Embed Size (px)
Citation preview
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 1 of 38
Records Management Policy
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 2 of 38
DOCUMENT CONTROL SHEET
Document Owner: Director of Nursing and Quality
Document Author(s): Company Secretary
Version: 4.1 Final
Directorate: Nursing and Quality
Approved By: Governance and Audit Committee
Date of Approval: March 2015
Date of Review: March 2017
Change History:
Version Date Reviewer(s) Revision Description
v3.0 18/09/2013 Caroline Law Final
v3.1 29/01/2015 Charlotte Travill Reformat
v4.0 March 2015 Sarah Feal Review of subject matter, Roles and responsibilities
v4.0 March 2015 IG Forum Review and agreement. Minor update to Retention and Disposal Schedule to include Continuing Healthcare
v4.1 March 2015 Governance and Audit Committee
Policy Approved
Implementation Plan:
Development and Consultation
Governance and Audit Committee Information Governance Forum
Dissemination Staff can access this policy via the Intranet and will be notified of new/revised versions via the staff briefing.
This policy will be included in the CCG's Publication Scheme in compliance with the Freedom of Information Act (FOI) 2000.
Training All staff members are required to carry out the mandatory IG training through the online NHS Information Governance Training Tool.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 3 of 38
Monitoring The Records Management Policy shall be monitored by the Information Governance Forum.
Staff must raise risks and issues regarding the safety and security of information and any practices which do not conform to this policy, or any other related information governance policies and/or risk frameworks. Incident reports and results of risk assessments will be used for monitoring purposes.
Review The implementation of this policy will be in line with the Records Management Strategy (Appendix 1) and will be managed by the Company Secretary.
The Records Management Policy will be reviewed bi-annually or in response to any organisational, regulatory or legislative changes.
Equality, Diversity and Privacy
March 2015 - Equality Impact Assessment
March 2015 - Privacy Impact Assessment
Associated Documents
• Freedom of Information Policy • Information Governance Policy
References Legislation • Access to Health Records Act 1990 • Data Protection Act 1998 • Freedom of Information Act 2000
Guidance and Standards • Information Governance Toolkit • Access to Health Records, Department of
Health (2010) • NHS Information Governance: Guide on Legal
and Professional Obligations (2007) • Records Management: NHS Code of Practice,
Department of Health (2008) • Records management: NHS Code of Practice
Parts 1 (2006) and Part 2 (2009), Department of Health
• Care Quality Commission standards • NHS Litigation Authority standards
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 4 of 38
Table of Contents
Section No. Section Name Page No.
1.0 Introduction 6
2.0 Scope 6
3.0 Purpose 7
4.0 Definitions 7
5.0 Roles and responsibilities 8
6.0 Process/Procedure for • The Information Lifecycle • Information Quality • Access to Information
9
Appendix 1 Records Management Policy 15
Appendix 2 Archiving Procedure 16
Appendix 3
Retention and Disposal Schedule 18
Appendix 4 Internal Confidential Courier Service (“Red bag” scheme)
28
Appendix 5 Equality Impact Assessment Stage 1 Screening 38
Appendix 6 Privacy Impact Assessment Stage 1 Screening 39
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 5 of 38
1.0 Introduction 1.1 NHS East and North Hertfordshire Clinical Commissioning Group (CCG)
recognise the need for an appropriate balance between openness and confidentiality in the management and use of information. The CCG fully supports the principles of corporate governance and recognises its public accountability, but equally places importance on the confidentiality of, and the security arrangements to safeguard, both personal information about patients and staff and commercially sensitive information.
1.2 The CCG also recognises the need to share information with other
health organisations and agencies in a controlled manner consistent with legislative requirements.
1.3 The CCG believes that timely and relevant information is essential to
deliver highest quality standards. As such it is the responsibility of all staff to ensure and promote the quality of information and to actively use information in decision making process.
1.4 The CCG works to a framework for handling personal information in a
confidential and secure manner to meet ethical and quality standards. This enables National Health Service organisations in England and individuals working within them to ensure personal information is dealt with legally, securely, effectively and efficiently to deliver the best possible care to patients and clients.
1.5 The CCG, via the Information Governance Toolkit, provides the means
by which NHS England can assess compliance with current legislation, Government and National guidance.
1.6 Information Governance (IG) covers: Data Protection & ICT Security
(including smart cards), Human Rights Act, Caldicott Principles, Common Law Duty of Confidentiality, Freedom of Information Regulations and Information Quality Assurance .
2.0 Scope 2.1 This policy applies to all CCG staff members, including Governing Body
Members and Practice Representatives whether permanent, temporary or contracted-in (either as an individual or through a third party supplier).
2.2 The policy sets out the main requirements for the management of all
clinical and corporate records within the CCG including but not limited to:
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 6 of 38
• All administrative records (e.g. personnel, estates, financial and accounting records, service level agreements, notes associated with complaints); and
• All service user health records (including their medical case notes, nursing care plans, visual or audio recordings, registers etc.)
2.3 The information lifecycle management policy applies to records in all
formats, whether electronic and those stored in various forms including photographs, x-rays, audio messages and CCTV images.
3.0 Purpose 3.1 The purpose of this policy is to ensure a consistent and effective
approach to the management of all information and/or records within the CCG.
3.2 Records are a valuable resource and must be efficiently managed and
available to those with authorised access in order to:
• Support the CCG’s administrative and managerial decision making. • Meet legal requirements including requests from service users under
access to records legislation. • Assist in providing evidence for internal and external reviews and other
audits. • Support day-to-day business. • Provide clinical and managerial effectiveness through multi-disciplinary
working within the CCG and with partner agencies. 3.3 This will help to enable:
• the formation and accountability / transparency in use of public resources;
• the empowerment of the CCG to support improvements through audit, research and archival functions by taking account of the historical importance of material and the needs of future research; and
• support of the investigation of complaints, claims and incidents. 4.0 Definitions 4.1 Archives - Records that are appraised as having permanent value for
evidence of on-going rights or obligation, for historical or statistical research or as part of the corporate memory of the organisation.
4.2 Destruction - The process of eliminating or deleting records beyond
any possible reconstruction (BS ISO 15488-1:2001). 4.3 Public records – Records as defined in the Public Records Act 1958 or
subsequently determined as public records by The National Archives.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 7 of 38
4.4 Records - This applies to electronic and paper records/information that provides evidence of actions and decisions made by the organisation. Records are the organisations corporate memory.
4.5 Records management - field of management responsible for the
efficient and systematic control of the creation, receipt, maintenance, use and disposal of records. Records management includes processes for capturing and maintaining evidence of and information about business activities and transactions in the form of records.
5.0 Roles and Responsibilities 5.1 Chief Executive
The Chief Executive is the Accountable Officer and is responsible for the management of records across the CCG and for ensuring appropriate mechanisms are in place to support service delivery and continuity. The Accountable Officer has ultimate responsibility for compliance with IG legislation.
5.2 The Information Governance Forum The Information Governance Forum is responsible for ensuring that this policy is implemented, including any supporting guidance and training deemed necessary to support the implementation, and for monitoring and providing Governing Body assurance in this respect.
5.3 The Caldicott Guardian The CCG’s Caldicott Guardian is the Director of Nursing and Quality and has a particular responsibility for reflecting patients’ interests regarding the use of patient identifiable information. The Caldicott Guardian has an advisory role and a particular focus on ensuring patient identifiable information is shared in an appropriate and secure manner.
5.4 Company Secretary The Company Secretary is responsible for advising on records management strategic direction, the development of policy and guidance for the CCG and the day to day management of the records management agenda.
5.5 The Senior Information Risk Owner
The CCG’s Senior Information Risk Owner (SIRO) is the Chief Finance Officer and also the Chair of the Information Governance Forum. The SIRO is accountable for information risk on the Governing Body and in internal discussions. They will provide written advice to the Accountable Officer on the content of their Annual Governance Statement in regard to information risk.
5.6 Governance Support Officer
The Governance Support Officer will manage the archiving process and identify records for secure disposal.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 8 of 38
5.7 Line Managers Line Managers are responsible for ensuring compliance within their areas, making sure records management issues are addressed and key performance targets around record keeping including retention schedules and training are met. Line Managers need to be fully conversant with the electronic records and computer system and supplementary reporting procedures that are used in their service area. Where further advice is required, the Company Secretary should be contacted.
5.8 Healthcare professionals Healthcare professionals have a duty to:
• Keep up to date, and adhere to, relevant legislation and national and local policy relating to information and record keeping.
• Keep up to date on best practice for health/social care records and communication practice standards
• Be proficient in the system they use to record and communicate health and social care information
• Meet the standards of their professional organisation.
5.9 All Staff All staff and anyone working on behalf of the CCG, involved in the receipt, handling or communication of person identifiable information, must adhere to this policy at all times and where relevant of their professional codes and standards. Anyone who records, handle, store or otherwise comes across person or patient identifiable information has a common law duty of confidence. This duty continues even after the death of an individual.
6.0 Processes and Procedures for: 6.1 Information Lifecycle
The Information lifecycle defines five distinct phases: Creation, Retention, Maintenance, Use and Disposal
1. Creation When creating information or records, the following should be adhered to. The information must be: • Available when needed • Accessible to all members of staff that require access in order to
enable them to carry out their day to day work • Interpretable, clear and concise • Trusted, accurate and relevant • Secure – the information must be secure from unauthorised access
or inadvertent alteration or erasure
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 9 of 38
2. Retention Information retention period varies dependant on the type of records and are retained for legal, operational, research and safety reasons. Some items may be considered for permanent preservation. For retention periods of documents held by the CCG please refer to the Retention and disposal schedule in Appendix 3.
3. Maintenance The qualities of availability, accessibility, interpretation and trustworthiness of information must be maintained for as long as the information is needed, perhaps permanently, despite changes in the format. The use of standardised filenames and version control methods should be applied consistently throughout the life of the information.
• Scanning – A brief summary should be entered into the scanned
document, with a reference to where the original is stored; i.e. the secondary paper file. All scanned documents must be dated and titled appropriately to enable easy identification and retrieval. The date should reflect the date of the correspondence/activity/incident, not the date it is being attached to the record.
• Archiving – For legal and organisational reasons, information must be
stored securely. Electronic records are automatically backed up and archived.
Contents within manual/paper records should be stored chronologically, the most recent part of the records accessible first. Storage arrangements must allow for retrieval with speed of access dependant on the urgency of requirement of access to the information. The procedure for archiving is in Appendix 2 of this policy. For further information and guidance on archiving, contact the Governance Support Officer.
• Tracing records – Tracer cards are in place to track the whereabouts
of records. Examples would include critical incident review files, complaints files. The minimum data which needs to be recorded includes: the name of the file; date the file was dispatched, destination and name of recipients, name of person releasing the file. A return receipt should always be requested and made clear to whom the records should be returned and by when. A chase and tracking system must be operated to ensure the file is safely returned to the relevant filing system and that absent records are chased regularly.
4. Use All information must be used and handled consistently with the purpose for which it was intended.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 10 of 38
• Disclosure – only the specific information should be disclosed to authorised parties and always in accordance and with strict adherence to the legislations.
• Transfer – the mechanism for transferring information from one
organisation to another should also be tailored to the sensitivity of the material contained within the records and the media on which they are held. The Head of Governance and ICT Infrastructure Manager can advise on appropriate safeguards. Public authorities are required to transfer certain information to The National Archive for permanent retention. The Head of Governance can provide guidance on such records.
• Posting confidential documents - Documents/clinical records should be put in a strong envelope, marked private and confidential and sent via special delivery. Confidential documents sent internally need to be put either in an internal transfer envelope or an envelope strong enough to take the contents and placed in a courier bag with a seal tab (tamper proof wallet/red bag). The envelope needs to clearly state the recipient and their full address, avoid abbreviations. The recipient of the document should inform the sender that the document has arrived as per the instructions on the tracer card. Access to health records ensures service user safety and continuity of care; a risk assessment needs to be carried out to ensure that the appropriate method of transportation is used. See Appendix 4 for more details of the internal confidential courier service (“red bag”) procedure.
• Closure – Records should be closed and transferred to secondary
storage as soon as they cease to be active. Where paper records or files have been closed, the date of closure and possible disposal date should be noted on the records. Where possible information on the intended disposal dates for electronic data should be maintained.
5. Disposal The disposal of a record is defined under the freedom of information legislation, as the point in their lifecycle when they are either archived or destroyed. It is important that the archivalal or destruction of records are carried out in a controlled manner.
It is vital that confidentiality is safeguarded at every stage and that the method used to dispose of or destroy records is fully effective and secures their complete illegibility and inability to be reconstructed. A record of the disposed or destroyed information should be maintained for reference. Confidential waste bins have been provided for disposal of confidential paper records.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 11 of 38
6.2 Information Quality 6.2.1 It is the responsibility of all staff to ensure the information generated or
received is legible, accurate, up to date and accessible. The quality of information produced can have a significant impact on the quality and efficiency of decision making and services provided by the CCG.
6.2.2 Naming conventions
The following rules should be followed when generating or entering documents onto the computer either for clinical or non-clinical use.
• Specific information should be recorded when naming a document e.g.
the content of the document. • Logical information should also be captured e.g. the name of the
person who created the document and the date the document was created (not the date it was entered onto records).
• Each file must have: o a unique name or number e.g. service user’s NHS number to
each document and each page o a meaningful name which closely reflects and records content o express elements of the name in a structured and predictable
order
• All clinical documents should have ‘please return this document’ to the relevant service’s address on the front.
