Embed Size (px)
Citation preview
Recognizing Clinical Reasoning Errors
Heidi Chumley, MD
Associate Professor, Family Medicine

Session Objectives
• At the end of this session, participants should be able to: – Outline the steps of the clinical reasoning
process.– Define cognitive dispositions to respond
(CDRs) and describe several CDRs seen with diagnostic reasoning errors.
– Recognize clinical reasoning errors in common educational settings.

Clinical Reasoning
• “the cognitive process necessary to evaluate and manage a medical problem”
Reasoning
KnowledgeSkill

Medical Errors
• 44,000 to 98,000 deaths per year due to medical errors
• Many systematic and individual factors contribute to medical errors
• Recent attention on cognitive errors (clinical reasoning, diagnostic reasoning, decision-making)

Cognitive Errors
Zhang, JAMIA, 2002

Cognitive Errors
• Of 301 Malpractice claims, 59% involved diagnostic errors that led to poor outcomes – Gandhi, 2006
• Of patients admitted with 10 days of outpatient visit, 10% due to diagnostic error – Singh, 2007
• Autopsy series showed 24% missed diagnosis – Shojania, 2003

Diagnostic process
Diagnosis Verification
Diagnosis Refinement
Differential Diagnosis Generation
Information gathering
Why are errors made?
• Failure/delay of eliciting information – Singh, 2007
• Suboptimal weighing of critical pieces of information from H&P – Singh, 2007
• Overreliance on diagnostic testing – Bordage, 1999
Cognitive Dispositions to Respond
• Biases that can lead to diagnostic errors
• Mental shortcuts running amuck
• Croskerry defines 32, Acad Med, 2003: 78(8)

Cognitive Dispositions to Respond
• Information-gathering– Unpacking– Availability– Anchoring– Premature closure
• System– Diagnosis momentum– Feedback sanction– Triage cueing
• Probability– Aggregate bias– Base-rate neglect– Gender bias– Gambler’s fallacy– Posterior probability
error
Croskerry, 2003

Information-gathering problems
• Unpacking – failure to elicit all relevant information
• Availability – recent exposure influences diagnosis
• Anchoring – holding onto a diagnosis after receiving contradictory information
• Premature closure – accepting a diagnosis before it is fully verified
Present at all levels, start watching for these in students

Clues to Information-Gathering Problems
• Limited differential diagnosis (unpacking, availability)
• Lack of attention to contradictory information (anchoring)
• Lack of pertinent negatives (premature closure)
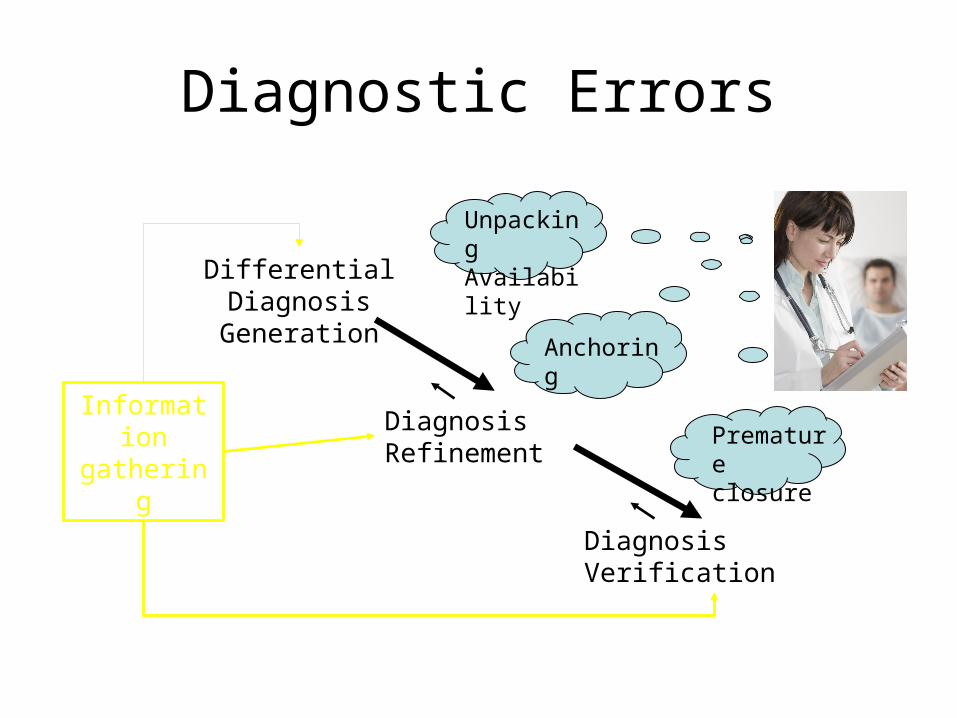
Diagnostic Errors
Diagnosis Verification
Diagnosis Refinement
Differential Diagnosis Generation
Information gathering
Unpacking Availability
Anchoring
Premature closure
Systems contributions
• Diagnosis momentum – early diagnosis by another provider is accepted as definite
• Feedback sanction – final diagnosis does not return to initial decision-maker
• Triage cueing – location cues management (seen through the lens of the first provider)
Present at all levels, more likely to see in residents

Clues to System Contributors
• Lack of primary symptom data (diagnostic momentum)
• Inattention to closing the loop (feedback sanction)
• Non diagnoses: non-cardiac chest pain; no gynecologic cause for lower abdominal pain (triage cueing)

Probability Pitfalls
• Aggregate bias – aggregate data do not apply to my patients
• Base-rate neglect – ignoring the true prevalence
• Gender bias – gender inappropriately colors probability
• Gambler’s fallacy – sequence of same diagnoses will not continue
• Posterior probability – sequence of same diagnoses will continue
Best seen during continuity experiences, residency

Clues to Probability Pitfalls
• Didn’t meet criteria, but I…(aggregate)
• Rare diagnoses high on list, increased testing (base-rate neglect)
• Comments about probability (Gambler’s fallacy, posterior probability)

Two Others
• Representative restraint – ruled out because the presentation is not typical
• Search satisfying – search is called off when something is found

Summing Up
• Reasoning errors are common
• Identifying/naming the CDRs is an important part of reflection
• No gold standard for assessing reasoning in our learners – nothing to replace our conversations and helping them think about how they are thinking
• Are cognitive errors treatable? Yes

Questions?