Embed Size (px)
Citation preview
1
Reconstruction of the Atrophic Edentulous Maxillas with Allograft Bone
(Fresh Frozen Bone) and Immediate Loading Implants
Celso Marques Oral and Maxillofacial Surgeon, Private Practice. Rua Artur de Azevedo, 1217 – cj 44 São Paulo, Brazil [email protected] Luiz Fernando Akaki Borges Specialist in Prosthodontics Dentistry by Dental School of Ribeirão Preto - University of São Paulo Master in Oral Medicine by Heliópolis Hospital – São Paulo, Brasil Private Practice, São Paulo - Brazil Alexandre Augusto Benetton Oral and Maxillofacial Surgeon, Private Practice. Alberto Barlattani Specialist in Stomatology, Implants at University La Sapienza, Roma. Medical Director of University Tor Vergata Facultà of Dentistry, Roma. Responsible Professor, Catedra of Prosthodontics in Tor Vergata University, Roma. Samuel Porfirio Xavier MSci, DDS, PhD Department of Oral & Maxillofacial Surgery, University of São Paulo, Ribeirao Preto, Brazil. Suzie Aparecida de Lacerda Department of Morphology, Stomatology and Physiology, Dental School of Ribeirão Preto – USP Specialist in Oral Pathology by Dental School of Ribeirão Preto - University of São Paulo Master in Oral Rehabilitation by Dental School of Ribeirão Preto - University of São Paulo Doctor in Oral Rehabilitation by Dental School of Ribeirão Preto - University of São Paulo

2
Reconstruction of the Atrophic Edentulous Maxillas with Allograft Bone
(Fresh Frozen Bone) and Immediate Loading Implants
Summary
Purpose: Assess the feasibility of reconstruction of the atrophic edentulous maxillas using
fresh frozen bone and their subsequent rehabilitation with immediate loading implants and
fixed prosthesis. Materials and Methods: Fourteen patients (average age 53.8) with severely
atrophic maxilla received fresh frozen bone grafts for width reconstruction (onlay block
grafts) and vertical augmentation of posterior regions (sinus augmentation) using particulate
bone and platelet-rich plasma). After an average of 6 month from the first surgical procedure,
the patients received 6 implants each with an immediate loading fixed prosthesis. Results:
Implant survival rate was 100% in the evaluation period (6 to 42 months) and no significant
complications occurred. Discussion: Histological evaluation of reconstructed atrophic
maxillas using fresh frozen bone grafts showed the presence of cellular nucleus in a
previously acellular tissue. This demonstrates the possibility of using the newly-formed bone,
confirming the feasibility of using this alternative material for grafting. The installation of
immediate loading osseointegrated implants 6 months after the graft has been shown to be
highly predictable and reliable. Radiographically, a normal bone aspect was noted in the sinus
areas that received bone grafts. The radiographs showed bone loss around the implants lower
than 0.5 mm after 42 months. Conclusions: The jaw bone reconstruction with fresh frozen
bone, and subsequent placement of immediate loading implants, and implant-supported fixed
prostheses was shown to be a viable and highly reliable alternative.
Key words: fresh frozen bone, bone grafts, reconstructive preprosthetic surgery,
augmentation, endosseous implants
3
Introduction
With the advent of osseointegrated implants, oral rehabilitation gained new
possibilities and perspectives. In the beginning, implants were installed in areas with
sufficient remaining bone. As time went by, several techniques were developed in order to
reconstruct atrophic areas, and subsequently install implants, for vertical (maxillary sinus
elevation, onlay bone graft, osteogenic distraction), or horizontal (onlay or particulate graft)
augmentation. Several materials were also used: autogenic, homogenic, xenogenic bone and
alloplastic materials.
The autogenic bone is considered the ideal standard and allows the comparison with
other techniques. However, the great inconvenience/difficulty is the morbidity produced by
another surgical site, frequently more painful than the receptor site. Hence, several researches
have been developed looking for a feasible substitute, with a reasonable cost, quality and
reliability similar to autogenic bone.
Conventional two-step dental implants have a high success rate. However, the time
period between implant installation and final prosthesis placement causes several damages.
For example, they may increase treatment time and the functional discomfort due to
temporary removable tissue-supported prostheses, especially for total edentulous patients.
Accordingly, research interest increased in shortening the time period between implant
placement and prosthetic rehabilitation. In recent years, several studies have demonstrated a
high success rate of early implant placement, with clinical application of immediate loading
implants, especially for the lower jaw(1,2). Recent publications also encourage early implant
placement for maxilla(3,4). However, patients with greatly reduced bone volume in the implant
receptor site need tissue augmentation. This can be obtained through the combination of
techniques for bone augmentation before the immediate loading implant placement(5).

4
Therefore, this paper presents a proposal for atrophic maxilla reconstruction using fresh
frozen allograft bone for width gains in the maxillary anterior region (onlay block) and
maxillary sinus elevation (particulate). After the graft maturation period (6 months), every
reconstructed maxilla received 6 strategically distributed implants that supported an
immediate loading implant-supported prosthesis. Fourteen cases were evaluated with clinical
and radiographic follow-up periods ranging from 6 to 44 months (average of 16.4 months).
5
Materials and Methods
The patients were submitted to a detailed anamnesis and the exclusion criteria were as
follows:
− Non-compensated systemic pathologies, such as diabetes and immune disorders;
− Recent history of chemotherapy for head and neck;
− Psychological disorders;
− Unavailability for return visits for long-term control;
− Remaining teeth with uncontrolled periodontal problems.
The patients were submitted to the following laboratory tests: hemogram,
coagulogram, glycemia test.
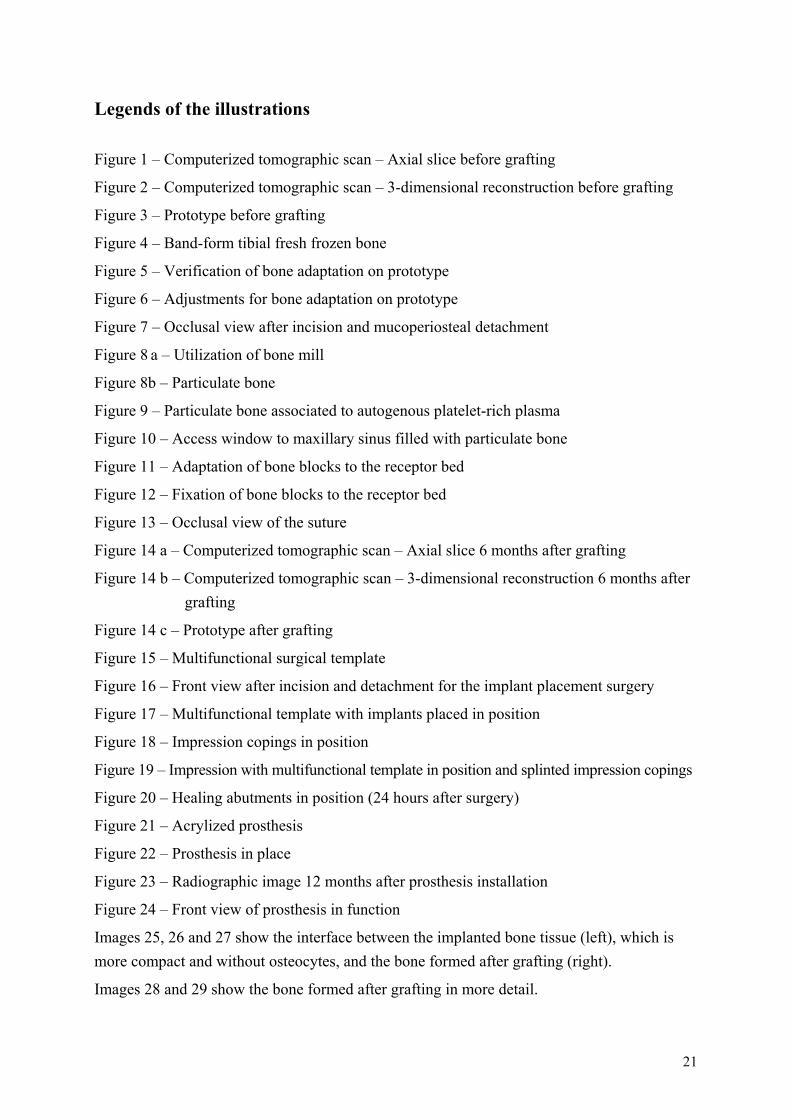
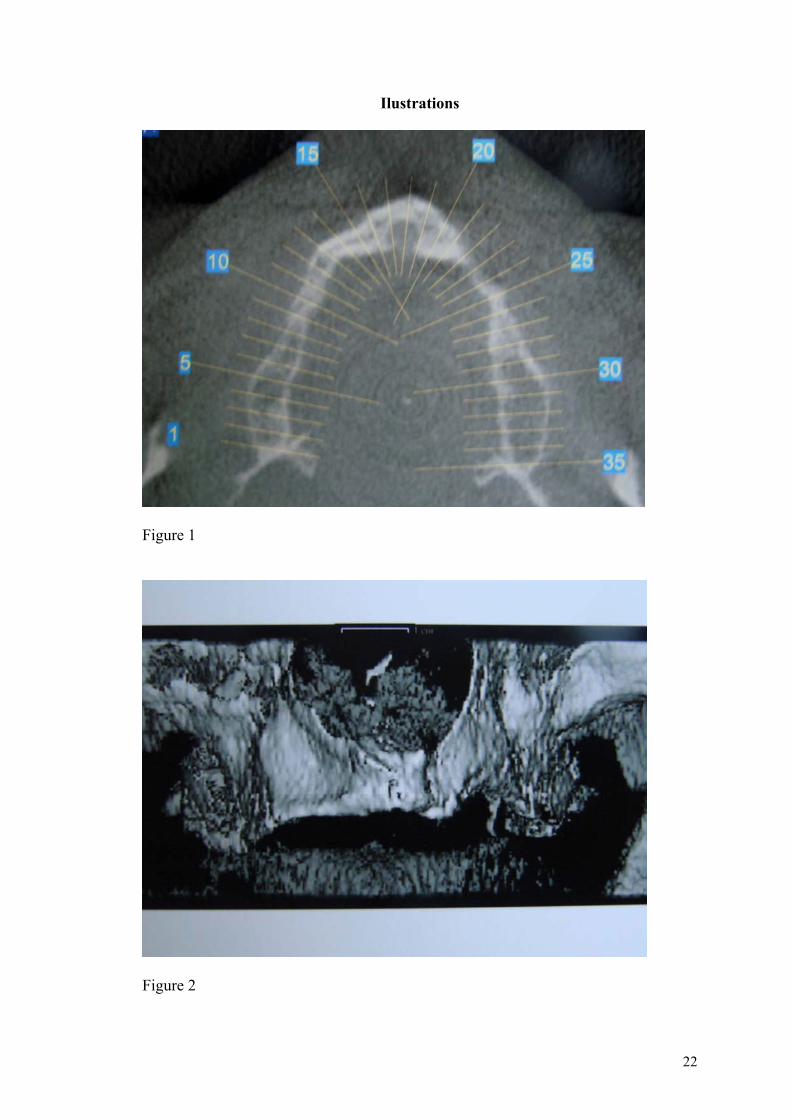
A computerized tomographic scan (CT) was requested to precisely measure the
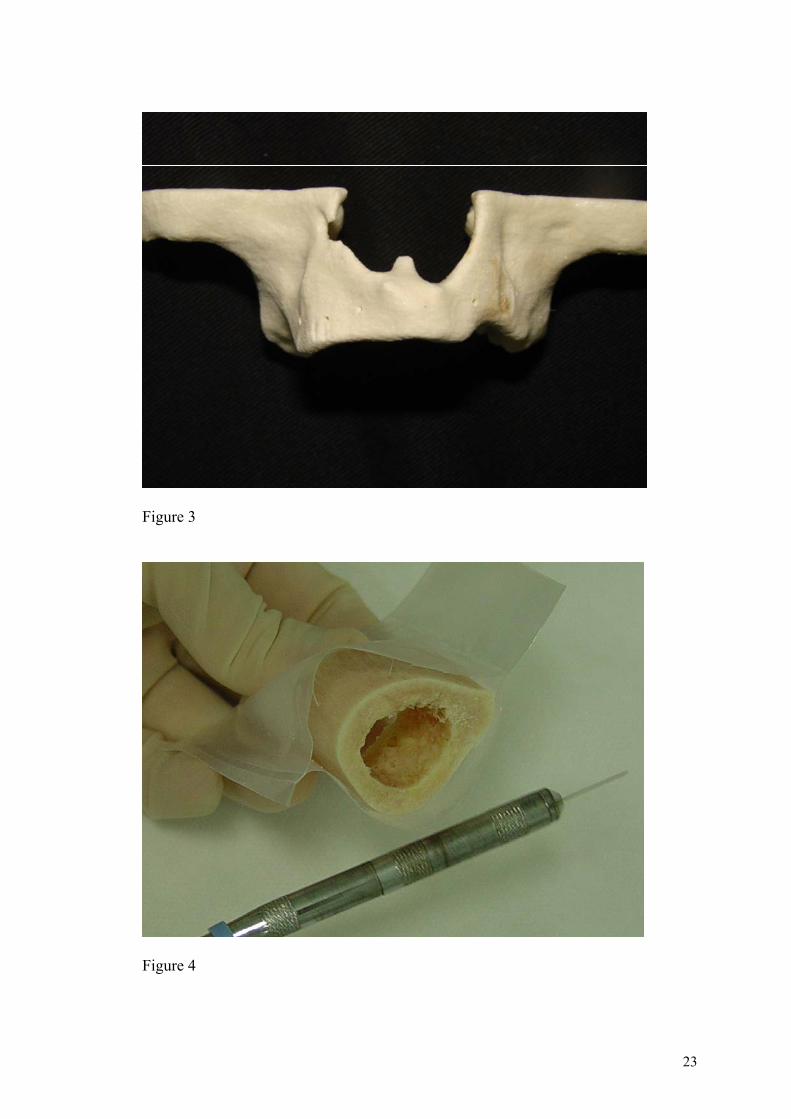
remaining bone (Figures 1 and 2), as well as to create a prototype of a precise 3-dimensional
(3D) stereolithographic model (Figure 3). All patients presented with edentulous maxilla. The
CT scans showed the presence of an atrophic ridge of the remaining bone Class VI(6) that
hinders the placement of the appropriate implants, in terms of size and location, for prosthetic
rehabilitation.