• Non- clinical records that need to be security marked should have: -
o Version control: Each document must contain a header or footer which shows the ‘Version Number’ of the document together with the date it was last modified.
o Watermarks: All draft documents must always contain a watermark stating the document is DRAFT. This will avoid confusion for any potential reader and prevent staff from believing the document may be an approved document. This will be removed once it has been finalised.
o Distribution lists: The distribution or circulation list of certain documents (e.g. agendas, consultation drafts etc.) must be clearly marked on all copies to avoid unnecessary duplication and to facilitate the recipients forwarding the document onto others who may also need to see it.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 12 of 38
6.3 Corporate and clinical records
• Records must be clear, legible and in a printable format if required for disclosure under relevant legislation.
• Jargon should be avoided and the information written in terms the staff or service user can understand.
• Paper and electronic records should clearly identify the date, time, the document author, and how it relates to other documents.
• Personal details contained in the record must be checked for accuracy and updated accordingly each time the individual sees the service user.
• Any discrepancies between electronic and paper records should be queried by the member of staff and amended accordingly.
• Unnecessary duplication between the paper and electronic record collections should be curbed.
• All information should be unambiguous, factual and consistent. Relevant, non-factual entries e.g. conclusions or opinions may be recorded and should be indicated as such.
• Records should not include personal views unless these have a potential bearing on management or service user.
• Documents which should not be disclosed should clearly be marked as such.
• Records must include details of the referral, assessment, treatment plan, progress and outcome for the service user and proposed plan of action/care and actions/care by practitioner and service user.
• A scheduled appointment or event should be created against each clinical entry where a telephone or face to face meeting with the service user, their representative, or another professional has taken place.
• Clinical notes must be entered as soon as possible following contact; the minimum standard is within 2 working days. Where this is not possible and there is a significant delay in recording the information, an explanation should be added at the start of the note, giving the reason for the delay and the date and source of any original notes taken.
• If an entry is to be highlighted, for ease of identification or to provide instruction, this should be done by using CAPITAL LETTERS and recording the name or instruction, e.g. ‘NOT FOR DISCLOSURE’ in the title or summary field.
6.4 Access to Information
6.4.1 Under the Data Protection Act 1998, living individuals have a right to request access to their personal data as held by the CCG. A written request for information known as a Subject Access Request (SAR) must be made. Details of the procedure can be found in the ‘Subject Access Request (SAR) Procedure’ document available on the Intranet.
6.4.2 Under the Freedom of Information Act 2000, the public has access to information held by public authorities. The CCG is obliged to publish certain information about its activities and members of the public are entitled to request information from the CCG.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 13 of 38
The CCG’s ‘Freedom of Information Policy’ and the ‘FOI Appeals and Complaints Procedure’ provide further details and can be accessed on the Intranet.
6.4.3 Under the Access to Health Records Act (AHRA) 1990, only specific people have the right to access the health records of someone who has died. These individuals are defined under the Act as ‘the patient’s personal representative and any person who may have a claim arising out of the patient’s death’. A next of kin does not have automatic right to a deceased individuals health records.
6.4.4 From time to time it may be necessary to provide read only access to information/records for legal and audit purposes.
Records Management Policy (v4.1) NHS East and North Hertfordshire Clinical Commissioning Group
Page 14 of 38
Appendix 1 - Records Management Strategy 1.0 Aims The aims of the Records Management Strategy are to ensure:
• a systematic and planned approach to information management, covering every stage of the lifecycle of a record;
• efficiency and best value through improvements in the quality and flow of information, and greater co-ordination of records and storage systems;
• compliance with statutory requirement; • responsibility and accountability of information and records • appropriate archiving of important records
2.0 Strategy 2.1 Responsibility and accountability - To provide a clear system of
accountability and responsibility for information and record creation, retention and use.
2.2 Information quality - To create and keep records which are adequate,
consistent, and necessary for statutory, legal and business requirements
2.3 Information use and management - To achieve systematic, orderly
and consistent creation, retention, appraisal and disposal procedures for records throughout their lifecycle.
2.4 Information security - To provide systems which maintain appropriate
confidentiality, security and integrity for records in their storage and use 2.5 Access to information – To provide clear and efficient access for those
with legitimate right of access and to ensure compliance with access to information legislation
2.6 Audit and review – To assess the level of compliance against the
Toolkit and other required standards. 2.7 Training – To provide training and guidance on legal and ethical
responsibilities and operational good practice for all staff involved in records management.
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 15 of 38
Appendix 2 - Archiving procedure Overall responsibility for archiving lies with the Company Secretary. Unless legal or clinical records, if electronic versions of documents are securely archived, then paper copies need not be retained. Responsibility for sorting, preparing, boxing up and clearly cataloguing any department’s documents for archiving rests with the department itself. Archive boxes, box labels, bar codes and log sheets are available from the Governance Support Officer at Charter House. Archiving should be prepared as follows:
Make an e-list (spread sheet) making sure you state the following clearly: name, description of contents (e.g. complaint log, NHS numbers etc. for patient related paperwork) Ideally NHS numbers should be listed and
Any departmental assigned box number
A copy of the e-list should be placed on the inside top of the archive box
Retention Period/Destruction date - see Appendix 3
2 x labels which also give details of the content of the box (the sample label below fits onto Niceday Laser Labels – EU Ref 980438)
The name of the staff member responsible for its contents
The e-list should then be sent to the Governance Support Officer
After sending the e-list the department should communicate with the Governance Support Officer to discuss where the boxes are to be located in the interim within Charter House. Boxes will then be bar coded and logged against a database before being transported by Iron Mountain to an off-site storage location.
Retrieval Contact the Governance Support Officer if you wish for a box to be retrieved from off-site archives. Destruction Please refer to the records retention and disposal list at the end of this policy for guidance. If you are unsure about disposal and retention dates or the record you hold is not mentioned in the schedule please contact the Company Secretary.
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 16 of 38
Sample label for archive boxes
Dept: (enter in your dept.name here)
NAME/TITLE OF DOCUMENTS YOU ARE ARCHIVING
BOX 1 / (enter total no. of boxes here)
Containing details of (enter general description):
1) 2) 3)
STORE DATE: (enter month here) 2015
DESTRUCTION DATE: (enter month & year here)
Owner: (enter address here) Archived by: (enter your name here) Account Details: (enter Cost Code + Account Code here if applicable)
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 17 of 38
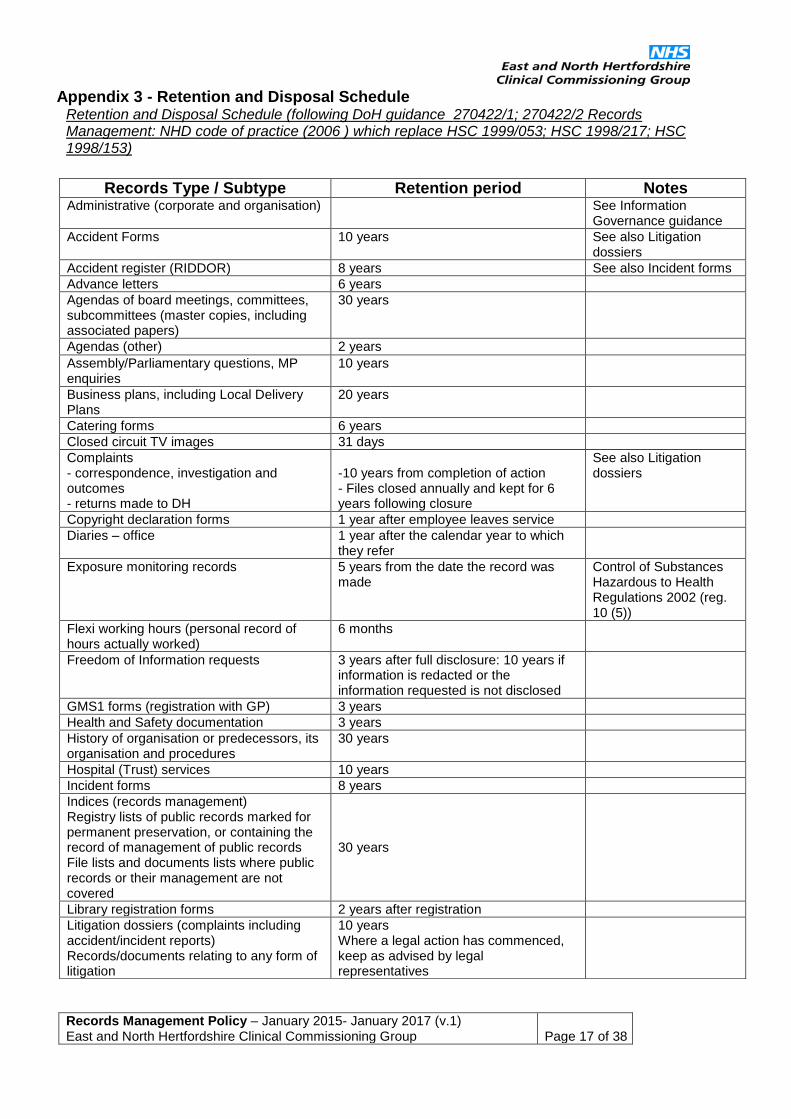
Appendix 3 - Retention and Disposal Schedule Retention and Disposal Schedule (following DoH guidance 270422/1; 270422/2 Records Management: NHD code of practice (2006 ) which replace HSC 1999/053; HSC 1998/217; HSC 1998/153)
Records Type / Subtype Retention period Notes Administrative (corporate and organisation) See Information
Governance guidance
Accident Forms 10 years See also Litigation dossiers
Accident register (RIDDOR) 8 years See also Incident forms
Advance letters 6 years
Agendas of board meetings, committees, subcommittees (master copies, including associated papers)
30 years
Agendas (other) 2 years
Assembly/Parliamentary questions, MP enquiries
10 years
Business plans, including Local Delivery Plans
20 years
Catering forms 6 years
Closed circuit TV images 31 days
Complaints - correspondence, investigation and outcomes - returns made to DH
-10 years from completion of action - Files closed annually and kept for 6 years following closure
See also Litigation dossiers
Copyright declaration forms 1 year after employee leaves service
Diaries – office 1 year after the calendar year to which they refer
Exposure monitoring records 5 years from the date the record was made
Control of Substances Hazardous to Health Regulations 2002 (reg. 10 (5))
Flexi working hours (personal record of hours actually worked)
6 months
Freedom of Information requests 3 years after full disclosure: 10 years if information is redacted or the information requested is not disclosed
GMS1 forms (registration with GP) 3 years
Health and Safety documentation 3 years
History of organisation or predecessors, its organisation and procedures
30 years
Hospital (Trust) services 10 years
Incident forms 8 years
Indices (records management) Registry lists of public records marked for permanent preservation, or containing the record of management of public records File lists and documents lists where public records or their management are not covered
30 years
Library registration forms 2 years after registration
Litigation dossiers (complaints including accident/incident reports) Records/documents relating to any form of litigation
10 years Where a legal action has commenced, keep as advised by legal representatives
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 18 of 38
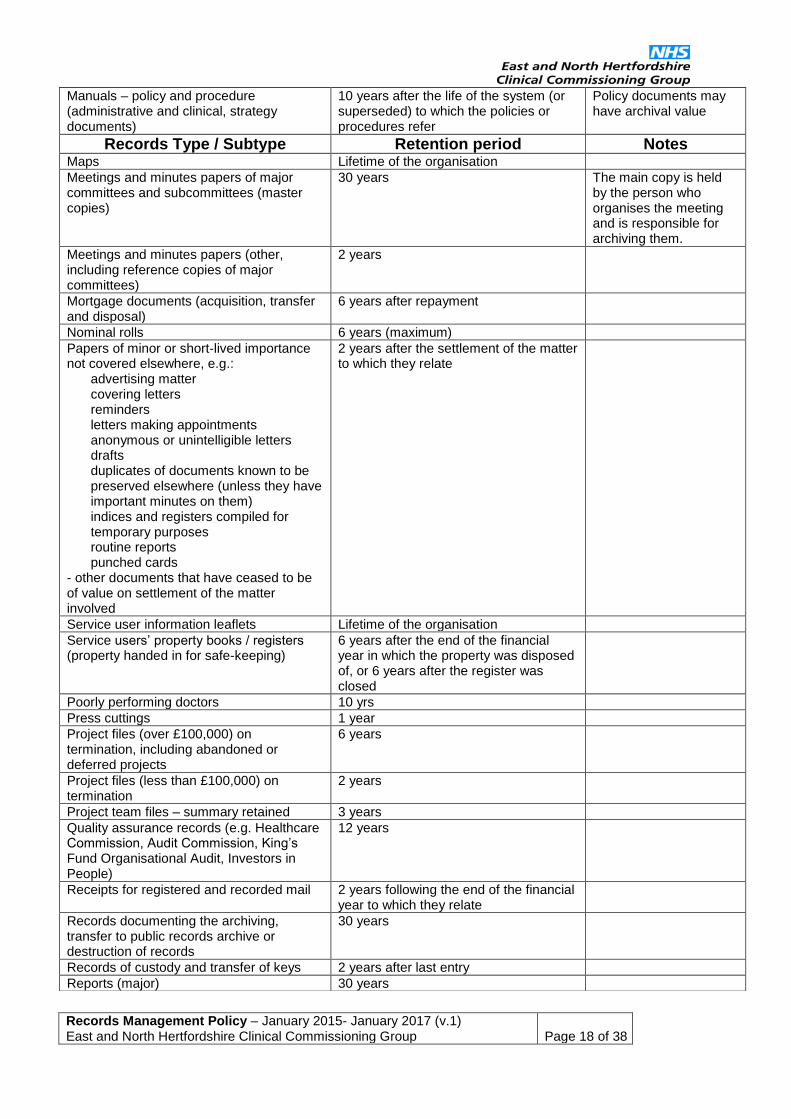
Manuals – policy and procedure (administrative and clinical, strategy documents)
10 years after the life of the system (or superseded) to which the policies or procedures refer
Policy documents may have archival value
Records Type / Subtype Retention period Notes Maps Lifetime of the organisation
Meetings and minutes papers of major committees and subcommittees (master copies)
30 years The main copy is held by the person who organises the meeting and is responsible for archiving them.
