Embed Size (px)
Citation preview

Seminars in Colon and Rectal Surgery 25 (2014) 13–18
Contents lists available at ScienceDirect
Seminars in Colon and Rectal Surgery
1043-14http://d
n CorrE-m
journal homepage: www.elsevier.com/locate/yscrs
Rectal cancer genomics
Aaron D. Falchook, MD, Joel E. Tepper, MDn
Department of Radiation Oncology, UNC/Lineberger Comprehensive Cancer Center, University of North Carolina School of Medicine, Chapel Hill, NC 27599-7512
a b s t r a c t
Cellular signaling abnormalities play an important rosignaling changes are frequently driven by genomic caltered cell signaling pathways in rectal cancer: WNT, Rboth physiologic (non-altered) function and common mare described. As rectal cancer is driven by genomic chpathway signaling mutations is included. Lastly, the useresponse to preoperative radiotherapy is described.
89/$ - see front matter & 2014 Elsevier Inc. Ax.doi.org/10.1053/j.scrs.2013.09.010
esponding author.ail address: [email protected] (J.E. Tepper)
le in the oncogenesis of rectal cancer. Thesehanges. This review describes five commonlyAS, TGF-β, p53, and PI3K. For these pathways,utations that contribute to abnormal signalinganges, a discussion of the prognostic value ofof genomic changes as predictive markers for
& 2014 Elsevier Inc. All rights reserved.
1. Introduction
The initiation and progression of colorectal carcinoma (CRC) isdriven by abnormalities that develop in cellular signaling path-ways. Many details about the genomic basis of CRC have beenclarified, although our understanding of this complex disease iscertainly incomplete.
There are a wide variety of genomic alterations that occur inCRC. Individual gene mutations may be activating or inactivating,and even within a single gene, mutations at various loci mayproduce different biological effects. In addition to gene mutations,alterations in gene expression levels, chromosomal aberrations,and epigenetic changes such as hyper- or hypo-methylationcontribute to the process of oncogenic transformation. Due to thiscomplexity, the study of a single gene or even a single cellsignaling pathway will yield a limited amount of information; atrue genomic understanding of any given cancer requires acomprehensive analysis.
The literature on the genomics of CRC is massive, so we haveintentionally been selective in reviewing topics that we think areof the greatest interest to this readership. In this paper we discussdetails of genomic alterations in critical cell signaling pathways asthey relate to CRC and we focus less on the downstream effects ofthese alterations. For example, mutations in the WNT–APC path-way lead to increased expression of C-MYC, which contributes toincreased cellular proliferation.1 Thus, increased levels of C-MYC inCRC represent a result of pathway dysregulation rather than acausative mechanism of oncogenesis. As our aim is to discuss thegenomic alterations that drive the development of CRC rather thandownstream effects of these pathways, the WNT pathway is
ll rights reserved.
.
discussed in greater detail below, while C-MYC is not furtheraddressed.
Molecules involved in angiogenesis such as vascular endothelialgrowth factor and hypoxia-inducible factor also have an importantrole in CRC.2 Angiogenesis pathway signaling has importantimplications for the development and use of targeted agents inthe treatment of CRC. However, the activation of angiogenesis ismost likely the result of altered cellular signaling rather than acause, and therefore we will limit our discussion of this topicas well.
An extensive genome-scale analysis of colorectal tumors per-formed by The Cancer Genome Atlas (TCGA) project recentlyreported a detailed account of genomic changes in CRC, which isthe most comprehensive analysis yet performed on colorectalcancers.3 To accomplish this genomic analysis, TCGA investigatedexome sequences, methylation patterns, chromosomal changes,and overall pathway alterations.
On a high-level evaluation, 16% of CRC tumors had very highmutation rates and were designated as hypermutated, while theremaining 84% of tumors were non-hypermutated. The vast major-ity of hypermutated tumors were located in the colon (predom-inantly in the right colon) and were rarely seen in the rectum. Thesetumors frequently had microsatellite instability and silencing ormutation of mismatch repair genes. Among the non-hypermutatedtumors, there were no significant differences in patterns of muta-tions between tumors located in the rectum and in the colon.Despite the fact that anatomical differences between the colon andrectum have led to different treatment approaches for rectal cancerand colon cancer, rectal tumors do not appear to have a distinctgenomic profile when compared to non-hypermutated tumorsarising in the rest of the large bowel.
The role of various genomic alterations seen in CRC has beendescribed in detail; WNT signaling abnormality due to mutantAPC and mismatch repair abnormalities have been extensively

A.D. Falchook, J.E. Tepper / Seminars in Colon and Rectal Surgery 25 (2014) 13–1814
reported, as these changes are associated with familial CRCsyndromes.4 Furthermore, alterations in P53, PI3K, and RAS signal-ing pathways have been shown to play an important role in CRC.The TCGA analysis further clarified details regarding mutations inthese genes and pathways and also illustrated alterations in otherpathways such as TGF-β. Details pertaining to the five mostcommon signaling pathway alterations found in CRC are illustratedin a concise yet thorough manner in Figure 4 of the articlepublished by TCGA. The purpose of this article is to review thegenomic changes in CRC with a specific focus on pathways thatcontribute to oncogenesis as well as to discuss how alterations inthese pathways relate to radiotherapy. To accomplish this, five ofthe most commonly altered signaling pathways in rectal cancerwill be discussed in more detail: WNT, RAS, TGF-β, p53, and PI3K.
