Embed Size (px)
Citation preview
Recognition and Treatment of a Hidden Problem
North Bay Literacy Council – Literacy and Health Presentation
Funding for the Literacy & Health Project
This project is funded by the Ontario Trillium Foundation, from the Ministry of Culture
The project provides funding for one year (December 2006-2007)
One person for three days per week
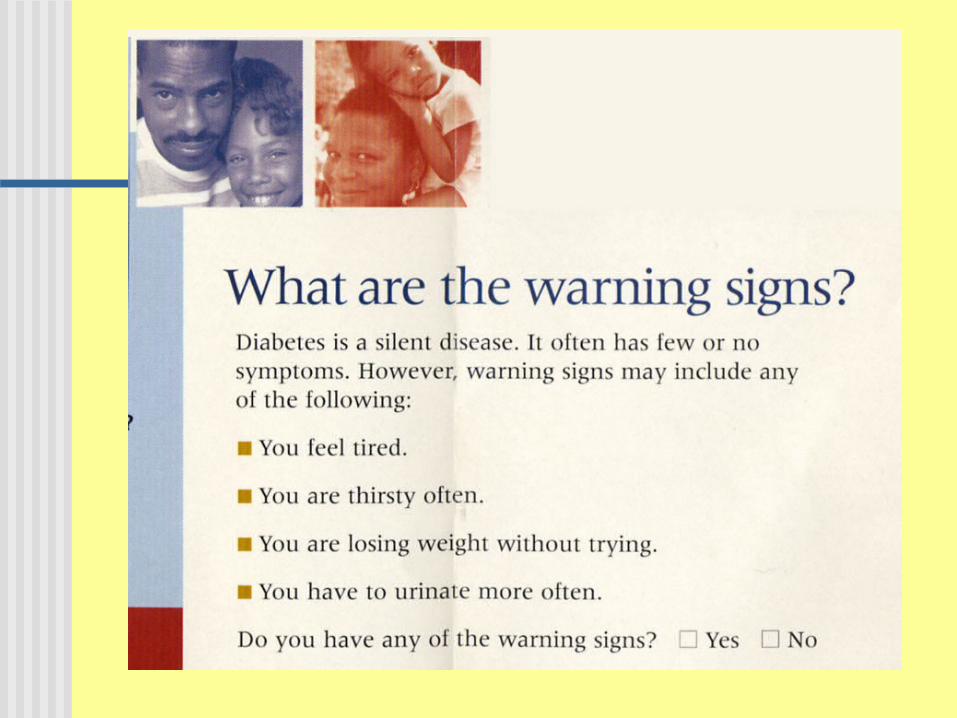
Do you know?
Which of the following is the strongest predictors of an individual’s health status?
A) AgeB) IncomeC) Literacy skillsD) Education level E) Racial or ethnic groupF) Average Beer Intake at Metro
Do you know?
Which of the following is the strongest predictors of an individual’s health status?
A) AgeB) IncomeC) Literacy skillsD) Education level E) Racial or ethnic groupF) Average Beer Intake at Metro
True or False? Most people with limited literacy
have low IQs. People will tell you if they have
trouble reading. The number of years of schooling is
a good general guide to determine literacy level
Most people with low literacy skills are poor, immigrants or minorities.
Goals of the Presentation Recognize the scope and
implications of health literacy issues. Identify and implement strategies to
enhance patient understanding. Learn to evaluate health care
literature and documentation Referral process for clients who want
help in the community.
Health Literacy
Health literacy is the degree to which people are able to access, understand, appraise and communicate information to engage with the demands of different health contexts in order to promote and maintain good health across the life-course.
