Embed Size (px)
Citation preview

Recognizing and Reporting Possible Disasters
Modules were developed as part of a grant from the HRSA BTCDP initiative
Basic Biodefense Curriculum Module 22005

Goal of the Module
To prepare students to: Find current information about the signs and
symptoms of exposure to various agents Use information to determine whether they need to
report a suspicious event.

Identify or list examples of agents within each CBRNE (or B-NICE) category
Describe the typical signs and symptoms for each class of agents
Explain how healthcare workers participate in surveillance and monitoring
Describe where to find current and accurate information about CBRNE (or B-NICE) agents
Use algorithms to guide information collecting and reporting
Describe how a suspicious event is reported
Learning Objectives

Disaster Timeline
Early recognition to mitigate (reduce) scope or impact of a full-blown disaster could be considered either a PREVENTION or an early RESPONSE activity.
1. Prevent

Early Recognition
Need to have an approach for deciding when to report a suspected public health threat
Be familiar with natural and accidental risks to your community
Be familiar with agents used to intentionally cause disasters

“The Usual Suspects” Agents Commonly Used as Weapons
B-NICE [bee-nice]:BiologicalNuclear (radioactive)Incendiary (fire)
ChemicalExplosive
CBRNE [see-burn]:ChemicalBiologicalRadioactiveNuclearExplosive
Types of agents and two ways to remember them!

Categorized by Ease of Detection
Overt (Obvious) Agents: Explosives Incendiaries
Covert (Hidden) Agents: Biologicals Chemicals Radioactive materials
Overt – Covert Combinations: Dirty bombs (explosives
with radioactive materials)
???

“E” Explosives
Most commonly used weapon of terror Used in 70% of attacks
Difficult to detect PRIOR to detonation
Blast injuries may be: Immediate or delayed Obvious or hidden

“I” Incendiary Devices
Three Parts of an Incendiary Device: Igniter (fuse) Container (body) Incendiary material (filler)
Injuries caused by: Burns Inhaled smoke and toxic fumes
Injuries usually occur soon after exposure

”E” and “I”… A Deadly Duo
Explosives often cause fires Fires often cause explosions
Watch for injuries and symptoms of both
Could it be a Triple Threat…?Assume a COVERT agent was released by
fire or explosion• Watch for unusual symptoms

Why Terrorists like Covert Agents
DELAYED onset and detection Terrorist escapes before attack detected False claims can be made Accidental secondary exposures
VAGUE, MILD early symptoms Delays in seeking care Early diagnosis is difficult
DETERMINATION is difficult: Causes speculation and panic
Follow the spores…
Psst…Sore Throat. Where should I look?**
**With apologies to Woodward and Bernstein

“C” Chemical Agents
Five Categories of Chemical Agents:
1. Nerve
2. Blister (or Vesicant)
3. Blood
4. Choking
5. Irritants

Chemical Agents
Examples of two-letter codes:Sarin (GB) – nerve agentMustard gas (H or HD) – blister agentCyanide (AC) – blood agent
What are the chemical risks in your community?

“C” Nerve Agents
Chemical agents in this class:Sarin (GB)Soman (GD)Tabun (GA)Agent V (VX) – most potent

“C” Nerve Agents
Rapid onset and often fatal
Signs of nerve agent release Dead animals, birds, or
humans Symptoms like
organophosphate pesticide poisoning
• Body produces excessive secretions (see S.L.U.D.G.E.)
S.L.U.D.G.E. Salivation Lacrimation Urination Defecation GI upset Emesis (or
pulmonary Edema)

“C” Blister Agents
Also called vesicants Example:
Mustard Gas (H, HD) Lewisite (L)
Prevent DNA from working, which kills the cells in the body
Symptoms depend on route of exposure Eyes and lungs most vulnerable Mimics severe burns

Blood Agents Example:
Cyanide (AC) Cyanogen (CK)
Interferes with oxygen transport in cells, which leads to cell death
Symptoms: cyanosis (blue lips, fingers), difficulty breathing, dizziness, headache

Choking Agents
Examples: Chlorine gasPhosgene gas
Suffocation by drowning in own fluids
Symptoms: Inability to breathe Eye irritation

Irritating Agents
Example: Tear gasMACE
Rarely lethal, but can be quite disruptive
cough…. ….cough …