The allogenic bone for the grafting was provided by the Skeletal Muscle Tissue Bank
of Hospital das Clínicas of Curitiba for 2 cases and by the Tissue Bank of the Orthopedics and
Traumatology Institute of the Hospital das Clínicas of São Paulo for 12 cases. This material
was harvested, processed, stored and distributed following the current standards for organ and
tissue transplantation. The patients were duly instructed and signed the patient informed
consent form for the procedures. The cases described used tibial bands.
6
The prototypes were sterilized in a 2% glutaraldehyde solution for 10 hours before the
surgery and were thoroughly washed with sterile physiological solution to be used in the
aseptic chain for adaptation of the graft.
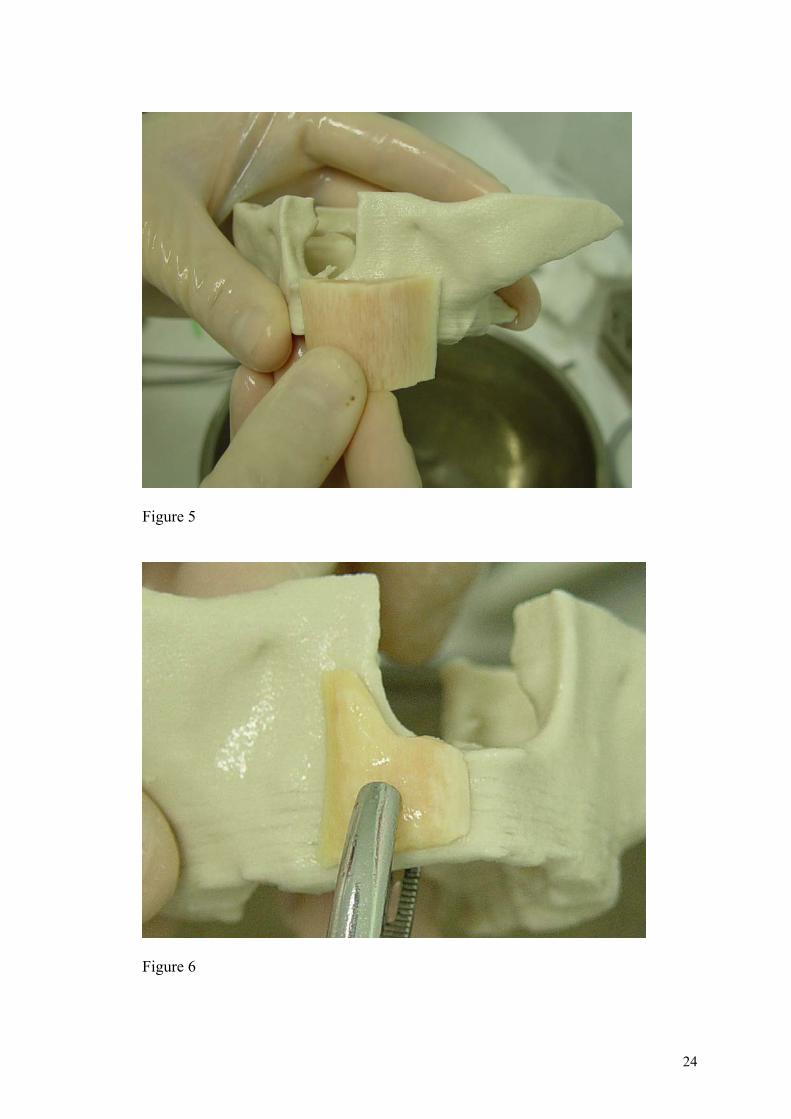
The bone graft material for the transplant was received one hour before the beginning
of the surgery, in accordance with the protocol suggested by transplant regulatory bodies.
These require that, as the bone graft is taken from the tissue bank, where it is stored in ultra-
low temperature (lower than -80°C), it has to be transported in a special sealed thermal box,
packed and surrounded with dry ice, by a professional of the tissue bank, who must deliver it
checking the internal temperature of the package, that has to be below – 50° C (Figure 4).
After the surgical field was assembled, maintaining the aseptic chain, the bone blocks
were first adjusted on the prototypes in order to be well adapted(7) (Figures 5 and 6).
When the adjustment step was almost completed, the patient was anesthetized and the
incision was made medial to the alveolar ridge, from one tuber to the other, totally detaching
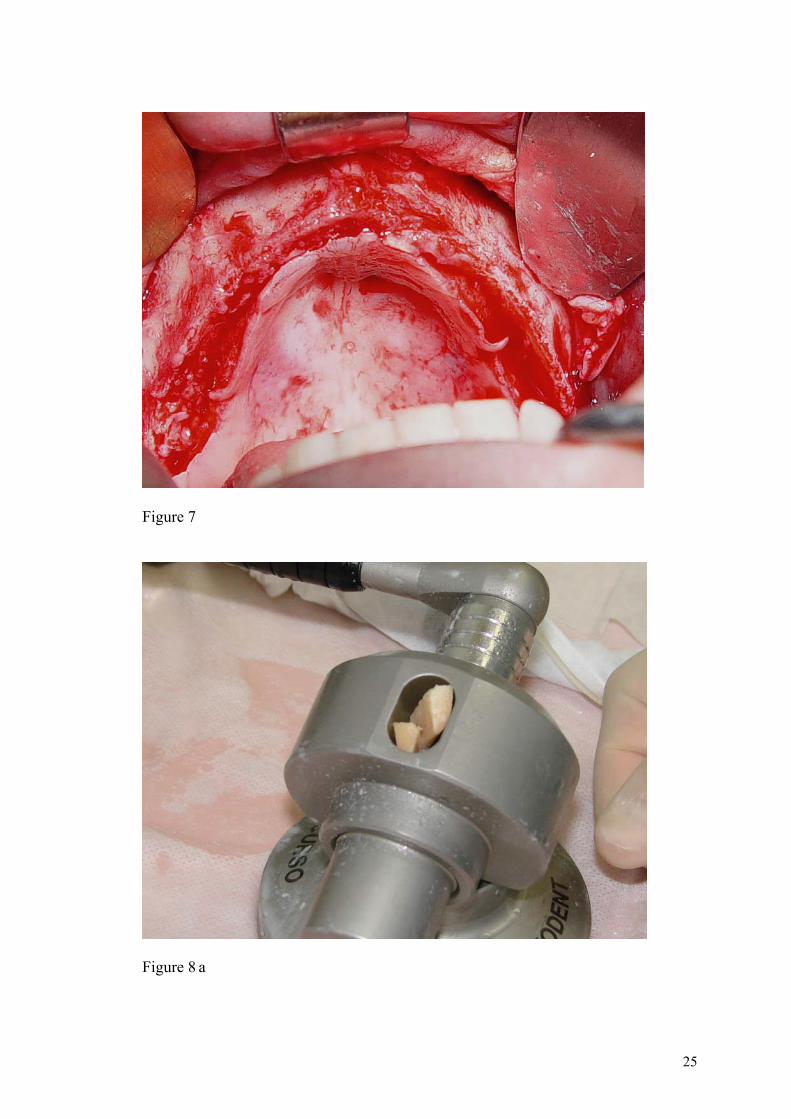
the flap and exposing the receptor beds. This medial shift of the incision aims at creating
better conditions for covering the graft, decreasing the tension of the suture (Figure 7).