Types of Illiteracy Functional illiteracy Sensory/physical illiteracy Cultural/language illiteracy Psychological illiteracy Computational illiteracy
Functional Literacy Ability to read, write and speak in
English Compute and solve problems at
levels of proficiency necessary to function in society
Ability to achieve one’s goals and develop one’s knowledge and potential
Physical Literacy Sensory
Visual Hearing Neurological
Psychological / Mental Health Other physical
Metabolic Endocrine
Cultural/Language Non-English speaking Immigrant status Ethnic interpretation of illness Spiritual and religious beliefs Majority of the lowest level readers
are white and native born
Computational – Health Numeracy
The degree to which individuals have the capacity to access, process, interpret, communicate, and act on numerical, quantitative, graphical, biostatistical, and probabilistic health information needed to make effective health decisions
Computational Numeracy
The ability to count, quantify, compute, and otherwise use simple manipulation of numbers, quantities, items, or visual elements in a health context so as to function in everyday situations. An example would be using nutritional labels correctly
Analytical Numeracy
This involves the ability to make sense of information, as well as higher functions like inference, estimation, proportions, percentages, frequencies, and equivalent situations. Information may be from multiple sources, and an example would be determining whether an analytical result was within the normal range, or understanding graphs
Statistical Numeracy
An understanding of basic biostatistics involving probability statements, skills to compare different scales (Probability, proportion, percent), to critically analyze quantitative information like life expectancy or risk, and understanding concepts like randomization and blinding. An example would be making choices between treatments based on standard outcomes of relative or absolute risk
Scope of the Problem LBS (Literacy Basic Skills)- Level 1 22% of adult Canadians are so limited
that they are unable to determine the correct dosage from reading the medicine label.
LBS (Literacy Basic Skills)- Level 2 A further 26% can read provided that the
materials are simple and presented in a familiar context.
LBS – Literacy Basic Skills
There are five levels The levels provide a summary of
skills for each level of written, verbal innumeracy outcomes
It offers a common language to describe learner levels and outcomes
LBS- Level 1 Indicates very low literacy skills where the
individual may, for example have difficulty identifying the correct amount of medicine to give a child from the information found on the package. These individuals are generally aware they have a problem
LBS Level One Grade 1-2 Can
Sign name Find expiration date on license Total bank deposit entry
Can’t Use bus schedule, find intersection on map Fill out health history form Total costs on an order form Can’t read a simple story to a child
LBS Level 2 Respondents can deal with material that
is simple, clearly laid out and in which the tasks involved are not too complex. This is significant because it identifies people who may have adapted to everyday life, but would have difficulty learning new health related material and making informed decisions. These individuals often do not recognize their own limitations.
LBS Level Two Grade 2-3 Can
Find intersection on map Locate info in news article Tell difference in two ticket prices (compare
and contrast) Can’t
Use bus schedule Read a bar graph Write a letter of complaint
What Happens? Problems with: Navigating from one clinic to
another Completing forms Following medication instructions Interactions with providers Coping strategies in general
What Happens? Limited general knowledge (Health
promotion & prevention) Do not ask for clarification Focus on details, hard to get them to
prioritize Don’t understand Likert scales, math Deal in literal/concrete concepts, not
abstract Essential vocabulary only Check answers without understanding
Why worry?
Not keeping appointments—26% Unable to find clinic/office Failure to take meds correctly—42% did
not understand “empty stomach” Incomplete history Overuse of emergency room Lack of informed consent Diagnosis made at later stages Unhealthy/risky behaviors
More reasons More than 80% of Canadians over 65
have low literacy skills and are unable to cope with the demands of everyday life and work.
Seniors with low literacy are more likely to have health problems than seniors with high literacy abilities
Non compliance can be life threatening
The elderly Fewer years of schooling, poorer—fixed
incomes > 50% do not take meds as directed 68% cannot interpret blood sugar value 76% cannot follow Upper GI instructions 2 billion dollars spent per year on hospital
admission for medication errors
Oh, I can tell…Oh no you can't
If you can tell which patients are illiterate, you are doing better than trained physicians
Shame and stigma therefore… 67% have never told their spouses
and 19% never told anyone
More on Identifying Forgot their glasses Eyes wandering over page, very slow to
finish, sounding out words, look confused NEVER ask “How well do you read.” Response will be: - Feign anger- Walk out rather than admit it.- If a person acts out, be curious.