“B” Biological Agents
Two Main Types of Agents: Toxic by-products that act as poisons Microorganisms that cause infectious disease
Bioterrorism: the use of biological toxins or infectious organisms in acts of terrorism Natural outbreaks of infectious disease have many of
the same characteristics

“B” Toxic Biologicals
Similar to Chemical AgentsSecondary exposures from contaminated
items or peopleDo NOT cause infections
Examples:Botulinum toxin Ricin

“B” Toxic Biologicals
Botulinum toxinProduced by Clostridium botulinum bacteriaGroup of several neurotoxic proteinsCauses descending paralysisOnset in 12-36 hours after ingestionEarly Signs:
• droopy eyelids, blurred vision, slurred speech

“B” Toxic Biologicals
RicinDerived from Castor Bean processing
wastesPrevents protein synthesis in cellsOnset and early signs: vary by route of
exposureMore likely used for assassinations than
large scale attacks

“B” Infectious Biologicals
Cause death through infection, not poisoning• Disease may spread to others causing secondary
outbreaks
Attack may mimic a natural outbreak
Onset of symptoms often delayed• Incubation period may take days
Fear that organisms will be altered genetically• Usual treatment or vaccine may not be effective

CDC CATEGORY A
Anthrax (Bacillus anthracis) Botulism (Clostridium botulinum toxin) Plague (Yersinia pestis) Smallpox (Variola major virus) Tularemia (Francisella tularensis) Viral hemorrhagic fevers
• Filoviruses [e.g., Ebola, Marburg] • Arenaviruses [e.g., Lassa, Machupo]
Biologicals most likely to be used as weapons; virulent or easy to disseminate.

CDC CATEGORY B
Brucellosis (Brucella species) Q fever (Coxiella burnetii) Ricin toxin (Castor Bean) Staphylococcal enterotoxin Cholera (Vibrio cholerae) Cryptosporidiosis (Cryptosporidium parvum)
Biologicals that are also potential weapons, but not as virulent as Category A.
(Includes food and water contaminants)

CDC Category C
Hantavirus Nipah virus Other emerging pathogens
Go to CDC website for more information on particular biological agents
Biologicals that are emerging pathogens; not yet of concern, but have potential to become weapons

Symptoms of “B” Exposure
Varies by ROUTE of exposure Topical: skin lesions Inhaled: respiratory symptoms Ingested: gastrointestinal symptoms Injected: systemic, whole body
Forms of infectious diseases based on route: Anthrax
• Topical Anthrax (also called Wool Sorters’ Disease)• Gastrointestinal Anthrax (swallow spores)• Inhalational Anthrax (inhale spores; most deadly form)

Early symptoms – vague, nonspecific Influenza-like Illnesses (ILI)
Late symptoms – more specific, diagnostic, laboratory confirmation
Can you distinguish between the early symptoms of common cold and influenza?
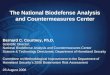
HealthyAcute illness:Disease-specific
symptoms appear
Subclinical:Organisms multiply,
but not yet impacting body
Exposure
Usual contagious period
Recovery:No new symptoms,existing symptoms
resolve, health returns
Healthy(or dead)
Time
Prodromal:Early,
nonspecificsymptoms
appear
HealthyAcute illness:Disease-specific
symptoms appear
Subclinical:Organisms multiply,
but not yet impacting body
Exposure
Usual contagious period
Recovery:No new symptoms,existing symptoms
resolve, health returns
Healthy(or dead)
Time
Prodromal:Early,
nonspecificsymptoms
appear
Timeline for Biological Exposure Symptoms

“R” Radioactive Agents
Radioactive Agents Types of Radiation:
Alpha Beta Gamma
Sources of Exposure: Nuclear bomb Conventional explosives Accidental release

Radioactive Agents

Detecting Radioactive Agents
Look for labels on containers Placards on transportation vehicles
Location Site may contain nuclear or
radioactive products.
Instruments designed to detect radiation: Geiger Counters

Decision-Making Tools
Available in many formats
Provide quick, but not necessarily complete information
Fit many, but not all situations• Still need to use your judgment

Decision-Making Tools CDC: http://www.bt.cdc.gov
SARIN – NIOSH Emergency Response Card Recognizing Chemical Exposure Anthrax – Case definition is found in “Diagnosis
and Evaluation”
US Army (has PDA downloads): http://www.usamriid.army.mil/education/bluebook.htm Isolation Precautions (Found in Appendix B) Differential diagnosis of chemical vs toxin
(Appendix H) (Army procedures may vary from civilian
procedures)