1.1. WNT
The WNT pathway plays an important part in the growth anddifferentiation of mucosal epithelial cells of the colon and rectum.This pathway is particularly important in CRC, as the vast majorityof CRC have genomic aberrations that cause altered WNT signaling.3
A critical signaling molecule in the WNT pathway is β-catenin.This protein is an intracellular molecule that can enter the nucleusand bind to transcription factors in the TCF/LEF family that targetsgenes that lead to cellular proliferation. Under physiologic con-ditions β-catenin activity is regulated by GSK-3β, Axin, and APC.These proteins combine and phosphorylate β-catenin, which leadsto the degradation of β-catenin in the proteasome. WNT is asignaling molecule that binds to plasma membrane-bound recep-tors such as Frizzled. Signaling from these receptors suppressesGSK-3β function. This leads to an increase in β-catenin levels, andthus, an increase in cellular proliferation (Fig. 1). As normal coloniccells grow and migrate away from the base of colonic crypts, thereis a reduction in WNT signaling and a reduction in cell growth witha concomitant increase in cell differentiation.5 The importance ofthe WNT pathway is seen most dramatically in patients withfamilial adenomatous polyposis, in which a mutated APC gene isunable to facilitate degradation of β-catenin, leading to uncon-trolled cell growth and widespread polyp formation throughoutthe colon.
The most common alteration in the WNT pathway found in CRCpatients is a mutation of APC. Approximately 93% of CRC tumors
Fig. 1. WNT signaling causes increased β-catenin-mediated signaling via down-regulation of GSK-3β. When bound by APC, GSK-3β and axin phosphorylateβ-catenin. This leads to degradation of β-catenin in the proteasome. Any loss-of-function mutation or signal-mediated down-regulation of APC, GSK-3β, or axin willlead to a decrease in phosphorylation and degradation of β-catenin. The resultanthigher cytoplasmic concentration of β-catenin facilitates entry into the nucleus,where it can bind to transcription factors such as TCF which activate genes that leadto increased cellular proliferation.
have altered WNT signaling, with 76% having mutations that leadto a loss of function in APC.3 Because the WNT pathway is almostalways altered in CRC, testing for mutations in this pathway islikely not useful as a predictive or prognostic marker. However, thehigh prevalence of mutations and changes in gene expression atvarious steps in the WNT pathway does suggest that the WNTpathway is a rich source of potential therapeutic targets in CRC.
Efforts to target individual components of the WNT pathwayhave met with limited success. In vitro and in vivo studies of CRCcell lines demonstrate that small interfering RNA (siRNA) directedagainst β-catenin inhibits the growth of cancer cells.6 A variety ofsmall-molecule β-catenin inhibitors have been identified, butmore research is needed to evaluate toxicological and pharmaco-logical properties of these drugs.7 To date, none of these agentshave seen widespread clinical use. Critical cell survival pathwaysappear to often have alternative means of activation, because theyare so critical to cell survival. By targeting multiple portions ofoncogenic pathways concurrently, the efficacy of targeted therapymay be further improved by removing the alternative means ofactivation. Silencing of both β-catenin and KRAS through the use ofshRNA has been shown to cause induction of apoptosis in vitro andtumor growth suppression in vivo.8 PKF115-584 is a specificinhibitor of the β-catenin/TCF4 interaction and pyrviniumpamoate is an anti-helminthic drug that induces degradation ofβ-catenin. When combined with salirasib, a specific RAS inhibitor,this three-drug combination was shown to be effective in inducingcell growth arrest and cell death in vitro. Unfortunately, prelimi-nary in vivo results were negative due to poor drug absorption.9
Furthermore, in a retrospective analysis, the synergistic effect ofcombined WNT and RAS targeting was not seen in cells withmutations in BRAF, which is observed in approximately 10% of CRCtumors.3,9
The WNT receptor Frizzled is overexpressed in approximately17% of all CRC and is sometimes expressed at levels greater than100-times normal.3 Increased Frizzled expression activates thecanonical WNT pathway independent of the presence of an APCmutation. Blocking Frizzled activity with siRNA decreased TCFtranscriptional activity and cell viability.10 A monoclonal antibodyhas been developed that targets Frizzled and blocks the canonicalWNT signaling, resulting in tumor growth inhibition in animalmodels.11
The role of WNT signaling in sensitivity to chemoradiotherapyin rectal cancer is not clear. WNT signaling is aberrant in nearly allcases of CRC but response to neoadjuvant chemoradiotherapy inrectal cancer is variable, ranging from pathologic completeresponse (pCR) to no response. Although the mutations or changesin expression of genes involving the WNT pathway may be relatedto radioresistance, it seems virtually certain that other factorscontribute to radioresistance of CRC tumors.