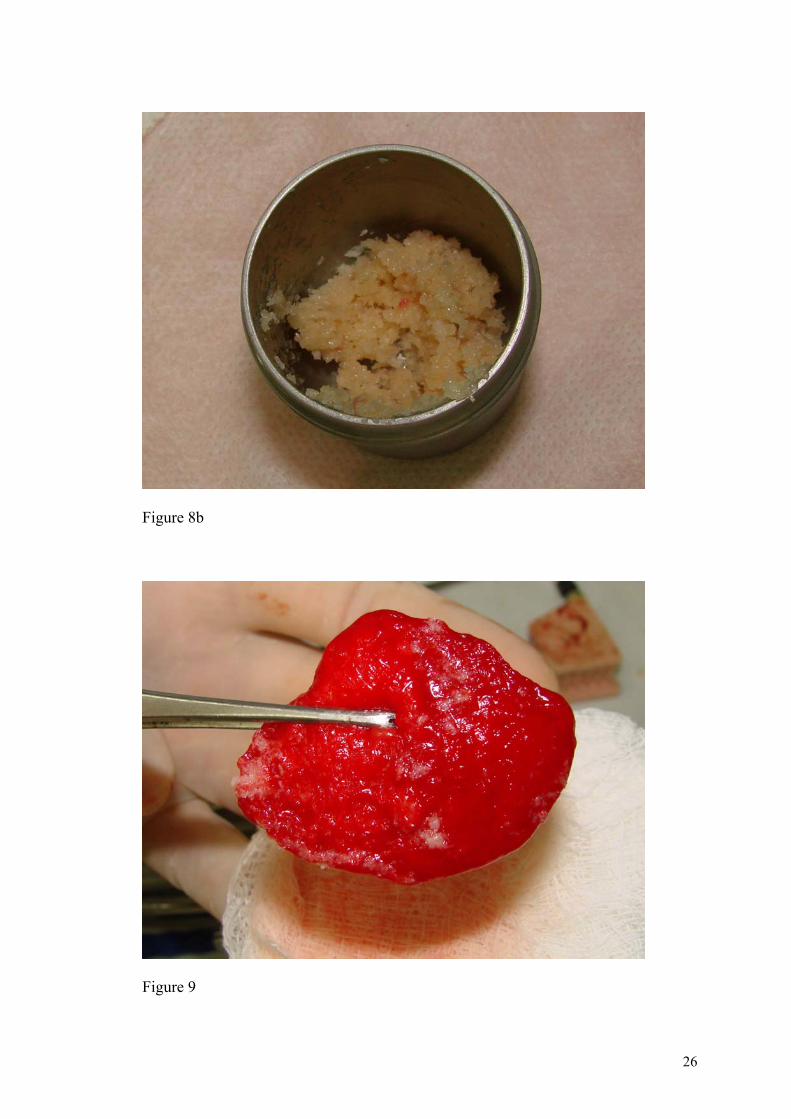
Some accesses were made bilaterally to the maxillary sinus. The maxillary sinus
received particulate bone (Figures 8a and 8b), associated to platelet-rich plasma (PRP) (Figure
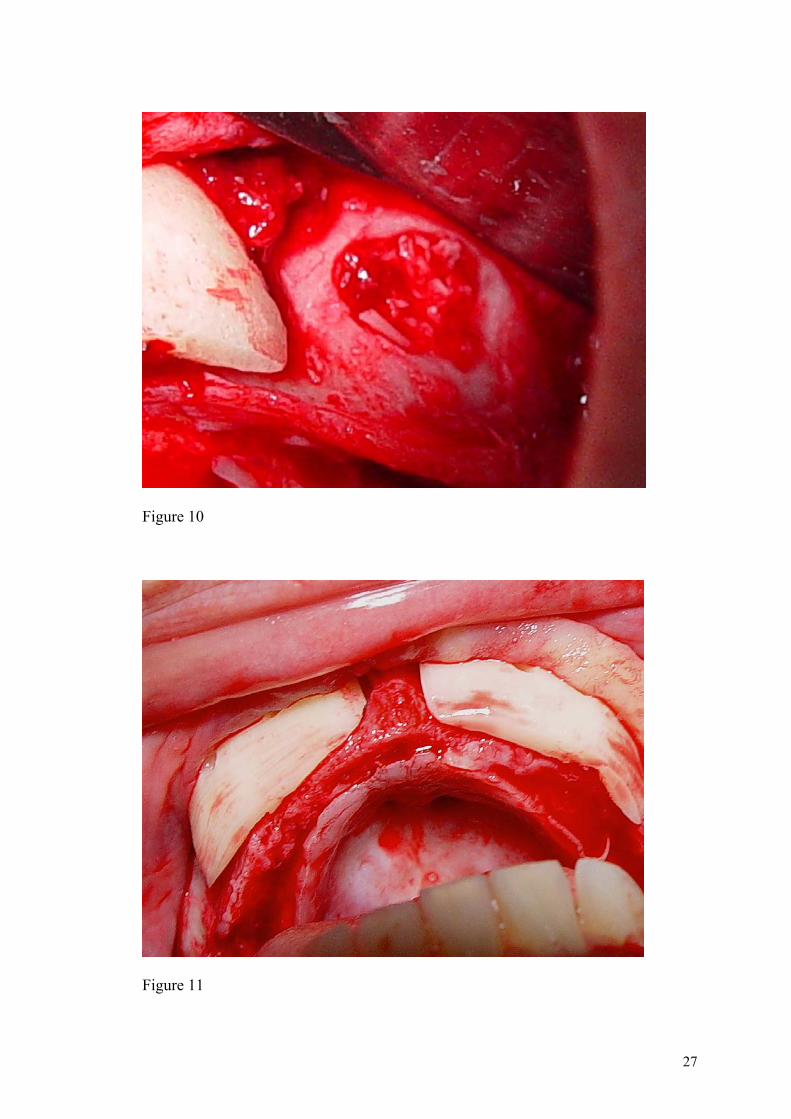
9), after the lateral wall opening and the sinusal membrane detachment, following the
conventional technique for augmentation of the maxillary sinus floor (Figure 10). In the
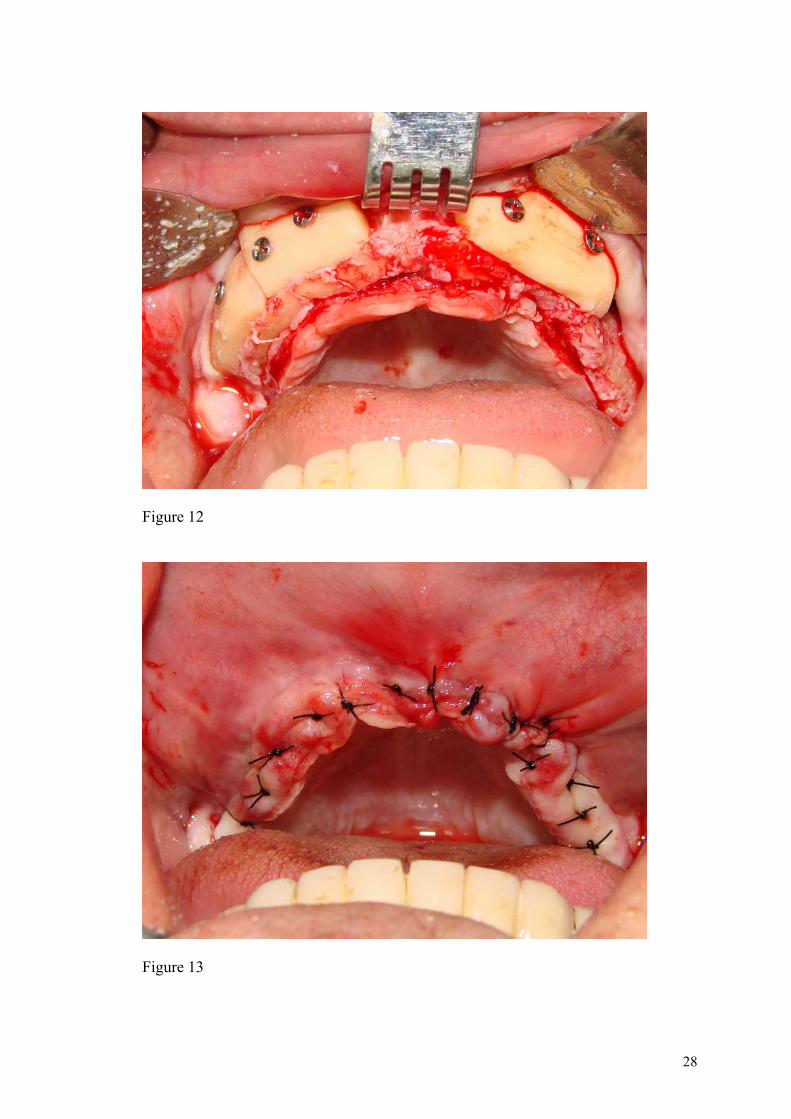
anterior regions, bone blocks fixed with 2 screws each were adapted (Figures 11 and 12). The
receptor cortical bone was perforated in some places with a round bur to facilitate the blood
supply and subsequent irrigation of the graft block. A 4.0 nylon thread was used for the suture
(Figure 13) and the patients were instructed not to wear dentures for 20 days. Mouthrinse with
0.12% chlorhexidine 3 times a day for 20 days was prescribed. After 7 days, the suture was
removed and the provisional prosthesis was readapted.
7
The drug protocol consisted of one tablet of azitromicine 500mg for 5 days and
dexametasone 4 mg every 12 hours for 3 days, in addition to analgesics depending on the
intensity of the pain.
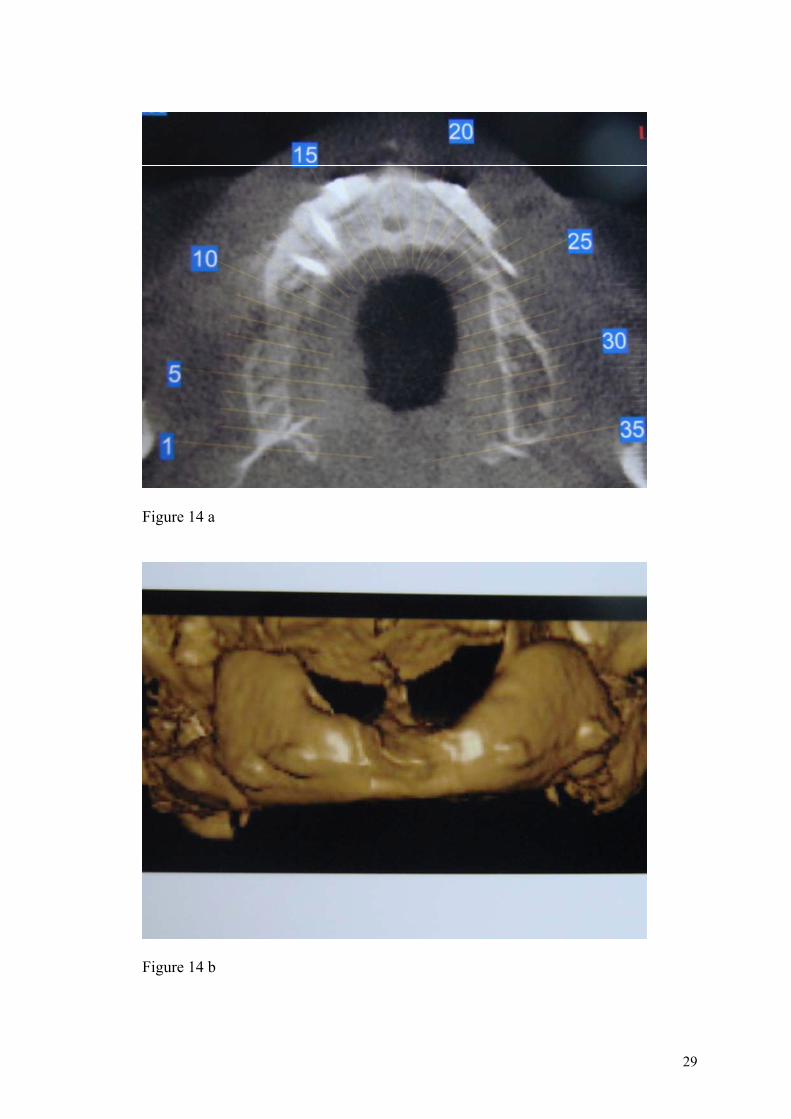
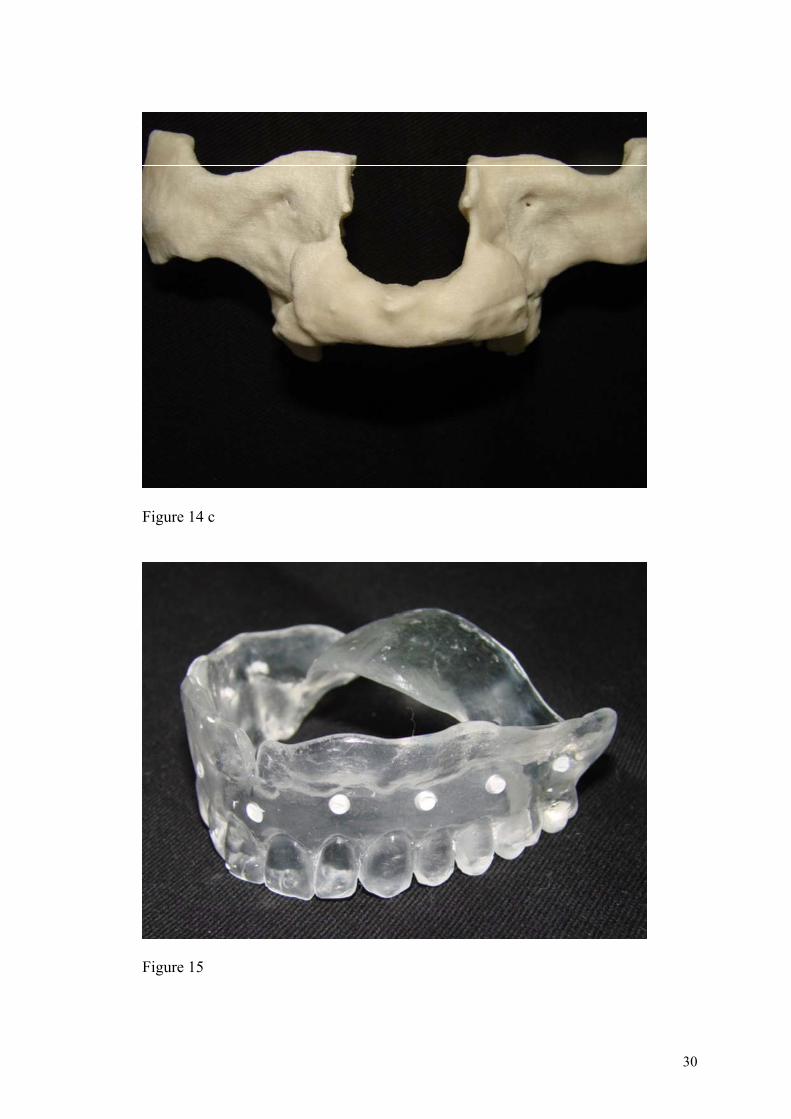
Six months after the surgical grafting procedures, CT scans were made to evaluate the
results and to plan the implant placement (Figures 14a, 14b and 14c).