Symptom Approach

Practice Case
Location: Near a Warehouse Fire
Symptoms: No fever Cough and shortness of breath Skin lesions (burns) No GI symptoms
Fever
Breathing
Skin
GI Tract
No
No
Yes
Yes

Epidemiological Approach
Are any of these unusual? Time of Year Combination of symptoms Timing of symptoms Type of population affected Cluster of cases in one area Outbreaks or exposure in other areas

Epidemiological Approach
Approach based on: Knowledge of natural behavior of disease
• Know common diseases (e.g., influenza, chickenpox) Case definitions
• Use descriptions of symptoms and causative agents
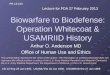
Simplified example of how a naturally-occurring disease outbreak might spread from an initial (index) case to close contacts and result in an epidemic.
Index Case

Epidemiological Approach
Gather the following information: Contact information (phone numbers, names) Onset date/time Signs and symptoms Illness in family or acquaintances Recent travel Recent events and activities Food and water sources Animals Unusual packages and envelopes

Seek Information About
Exposure risk Early symptoms Specific symptoms
Transmission Vulnerable
populations

Another Practice Case: Three days after the Fourth of July weekend, Alice, Burt
and Charlie complain that they had the “flu.”
Their early symptoms included severe fever with chills, aching muscles, no energy, and a dry cough, but after several days, they began to feel better.
What type of exposure could this be? Epidemiology approach: July is unusual time of year and no one
else appears to be sick Symptom approach: fever indicates infection or radiation. Other
symptoms very vague or “I-L-I” like Decision: unusual isolated outbreak of infections that should be
checked by physician.

Validating Your Suspicions
Seek more detailed information• Were the three individuals at the same get together – is
there a common source?
Check with colleagues about similar cases• Have other providers heard similar stories from other
patients?
Stick to the facts – avoid starting rumors• Let colleagues know you have an unusual case that you
are checking out

Reporting Unusual Cases
For a public health emergency, you should: 1. Call local health department 2. If no answer and situation is urgent, call 9-1-1
operator
Information to leave: Your name & contact information Reason for calling Facts of situation; no speculation

ReportingPersonal
Awareness
Suspicion
Report to:
ImmediateSupervisor
Local HealthDepartment
State Health Department
CDC (federal)
Disease Identification CoursesReportable Diseases and ProceduresInformation SourcesInfection Control Procedures (PPE)
Check CDC / information sourcesUse appropriate PPE
Reporting Algorithm
Fill in the phone numbers(___)
(___)
Personal Awareness
Suspicion
Report to:
ImmediateSupervisor
Local HealthDepartment
State Health Department
CDC (federal)
Disease Identification CoursesReportable Diseases and ProceduresInformation SourcesInfection Control Procedures (PPE)
Check CDC / information sourcesUse appropriate PPE
Reporting Algorithm
Fill in the phone numbers(___) (___)
(___) (___)

Staying in the Loop
Join CDC Listserv Clinicians’ Listserv: www.cdc.gov/subscribe.html
Check reliable websites Make local contacts Identify experts and key agencies
Gather contact information

Summary
All healthcare workers should remain vigilant for signs of public health threats.
Recognize unusual diseases clusters by knowing signs and symptoms of common and uncommon diseases or exposures Use B-NICE or CBRNE to remember categories of
agents most likely to be weaponized
First, try to validate your suspicions; then contact local authorities.

Authors
Jean Carter Sandra Kuntz Earl Hall Steven Fehrer Steven Glow
Basic Basic BioBio--DefenseDefense
ProjectProject
Emergency Preparedness Curriculum
Jacqueline Elam Michele Sare Lisa Wrobel Michael Minnick
Modules prepared as part of the Montana Basic BioDefense Curriculum For Pharmacy, Nursing, and Allied Health
Funded by the HRSA CFDA 93.996 initiative

Photo Credits
Do not reproduce individual photos or videoclips without permission from original source.
A list of photo credits was included in the instructor’s packet.
To request a copy of the photo credits, send an email to [email protected]
Basic Basic BioBio--DefenseDefense
ProjectProject
Emergency Preparedness Curriculum
Modules prepared as part of the Montana Basic BioDefense Curriculum For Pharmacy, Nursing, and Allied Health
Funded by the HRSA CFDA 93.996 initiative