No data have established a direct causative mechanism forchemoradioresistance caused by aberrant WNT signaling. How-ever, a study of the gene expression signature of 12 CRC cell linesfound that cell lines with changes in expression of genes involvedin the WNT pathway were significantly associated with increasedradioresistance in vitro.12 Furthermore, TCF4, a transcription factorthat is a target of β-catenin, has been shown to be overexpressed insome rectal cancers resistant to chemoradiotherapy. The use ofshRNA to silence TCF4 has been demonstrated to sensitize CRCcells to ionizing radiation in vitro.13 These data suggest that genesin the WNT pathway are a potential target for the development ofradiosensitizing drugs.
1.2. RTK–RAS
RAS is a membrane-bound nucleotide-binding protein that isnormally activated in response to the binding of signal molecules.

A.D. Falchook, J.E. Tepper / Seminars in Colon and Rectal Surgery 25 (2014) 13–18 15
There are three major isoforms of RAS: HRAS, NRAS, and KRAS.These isoforms vary primarily at the C-terminal domain. Differ-ences in this domain allow posttranscriptional modification of theprotein by addition of molecules such as farnesyl pyrophosphateor palmitate. The addition of these molecules is critical in bindingRAS to the plasma membrane as well as membranes within thecell, which is required for proper functioning. KRAS is the mostcommonly mutated isoform seen in 30% of CRC, although NRAS ismutated in 10% of CRC.3
Once it is membrane-bound, KRAS can be activated by anumber of signaling pathways. The receptor tyrosine kinase(RTK) activation pathway is of significant importance in CRC. Inresponse to extracellular signals, plasma membrane RTK induces aGTP-bound active state of KRAS. When activated, KRAS activates anumber of pathways that are important for cellular growth andproliferation. RAS proteins possess an intrinsic GTPase activity thatallows conversion of bound GTP to GDP, thereby transforming RASto the inactive state.
A critical mutation that can occur in the process of oncogenictransformation of CRC is an activating KRAS mutation. Thismutation causes impaired function of the intrinsic GTPase activityof KRAS, causing the protein to be perpetually bound to GTP in anactive state. Over 90% of these mutations occur at codons 12 and13, but there are a number of different amino acid substitutionsthat can occur. There are data to suggest that the location and typeof amino acid substitution, rather than simply the presence orabsence of any KRAS mutation, are prognostic for outcome in CRCpatients.14
A recent meta-analysis did not show a statistically significantcorrelation between KRAS mutation status and outcomes inpatients with CRC.15 Heterogeneity of study populations as wellas differences in the location and type of KRAS mutation mayexplain why statistically significant differences in outcome aredifficult to detect in clinical studies. Furthermore, other genemutations such as BRAF or TP53 can confound efforts to studythe prognostic significance of a KRAS mutation. For example, BRAFmutations occur almost exclusively in KRAS wild-type tumors, andtherefore one must account for BRAF mutation status in thepatients with wild-type KRAS. However, BRAF mutation appearsto confer a worse prognosis than a KRAS mutation.
An important question for oncologists is whether KRAS muta-tion predicts for response to neoadjuvant chemoradiotherapy. Ameta-analysis of 8 published articles containing approximately700 patients examined differences in pathologic completeresponse rate, tumor down-staging, or increase in cancer-relatedmortality for patients with KRAS mutations versus wild-typetumors.16 KRAS mutation was not associated with statisticallysignificant decreased rates of pCR (odds ratio[OR] ¼ 0.778,p ¼ 0.418), decreased rates of tumor down-staging (OR ¼ 0.846,p ¼ 0.728), or an increase in cancer-related mortality (OR ¼ 1.239,p ¼ 0.555). However, heterogeneity of KRAS mutation type as wellas concomitant mutations in other oncogenes was not accountedfor in that analysis. A series of 148 patients with Stage II–III rectalcancer treated with neoadjuvant chemoradiotherapy demon-strated a 0% pCR rate in the 12 patients with a KRAS mutation incodon 13 versus a 17% pCR rate in 48 patients with mutations inother codons and a 33% pCR rate in the 88 patients with wild-typeKRAS.17 Furthermore, 75% of tumors with KRAS mutations incodon 13 also had p53 mutations, while fewer than 40% of tumorswith KRAS mutations in other codons had p53 mutations. Detailedanalysis of KRAS mutations in CRC has shown that mutations at agiven codon may have variable significance, depending on whichamino acid is substituted. When compared to patients with wild-type KRAS, the multivariate hazard ratio for CRC-specific mortalityin patients with a p.G12V mutation at codon 12 of KRAS was 2.00(95% confidence interval ¼ 1.38–2.90), whereas the multivariate
hazard ratio for CRC-specific mortality for patients with anymutation in codon 12 of KRAS was only 1.30 (95% confidenceinterval ¼ 1.02–1.67).14 These findings illustrate the importance ofaccounting for codon location and mutation type as well asconcomitant mutations in other oncogenes when attempting todetermine the prognostic or predictive significance of KRASmutations in rectal cancer.