Meetings and minutes papers (other, including reference copies of major committees)
2 years
Mortgage documents (acquisition, transfer and disposal)
6 years after repayment
Nominal rolls 6 years (maximum)
Papers of minor or short-lived importance not covered elsewhere, e.g.:
advertising matter covering letters reminders letters making appointments anonymous or unintelligible letters drafts duplicates of documents known to be preserved elsewhere (unless they have important minutes on them) indices and registers compiled for temporary purposes routine reports punched cards
- other documents that have ceased to be of value on settlement of the matter involved
2 years after the settlement of the matter to which they relate
Service user information leaflets Lifetime of the organisation
Service users’ property books / registers (property handed in for safe-keeping)
6 years after the end of the financial year in which the property was disposed of, or 6 years after the register was closed
Poorly performing doctors 10 yrs
Press cuttings 1 year
Project files (over £100,000) on termination, including abandoned or deferred projects
6 years
Project files (less than £100,000) on termination
2 years
Project team files – summary retained 3 years
Quality assurance records (e.g. Healthcare Commission, Audit Commission, King’s Fund Organisational Audit, Investors in People)
12 years
Receipts for registered and recorded mail 2 years following the end of the financial year to which they relate
Records documenting the archiving, transfer to public records archive or destruction of records
30 years
Records of custody and transfer of keys 2 years after last entry
Reports (major) 30 years
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 19 of 38
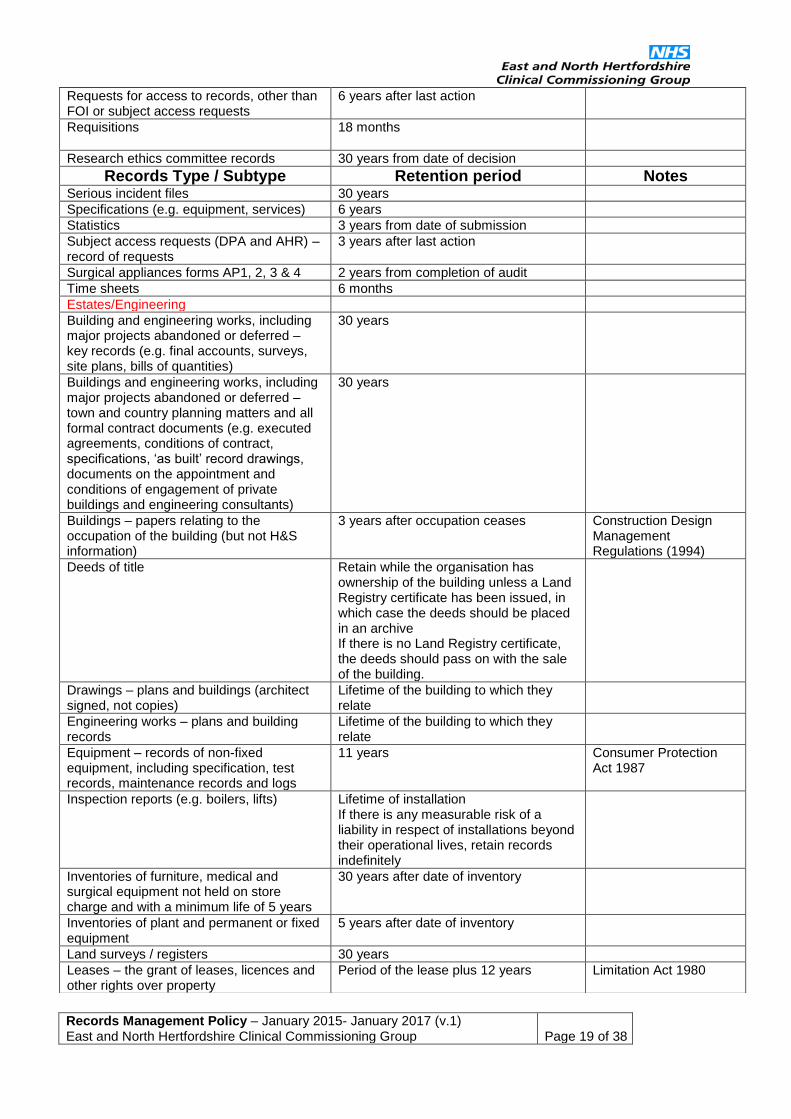
Requests for access to records, other than FOI or subject access requests
6 years after last action
Requisitions
18 months
Research ethics committee records 30 years from date of decision
Records Type / Subtype Retention period Notes Serious incident files 30 years
Specifications (e.g. equipment, services) 6 years
Statistics 3 years from date of submission
Subject access requests (DPA and AHR) – record of requests
3 years after last action
Surgical appliances forms AP1, 2, 3 & 4 2 years from completion of audit
Time sheets 6 months
Estates/Engineering
Building and engineering works, including major projects abandoned or deferred – key records (e.g. final accounts, surveys, site plans, bills of quantities)
30 years
Buildings and engineering works, including major projects abandoned or deferred – town and country planning matters and all formal contract documents (e.g. executed agreements, conditions of contract, specifications, ‘as built’ record drawings, documents on the appointment and conditions of engagement of private buildings and engineering consultants)
30 years
Buildings – papers relating to the occupation of the building (but not H&S information)
3 years after occupation ceases Construction Design Management Regulations (1994)
Deeds of title Retain while the organisation has ownership of the building unless a Land Registry certificate has been issued, in which case the deeds should be placed in an archive If there is no Land Registry certificate, the deeds should pass on with the sale of the building.
Drawings – plans and buildings (architect signed, not copies)
Lifetime of the building to which they relate
Engineering works – plans and building records
Lifetime of the building to which they relate
Equipment – records of non-fixed equipment, including specification, test records, maintenance records and logs
11 years Consumer Protection Act 1987
Inspection reports (e.g. boilers, lifts) Lifetime of installation If there is any measurable risk of a liability in respect of installations beyond their operational lives, retain records indefinitely
Inventories of furniture, medical and surgical equipment not held on store charge and with a minimum life of 5 years
30 years after date of inventory
Inventories of plant and permanent or fixed equipment
5 years after date of inventory
Land surveys / registers 30 years
Leases – the grant of leases, licences and other rights over property
Period of the lease plus 12 years Limitation Act 1980
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 20 of 38
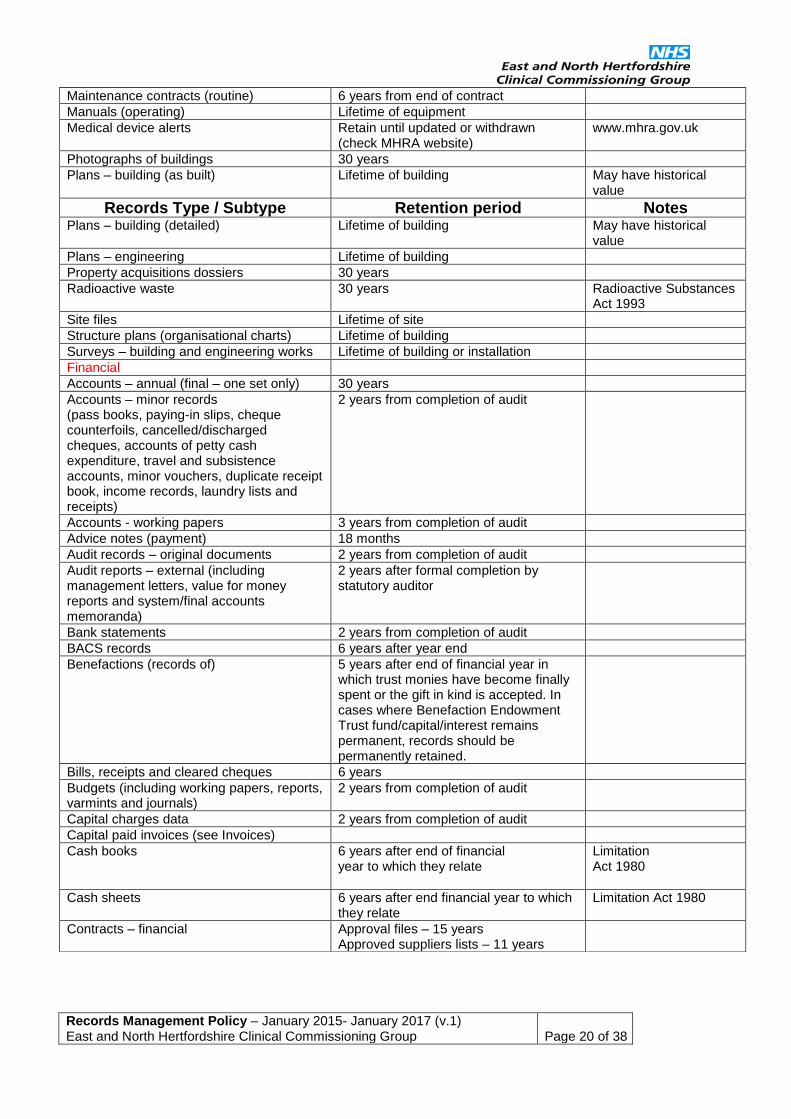
Maintenance contracts (routine) 6 years from end of contract
Manuals (operating) Lifetime of equipment
Medical device alerts Retain until updated or withdrawn (check MHRA website)
www.mhra.gov.uk
Photographs of buildings 30 years
Plans – building (as built) Lifetime of building May have historical value
Records Type / Subtype Retention period Notes Plans – building (detailed) Lifetime of building May have historical
value
Plans – engineering Lifetime of building
Property acquisitions dossiers 30 years
Radioactive waste 30 years Radioactive Substances Act 1993
Site files Lifetime of site
Structure plans (organisational charts) Lifetime of building
Surveys – building and engineering works Lifetime of building or installation
Financial
Accounts – annual (final – one set only) 30 years
Accounts – minor records (pass books, paying-in slips, cheque counterfoils, cancelled/discharged cheques, accounts of petty cash expenditure, travel and subsistence accounts, minor vouchers, duplicate receipt book, income records, laundry lists and receipts)
2 years from completion of audit
Accounts - working papers 3 years from completion of audit
Advice notes (payment) 18 months
Audit records – original documents 2 years from completion of audit
Audit reports – external (including management letters, value for money reports and system/final accounts memoranda)
2 years after formal completion by statutory auditor
Bank statements 2 years from completion of audit
BACS records 6 years after year end
Benefactions (records of) 5 years after end of financial year in which trust monies have become finally spent or the gift in kind is accepted. In cases where Benefaction Endowment Trust fund/capital/interest remains permanent, records should be permanently retained.
