport, healthy food production, zero-carbon houses will not only ensure the future of manhood but also have health benefits across society!
POLICY RECOMMENDATION Based on the evidence the research team has assembled their recommendations are grouped into six policy objectives, which are underpinned by policy mechanisms, e.g. considering equality and health equity in all policies, across the whole of government, not just the health sector: • Give every child the best start in life• Enable all children, young people and
adults to maximise their capabilities and have control over their lives
• Create fair employment & good work for all
• Ensure a healthy standard of living for all• Create and develop healthy and
sustainable places and communities• Strengthen the role and impact of ill-
health prevention
*Information, pictures and visualisations sourced from: The Marmot Review - Strategic Review of Health Inequalities in England Post-2010
THE MARMOT REVIEW -a clear village discussion
HIGHLIGHTS OF OUR DISCUSSIONKarsten Stampa, team member of Clear Village Charitable Trust, met Ms. Ilaria Geddes who is part of the Marmot Review research team and responsible for observing the operationalisation of suggested policy recommendations. We discussed Clear Village’s view on the Marmot Review and its policy recommendations intensively, especially our holistic view on societal well-being, the importance of economic growth in today’s global and political setting.It came to fore that we completely share the holistic view of the Review, which goes far
beyond the border of pure health issues, and that Clear Village would be able to assist the implementation process with our co-creative methodology especially in creating and developing healthy and sustainable places and communities, to improve communities’ well-being thus diminish health inequalities.In the end we invited Ilaria to our network of experts and agreed on a partnership between the UCL department & Clear Village.
MORE INFORMATION+ Marmot Review website: www.marmotreview.org+ UCL / Marmot Department website: www.ucl.ac.uk/gheg/marmotreview
Photo: Anthony Strack/Getty Images
50
70
90
110
130
150
170
190
Standardised Mortality Rate
I II IIIN IIIM IV V I II IIIN IIIM IV V
Social Class
Employed in 1981 Unemployed in 1981
Source: Office for National Statistics Longitudinal Study19
Figure 8 Mortality of men in England and Wales in 1981–92, by social class and employment status at the 1981 Census
executive summary —
photo: NHS South West
0
100
200
300
400
500
600
700
800
Region
Semi-routine
Lower supervisory & technical
Small employers, own account workers
Intermediate
Lower managerial, professional
Higher managerial, professional
Mortality rate per 100,000
Routine
England & Wales
0
100
200
300
400
500
600
700
800
Region
Semi-routine
Lower supervisory & technical
Small employers, own account workers
Intermediate
Lower managerial, professional
Higher managerial, professional
Mortality rate per 100,000
Routine
England & Wales
Source: Office for National Statistics51
Figure 2.6 Age standardised mortality rates by socioeconomic classification (NS-SEC) and region, men aged 25–64, 2001–2003
: health inequalities and the social determinants of health —
NHS Portsmouth City PCT
0
100
200
300
400
500
600
700
800
Region
Semi-routine
Lower supervisory & technical
Small employers, own account workers
Intermediate
Lower managerial, professional
Higher managerial, professional
Mortality rate per 100,000
Routine
England & Wales
0
10
20
30
40
50
Bottom 2nd 3rd 4th Top
Quintile of household equivalised disposable income
Percent
All indirect taxes
All direct taxes
0
10
20
30
40
50
Bottom 2nd 3rd 4th Top
Quintile of household equivalised disposable income
Percent
All indirect taxes
All direct taxes Source: Office for National Statistics21
Figure 9 Taxes as a percentage of gross income, by quintile, 2007/8
executive summary —
photo: NHS South WestProf. Sir Micheal Marmot

THE MARMOT REVIEW - POLICY RECOMMENDATIONS
A - Give every child the best start in life
A1: increase proportion of overall expenditure allocated to early years
A2: support families to achieve progressive improvements in early year development• priority to pre- & post natal
interventions• providing paid parental
leave• provide routine support to
families through parenting programmes
• develop programmes for transition to school
A3: provide good quality early years education & childcare• combined with outreach
to increase take-up by children
• provided on basis of evaluated models & meet quality standards
B - Enable all children, young people & adults to maximise their capabilities and have control over lifeB1: reducing social inequalities in pupil’s education
B2: reducing social inequalities in life skills• extend role of school
supporting families and communities, taking the ‘whole child’ approach
• implementation of full range of extended services in & around schools
• develop school-based workforce across school-home boundaries
B3: Increase access and use of life-long learning • providing support and
advice for 16-25 year olds• providing work-based
learning for young people• increasing availability of
non-vocational life-long learning
C - Create fair employment and good work for all
C1: Prioritise active labour market programmes
C2: Implementation of measures to improve quality• public & private sector
adhere to guidance & legislation
• guidance on stress management, wellbeing, physical & mental health
C3: Develop greater security and flexibility in employment • retirement age• encouraging employers
to create jobs suitable for lone parents, carers and disabled
D - Ensure healthy standard of living for all
D1: Develop & implement standards for a minimum income for healthy living
D2: review and implementation of systems of taxation, benefits, pensions, tax credits to provide minimum standard of healthy living
D3: remove ‘cliff edges’ for those moving in and out of work
E - Create and develop healthy & sustainable places and communities
E1: Prioritise policies & interventions that reduce health inequalities and mitigate climate change• improve active travel• improve open & green
space• improve food environment• improve energy-efficiency
of housing
E2: fully integrate planning, transport, housing, environment, health systems in each locality
E3: support locally developed and evidence-based community regeneration programmes that• remove barriers to
community participation• reduce social isolation
F - Strengthen the role and impact of ill health prevention
F1: Prioritise investment in ill health prevention & health promotion across government departments
F2: implement evidence-based programmes of ill health prevention• scale & quality of drug
treatment programmes• focussing on public health
interventions such as smoking cessation
• improving programmes to address causes of obesity
F3: Focus core efforts of public health departments on effective interventions related to the social determinants of health
communitywell-being