1.3. TGF-β
Transforming growth factor beta (TGF-β) is a dimeric polypep-tide cytokine and is important in the regulation of cellularproliferation, differentiation, wound healing, immune response,angiogenesis, and tumor suppression.18 There are three isoforms ofTGF-β that are expressed in different tissue types: TGF-β1 mRNA isexpressed in endothelial, hematopoietic, and connective tissuecells; TGF-β2 is expressed in epithelial and neuronal cells; andTGF-β3 is primarily expressed in mesenchymal cells. Almost allcells in the human body produce TGF-β and have receptors forTGF-β. TGF-β signaling is mediated via phosphorylation of Smadproteins that enter the nucleus to interact with transcriptionfactors.
An important function of TGF-β is cell cycle regulation; itstimulates cell cycle arrest in the G1 phase by inhibition ofcyclin-dependent kinases as well as cyclin proteins, which resultsin down-regulation of signaling via the E2F–Rb pathway. Thiscauses decreased expression of c-Myc. Therefore, decreased TGF-βsignaling can lead to increased cellular proliferation and decreasedapoptosis. TGF-β also functions in the extracellular matrix (ECM) tostimulate the production of ECM proteins as well as to decreaseproduction of enzymes that degrade ECM. Furthermore, TGF-β is adirect stimulator of angiogenesis. Due to these effects on the ECMand angiogenesis, TGF-β signaling is important in cancer invasionand metastasis.
In vivo evidence suggests that the TGF-β pathway is importantin carcinogenesis. Mice with a homozygous deletion of Smad3(a downstream protein in the TGF-β pathway) develop aggressivemetastatic colorectal cancer at an early age.19 However, Smad3mutations are seen infrequently in human CRC, although theoverall rate of mutation in the TGF-β pathway in human CRC isapproximately 30%.3 Tumor cells with mutations in the TGF-βpathway usually demonstrate resistance to growth inhibition byTGF-β, which leads to a subsequent increase in the production ofTGF-β by both the tumor cells and surrounding stromal cells. Theincreased concentration of TGF-β may contribute to tumor pro-gression via stimulation of angiogenesis and cellular motility.Previous studies have shown increased levels of TGF-β in meta-static human CRC.20 Furthermore, a recent study of more than2300 patients with CRC found that abnormalities in the TGF-βsignaling pathway were associated with a statistically significantincreased risk of death.21 The authors identified gene mutationsand single nucleotide polymorphisms in the TGF-β pathwayassociated with overall survival in rectal cancer and found a hazardratio of 6.03 (95% confidence interval ¼ 2.83–12.75) for patientswith tumors that had a high-risk genomic profile.
The interaction between the TGF-β pathway and toxicity fromradiotherapy has been the subject of much research. Because ofthe important role that TGF-β plays in wound healing, inflamma-tion, cellular proliferation, and angiogenesis, it has been proposedthat TGF-β promotes late tissue injury following radiotherapy.22
This hypothesis is supported by animal experiments; one studydemonstrated that mice lacking Smad3 (and therefore havingimpaired TGF-β pathway signaling) have a lower risk of cutaneousinjury after exposure to ionizing radiation.23 The hypothesis thatthere is a relationship between the TGF-β pathway and toxicity isalso supported by data based on studies in humans. An analysis of
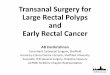
Fig. 2. EGFR can activate both the RAS and PI3K pathways, which lead to genetranscription resulting in increased cellular proliferation.
A.D. Falchook, J.E. Tepper / Seminars in Colon and Rectal Surgery 25 (2014) 13–1816
163 patients with rectal cancer who received neoadjuvant chemo-radiotherapy showed that all 21 patients carrying the TGFB1Arg25Pro polymorphism had grade 2 or greater toxicity for enter-itis, proctitis, cystitis, or dermatitis (toxicity was measured usingCommon Terminology Criteria for Adverse Events).24 However, thenegative predictive value of this polymorphism for toxicity wasonly 40% due to a relatively low frequency of the Pro25 variant andhigh frequency of toxicity in all patients.
The response to neoadjuvant chemoradiotherapy may berelated to signaling in the TGF-β pathway. A study of 17 rectaltumors in patients who received neoadjuvant chemoradiotherapyshowed higher expression of TGF-β1 by a factor of 1.32 (p ¼ 0.045)in tumors that responded to neoadjuvant therapy compared totumors that showed less response.25 Genes regulating matrixmetalloproteinases, apoptosis, DNA repair, and cellular prolifera-tion were also overexpressed by up to a factor of 2.63 (p ¼ 0.007)in tumors that responded to neoadjuvant therapy. A better under-standing of the gene expression changes and mutations in theTGF-β signaling pathway is needed to help predict how patientswill respond to neoadjuvant chemoradiotherapy in terms of bothtoxicity as well as tumor response.