Bills, receipts and cleared cheques 6 years
Budgets (including working papers, reports, varmints and journals)
2 years from completion of audit
Capital charges data 2 years from completion of audit
Capital paid invoices (see Invoices)
Cash books
6 years after end of financial year to which they relate
Limitation Act 1980
Cash sheets
6 years after end financial year to which they relate
Limitation Act 1980
Contracts – financial Approval files – 15 years Approved suppliers lists – 11 years
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 21 of 38
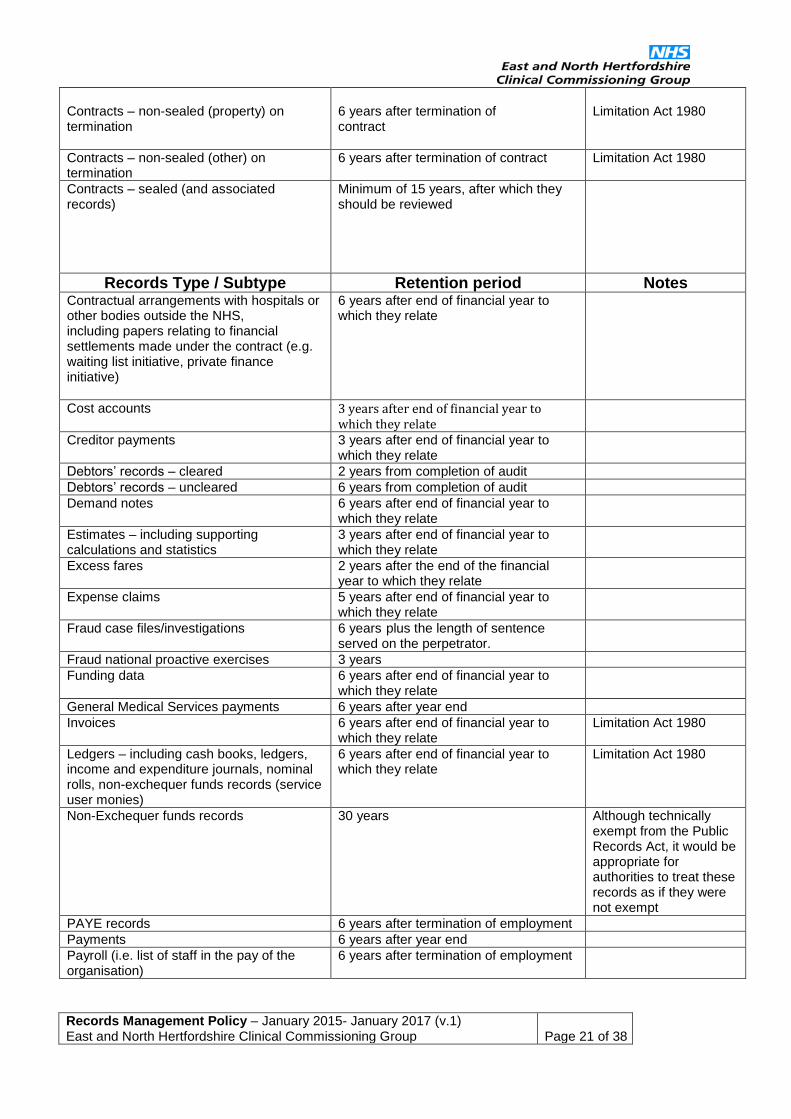
Contracts – non-sealed (property) on termination
6 years after termination of contract
Limitation Act 1980
Contracts – non-sealed (other) on termination
6 years after termination of contract Limitation Act 1980
Contracts – sealed (and associated records)
Minimum of 15 years, after which they should be reviewed
Records Type / Subtype Retention period Notes Contractual arrangements with hospitals or other bodies outside the NHS, including papers relating to financial settlements made under the contract (e.g. waiting list initiative, private finance initiative)
6 years after end of financial year to which they relate
Cost accounts 3 years after end of financial year to which they relate
Creditor payments 3 years after end of financial year to which they relate
Debtors’ records – cleared 2 years from completion of audit
Debtors’ records – uncleared 6 years from completion of audit
Demand notes 6 years after end of financial year to which they relate
Estimates – including supporting calculations and statistics
3 years after end of financial year to which they relate
Excess fares 2 years after the end of the financial year to which they relate
Expense claims 5 years after end of financial year to which they relate
Fraud case files/investigations 6 years plus the length of sentence served on the perpetrator.
Fraud national proactive exercises 3 years
Funding data 6 years after end of financial year to which they relate
General Medical Services payments 6 years after year end
Invoices 6 years after end of financial year to which they relate
Limitation Act 1980
Ledgers – including cash books, ledgers, income and expenditure journals, nominal rolls, non-exchequer funds records (service user monies)
6 years after end of financial year to which they relate
Limitation Act 1980
Non-Exchequer funds records 30 years Although technically exempt from the Public Records Act, it would be appropriate for authorities to treat these records as if they were not exempt
PAYE records 6 years after termination of employment
Payments 6 years after year end
Payroll (i.e. list of staff in the pay of the organisation)
6 years after termination of employment
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 22 of 38
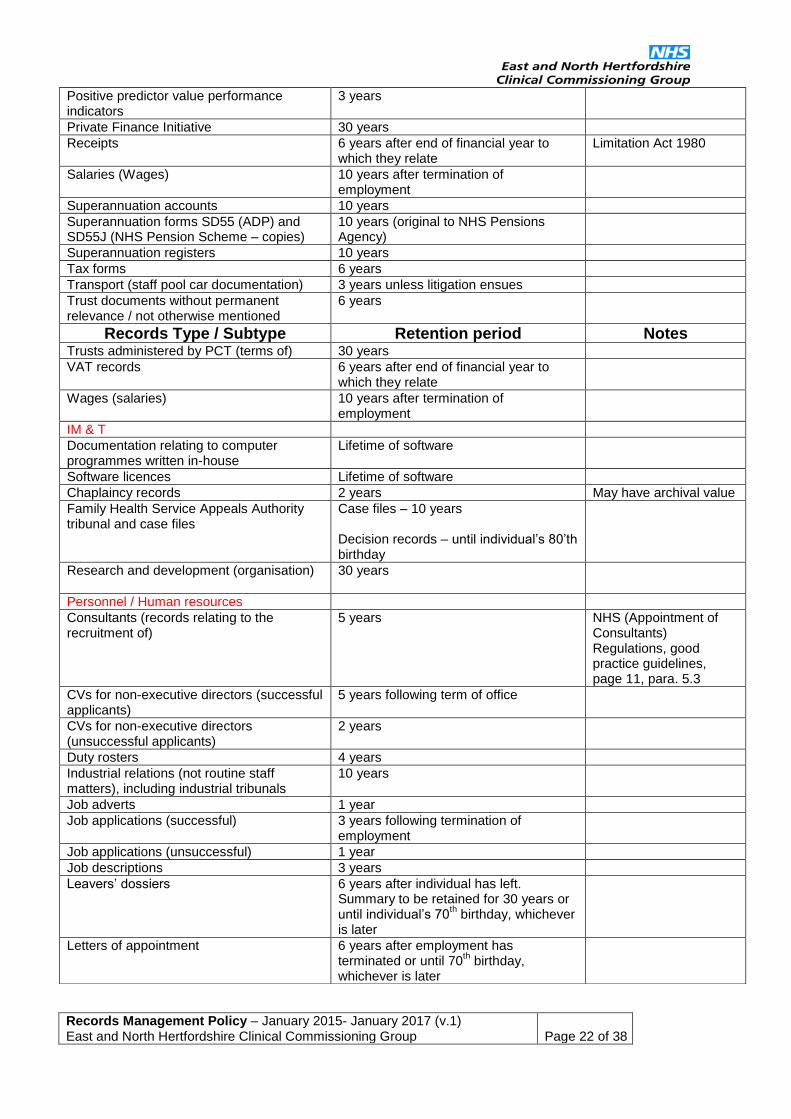
Positive predictor value performance indicators
3 years
Private Finance Initiative 30 years
Receipts 6 years after end of financial year to which they relate
Limitation Act 1980
Salaries (Wages) 10 years after termination of employment
Superannuation accounts 10 years
Superannuation forms SD55 (ADP) and SD55J (NHS Pension Scheme – copies)
10 years (original to NHS Pensions Agency)
Superannuation registers 10 years
Tax forms 6 years
Transport (staff pool car documentation) 3 years unless litigation ensues
Trust documents without permanent relevance / not otherwise mentioned
6 years
Records Type / Subtype Retention period Notes Trusts administered by PCT (terms of) 30 years
VAT records 6 years after end of financial year to which they relate
Wages (salaries) 10 years after termination of employment
IM & T
Documentation relating to computer programmes written in-house
Lifetime of software
Software licences Lifetime of software
Chaplaincy records 2 years May have archival value
Family Health Service Appeals Authority tribunal and case files
Case files – 10 years Decision records – until individual’s 80’th birthday
Research and development (organisation)
30 years
Personnel / Human resources
Consultants (records relating to the recruitment of)
5 years
NHS (Appointment of Consultants) Regulations, good practice guidelines, page 11, para. 5.3
CVs for non-executive directors (successful applicants)
5 years following term of office
CVs for non-executive directors (unsuccessful applicants)
2 years
Duty rosters 4 years
Industrial relations (not routine staff matters), including industrial tribunals
10 years
Job adverts 1 year
Job applications (successful) 3 years following termination of employment
Job applications (unsuccessful) 1 year
Job descriptions 3 years
Leavers’ dossiers 6 years after individual has left. Summary to be retained for 30 years or until individual’s 70
th birthday, whichever
is later
Letters of appointment 6 years after employment has terminated or until 70
th birthday,
whichever is later
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 23 of 38
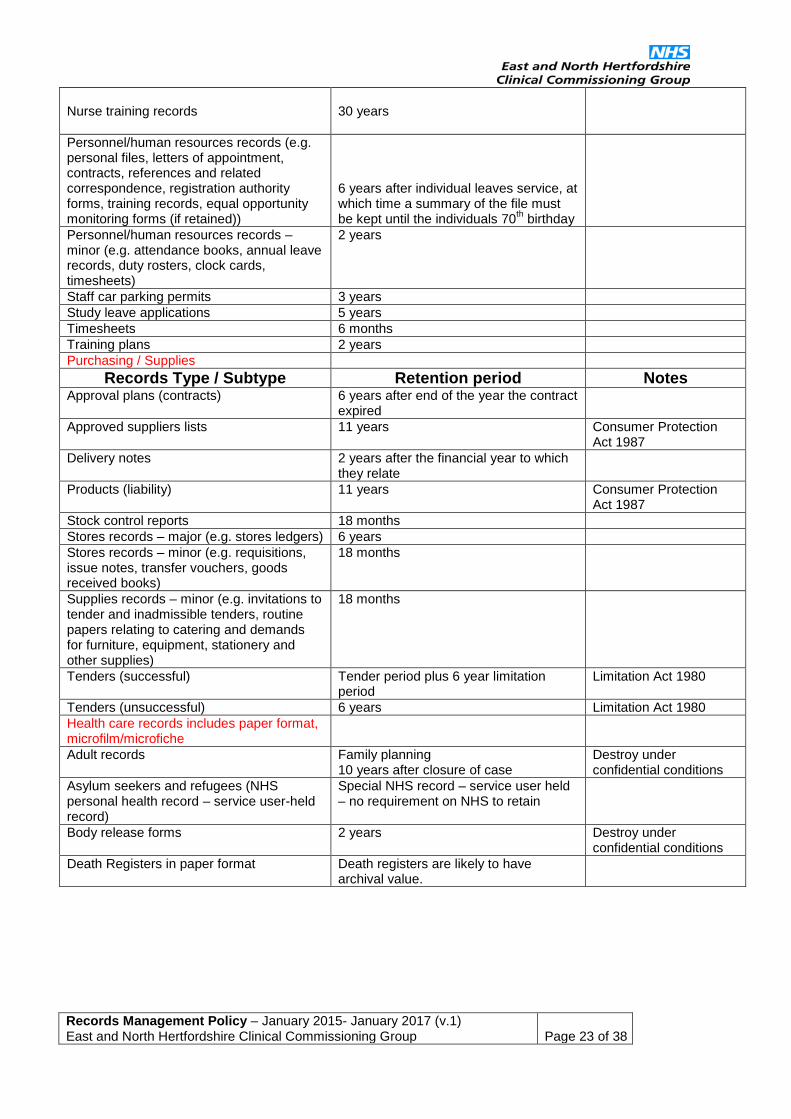
Nurse training records
30 years
Personnel/human resources records (e.g. personal files, letters of appointment, contracts, references and related correspondence, registration authority forms, training records, equal opportunity monitoring forms (if retained))
6 years after individual leaves service, at which time a summary of the file must be kept until the individuals 70
th birthday
Personnel/human resources records – minor (e.g. attendance books, annual leave records, duty rosters, clock cards, timesheets)
2 years
Staff car parking permits 3 years
Study leave applications 5 years
Timesheets 6 months
Training plans 2 years
Purchasing / Supplies
Records Type / Subtype Retention period Notes Approval plans (contracts) 6 years after end of the year the contract
expired
Approved suppliers lists 11 years Consumer Protection Act 1987
Delivery notes 2 years after the financial year to which they relate
Products (liability) 11 years Consumer Protection Act 1987
Stock control reports 18 months
Stores records – major (e.g. stores ledgers) 6 years
Stores records – minor (e.g. requisitions, issue notes, transfer vouchers, goods received books)
18 months
Supplies records – minor (e.g. invitations to tender and inadmissible tenders, routine papers relating to catering and demands for furniture, equipment, stationery and other supplies)
18 months
Tenders (successful) Tender period plus 6 year limitation period
Limitation Act 1980
Tenders (unsuccessful) 6 years Limitation Act 1980
Health care records includes paper format, microfilm/microfiche
Adult records Family planning 10 years after closure of case
Destroy under confidential conditions
Asylum seekers and refugees (NHS personal health record – service user-held record)
Special NHS record – service user held – no requirement on NHS to retain
Body release forms
2 years Destroy under confidential conditions
Death Registers in paper format Death registers are likely to have archival value.