Before the surgery for implant placement, conventional impressions were taken for the
total prosthesis, wax rims were made and the teeth were mounted. After the evaluation of the
vertical dimension of occlusion and of the intermaxillary relation, multifunctional acrylic
surgical templates were fabricated (Figure 15), similar to the total prostheses, to guide the
implant positioning, and to transfer them to the working cast, in addition to record the
maxillomandibular relation for articulator mounting.
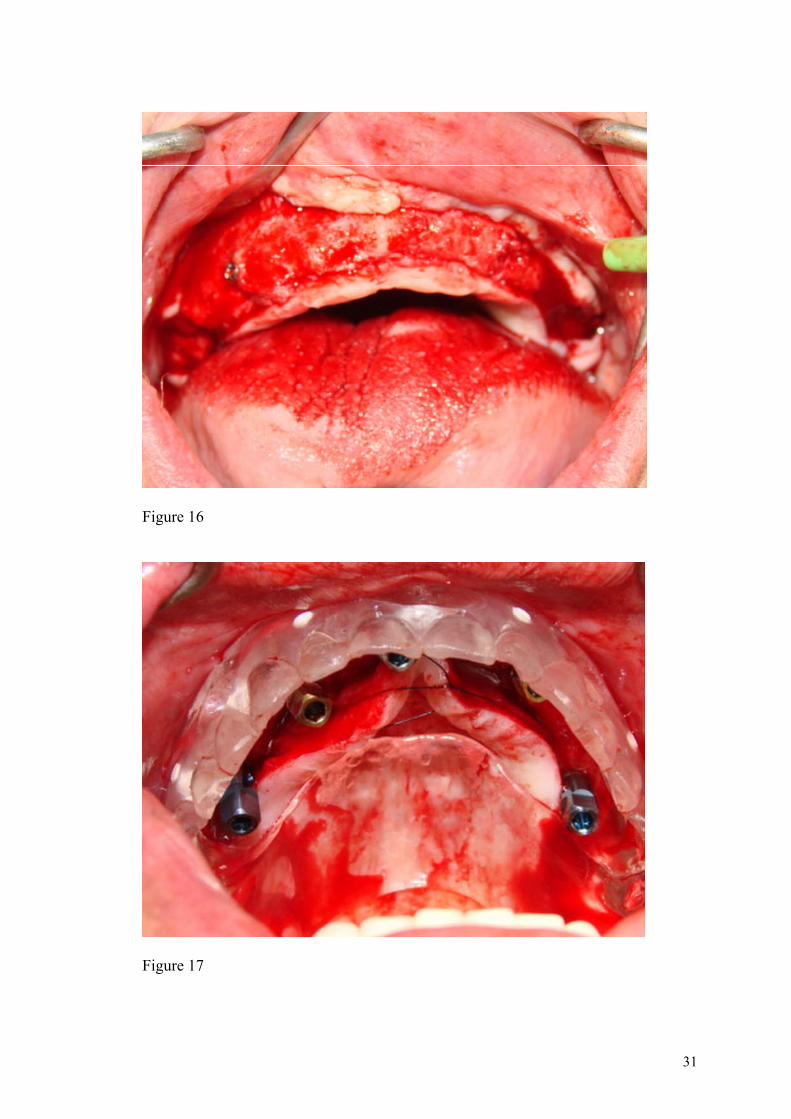
The placement of the implants was performed under local anesthesia. The incisions
were made on the alveolar ridge, the total flaps were detached, and the graft fixation screws
were removed (Figure 16). The multifunctional surgical templates, stored in a glutaraldehyde
solution, were thoroughly washed with 0.9% physiological solution and positioned. Six
BTLock System implants (3.75 mm diameter and 13 or 15 mm length; BTLock Vicenza,
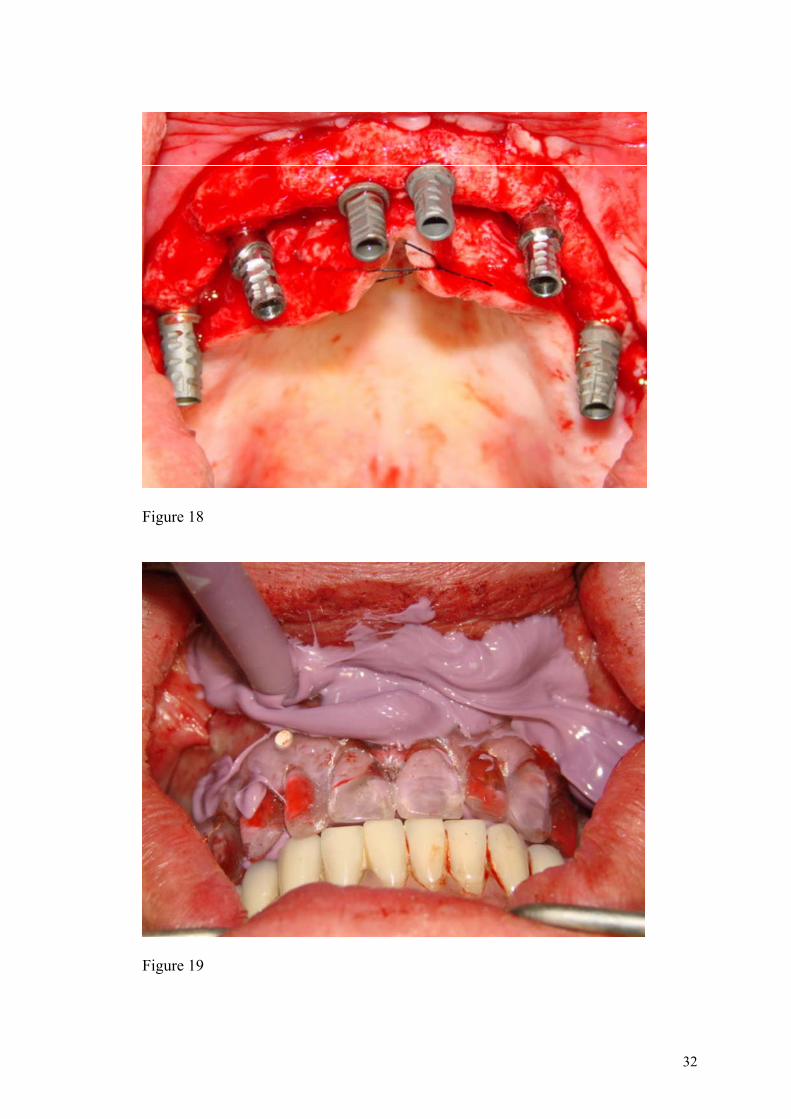
Italy) were placed and strategically distributed, forming a polygon (Figure 17). The minimum
insertion torque was 32 N. The implant mounters slided easily into the surgical template
grooves. Vicryl type sutures were made without removing the implant mounters, which work
as impression copings (Figure 18). The surgical templates were filled with addition-type
silicone impression material (Monophase Stern Vantage; Sterngold Restorative Systems,
Germany) and placed in position. The prefabricated mounters were then fixed to the templates
with chemically curing resin (Pattern Resin-GC America Inc, Alsip, USA), using a procedure
similar to the one used for the impression of implants with an open-tray impression. It is
important that the mounters do not cause any occlusal interference, since a bite record with
8
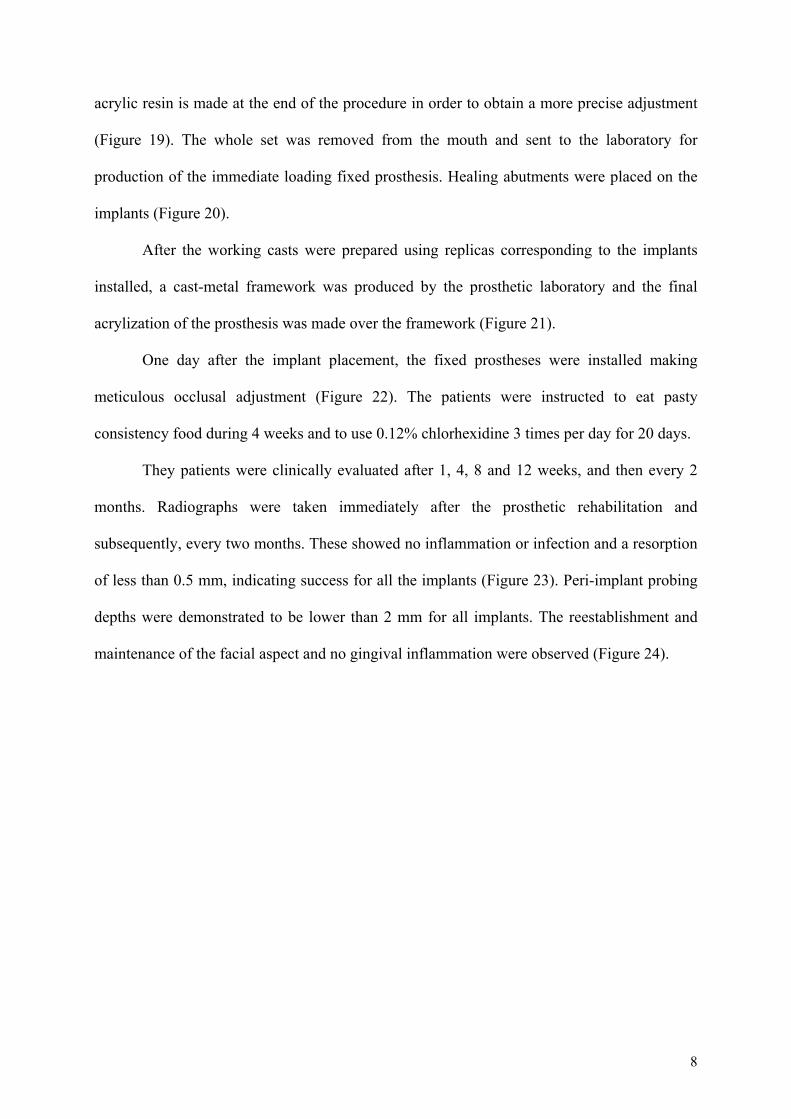
acrylic resin is made at the end of the procedure in order to obtain a more precise adjustment
(Figure 19). The whole set was removed from the mouth and sent to the laboratory for
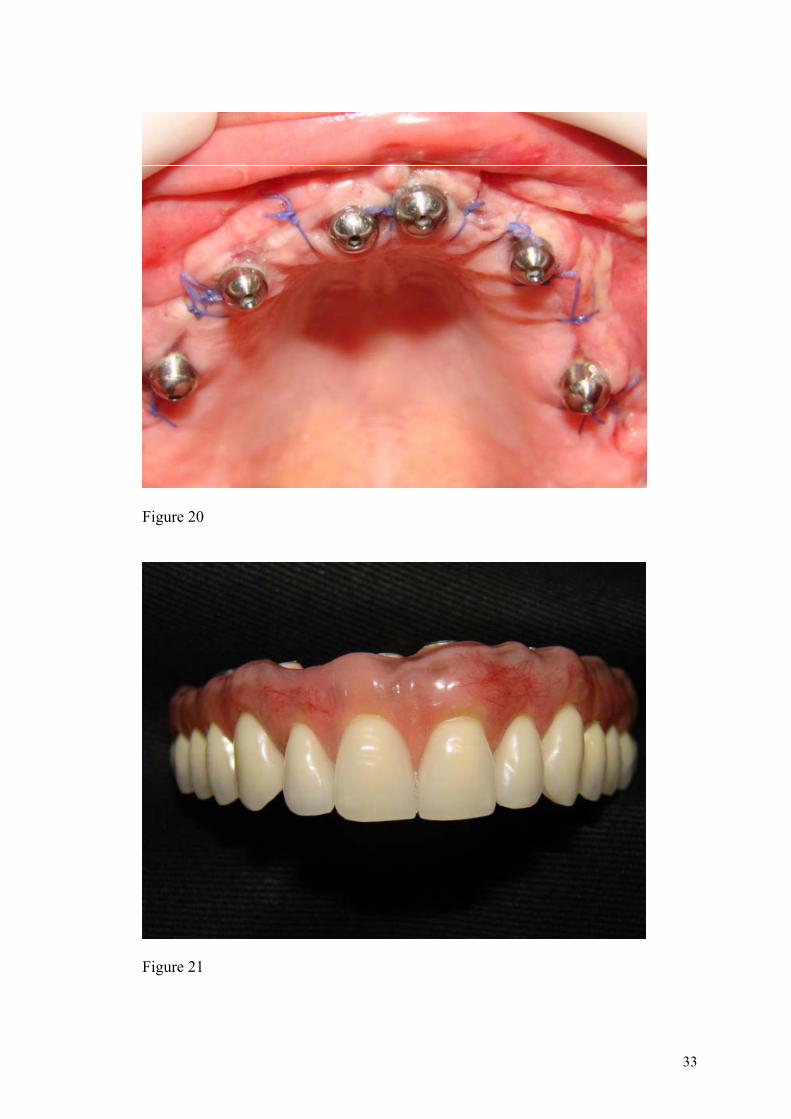
production of the immediate loading fixed prosthesis. Healing abutments were placed on the
implants (Figure 20).