1.4. p53
Mutations of the tumor suppressor p53 are frequently detectedin human cancers. The p53 protein is encoded by the TP53 gene,located on the short arm of chromosome 17. The negative regulatorMDM2 functions to inactivate p53 under physiologic conditions. Inresponse to DNA damage, hypoxia, or other cellular stressors, p53and MDM2 dissociate. This allows p53 to enter the nucleus, whereit promotes transcription of genes responsible for cell cycle arrest,DNA repair, and apoptosis. The net effect is that a functioning p53pathway leads to either repair of damaged DNA or apoptosis incells that have suffered irreparable damage.
The p53 protein forms a homotetramer that is essential for p53to function in vivo. Mutations can occur in the homo-oligomerization domain of p53, which leads to an inability forthe formation of the functional homotetramer; these types ofmutations demonstrate a dominant negative effect. Mutations thatoccur in the DNA-binding core domain of p53 interfere with theability of p53 to bind to its target DNA sequences. These types ofmutations demonstrate a recessive negative effect.
Inactivating mutations in p53 occur in over 50% of human CRC.3
Although a small study of 31 men demonstrated a statisticallysignificant inverse relationship between survival and p53 muta-tion,26 a larger study of over 1000 patients did not show asignificant association between p53 mutation status and overallsurvival.27 Interestingly, the authors of the larger study detectedan effect of p53 mutation on overall survival when body massindex (BMI) was taken into account; non-obese patients with ap53 mutation had a shorter cancer-specific survival (hazard ratio¼ 1.53, 95% confidence interval ¼ 1.17–2.00). Among obesepatients (BMI 4 30), p53 mutation was not associated withsurvival and the adverse effect of BMI on survival was limited topatients with wild-type p53. A proposed explanation for thisfinding is that changes in cellular energy metabolism due to p53mutations may interact with cell cycle dysregulation, which is alsoseen in p53 mutated cells. It is important to consider the role ofp53 mutations in all aspects of cell signaling and not just inpathways that have been traditionally been considered oncogenic.
The clinical significance of p53 mutation status on responseto neoadjuvant radiotherapy in rectal cancer is still under inves-tigation. Cells with mutated p53 may be less likely to undergo cellcycle arrest and/or apoptosis after exposure to DNA damagecaused by ionizing radiation. Studies on animals have shown thatmouse thymocytes with mutated p53 do not undergo apoptosis
after exposure to ionizing radiation, while cell lines with intactp53 are sensitive to radiation.28 Whether this effect holds true inrectal cancer patients is not known.
A recent meta-analysis of 30 published studies including 1830patients suggests that tumors with wild-type p53 may be morelikely to exhibit good response or complete response to neo-adjuvant radiotherapy compared to mutated p53 tumors.29 How-ever, the effect of p53 mutation was modest; the relative risk forgood response to neoadjuvant treatment for tumors with p53mutations was 0.84 (95% confidence interval ¼ 0.75–0.96, p ¼0.007). Furthermore, mutation status of p53 did not affect patientsurvival or degree of tumor regression after radiotherapy for rectalcancer in several recent series.30–32
1.5. PI3K
Phosphatidylinositide 3-kinases (PI3K) are a family of enzymesthat phosphorylate the hydroxyl group at the third position of theinositol ring of phosphatidylinositol. These enzymes play animportant role in signaling mediated by the insulin receptorsubstrate that regulates glucose uptake. This pathway is alsoinvolved in other cellular functions such as cell growth, differ-entiation, motility, and survival. The PI3K enzymes are divided intothree classes based on structure and function; one of the mostimportant gene products is the p110α catalytic subunit (encodedby the PIK3CA gene) which is an oncogene.33 Although there isaltered signaling in the PI3K pathway in approximately 50% of CRC,there is an activating mutation in PIK3CA present in approximately15% of non-hypermutated tumors.3 The relationship betweenEGFR, RAS, and PI3K is shown in Figure 2.
An analysis of 1170 colon and rectal cancers was performed todetermine the prognostic value of PIK3CA mutation in patientswith CRC.34 After adjusting for clinical and molecular features(including KRAS and BRAF mutation status), a significantly worsecancer-specific survival (multivariate hazard ratio 3.51, 95% con-fidence interval ¼ 1.28–9.62, log rank p ¼ 0.031) was observed inpatients with tumors that had mutations in both exon 9 and exon20 of PIK3CA. Mutations in either exon 9 or exon 20 alone were notassociated with survival. Evaluation of 240 tumors from non-irradiated patients in the Dutch Total Mesorectal Excision (TME)trial found an increased 5-year risk of local recurrence of 28% inPIK3CA-mutated tumors versus 9% in non-mutated tumors.35

Table 1Studies that evaluate the genomic profile of CRC and tumor response to radiotherapy.