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 24 of 38
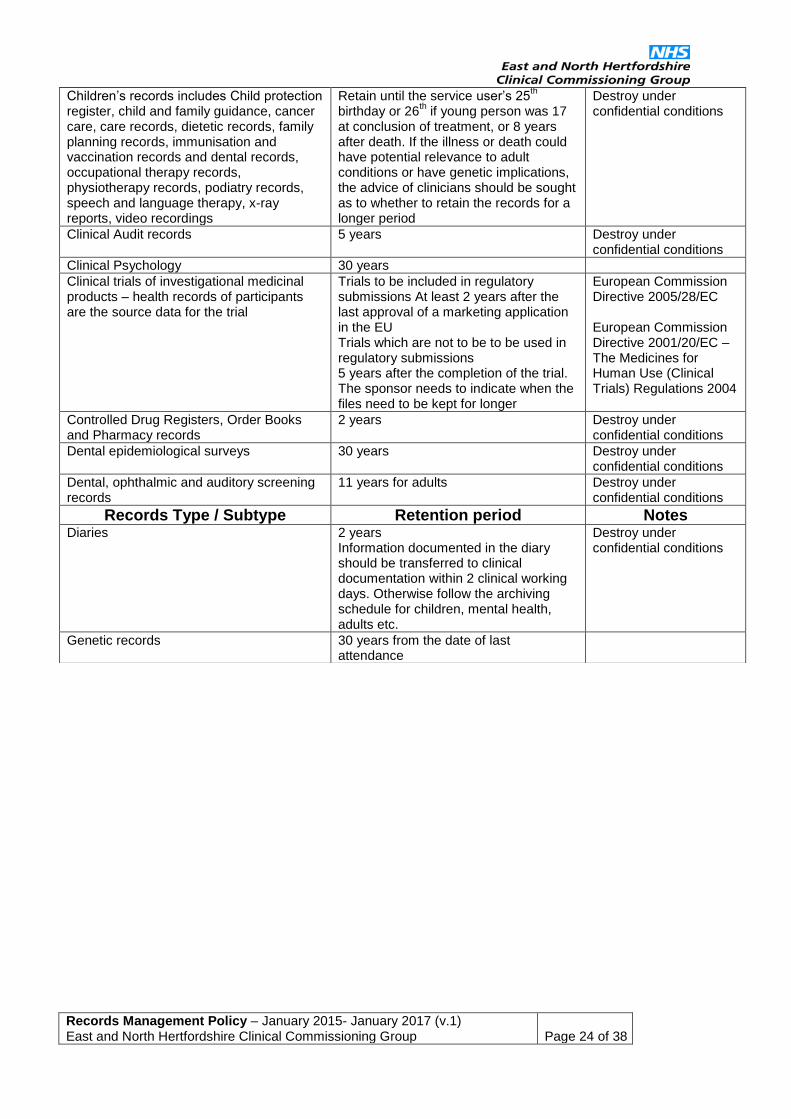
Children’s records includes Child protection register, child and family guidance, cancer care, care records, dietetic records, family planning records, immunisation and vaccination records and dental records, occupational therapy records, physiotherapy records, podiatry records, speech and language therapy, x-ray reports, video recordings
Retain until the service user’s 25th
birthday or 26th if young person was 17
at conclusion of treatment, or 8 years after death. If the illness or death could have potential relevance to adult conditions or have genetic implications, the advice of clinicians should be sought as to whether to retain the records for a longer period
Destroy under confidential conditions
Clinical Audit records 5 years Destroy under confidential conditions
Clinical Psychology 30 years
Clinical trials of investigational medicinal products – health records of participants are the source data for the trial
Trials to be included in regulatory submissions At least 2 years after the last approval of a marketing application in the EU Trials which are not to be to be used in regulatory submissions 5 years after the completion of the trial. The sponsor needs to indicate when the files need to be kept for longer
European Commission Directive 2005/28/EC European Commission Directive 2001/20/EC – The Medicines for Human Use (Clinical Trials) Regulations 2004
Controlled Drug Registers, Order Books and Pharmacy records
2 years Destroy under confidential conditions
Dental epidemiological surveys 30 years Destroy under confidential conditions
Dental, ophthalmic and auditory screening records
11 years for adults Destroy under confidential conditions
Records Type / Subtype Retention period Notes Diaries 2 years
Information documented in the diary should be transferred to clinical documentation within 2 clinical working days. Otherwise follow the archiving schedule for children, mental health, adults etc.
Destroy under confidential conditions
Genetic records 30 years from the date of last attendance
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 25 of 38
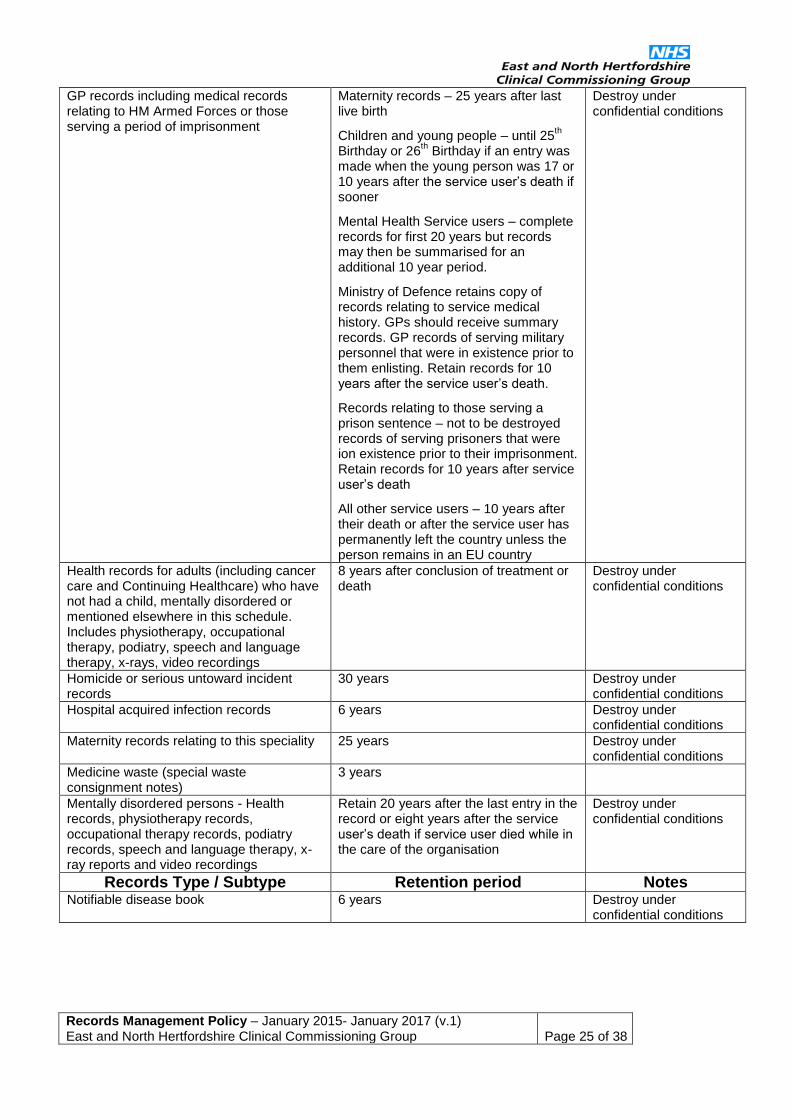
GP records including medical records relating to HM Armed Forces or those serving a period of imprisonment
Maternity records – 25 years after last live birth
Children and young people – until 25th
Birthday or 26th Birthday if an entry was
made when the young person was 17 or 10 years after the service user’s death if sooner
Mental Health Service users – complete records for first 20 years but records may then be summarised for an additional 10 year period.
Ministry of Defence retains copy of records relating to service medical history. GPs should receive summary records. GP records of serving military personnel that were in existence prior to them enlisting. Retain records for 10 years after the service user’s death.
Records relating to those serving a prison sentence – not to be destroyed records of serving prisoners that were ion existence prior to their imprisonment. Retain records for 10 years after service user’s death
All other service users – 10 years after their death or after the service user has permanently left the country unless the person remains in an EU country
Destroy under confidential conditions
Health records for adults (including cancer care and Continuing Healthcare) who have not had a child, mentally disordered or mentioned elsewhere in this schedule. Includes physiotherapy, occupational therapy, podiatry, speech and language therapy, x-rays, video recordings
8 years after conclusion of treatment or death
Destroy under confidential conditions
Homicide or serious untoward incident records
30 years Destroy under confidential conditions
Hospital acquired infection records 6 years Destroy under confidential conditions
Maternity records relating to this speciality 25 years Destroy under confidential conditions
Medicine waste (special waste consignment notes)
3 years
Mentally disordered persons - Health records, physiotherapy records, occupational therapy records, podiatry records, speech and language therapy, x-ray reports and video recordings
Retain 20 years after the last entry in the record or eight years after the service user’s death if service user died while in the care of the organisation
Destroy under confidential conditions
Records Type / Subtype Retention period Notes Notifiable disease book 6 years Destroy under
confidential conditions
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 26 of 38
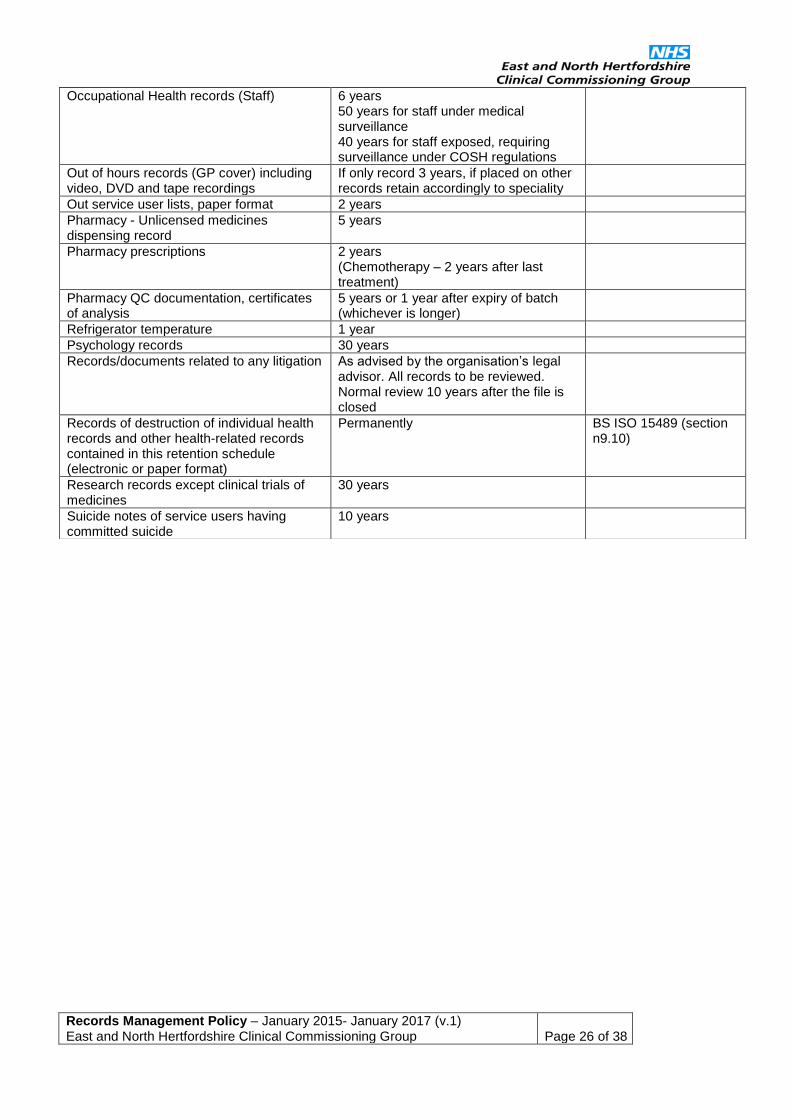
Occupational Health records (Staff) 6 years 50 years for staff under medical surveillance 40 years for staff exposed, requiring surveillance under COSH regulations
Out of hours records (GP cover) including video, DVD and tape recordings