After the working casts were prepared using replicas corresponding to the implants
installed, a cast-metal framework was produced by the prosthetic laboratory and the final
acrylization of the prosthesis was made over the framework (Figure 21).
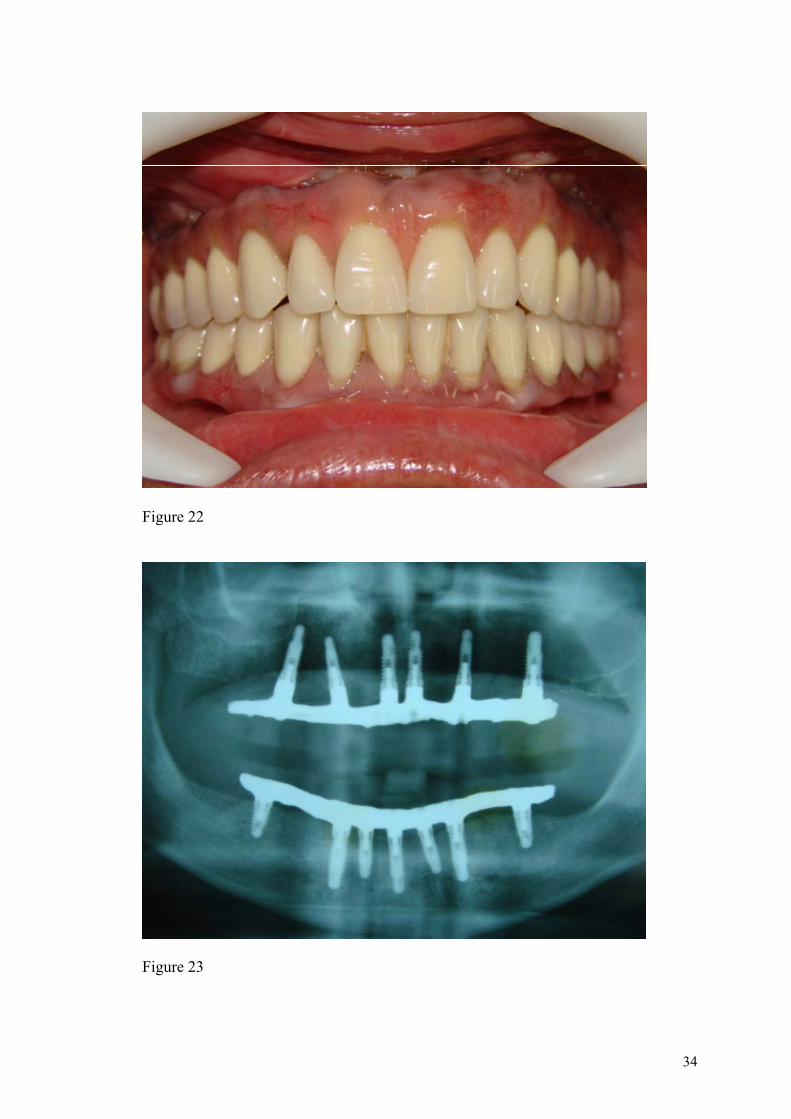
One day after the implant placement, the fixed prostheses were installed making
meticulous occlusal adjustment (Figure 22). The patients were instructed to eat pasty
consistency food during 4 weeks and to use 0.12% chlorhexidine 3 times per day for 20 days.
They patients were clinically evaluated after 1, 4, 8 and 12 weeks, and then every 2
months. Radiographs were taken immediately after the prosthetic rehabilitation and
subsequently, every two months. These showed no inflammation or infection and a resorption
of less than 0.5 mm, indicating success for all the implants (Figure 23). Peri-implant probing
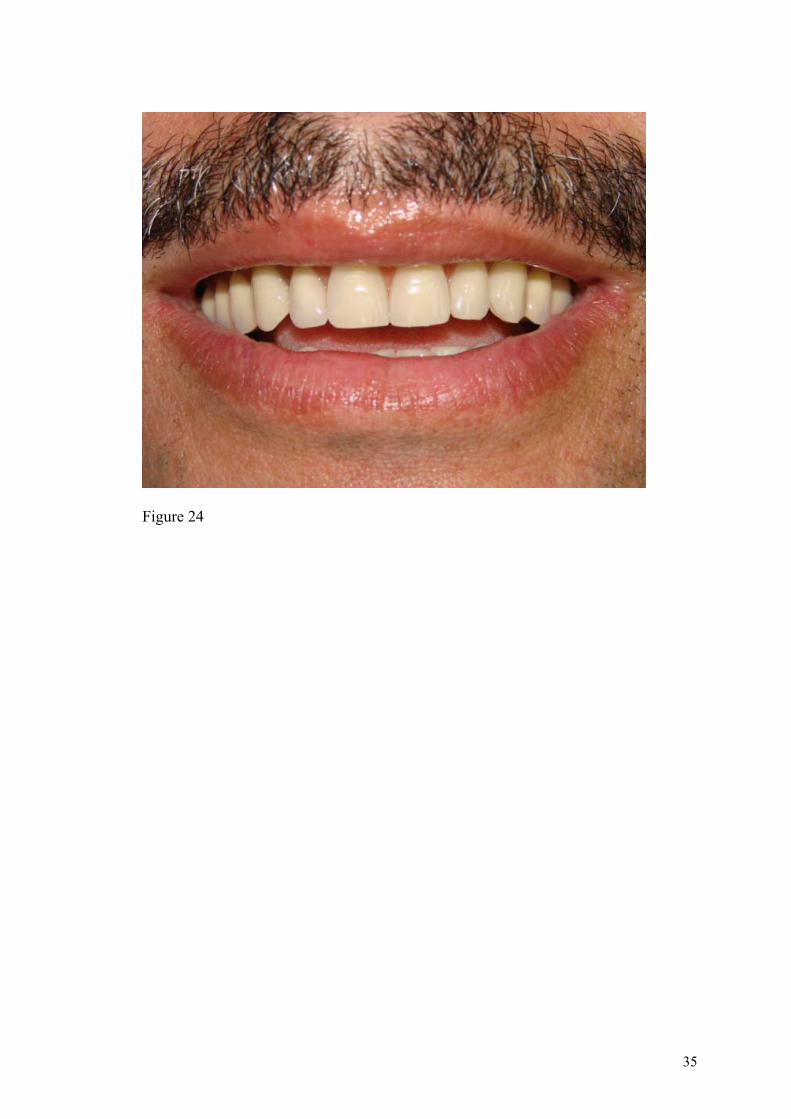
depths were demonstrated to be lower than 2 mm for all implants. The reestablishment and
maintenance of the facial aspect and no gingival inflammation were observed (Figure 24).
9
Results
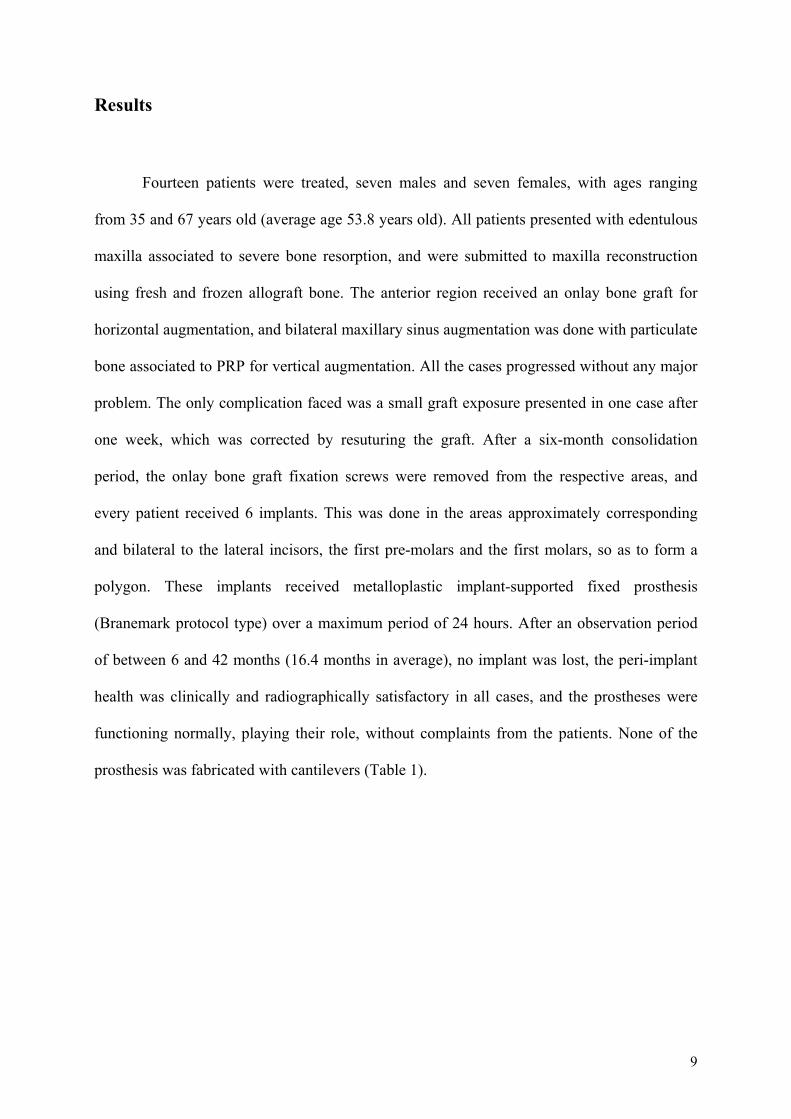
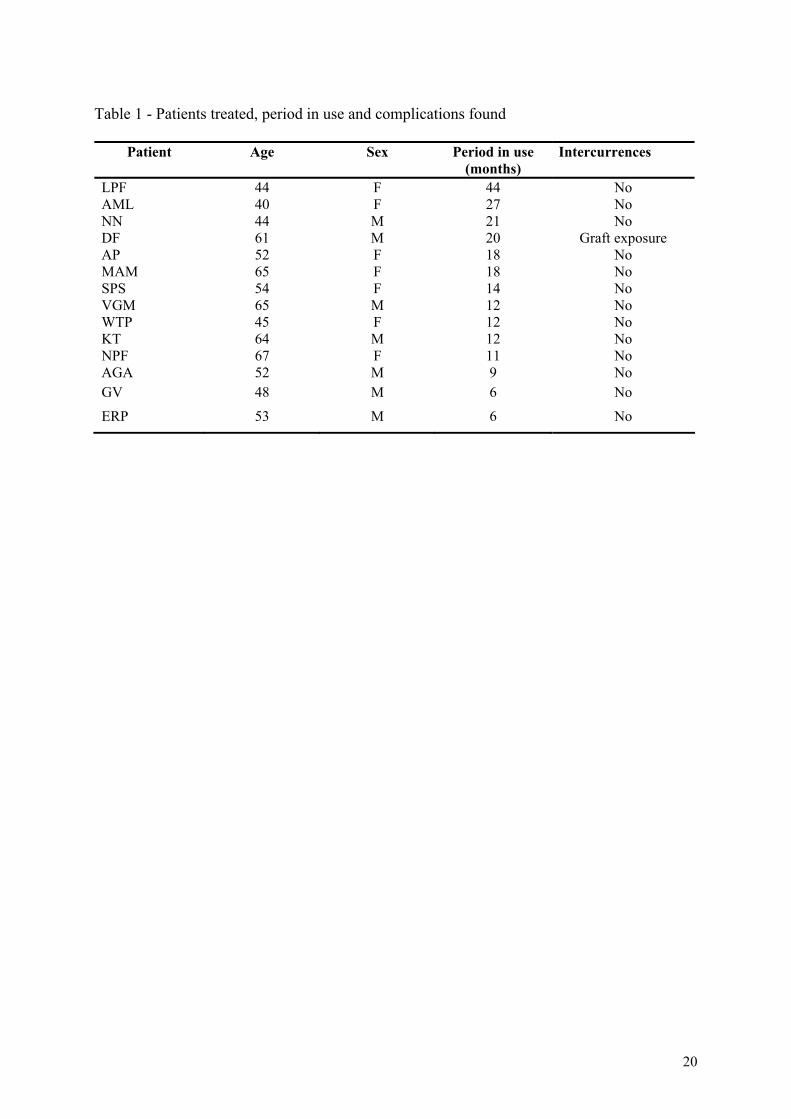
Fourteen patients were treated, seven males and seven females, with ages ranging
from 35 and 67 years old (average age 53.8 years old). All patients presented with edentulous
maxilla associated to severe bone resorption, and were submitted to maxilla reconstruction
using fresh and frozen allograft bone. The anterior region received an onlay bone graft for
horizontal augmentation, and bilateral maxillary sinus augmentation was done with particulate
bone associated to PRP for vertical augmentation. All the cases progressed without any major
problem. The only complication faced was a small graft exposure presented in one case after
one week, which was corrected by resuturing the graft. After a six-month consolidation
period, the onlay bone graft fixation screws were removed from the respective areas, and
every patient received 6 implants. This was done in the areas approximately corresponding
and bilateral to the lateral incisors, the first pre-molars and the first molars, so as to form a
polygon. These implants received metalloplastic implant-supported fixed prosthesis
(Branemark protocol type) over a maximum period of 24 hours. After an observation period
of between 6 and 42 months (16.4 months in average), no implant was lost, the peri-implant
health was clinically and radiographically satisfactory in all cases, and the prostheses were
functioning normally, playing their role, without complaints from the patients. None of the
prosthesis was fabricated with cantilevers (Table 1).