References Title Year published Genes studied
Spitzner et al.12 A gene expression signature for chemoradiosensitivity ofcolorectal cancer cells
2010 STAT3, RASSF1, DOK3, ERBB2, WNT, and insulin
Nishioka et al.25 Gene expression profile can predict pathological response topreoperative chemoradiotherapy in rectal cancer
2011 MMP, NFκB, TGFB1, Topoisomerase, and integrin
Ghadimi et al.41 Effectiveness of gene expression profiling for responseprediction of rectal adenocarcinomas to preoperativechemoradiotherapy
2005 54 genes
Edden et al.42 The use of molecular markers as a method to predict theresponse to neoadjuvant therapy for advanced-stage rectaladenocarcinoma
2012 COX-2, VEGF, P53, P21, P27, BAS, BCL-2, and APAF-1
Chen et al.43 Molecular diagnosis of response to neoadjuvantchemoradiation therapy in patients with locally advancedrectal cancer
2011 KRAS and P53
Garcia-Aguilar et al.44 Identification of a biomarker profile associated with resistanceto neoadjuvant chemoradiation therapy in rectal cancer
2011 KRAS, CCND1 G870A polymorphisms, MTHFR C667Tpolymorphism, and P53
A.D. Falchook, J.E. Tepper / Seminars in Colon and Rectal Surgery 25 (2014) 13–18 17
Furthermore, median time to local recurrence was shorter at7.9 months versus 19.6 months in the group with wild-typePIK3CA.
Based on the increased risk of local recurrence associated withPIK3CA mutation, one may surmise that patients with this mutationhave a strong indication for treatment with chemoradiotherapy. Toexamine this question, the authors of the Dutch TME trial performedan analysis of PIK3CA mutation status for 30 out of 32 tumorsamples in patients who received irradiation and had a localrecurrence as well as in 24 out of 74 patients who did not receiveirradiation and had a local recurrence.36 This demonstrated aPIK3CA mutation prevalence of 2/30 (6.7%) in the irradiated tumorsthat recurred versus 5/24 (20.8%) in the non-irradiated tumors thatrecurred; the corresponding interaction odds ratio of 0.3 (95%confidence interval ¼ 0.05–1.56) suggests a possible increasedrelative benefit from radiotherapy among PIK3CA-mutated patientswith respect to local recurrence. However, this unplanned retro-spective analysis was underpowered to detect such a difference andthese results should be viewed as hypothesis generating.
The presence or absence of a PIK3CA mutation may haveimplications regarding medical therapy in CRC as well. A studyof 964 patients with CRC from several health registries indicatedthat in patients with PIK3CA-mutated cancers, regular use ofaspirin after diagnosis was associated with superior cancer-specific survival with a multivariate hazard ratio of 0.18 (p o0.001).37 The benefit of aspirin was not observed in cancers withwild-type PIK3CA. The proposed explanation for this phenomenonis that inhibition of cyclooxygenase-2 (COX-2) by aspirin downregulates PI3K signaling activity. Experimental evidence hasshown that activation of PI3K and WNT signaling is associatedwith COX-2/prostaglandin E2 production, which in turn leads toinhibition of apoptosis in colon cancer, and that the use of COXinhibitors to target this pathway can restore apoptosis.38
2. Response to neoadjuvant radiotherapy
It is desirable to identify which patients are more likely torespond to neoadjuvant treatment because patients with a favor-able genomic profile who demonstrate a pCR to neoadjuvanttherapy may be candidates for treatment de-intensification. Sev-eral published series have shown that carefully selected rectalcancer patients who demonstrate pCR to neoadjuvant chemo-therapy can avoid surgery if they are followed up with very closesurveillance.39,40 However, genomic profiling of tumors was notutilized in these studies to determine which patients should notreceive surgery.
Conversely, patients who are found to have an unfavorabletumor genomic profile at diagnosis may be candidates for differenttherapeutic approaches including use of alternative biologic orchemotherapeutic agents, new radiosensitizing agents, or initialsurgical management. Despite advances in our understanding ofoncogenic pathways in CRC, determining the exact genomic factorsresponsible for the heterogeneous response to neoadjuvant radio-therapy in rectal cancer has proven elusive.
A systematic review of the literature published by Kuremskyet al.32 examined the most commonly researched biomarkers forpredicting rectal cancer response to neoadjuvant chemoradiother-apy. The authors investigated six biomarkers as potential markersof response to radiotherapy: p53, epidermal growth factor recep-tor (EGFR), thymidylate synthase, Ki-67, p21, and bcl-2/bax. Basedon the available data, they concluded that p53, Ki-6, and bcl-2 areunlikely to be useful as predictors of response; EGFR and thymi-dylate synthase were promising as predictors of response; and p21and bax required further study.
There is great interest in developing predictive and prognosticmolecularly based models. None of these have fully demonstratedclinical utility as the ability to have a high positive and negativepredictive value has been difficult to attain. In addition, severalrecent studies have aimed to correlate the genomic profile of rectaltumors with response to chemoradiotherapy. An accurate profilecould potentially define patients who could be cured by primaryradiation therapy with concurrent chemotherapy or patients whowould be unlikely to benefit from the use of radiation treatment.These studies are briefly described in Table 1.12,25,41–44
3. Conclusion
Extensive research has significantly expanded our understand-ing of CRC genomics, as outlined by the above discussion of thefive most commonly involved oncogenic pathways. However, ourknowledge of CRC genomics is somewhat limited in its ability toprovide information that is routinely used to guide clinicaldecisions. Continued research into the genomic profile of CRC willallow clinicians to optimize treatment strategies and better under-stand this complex disease.