If only record 3 years, if placed on other records retain accordingly to speciality
Out service user lists, paper format 2 years
Pharmacy - Unlicensed medicines dispensing record
5 years
Pharmacy prescriptions 2 years (Chemotherapy – 2 years after last treatment)
Pharmacy QC documentation, certificates of analysis
5 years or 1 year after expiry of batch (whichever is longer)
Refrigerator temperature 1 year
Psychology records 30 years
Records/documents related to any litigation As advised by the organisation’s legal advisor. All records to be reviewed. Normal review 10 years after the file is closed
Records of destruction of individual health records and other health-related records contained in this retention schedule (electronic or paper format)
Permanently BS ISO 15489 (section n9.10)
Research records except clinical trials of medicines
30 years
Suicide notes of service users having committed suicide
10 years
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 27 of 38
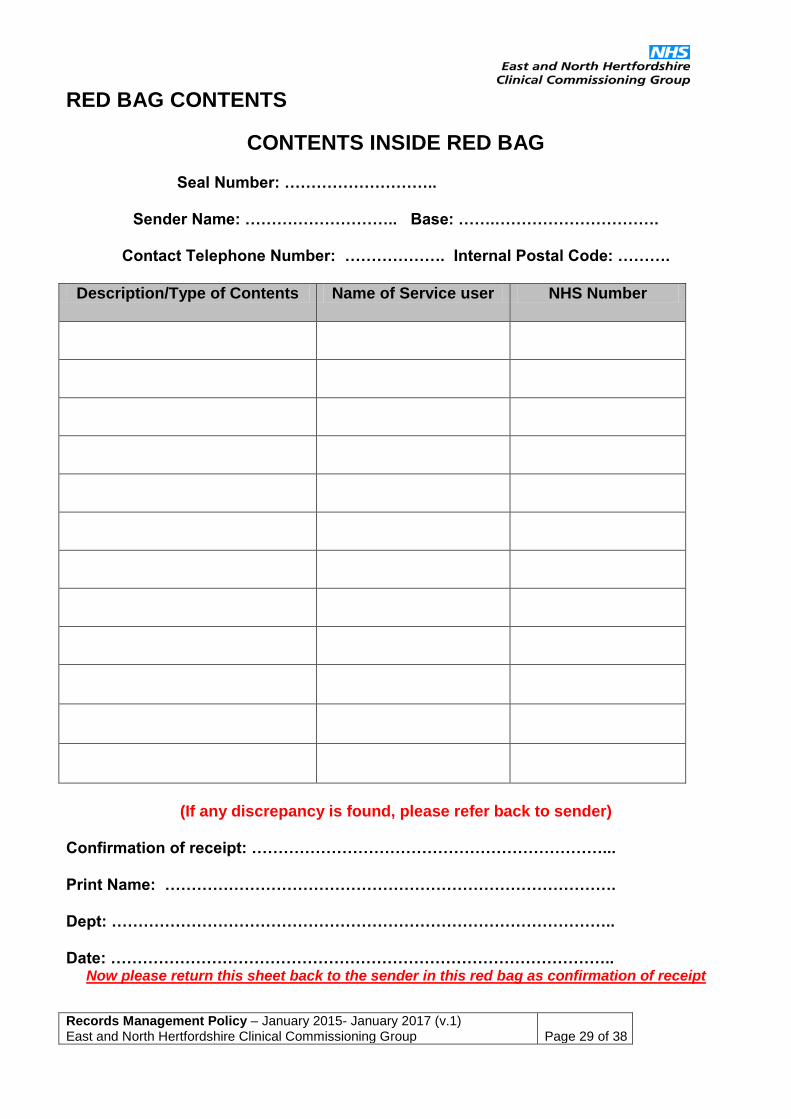
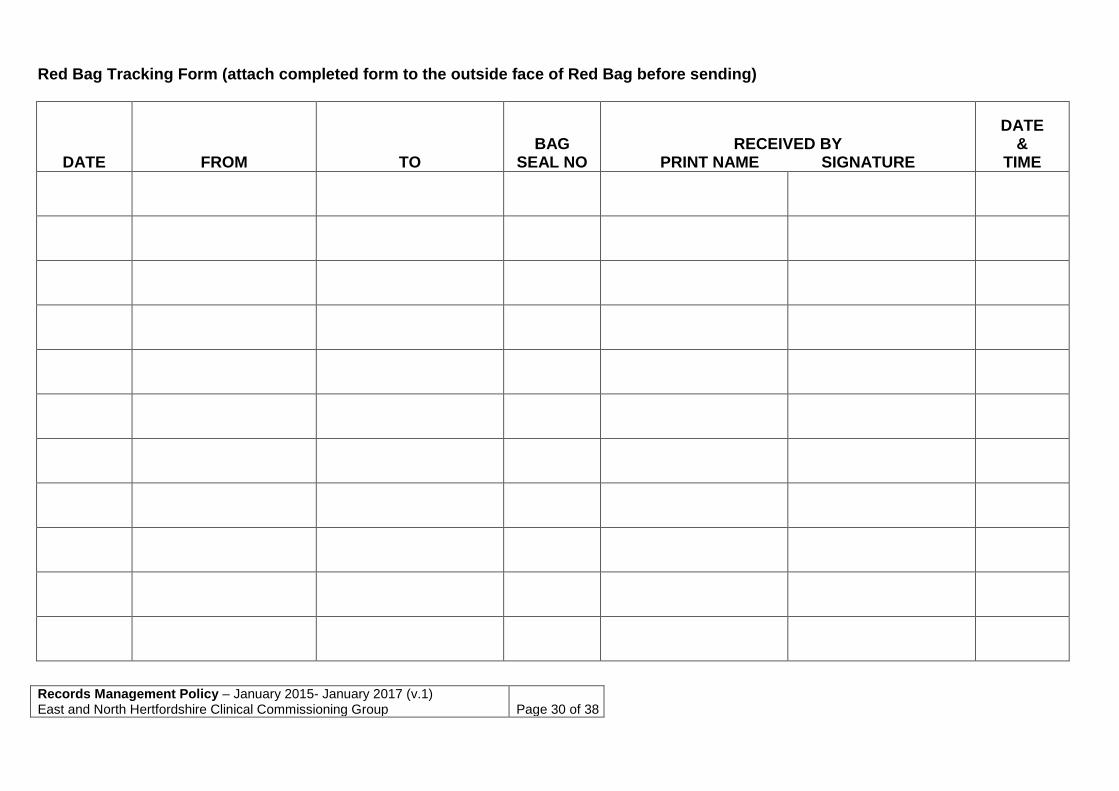
Appendix 4 - Internal Confidential Courier Service (“Red bag” scheme) Purpose: To ensure confidential mail is safely and securely transported between sites. Contents of Bags The contents sheet must be completed for every bag. When sending service user notes and important documents the correct information should be recorded on the contents form for each individual service user. When sending service user slips, i.e. development checks, A & E slips etc. these can be bundled up and put into one envelope which is recorded on the contents sheets just listing the envelope. The completed red bag contents sheet is to be placed inside the red bag with the confidential material. Make a copy of the contents sheet and retain until receiving the original back from the receiving unit. The bag is then sealed using a security tag. Bags will not be collected by the courier unless sealed. The completed Tracker Form is then secured to the outside of the bag. Numbered White Security Seals: Come in Box of 500s £8.32 Order via: NHS Supplies Code: WYY207 (costs as at 2010 prices) Tracker Forms Complete the tracker form recording all the details as directed on the form. If the transfer route includes a post room please tick the relevant box, if known. Operating Requirements 1. Trust courier drivers collect or deliver children services secured mail from designated area
as per run sheet. Courier drivers collecting mail must sign for it upon collection only if it is in a secured mailing pouch. Courier drivers delivering children services couriered mail must ensure it is signed over to a member of staff at the delivery destination.
2. Driver to sign and date the tracker form on every run. 3. If returning to Lister/QEII for onward travel secured mail pouch (red bag) should be
delivered to the post room. Member of post room staff must sign for the secured pouch (red bag) from the Driver
4. If there is no mail personnel in the post room on return from the final run the secured mail pouch (red bag) should be placed in the designated pigeon hole.
5. Drivers must ensure that they sign for any secured mailing pouches that they receive from the post room.
6. Driver will then deliver secured mailing pouch (red bag) to designated delivery point. Upon arrival at destination a member of staff must sign for the secured mailing pouch (red bag) before delivery can be finalised.
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 28 of 38
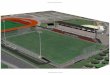
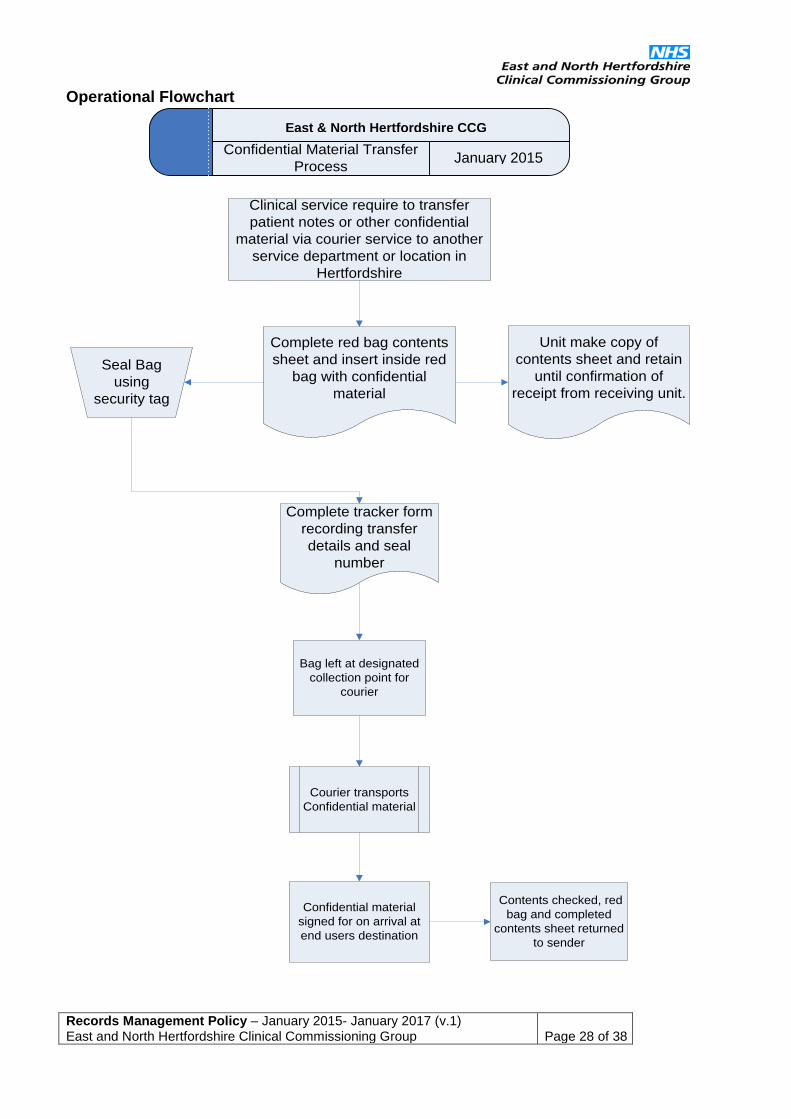
Operational Flowchart
Confidential Material Transfer
Process4 Jan 2011
Hertfordshire PCTs
Clinical service require to transfer
patient notes or other confidential
material via courier service to another
service department or location in
Hertfordshire
Complete red bag contents
sheet and insert inside red
bag with confidential
material
Seal Bag
using
security tag
Complete tracker form
recording transfer
details and seal
number
Bag left at designated
collection point for
courier
Courier transports
Confidential material
Confidential material
signed for on arrival at
end users destination
Unit make copy of
contents sheet and retain
until confirmation of
receipt from receiving unit.
Contents checked, red
bag and completed
contents sheet returned
to sender
East & North Hertfordshire CCG
January 2015
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 29 of 38
RED BAG CONTENTS
CONTENTS INSIDE RED BAG
Seal Number: ………………………..
Sender Name: ……………………….. Base: …….………………………….
Contact Telephone Number: ………………. Internal Postal Code: ……….
Description/Type of Contents Name of Service user NHS Number
(If any discrepancy is found, please refer back to sender)
Confirmation of receipt: …………………………………………………………... Print Name: …………………………………………………………………………. Dept: ………………………………………………………………………………….. Date: …………………………………………………………………………………..