10
Discussion
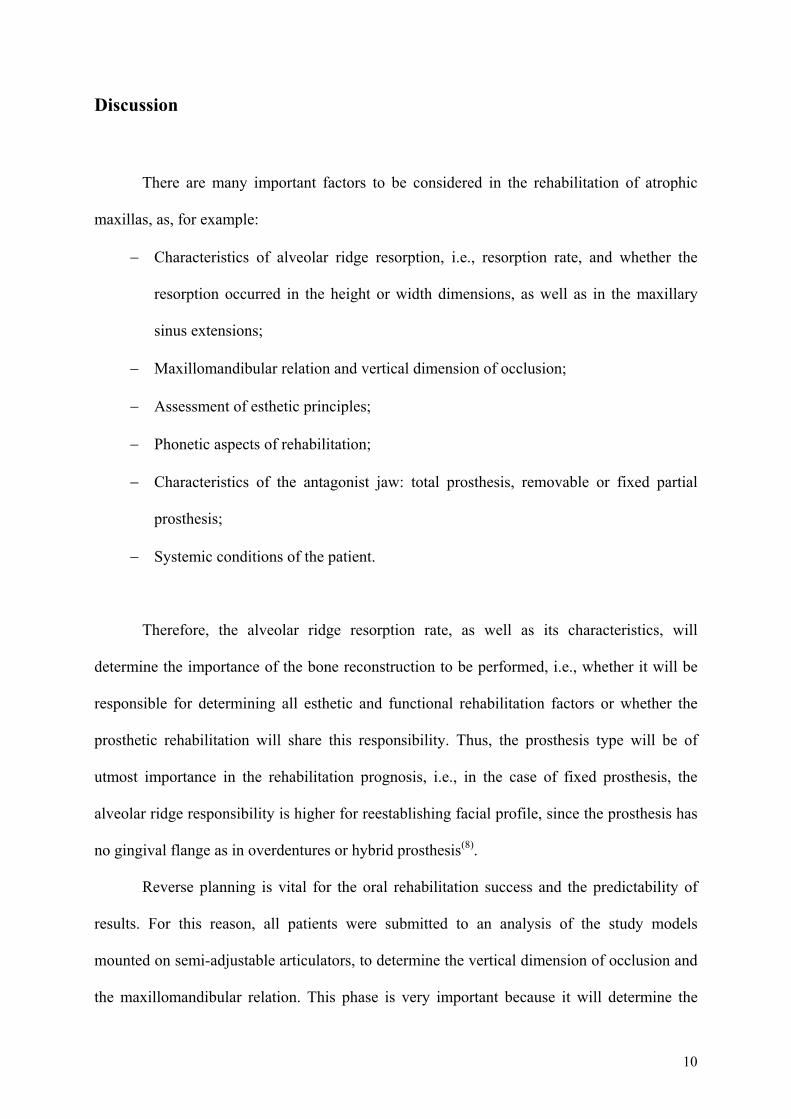
There are many important factors to be considered in the rehabilitation of atrophic
maxillas, as, for example:
− Characteristics of alveolar ridge resorption, i.e., resorption rate, and whether the
resorption occurred in the height or width dimensions, as well as in the maxillary
sinus extensions;
− Maxillomandibular relation and vertical dimension of occlusion;
− Assessment of esthetic principles;
− Phonetic aspects of rehabilitation;
− Characteristics of the antagonist jaw: total prosthesis, removable or fixed partial
prosthesis;
− Systemic conditions of the patient.
Therefore, the alveolar ridge resorption rate, as well as its characteristics, will
determine the importance of the bone reconstruction to be performed, i.e., whether it will be
responsible for determining all esthetic and functional rehabilitation factors or whether the
prosthetic rehabilitation will share this responsibility. Thus, the prosthesis type will be of
utmost importance in the rehabilitation prognosis, i.e., in the case of fixed prosthesis, the
alveolar ridge responsibility is higher for reestablishing facial profile, since the prosthesis has
no gingival flange as in overdentures or hybrid prosthesis(8).
Reverse planning is vital for the oral rehabilitation success and the predictability of
results. For this reason, all patients were submitted to an analysis of the study models
mounted on semi-adjustable articulators, to determine the vertical dimension of occlusion and
the maxillomandibular relation. This phase is very important because it will determine the
11
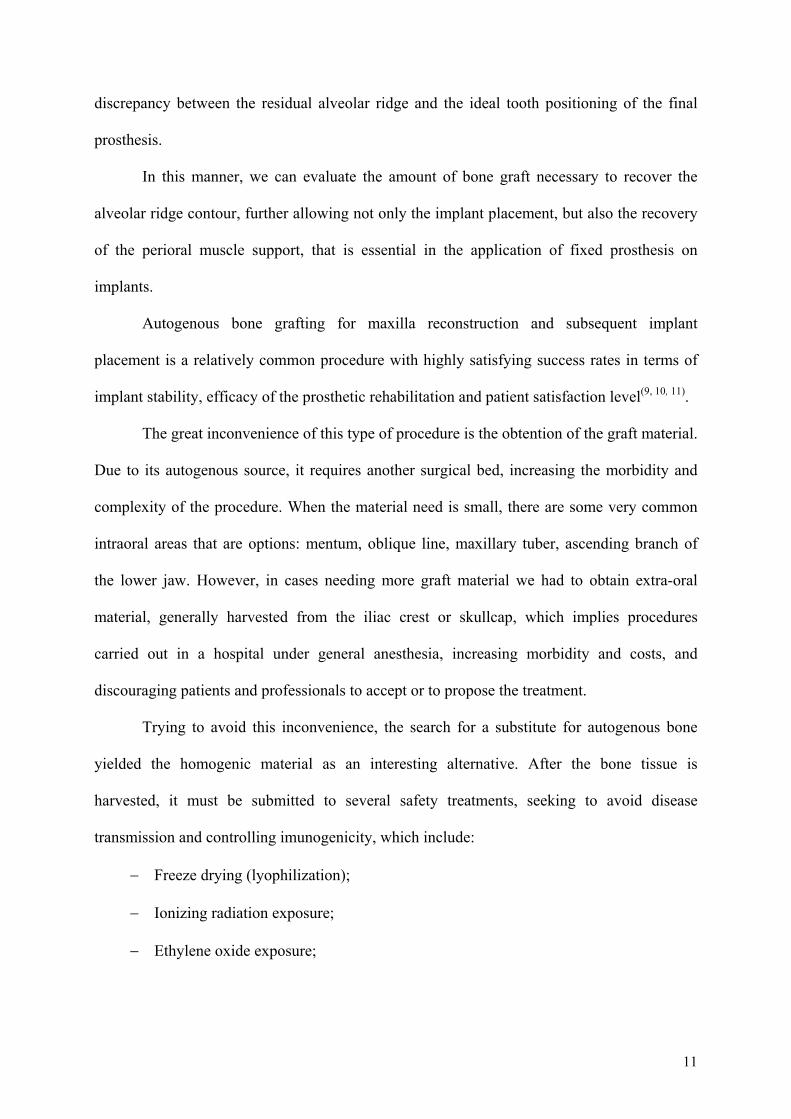
discrepancy between the residual alveolar ridge and the ideal tooth positioning of the final
prosthesis.
In this manner, we can evaluate the amount of bone graft necessary to recover the
alveolar ridge contour, further allowing not only the implant placement, but also the recovery
of the perioral muscle support, that is essential in the application of fixed prosthesis on
implants.
Autogenous bone grafting for maxilla reconstruction and subsequent implant
placement is a relatively common procedure with highly satisfying success rates in terms of
implant stability, efficacy of the prosthetic rehabilitation and patient satisfaction level(9, 10, 11).
The great inconvenience of this type of procedure is the obtention of the graft material.
Due to its autogenous source, it requires another surgical bed, increasing the morbidity and
complexity of the procedure. When the material need is small, there are some very common
intraoral areas that are options: mentum, oblique line, maxillary tuber, ascending branch of
the lower jaw. However, in cases needing more graft material we had to obtain extra-oral
material, generally harvested from the iliac crest or skullcap, which implies procedures
carried out in a hospital under general anesthesia, increasing morbidity and costs, and
discouraging patients and professionals to accept or to propose the treatment.
Trying to avoid this inconvenience, the search for a substitute for autogenous bone
yielded the homogenic material as an interesting alternative. After the bone tissue is
harvested, it must be submitted to several safety treatments, seeking to avoid disease
transmission and controlling imunogenicity, which include:
− Freeze drying (lyophilization);
− Ionizing radiation exposure;
− Ethylene oxide exposure;
12
− Mechanical cleaning and ultra-low temperature freezing (-80ºC), to remove living
cells from the tissue that will be transplanted.
The freeze drying process (lyophilization) presents the advantage of sterilizing the
osseous tissue and making it easy to store. However, during these procedures there is a
significant loss of structural properties(12) with destruction of bone-inducing proteins(13). The
use of demineralized freeze dried bone (DFDB) allograft to recover atrophic areas is a
relatively common procedure, but with controversial results, as some authors obtained good
results(14) while others not so good(15).
The ionizing radiation exposure is effective to avoid the transmission of bacteria(16)
and to inactivate HIV in relatively low doses(17). However, grafted tissue loses desirable
biomechanical properties(18).
Irradiation was considered responsible for the poor results obtained in a study on
femoral homografts(19). The use of ethylene oxide preserves bone integrity, but it is important
to consider the toxic effects for the receptor(20).