References
1. Wilkins JA, Sansom OJ. C-Myc is a critical mediator of the phenotypes of Apcloss in the intestine. Cancer Res. 2008;68(13):4963–4966.
2. Sun W. Angiogenesis in metastatic colorectal cancer and the benefits oftargeted therapy. J Hematol Oncol. 2012;5:63 10.1186/1756-8722-5-63.

A.D. Falchook, J.E. Tepper / Seminars in Colon and Rectal Surgery 25 (2014) 13–1818
3. The Cancer Genome Atlas Network. Comprehensive molecular characterizationof human colon and rectal cancer. Nature. 2012;487(7407):330–337.
4. Fearon ER. Molecular genetics of colorectal cancer. Annu Rev Pathol.2011;6:479–507 10.1146/annurev-pathol-011110-130235.
5. van de Wetering M, Sancho E, Verweij C, et al. The beta-catenin/TCF-4 compleximposes a crypt progenitor phenotype on colorectal cancer cells. Cell. 2002;111(2):241–250.
6. Verma UN, Surabhi RM, Schmaltieg A, et al. Small interfering RNAs directedagainst b-catenin inhibit the in vitro and in vivo growth of colon cancer cells.Clin Cancer Res. 2003;9(4):1291–1300.
7. Thakur R, Mishra DP. Pharmacological modulation of beta-catenin and itsapplications in cancer therapy. J Cell Mol Med. 2013;17(4):449–456.
8. Mologni L, Dekhil H, Ceccon M, et al. Colorectal tumors are effectivelyeradicated by combined inhibition of β-catenin, KRAS, and the oncogenictranscription factor ITF2. Cancer Res. 2010;70(18):7253–7263.
9. Mologni L, Brussolo S, Ceccon M, et al. Synergistic effects of combined wnt/KRAS inhibition in colorectal cancer cells. PLoS One. 2012;7(12):e51449.
10. Ueno K, Hiura M, Suehiro Y, et al. Frizzled-7 as a potential therapeutic target incolorectal cancer. Neoplasia. 2008;10(7):697–705.
11. Gurney A, Axelrod F, Bond CJ, et al. Wnt pathway inhibition via the targeting offrizzled receptors results in decreased growth and tumorigenicity of humantumors. Proc Natl Acad Sci U S A. 2012;109(29):11717–11722.
12. Spitzner M, Emons G, Kramer F, et al. A gene expression signature forchemoradiosensitivity of colorectal cancer cells. Int J Radiat Oncol Biol Phys.2010;78(4):1184–1192.
13. Kendziorra E, Ahlborn K, Spitzner M, et al. Silencing of the Wnt transcriptionfactor TCF4 sensitizes colorectal cancer cells to (chemo-) radiotherapy. Carcino-genesis. 2011;32(12):1824–1831.
14. Imamura Y, Morikawa T, Liao X, et al. Specific mutations in KRAS codons 12 and13, and patient prognosis in 1075 BRAF wild-type colorectal cancers. ClinCancer Res. 2012;18(17):4753–4763.
15. Ren JJ, Li GX, Ge J, et al. Is K-ras gene mutation a prognostic factor for colorectalcancer: a systematic review and meta-analysis. Dis Colon Rectum. 2012;55(8):913–923.
16. Clancy C, Burke JP, Coffey JC. KRAS mutation does not predict the efficacy ofneo-adjuvant chemoradiotherapy in rectal cancer: a systematic review andmeta-analysis. Surg Oncol. 2013;22(2):105–111.
17. Duldulao MP, Lee W, Nelson RA, et al. Mutations in specific codons of the KRASoncogene are associated with variable resistance to neoadjuvant chemoradiationtherapy in patients with rectal adenocarcinoma. Ann Surg Oncol. 2013;(7):2166–2171.
18. Blobe GC, Scheimann WP, Lodish HF. Role of transforming growth factor β inhuman disease. N Engl J Med. 2000;342(18):1350–1358.
19. Zhu Y, Richardson JA, Parada LF, et al. Smad3 mutant mice develop metastaticcolorectal cancer. Cell. 1998;94(6):03–714.
20. Picon A, Gold LI, Wang J, et al. A subset of metastatic human colon cancersexpresses elevated levels of transforming growth factor beta-1. Cancer Epide-miol Biomarkers Prev. 1998;7(6):497–504.
21. Slattery ML, Lundgreen A, Herrick JS, et al. Genetic variation in the transforminggrowth factor-β signaling pathway and survival after diagnosis with colon andrectal cancer. Cancer. 2011;117(18):4175–4183.