Now please return this sheet back to the sender in this red bag as confirmation of receipt
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 30 of 38
Red Bag Tracking Form (attach completed form to the outside face of Red Bag before sending)
DATE FROM TO BAG
SEAL NO RECEIVED BY
PRINT NAME SIGNATURE
DATE &
TIME
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 31 of 38
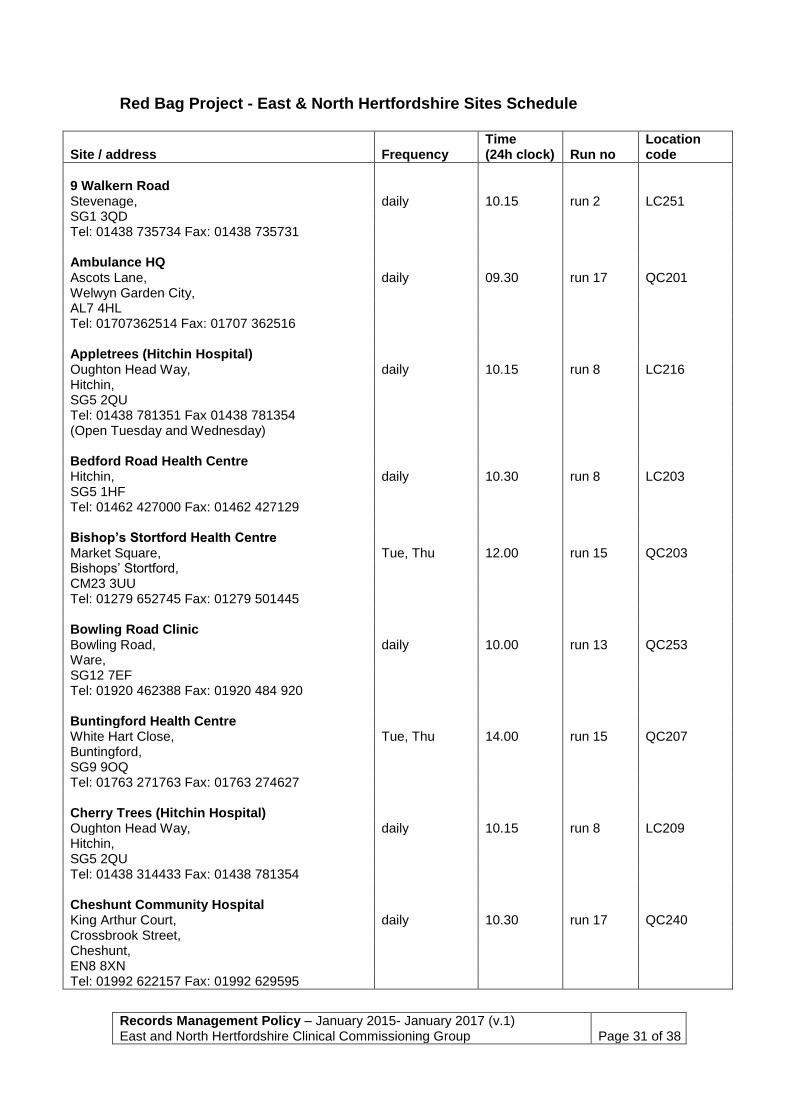
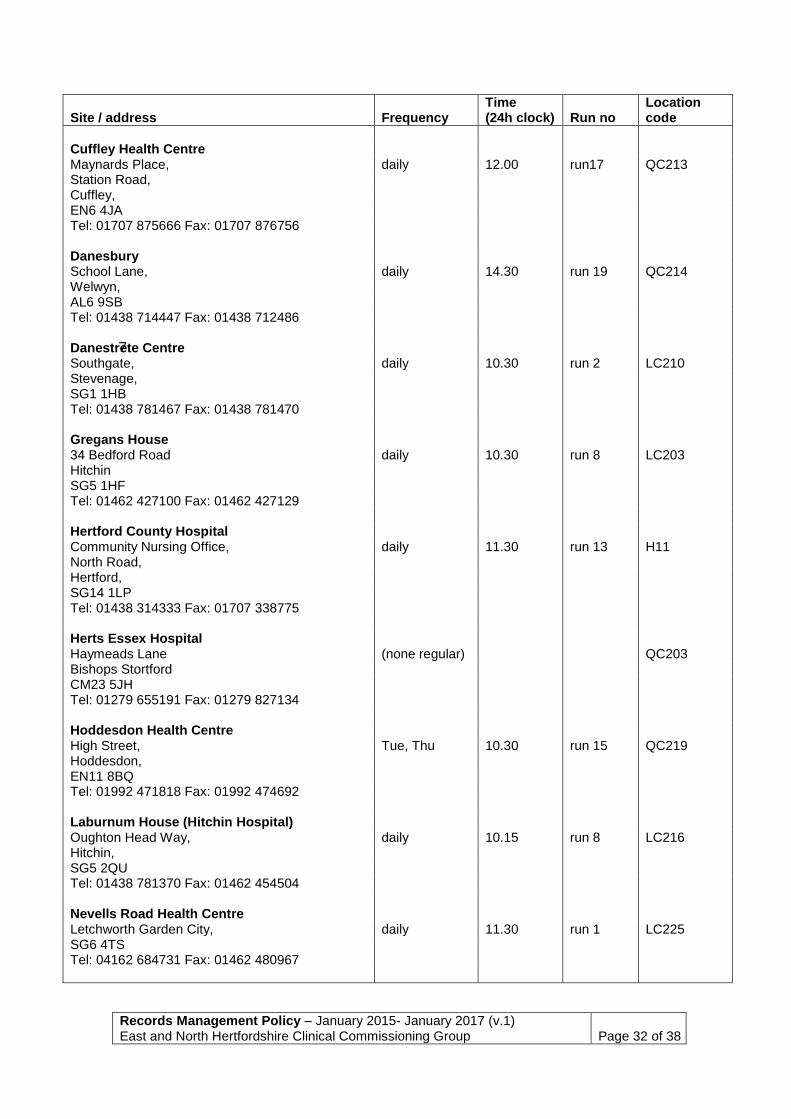
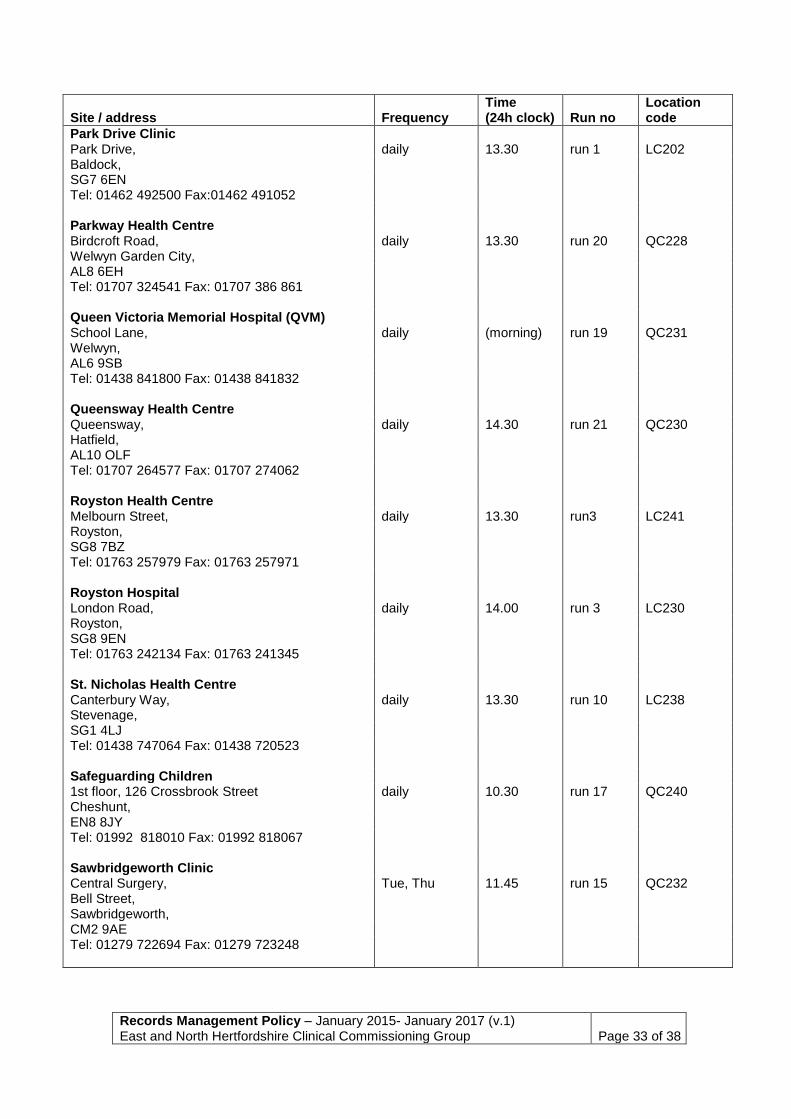
Red Bag Project - East & North Hertfordshire Sites Schedule
Site / address Frequency Time (24h clock) Run no
Location code
9 Walkern Road Stevenage, daily 10.15 run 2 LC251 SG1 3QD Tel: 01438 735734 Fax: 01438 735731 Ambulance HQ Ascots Lane, daily 09.30 run 17 QC201 Welwyn Garden City, AL7 4HL Tel: 01707362514 Fax: 01707 362516 Appletrees (Hitchin Hospital) Oughton Head Way, daily 10.15 run 8 LC216 Hitchin, SG5 2QU Tel: 01438 781351 Fax 01438 781354 (Open Tuesday and Wednesday) Bedford Road Health Centre Hitchin, daily 10.30 run 8 LC203 SG5 1HF Tel: 01462 427000 Fax: 01462 427129 Bishop’s Stortford Health Centre Market Square, Tue, Thu 12.00 run 15 QC203 Bishops’ Stortford, CM23 3UU Tel: 01279 652745 Fax: 01279 501445 Bowling Road Clinic Bowling Road, daily 10.00 run 13 QC253 Ware, SG12 7EF Tel: 01920 462388 Fax: 01920 484 920 Buntingford Health Centre White Hart Close, Tue, Thu 14.00 run 15 QC207 Buntingford, SG9 9OQ Tel: 01763 271763 Fax: 01763 274627 Cherry Trees (Hitchin Hospital) Oughton Head Way, daily 10.15 run 8 LC209 Hitchin, SG5 2QU Tel: 01438 314433 Fax: 01438 781354 Cheshunt Community Hospital King Arthur Court, daily 10.30 run 17 QC240 Crossbrook Street, Cheshunt, EN8 8XN Tel: 01992 622157 Fax: 01992 629595
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 32 of 38
Site / address Frequency Time (24h clock) Run no
Location code
Cuffley Health Centre Maynards Place, daily 12.00 run17 QC213 Station Road, Cuffley, EN6 4JA Tel: 01707 875666 Fax: 01707 876756 Danesbury School Lane, daily 14.30 run 19 QC214 Welwyn, AL6 9SB Tel: 01438 714447 Fax: 01438 712486 Danestrete Centre Southgate, daily 10.30 run 2 LC210 Stevenage, SG1 1HB Tel: 01438 781467 Fax: 01438 781470 Gregans House 34 Bedford Road daily 10.30 run 8 LC203 Hitchin SG5 1HF Tel: 01462 427100 Fax: 01462 427129 Hertford County Hospital Community Nursing Office, daily 11.30 run 13 H11 North Road, Hertford, SG14 1LP Tel: 01438 314333 Fax: 01707 338775 Herts Essex Hospital Haymeads Lane (none regular) QC203 Bishops Stortford CM23 5JH Tel: 01279 655191 Fax: 01279 827134 Hoddesdon Health Centre High Street, Tue, Thu 10.30 run 15 QC219 Hoddesdon, EN11 8BQ Tel: 01992 471818 Fax: 01992 474692 Laburnum House (Hitchin Hospital) Oughton Head Way, daily 10.15 run 8 LC216 Hitchin, SG5 2QU Tel: 01438 781370 Fax: 01462 454504 Nevells Road Health Centre Letchworth Garden City, daily 11.30 run 1 LC225 SG6 4TS Tel: 04162 684731 Fax: 01462 480967
7
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 33 of 38
Site / address Frequency Time (24h clock) Run no
Location code
Park Drive Clinic Park Drive, daily 13.30 run 1 LC202 Baldock, SG7 6EN Tel: 01462 492500 Fax:01462 491052 Parkway Health Centre Birdcroft Road, daily 13.30 run 20 QC228 Welwyn Garden City, AL8 6EH Tel: 01707 324541 Fax: 01707 386 861 Queen Victoria Memorial Hospital (QVM) School Lane, daily (morning) run 19 QC231 Welwyn, AL6 9SB Tel: 01438 841800 Fax: 01438 841832 Queensway Health Centre Queensway, daily 14.30 run 21 QC230 Hatfield, AL10 OLF Tel: 01707 264577 Fax: 01707 274062 Royston Health Centre Melbourn Street, daily 13.30 run3 LC241 Royston, SG8 7BZ Tel: 01763 257979 Fax: 01763 257971 Royston Hospital London Road, daily 14.00 run 3 LC230 Royston, SG8 9EN Tel: 01763 242134 Fax: 01763 241345 St. Nicholas Health Centre Canterbury Way, daily 13.30 run 10 LC238 Stevenage, SG1 4LJ Tel: 01438 747064 Fax: 01438 720523 Safeguarding Children 1st floor, 126 Crossbrook Street daily 10.30 run 17 QC240 Cheshunt, EN8 8JY Tel: 01992 818010 Fax: 01992 818067 Sawbridgeworth Clinic Central Surgery, Tue, Thu 11.45 run 15 QC232 Bell Street, Sawbridgeworth, CM2 9AE Tel: 01279 722694 Fax: 01279 723248

Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 34 of 38
Site / address Frequency Time (24h clock) Run no
Location code
Southgate Health Clinic Stevenage, daily 10.30 run 2 LC233 SG1 1HB Tel: 01438 781404 Fax: 01438 781409 Stanmore Road Health Centre Stevenage, daily 10.00 run 2 LC239 SG1 3QA Tel: 01438 727161 Fax: 01438 314248 Standon Health Centre Station Road, Tue, Thu 13.00 run 15 QC235 Puckeridge, SG11 1TF Tel: 01920 822018 Fax: 01920 823985 Valley View Surgery Goffs Lane, daily 10.50 run 17 QC249 Goffs Oak, EN8 5ET Tel: 01707 875223 Fax: 01707 875033 Waltham Cross Clinic Stanhope Road, Tue, Thu 10.40 run 15 QC251 Waltham Cross, EN8 7DJ Tel: 01992 621613 Fax: 01992 780168 Warden Lodge Glen Luce, daily 10.15 run 17 QC252 Turners Hill, Cheshunt, EN8 7DJ Tel: 01992 622324 Fax: 01992 636900 Ware Clinic 15 Bowling Rd daily 10.00 run 13 QC253 Ware Herts SG12 7EF Tel: 01920 46238 Fax: 01920 484920 Wheelchair Services Unit 17 & 19 Mon, Wed, Fri 13.30 run 20 QC255 South Mundells Welwyn Garden City AL7 1EP Tel: 01707 382000 Fax: 01707 382092 Wormley Health Centre Fairfield Drive, (none regular) Wormley, EN10 6DX Tel: 01992 474674 Fax: 01992 474694

Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 35 of 38
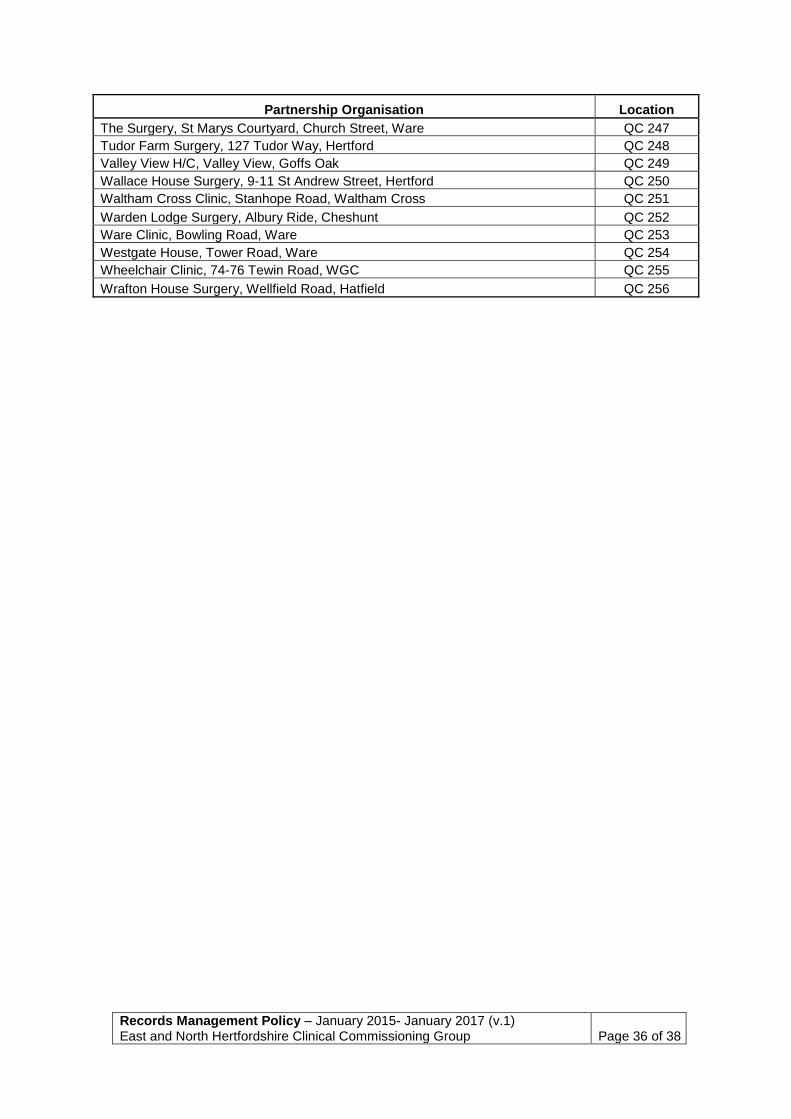
Partnership Organisations – East & North Hertfordshire Location Codes
Partnership Organisation Location
305 Ware Road, Ware QC 200
Ambulance HQ, Ascots Lane, Welwyn Garden City QC 201
Amwell View School, Stanstead Abbotts, Ware QC 202
Bishops Stortfold H/C, Market Square, Bishops Stortfold QC 203
Bridge Cottage Surgery, 51 Bridge Road East, WGC QC 204
Brocket Road Surgery, Hoddesdon QC 205