The osseous tissue processing involving harvesting, mechanical cleaning and ultra-low
temperature freezing (-80ºC) produces the so called “Fresh Frozen Bone”. The low
temperature contributes to the preservation of the bone-inducing properties of osseous tissue,
and the maintenance of this biological property is very important for bone volume
recovery(21).
The risk of contamination with diseases like hepatitis B and C and AIDS in this type
of transplantation is minimal. In addition to the tests applied to all the samples donated, the
contamination rate of the donors tends to be lower than the rate observed in the population in
general(22).
13
The ultra-low temperature is thought to be able to rupture the cell membrane through
the crystallization of the water in the cells, makes the tissue bacteria free. The presence of live
cells in the fresh and cryopreserved bone samples was observed in the studies of Heyligers
and Klein-Nulend(23). Risk reduction for virus transmission and bacterial contamination with
this type of transplantation still depends on effective serum tests of the donor. In Brazil, the
Skeletal Muscle Tissue Banks follow the standards and procedures recommended by the
Sistema Nacional de Transplantes – SNT (Transplantation National System).
The prevalence of disease transmission through Fresh Frozen Bone transplantation is
low, considering the high number of procedures conducted today(24). A study with 138
patients who underwent arthroplasty of the hip using this type of transplantation showed
infection rates lower than 1% and these were proved not to be due to the transplanted
tissue(25).
Another factor to be considered when using Fresh Frozen Bone for transplantation is
the potential immune reaction, which includes transplanted tissue rejection. The ultra-low
temperature cryopreservation reduces graft immunogenicity(26). Therefore, there is no need to
submit receptors to immunosuppression, although the meaning and the incidence of the
immune response to this type of graft material are still not well established.
Some studies attempted to explain the risk factors of using bone grafts through the
analysis of human leukocyte antigen (HLA) in blood samples. The comparison of
pretransplant serum of 40 patients(27), followed by HLA analyses of samples after 3, 6, 9, 12,
18 and 24 months, revealed that sensitization occurred in 53% of the cases studied. No
evidence was found, however, linking this sensitization as a risk factor influencing the
incorporation of the bone graft. Another multicenter study(28) evaluated 84 patients
transplanted with fresh and frozen allograft bone. Serum samples for HLA analysis were
obtained before surgery, and during a follow-up period from 1 month to 4 years after surgery.
14
Sensitization before transplanting was shown in an average of 39% of the cases, probably due
to a positive history of blood transfusions and pregnancies. After grafting, there was an
increase in the average of sensitization cases from 39% to 67%, with evidence of the potential
immune sensitization. Notwithstanding, the link between this sensitization and grafting
success was not conclusive.
The use of fresh and frozen human bone is based on the selection of a material that
safely maintains as much as possible of the desirable properties, biological and
biomechanical, for maxillomandibular bone reconstruction.
The maintenance of the biological properties (still quantitatively uncertain) basically
refers to maintaining the bone-inducing potential of the bone graft. The death of the bone
matrix is believed to provide osteoblast-inducing factors and other essential proteins and/or an
osteoclast substrate for direct bone remodeling(29).
As to the maintenance of biomechanical properties, it is important to notice that the
peri-implant bone is frequently submitted to mechanical stress. Therefore, the formation of
bone with good density is desirable. Cryopreservation maintains the structural characteristics
of osseous tissue(30), and this is an important factor for the promotion of a proper osseous
conduction. Onlay block grafts lose their structural integrity when submitted to lyophilization
or irradiation(12, 18,30).
The fresh frozen bone discussed in this paper has been used for a long time in
orthopedics, but there is limited literature in oral and maxillofacial surgery(31).
In this study, all graft surgeries were carried out with platelet rich plasma placed
between the bone block and the receptor bed. This was done in the cases of onlay block graft,
as well as when added to the particulate bone used for maxillary sinus augmentation, in order
to accelerate new bone formation(32) and to facilitate the handling of the particulate
material(33).
15
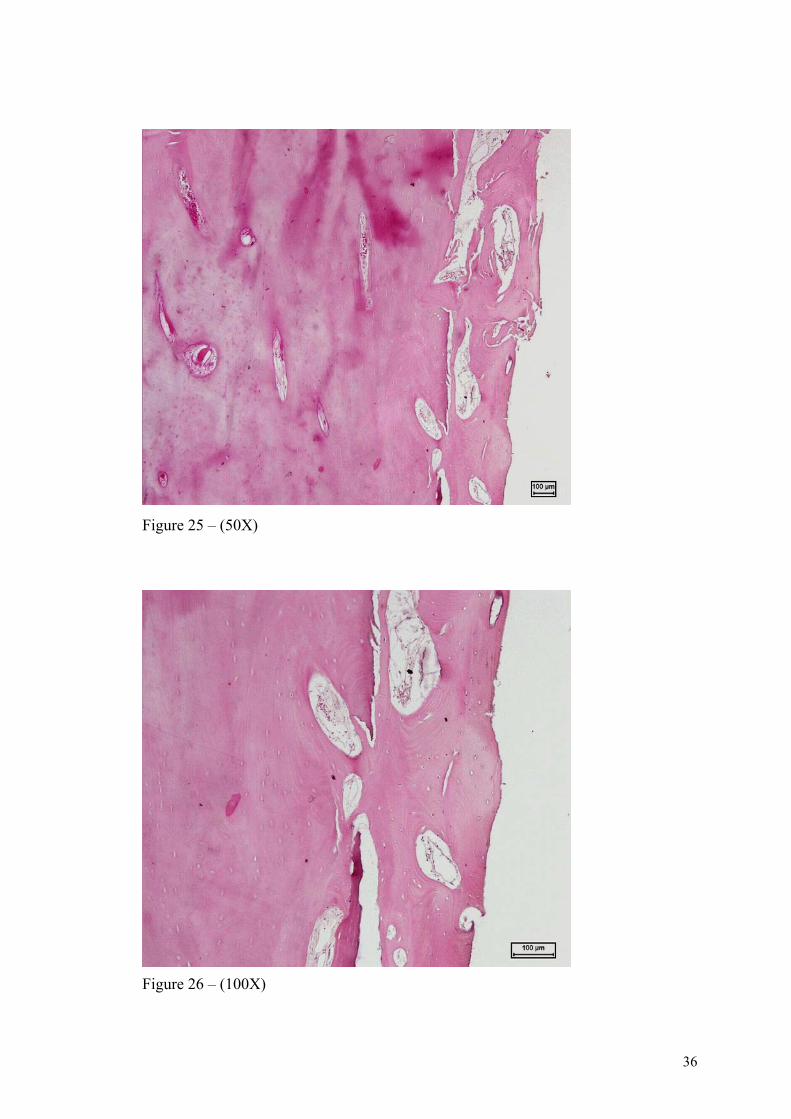
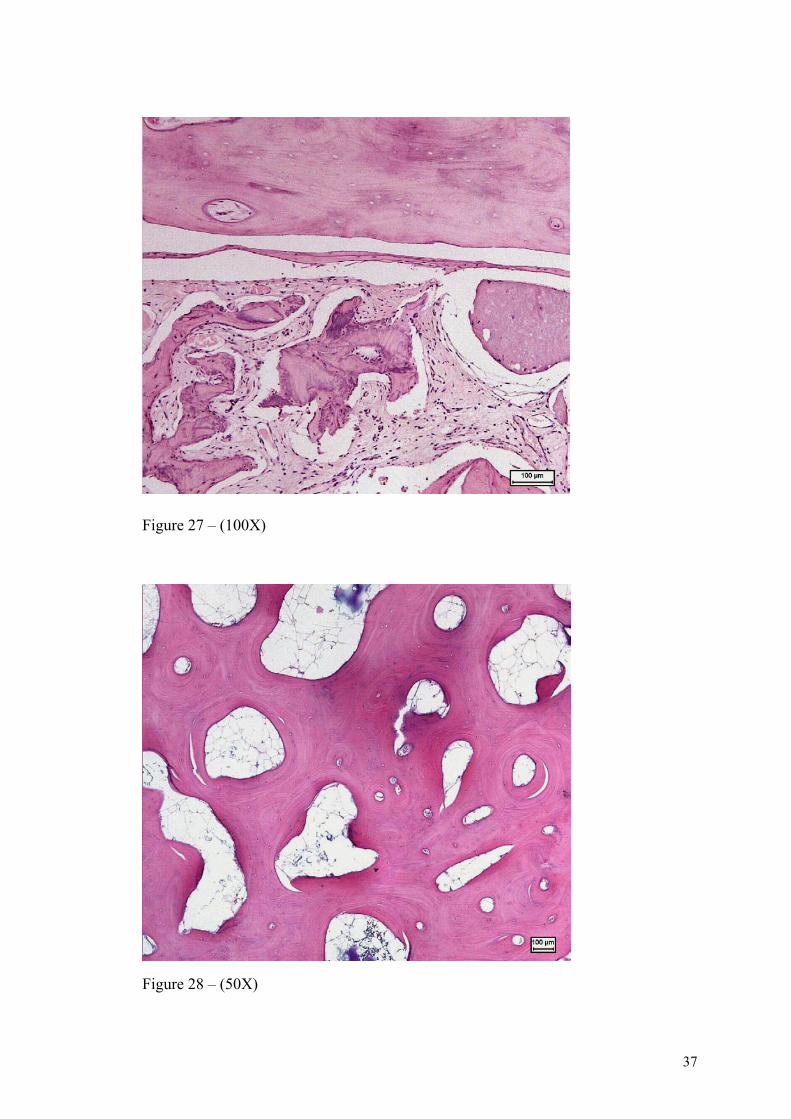
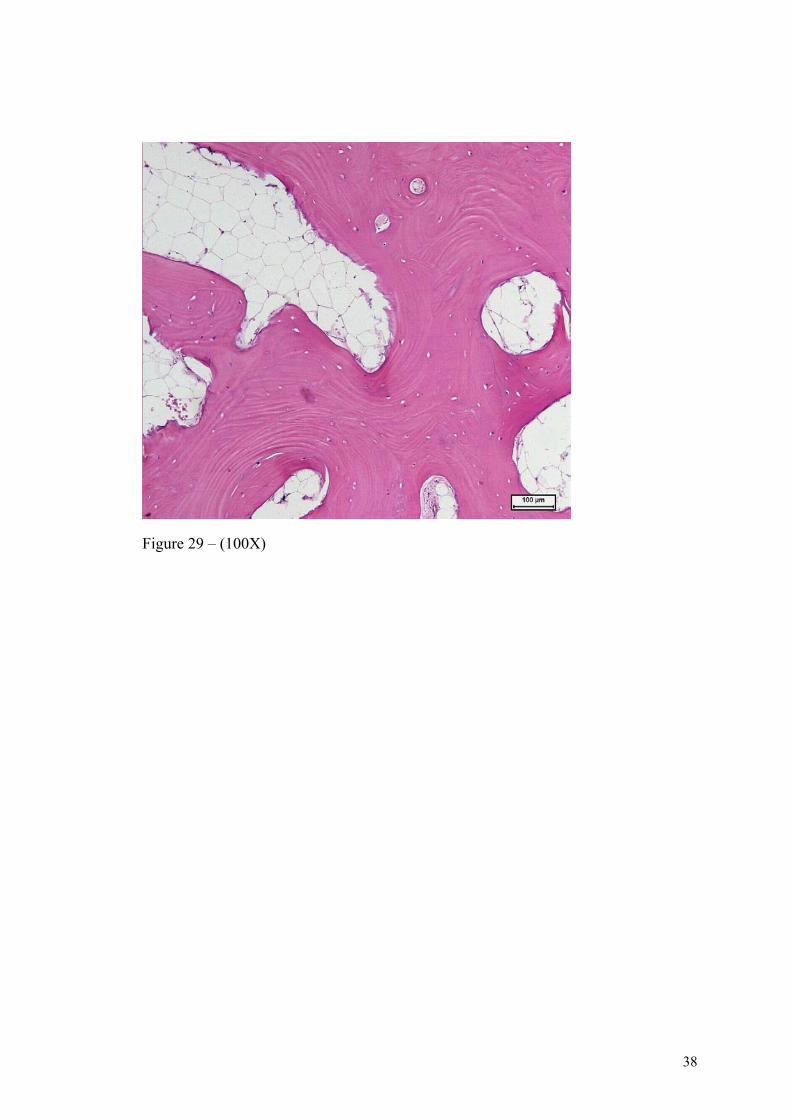
It is possible to see the ossification on the histological study. These histological
sections were obtained at the time of implant placement and focus on the interface between
receptor bone and graft.