More on Identifying 98% will bring someone with them
who read. 88% will watch others or copy. 90% will ask for help from the staff(front desk person) 80% will ask for help from other
patients. Take forms home to complete
More on Identifying Read too slowly or too quickly Ask a lot of questions or none Frequently use health care system Routinely miss scheduled
appointments Never refer to written information
they have received Non-compliance with directions
Who Are They? Not stupid All social classes No racial/ethnic bias Amazing ability to function
Literacy Tests
Always assume and ask in sensitive way—”How do you like to get your information?” or “What things do you like to read?” or “How satisfied are you with how you read?” Treat all the same.
So, do I test them? Time/place/training Confidentiality and ethics Cost Reliability and validity Timing re: patient Age, sight, hearing, cognitive Language
What to do Whole staff must be aware and sensitive Speak slowly and start with context Quiet room with minimal distractions Use monosyllabic and colloquial terms—avoid
technical terms. Be concrete and use active voice.
Start with the most important information first and limit new information
No more than one or two instructions at a time—and check on each as you go: “Chunks and Checks”
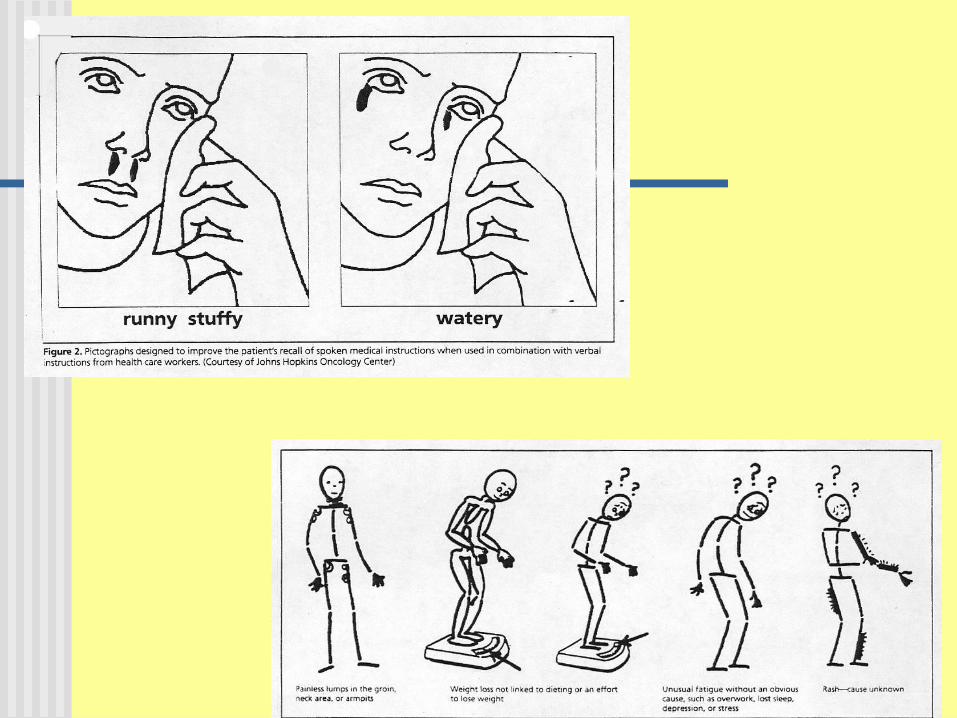
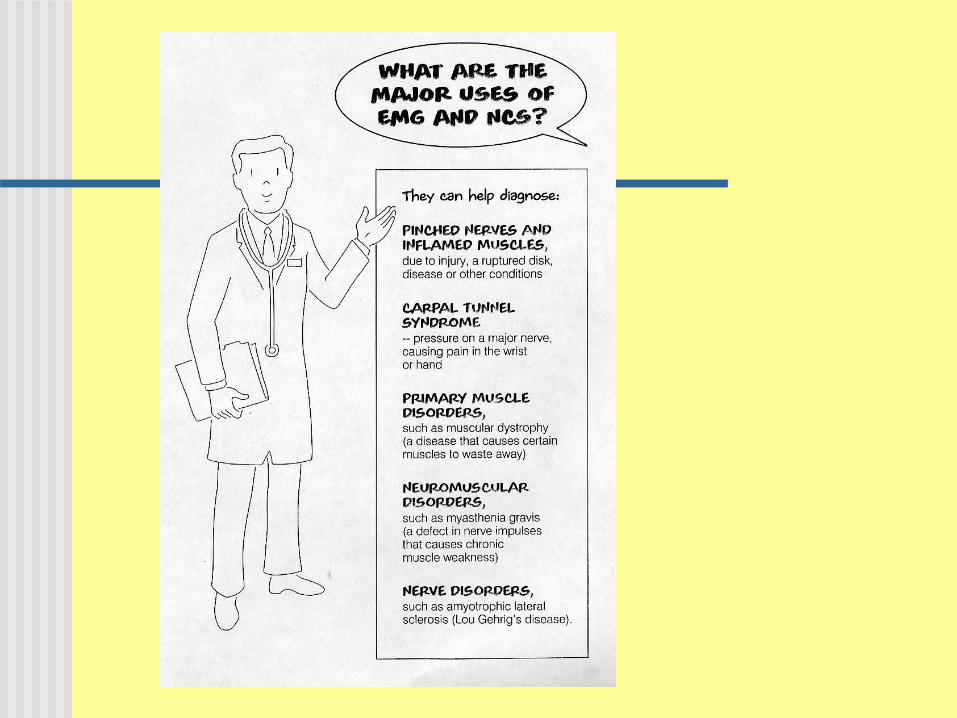
More hints Use repetition Have the patient repeat the information Use the “teach back” method Never ask “Do you understand?” Use models, sketches, pictures, symbols
demonstrations Consider follow up phone calls Give instructions to several of family
members If you are rushed, get someone else to do
it
More interventions Know what languages and cultures you
will encounter in your community-know what resources you will need