Bull Plain Clinic, Bull Plain, Hertford QC 206
Buntingford H/C, White Hart Close, Buntingford QC 207
Burvill House Surgery, 52/54 Dellfield Road, Hatfield QC 208
Castle Gate Surgery, Castle Street, Hertford QC 209
Charter House, Parkway, WGC QC 210
Church Street Partnership, 30A Church Street, Bishops Stortford QC 211
County Hall, Hertford QC 212
Cuffley Health Centre, Maynards Place, Cuffley QC 213
Danesbury, School Lane, Welwyn QC 214
Dolphin House Surgery, 6-7 East Street, Ware QC 215
Hanscombe House Surgery, 52A St Andrew Street, Hertford QC 216
Hatfield University, College lane, Hatfield QC 217
High View, 20 Southgate Road, Potters Bar QC 218
Hoddesdon H/C, High Street, Hoddesdon QC 219
Jim McDonald Day Centre, High View, Hatfield QC 220
Lakeside School, Lemsford Lane, WGC QC 221
Lister House Surgery, The Common, Hatfield QC 222
Luton & Dunstable Hospital/Clinic QC 223
Moorswalk Surgery, Panshanger, WGC QC 224
Much Hadham H/C, Ash Meadow, Much Hadham QC 225
North Place, Hatfield QC 226
Northdown Road, Hatfield QC 227
Parkway Health Centre, WGC QC 228
Potterells Medical Centre, Station Road, North Mymms QC 229
Queensway Clinic, Queensway, Hatfield QC 230
QVM, School Lane, Welwyn QC 231
Sawbridgeworth Clinic, 2B The Square, Sawbridgeworth QC 232
Seward Lodge, Stanstead Road, Hertford QC 233
St Albans Hospital/Clinic QC 234
Standon H/C, Station Road, Puckeridge QC 235
Stockwell Lodge Medical Centre, Rosedale Way, Cheshunt QC 236
The Bridge, CMHT, 26 Bridge Road East, WGC QC 257
The Maltings Surgery, 15 Amwell End, Ware QC 237
The Surgery, 11 Guessons Road, WGC QC 238
The Surgery, 110 Peartree Lane, WGC QC 239
The Surgery, 126 Crossbrook Street, Cheshunt QC 240
The Surgery, 185 Knightsfield, WGC QC 241
The Surgery, 20 Parkway, WGC QC 242
The Surgery, 4 Hall Grove, WGC QC 243
The Surgery, 59 Ware Road, Hoddesdon QC 244
The Surgery, 77 Ware Road, Hertford QC 245
The Surgery, 8-14 Limes Court, Conduit Lane, Hoddesdon QC 246
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 36 of 38
Partnership Organisation Location
The Surgery, St Marys Courtyard, Church Street, Ware QC 247
Tudor Farm Surgery, 127 Tudor Way, Hertford QC 248
Valley View H/C, Valley View, Goffs Oak QC 249
Wallace House Surgery, 9-11 St Andrew Street, Hertford QC 250
Waltham Cross Clinic, Stanhope Road, Waltham Cross QC 251
Warden Lodge Surgery, Albury Ride, Cheshunt QC 252
Ware Clinic, Bowling Road, Ware QC 253
Westgate House, Tower Road, Ware QC 254
Wheelchair Clinic, 74-76 Tewin Road, WGC QC 255
Wrafton House Surgery, Wellfield Road, Hatfield QC 256
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 37 of 38
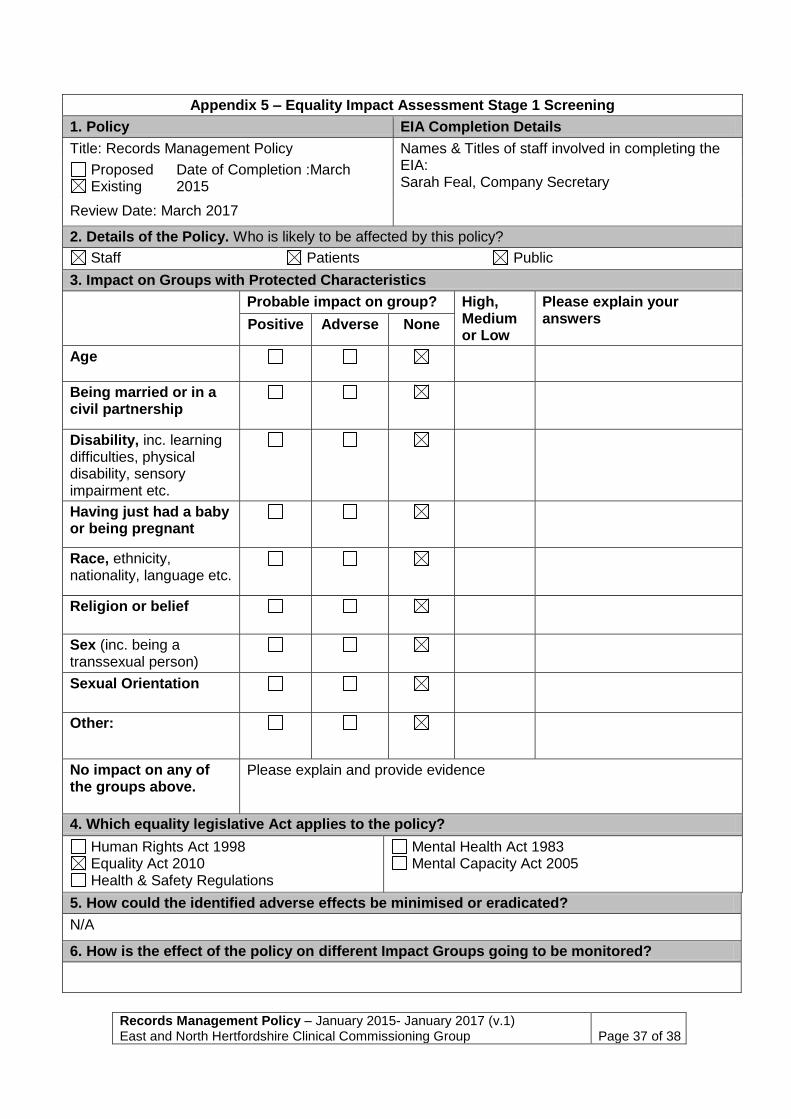
Appendix 5 – Equality Impact Assessment Stage 1 Screening
1. Policy EIA Completion Details
Title: Records Management Policy Names & Titles of staff involved in completing the EIA: Sarah Feal, Company Secretary
Proposed Existing
Date of Completion :March 2015
Review Date: March 2017
2. Details of the Policy. Who is likely to be affected by this policy?
Staff Patients Public
3. Impact on Groups with Protected Characteristics
Probable impact on group? High, Medium or Low
Please explain your answers Positive Adverse None
Age
Being married or in a civil partnership
Disability, inc. learning difficulties, physical disability, sensory impairment etc.
Having just had a baby or being pregnant
Race, ethnicity, nationality, language etc.
Religion or belief
Sex (inc. being a transsexual person)
Sexual Orientation
Other:
No impact on any of the groups above.
Please explain and provide evidence
4. Which equality legislative Act applies to the policy?
Human Rights Act 1998 Equality Act 2010 Health & Safety Regulations
Mental Health Act 1983 Mental Capacity Act 2005
5. How could the identified adverse effects be minimised or eradicated?
N/A
6. How is the effect of the policy on different Impact Groups going to be monitored?
Records Management Policy – January 2015- January 2017 (v.1) East and North Hertfordshire Clinical Commissioning Group
Page 38 of 38
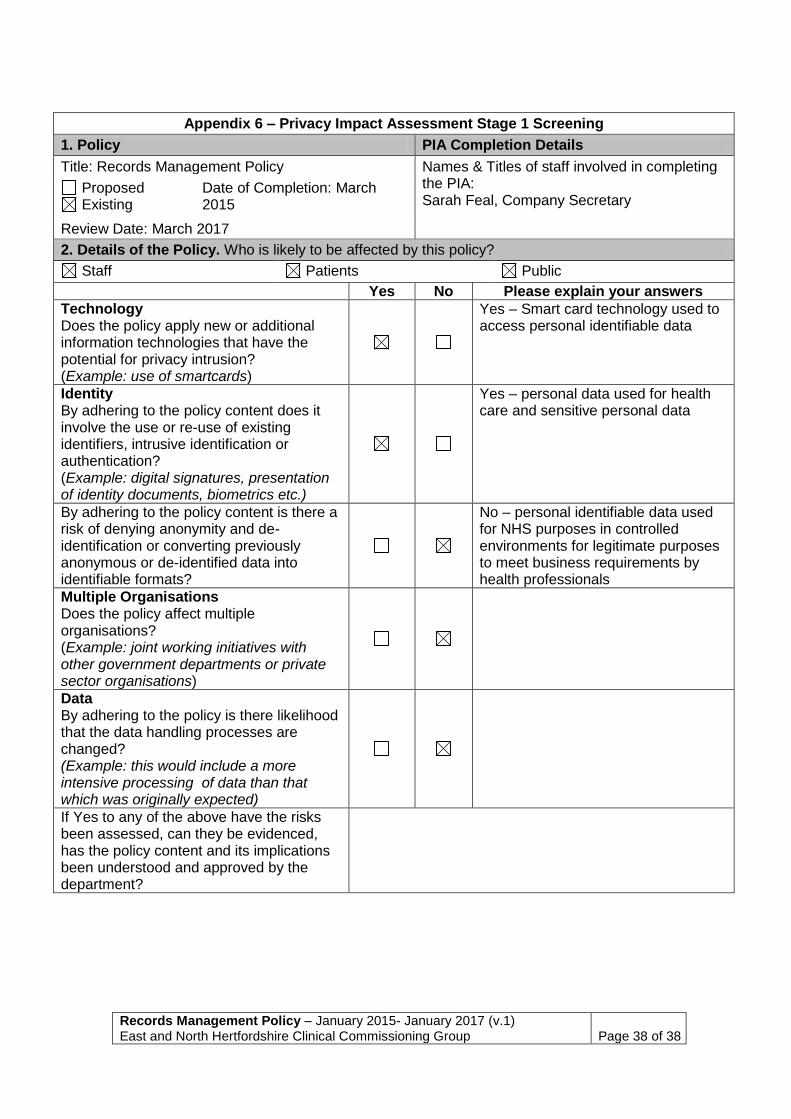
Appendix 6 – Privacy Impact Assessment Stage 1 Screening
1. Policy PIA Completion Details
Title: Records Management Policy Names & Titles of staff involved in completing the PIA: Sarah Feal, Company Secretary
Proposed Existing
Date of Completion: March 2015
Review Date: March 2017
2. Details of the Policy. Who is likely to be affected by this policy?
Staff Patients Public
Yes No Please explain your answers
Technology Does the policy apply new or additional information technologies that have the potential for privacy intrusion? (Example: use of smartcards)
Yes – Smart card technology used to access personal identifiable data
Identity By adhering to the policy content does it involve the use or re-use of existing identifiers, intrusive identification or authentication? (Example: digital signatures, presentation of identity documents, biometrics etc.)
Yes – personal data used for health care and sensitive personal data
By adhering to the policy content is there a risk of denying anonymity and de-identification or converting previously anonymous or de-identified data into identifiable formats?
No – personal identifiable data used for NHS purposes in controlled environments for legitimate purposes to meet business requirements by health professionals
Multiple Organisations Does the policy affect multiple organisations? (Example: joint working initiatives with other government departments or private sector organisations)
Data By adhering to the policy is there likelihood that the data handling processes are changed? (Example: this would include a more intensive processing of data than that which was originally expected)
If Yes to any of the above have the risks been assessed, can they be evidenced, has the policy content and its implications been understood and approved by the department?