22. Caney PA, Dean S. Transforming growth factor beta: a promotor of lateconnective tissue injury following radiotherapy? Br J Radiol. 1990;63(752):620–623.
23. Flanders KC, Sullivan CD, Fujii M, et al. Mice lacking Smad3 are protectedagaints cutaneous injury following ionizing radiation. Am J Pathol. 2002;160(3):1057–1068.
24. Schirmer MA, Mergler CP, Rave-Frank M, et al. Acute toxicity of radiochemo-therapy in rectal cancer patients: a risk particularly for carriers of the TGFB1Pro25 variant. Int J Radiat Oncol Biol Phys. 2012;83(1):149–157.
25. Nishioka M, Shimada M, Kurita N, et al. Gene expression profile can predictpathological response to preoperative chemoradiotherapy in rectal cancer.Cancer Genomics Proteomics. 2011;8(2):87–92.
26. Lumachi F, Orlando R, Marino F, et al. Expression of p53 and Ki-67 as prognosticfactors for survival of men with colorectal cancer. Anticancer Res. 2012;32(9):3965–3967.
27. Morikawa T, Kuchiba A, Liao X, et al. Tumor TP53 expression status, body massindex and prognosis in colorectal cancer. Int J Cancer. 2012;131(5):1169–1178.
28. Lowe SW, Schmitt EM, Smith SW, et al. p53 is required for radiation-inducedapoptosis in mouse thymocytes. Nature. 1993;362(6423):847–849.
29. Chen MB, Wu XY, Yu R, et al. P53 status as a predictive biomarker for patientsreceiving neoadjuvant radiation based treatment: a meta-analysis in rectalcancer. PLoS One. 2012;7(9):e45388.
30. Andrade NR, Oshima CT, Gomes TS, et al. Imunoexpression of Ki-67 and p53 inrectal cancer tissue after treatment with neoadjuvant chemoradiation. J Gastro-intest Cancer. 2011;42(1):34–39.
31. Garcia VM, Batlle JF, Casado E, et al. Immunohistochemical analysis of tumourregression grade for rectal cancer after neoadjuvant chemoradiotherapy. Color-ectal Dis. 2011;13(9):989–998.
32. Kuremsky JG, Tepper JE, McLeod HL. Biomarkers for response to neoadjuvantchemoradiation for rectal cancer. Int J Radiat Oncol Biol Phys. 2009;74(3):673–688.
33. Ma YY, Wei SJ, Lin YC, et al. PIK3CA as an oncogene in cervical cancer. Oncogene.2000;19(23):2739–2744.
34. Liao X, Morikawa T, Lochhead P, et al. Prognostic role of PIK3CA mutation incolorectal cancer: cohort study and literature review. Clin Cancer Res. 2012;18(8):2257–2268.
35. He Y, Van't Veer LJ, Mikolajewska-Hanclich I, et al. PIK3CA mutations predictlocal recurrences in rectal cancer patients. Clin Cancer Res. 2009;15(22):6956–6962.
36. He Y, Van't Veer LJ, Lopez-Yurda, et al. Do rectal cancer patients with PIK3CAmutations benefit from preoperative radiotherapy with regard to local recur-rences? Clin Cancer Res. 2010;16(24):6179.
37. Liao X, Lochhead P, Nishihara R, et al. Aspirin use, tumor PIK3CA mutation, andcolorectal-cancer survival. N Engl J Med. 2012;367(17):1596–1606.
38. Kaur J, Sanyal SN. PI3-kinase/Wnt association mediates COX-2/PGE(2) pathwayto inhibit apoptosis in early stages of colon carcinogenesis: chemopreventionby diclofenac. Tumour Biol. 2010;31(6):623–631.
39. Habr-Gama A, Perez RO, Nadalin W, et al. Operative versus nonoperativetreatment for stage 0 distal rectal cancer following chemoradiation therapy:long-term results. Ann Surg. 2004;240(4):711–717.
40. Maas M, Beets-Tan RG, Lambregts DM, et al. Wait-and-see policy for clinicalcomplete responders after chemoradiation for rectal cancer. J Clin Oncol.2011;29(35):4633–4640.
41. Ghadimi BM, Grade M, Difilippantonio MJ, et al. Effectiveness of geneexpression profiling for response prediction of rectal adenocarcinomas topreoperative chemoradiotherapy. J Clin Oncol. 2005;23(9):1826–1838.
42. Edden Y, Wexner SD, Berho M. The use of molecular markers as a method topredict the response to neoadjuvant therapy for advanced stage rectaladenocarcinoma. Colorectal Dis. 2012;14(5):555–561.
43. Chen Z, Duldulao MP, Li W, et al. Molecular diagnosis of response to neo-adjuvant chemoradiation therapy in patients with locally advanced rectalcancer. J Am Coll Surg. 2011;212(6):1008–1017.
44. Garcia-Aguilar J, Chen Z, Smith DD, et al. Identification of a biomarker profileassociated with resistance to neoadjuvant chemoradiation therapy in rectalcancer. Ann Surg. 2011;254(3):486–492.