Check the reading level of materials you give to patients
Consider referring your patient to the North Bay Literacy Council
Develop partnerships between the health and literacy sectors
Work with your schools to get health education into the K—12 curriculum
Printed Materials (Secondary to Verbal) Use pictures, photos, videos and other visuals—
including med charts Monosyllabic and simple language Read over the instructions—highlight important
parts with color Lots of white space Review materials for literacy level—rewrite as
necessary, ask patients for help Writing style should be clear, concise, organized,
and jargon-free
Assessing level of literature Most pamphlets at 10-12th grade
level Informed consents at 14.3—16th
grade level Internet health resources at similar
grade levels SMOG
Speaking Plainly Request and respect patients prior
knowledge, opinion and experience Speaking plainly is as important as writing
plainly Avoid jargon Use everyday examples to explain
technical or medical terms Teach in an organized manner Use the “interactive communication loop”
Legal issues Informed consent and living wills need
post-college level comprehension Must explain verbally as well as give
written—just handing them the form to sign is not informed consent
Legal right to understand alternatives for care and risk of care
Avoid legal jargon/keep short
It is all of these things that have made them what they are and these are the things that you cannot come to know
by hearsay; you can only know them if you have lived them.”
Somerset Maughan, The Razor’s Edge (Introduction), 1944.
To Conclude
“ …follow the counsel of Aristotle, to speak as the common people do, to think as wise men do; and so should every man understand him, and the judgment of wise men follow him.”—
Roger Ascham (1515-1568)





