The sections examined reveal bone tissue composed of mature trabeculae with
osteocytes inside surrounded by medullary connective tissue, rich in blood vessels, fibers and
cells with normal histological appearance.
Images 25, 26 and 27 show the interface between the implanted bone tissue (left),
which is more compact and without osteocytes, and the bone formed after grafting (right).
Images 28 and 29 show the bone formed after grafting in more detail.
Today, immediate or early prosthetic rehabilitation on implants for edentulous
maxillas is a predictable and reliable procedure(4,34). In addition, the possibility of using
osseointegrated implants for reconstructed maxillas through bone grafting is well
demonstrated(10,11,35,36) and represents today a relatively common treatment alternative.
In this study, at the time of the graft reopening and placement of the implants, the
bone appeared to be of excellent quality. This property provided good initial stability, with
insertion torque higher than 32N, sufficient to indicate immediate loading(3,37). A discrete
bone resorption was observed, probably due to the graft being cortical.

16
Conclusions
Reconstruction of atrophic maxillas using Fresh Frozen Bone presented encouraging
results with preservation terms of up to 42 months. In addition, immediate loading on
edentulous maxillas is viable as long as there is quality bone structure in a sufficient amount
to enable good distribution and primary stability of the implants. However, this is still a
fruitful field for further research.
17
References
1. Jaffin RA, Kumar A, Berman CL. Immediate loading of implants in partially and fully edentulous jaws. A series of 27 case reports. J Periodontol 2000;71:833-838.
2. Rocci A, Martignoni M, Gottlow J. Immediate function of single and partial reconstructions in maxilla using MKIV fixtures.A retrospective analysis. Appl Osseointegration Res 2001;2;22-6.
3. Uribe R, Peñarrocha M, Balaguer J, Fulgueiras N. Immediate loading in oral implants. Present situation. Med Oral Patol Oral Cir Bucal 2005;10(2):E143-53.
4. Cooper L, De Kok IJ, Reside GJ, Pungpapong P, Rojas-Vizcaya FV. Immediate fixed restoration of the edentulous maxilla after implant placement. J Oral Maxillofac Surg 2005;63(2):97-110.
5. Raghoebar GM, Schoen P, Meijer HJA, Stellingsma K, Vissink A. Early loading of endosseous implants in the augmented maxilla: a 1-year prospective study. Clin Oral Impl Res 2003;14:697-702.
6. Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg 1988;17:232-6.
7. Jacotti M. Simplified onlay grafting with a 3-dimensional block technique: a technical note. Int J Oral Maxillofac Implants 2006, 21:635-639.
8. Desjardins RP. Prothesis Design for Osseointegrated Implants in Edentulous Maxilla. Int J Oral Maxillofac Implants 1992;7:311-20.
9. Sjöström M, Sennerby L, Nilson H, Lundgren S. Reconstruction of the Atrophic Edentulous Maxilla with Free Iliac Crest Grafts and Implants: A 3-Year Report of a Prospective Clinical Study. Clin Oral Implants Res 2007;15:46-59.
10. Clayman L. Implant Reconstruction of the Bone-Grafted Maxilla: Review of the Literature and Presentation of 8 Cases. J Oral Maxillofac Surg 2006;64:674-82.
11. Leung ACF, Cheung LK. Dental Implants in Reconstructed Jaws: Patients’ Evaluation of Functional and Quality-of-Life Outcomes. Int J Oral Maxillofac Implants 2003;18:127-34.
12. Nather A, Thambyah A, Goh JC. Biomechanical strength of deep-frozen versus lyophilized large cortical allografts. Clin Biomech (Bristol, Avon) 2004;19:526-33.
13. Urist MR. Fundamental and Clinical Bone Physiology. Philadelphia, JB Lippincott Co, 1980.
14. Simion M, Jovanovic SA, Trisi P, Scarano A, Piattelli A. Vertical ridge augmentation around dental implants using a membrane technique and autogenous bone or allografts in humans. Int J Periodont Rest Dent 1998;18:9-23.
18
15. Caplanis N, Sigurdsson TJ, Rohrer MD, Wikesjö UME. Effect of allogenic, freeze-dried, demineralized bone matrix on guided bone regeneration in supra-alveolar peri-implant defects in dogs. Int J Oral Maxillofac Implants 1997;12:634-42.
16. Loty B, Courpied JP, Tomeno B, Postel M, Forest M, Abelanet R. Bone allografts sterilizedsterilised by irradiation. International Orthop 1990;14:237-42.
17. Hernigou P, Kergrohen F, Février MJ, Goutallier D. Ètude du risque de transmission di virus HIV lors d'une intervencion programmée en chirurgie orthopédique et mesures préventives. Revue du Rheumatisme 1991;58(6):427-31.
18. Power RA, Day RE, Wood DJ. The effects of gamma irradiation on the biomechanical properties of human cortical bone. J Bone Joint Surg [Br] 1995;77B(Supp III):321.
19. Robinson DE, Lee MB, Smith EJ, Learmonth ID. Femoral impactions grafting in revisionship arthroplasty with irradiated bone. J Arthroplasty 2002;17:834-40.
20. Thoren K, Aspenberg P. Ethylene oxide sterelization impairs allograft incorporationin a conduction chamber. Clin Orthop 1995;318:259-64.
21. Friedlander GE. Bone grafts: the basic science rationale for clinical applications. J Bone Joint Surg [Am] 1987;69-A:786-90.
22. Zou S, Dodd RY, Stramer SL, Michael Strong DM. Probability of Viremia with HBV, HCV, HIV and HTLV among Tissue Donors in the United States. N Engl J Med 2004;351:751-9.
23. Heyligers IC, Klein-Nulend J. Detection of living cells in non-processed but deep-frozen bone. Cell Tissue Bank 2005; 6(1):25-31.
24. Tomford WW, Mankin HJ. Bone banking: update on methods and materials. Orthop Clin North Am 1999;30:565-70.
25. Kwong FNK, Ibrahim T, Power RA. Incidence of infection with the use of non-irradiated morcellised allograft bone washed at the time of revision arthroplasty of the hip. J Bone Joint Surg Br 2005;87(11):1524-6.
26. Weyts FA, Bos PK, Dinjens WN, van Doorn WJ, van Biezen FC, Weinans H. et al. Living cells in 1 of 2 frozen femoral heads. Acta Orthop Scand 2003;74(6):661-4.
27. Ward WG, Heise E, Boles C, Kiger D, Gautreaux M, Rushing J. et al. Human leukocyte antigen sensitization after structural cortical allograft implantations. Clin Orthop Relat Res 2005;(435):31-5.
28. Strong DM, Friedlander GE, Tomford WW, Springfield DS, Shives TC, Burchardt H. et al. Immunologic responses in human recipients of osseous and osteochondral allografts. Clin Orthop 1996;326:107-14.
29. Kingsmill VJ, Boyde A, Jones SJ. The resorption of vital and devitalized bone in vitro. Calcif tissue 1999;64:252-6.
19
30. Hamer AJ, Strachan M, Black M, Ibbotson CJ, Stockey I, Elson RA. Biomechanical properties of cortical allograft bone using a new method of bone strength measurement: A comparison of fresh, fresh-frozen and irradiated bone. J Bone Joint Surg Br 1996;78-B:363-8.
31. Benetton AA, Borges LFA, Marques C. Reconstruction of atrophic maxilla with the use of allograft bone (fresh and frozen bone) and implants immediate loading. Implant News 2007; 4(5):529-34.
32. Gerard D, Carlson ER, Gotcher JE, Jacobs M. Healing of autologous bone grafted mandibular defects in dogs J Oral Maxillofac Surg 2006;64:443-51.
33. Froum SJ, Wallace SS, Tarnow DP, Cho SC. Effect of Platelet-Rich Plasma on Bone Growth and Osseointegration in Human Maxillary Sinus Grafts: Three Bilateral Case Reports. Int J Periodontics Restorative Dent 2002;22:45-53.
34. Jaffin RA, Kumar A, Berman CL. Immediate loading of dental implants in the completely edentolous maxilla: A clinical report. Int J Oral Maxillofac Implants 2004;19:721-30.
35. Cheung LK, Leung ACF. Dental Implants in Reconstructed Jaws: Implant Longevity and Peri-Implant Tissue Outcomes. J Oral Maxillofac Surg 2003;61:1263-74.
36. Gerry M, Raghoebar PS, Henny JA, Meijer KS, Arjan V. Early loading of endosseous implants in the augmented maxilla: a 1-year prospective study. Clin Oral Impl Res 2003;14:697-702.
37. Ottoni JM, Oliveira ZF, Mansini R, Cabral AM. Correlation between placement torque and survival of single-tooth implants. Int J Oral Maxillofac Implants 2005;20(5):769-76.
20
Table 1 - Patients treated, period in use and complications found
Patient Age Sex Period in use (months)
Intercurrences
LPF 44 F 44 No AML 40 F 27 No NN 44 M 21 No DF 61 M 20 Graft exposure AP 52 F 18 No MAM 65 F 18 No SPS 54 F 14 No VGM 65 M 12 No WTP 45 F 12 No KT 64 M 12 No NPF 67 F 11 No AGA 52 M 9 No GV 48 M 6 No
ERP 53 M 6 No
21
Legends of the illustrations
Figure 1 – Computerized tomographic scan – Axial slice before grafting
Figure 2 – Computerized tomographic scan – 3-dimensional reconstruction before grafting
Figure 3 – Prototype before grafting
Figure 4 – Band-form tibial fresh frozen bone
Figure 5 – Verification of bone adaptation on prototype
Figure 6 – Adjustments for bone adaptation on prototype
Figure 7 – Occlusal view after incision and mucoperiosteal detachment
Figure 8 a – Utilization of bone mill
Figure 8b – Particulate bone
Figure 9 – Particulate bone associated to autogenous platelet-rich plasma
Figure 10 – Access window to maxillary sinus filled with particulate bone
Figure 11 – Adaptation of bone blocks to the receptor bed
Figure 12 – Fixation of bone blocks to the receptor bed
Figure 13 – Occlusal view of the suture
Figure 14 a – Computerized tomographic scan – Axial slice 6 months after grafting
Figure 14 b – Computerized tomographic scan – 3-dimensional reconstruction 6 months after grafting
Figure 14 c – Prototype after grafting
Figure 15 – Multifunctional surgical template
Figure 16 – Front view after incision and detachment for the implant placement surgery
Figure 17 – Multifunctional template with implants placed in position
Figure 18 – Impression copings in position
Figure 19 – Impression with multifunctional template in position and splinted impression copings
Figure 20 – Healing abutments in position (24 hours after surgery)
Figure 21 – Acrylized prosthesis
Figure 22 – Prosthesis in place
Figure 23 – Radiographic image 12 months after prosthesis installation
Figure 24 – Front view of prosthesis in function
Images 25, 26 and 27 show the interface between the implanted bone tissue (left), which is more compact and without osteocytes, and the bone formed after grafting (right).
Images 28 and 29 show the bone formed after grafting in more detail.
22
Ilustrations
Figure 1
Figure 2
23
Figure 3
Figure 4
24
Figure 5
Figure 6
25
Figure 7
Figure 8 a
26
Figure 8b
Figure 9
27
Figure 10
Figure 11
28
Figure 12
Figure 13
29
Figure 14 a
Figure 14 b
30
Figure 14 c
Figure 15
31
Figure 16
Figure 17
32
Figure 18
Figure 19
33
Figure 20
Figure 21
34
Figure 22
Figure 23
35
Figure 24
36
Figure 25 – (50X)
Figure 26 – (100X)
37
Figure 27 – (100X)
Figure 28 – (50X)
38
Figure 29 – (100X)










![Rehabilitation of atrophic jaw using iliac onlay bone ...routine treatment for the rehabilitation of partially and totally edentulous patients [1]. Sufficient residual bone volume](https://img.pdfslide.net/doc/110x75/5f5d63a58b24f126055f3fbd/rehabilitation-of-atrophic-jaw-using-iliac-onlay-bone-routine-treatment-for.jpg)