Embed Size (px)
DESCRIPTION
Citation preview

Rectum and Rectum and anusanus
Celso M. Fidel, MD, FPCS, FPSGSCelso M. Fidel, MD, FPCS, FPSGS
Diplomate Philippine Board of SurgeryDiplomate Philippine Board of Surgery

EmbryologyEmbryology
The embryonic gastrointestinal tract begins The embryonic gastrointestinal tract begins developing during the developing during the fourth weekfourth week of of gestation.gestation.
The primitive gut is derived from the endoderm The primitive gut is derived from the endoderm and divided into and divided into three segmentsthree segments: :
1. Foregut 1. Foregut
2. Midgut 2. Midgut
3. Hindgu3. Hindgutt
Both Both midgutmidgut and and hindguthindgut contribute to the contribute to the colon, rectum, and anus.colon, rectum, and anus.

EmbryologyEmbryology The The hindguthindgut develops into the distal transverse develops into the distal transverse colon, descending colon, colon, descending colon, rectumrectum, and , and proximal anusproximal anus, all of which receive their blood , all of which receive their blood supply from the supply from the inferior mesenteric arteryinferior mesenteric artery. .
During the During the sixth week sixth week of gestation, the distal-of gestation, the distal-most end of the hindgut, the most end of the hindgut, the cloacacloaca, is divided , is divided by the urorectal septum into the by the urorectal septum into the urogenital urogenital sinus sinus and the and the rectum.rectum.

EmbryologyEmbryology The distal anal canal is derived from: The distal anal canal is derived from:
ectoderm ectoderm and receives its blood supply from and receives its blood supply from the internal the internal pudendal arterypudendal artery. .
The The dentate line dentate line divides the endodermal divides the endodermal hindgut from the ectodermal distal anal canal.hindgut from the ectodermal distal anal canal.

AnatomyAnatomy
The large intestine extends from the ileocecal The large intestine extends from the ileocecal valve to anus. Anatomically & functionally valve to anus. Anatomically & functionally divided to the divided to the colon, rectumcolon, rectum, and , and anal canalanal canal. .
The rectum comprise five distinct layers: The rectum comprise five distinct layers:
1.1. MucosaMucosa
2.2. SubmucosaSubmucosa
3.3. Inner circular muscleInner circular muscle
4.4. Outer longitudinal muscleOuter longitudinal muscle
5.5. Serosa. Serosa.

AnatomyAnatomy
TThe outer longitudinal muscle is separated into he outer longitudinal muscle is separated into three teniae colithree teniae coli, which converge proximally , which converge proximally at the at the appendixappendix and distally at the and distally at the rectumrectum
The outer longitudinal muscle layer of rectum is The outer longitudinal muscle layer of rectum is circumferentialcircumferential

AnatomyAnatomy
In the distal rectum, the In the distal rectum, the inner smooth-muscle inner smooth-muscle layer coalesces to form the layer coalesces to form the internal anal internal anal sphincter.sphincter.
The The intraperitoneal colon intraperitoneal colon and and proximal one proximal one third third of the rectum are covered by of the rectum are covered by serosaserosa; the ; the mid and lower rectum lack serosa.mid and lower rectum lack serosa.

AnatomyAnatomy
The rectosigmoid junction is found at The rectosigmoid junction is found at approximately the level of the approximately the level of the sacral promontorysacral promontory and is arbitrarily described as the point at which and is arbitrarily described as the point at which the three the three teniae coliteniae coli coalesce to form the outer coalesce to form the outer longitudinal smooth muscle layer of the rectum longitudinal smooth muscle layer of the rectum

ARTERIAL SUPPLYARTERIAL SUPPLYMCA IMA
SMA LCA
SRA Sig. A
ICA
RCA

Marginal artery of Drummond

Blood SupplyBlood Supply The The inferior mesenteric arteryinferior mesenteric artery branches into the branches into the
left colic arteryleft colic artery, which supplies the , which supplies the descending descending colon,colon, several several sigmoidal branchessigmoidal branches, which , which supply the supply the sigmoid colonsigmoid colon, and the , and the superior superior rectal arteryrectal artery,, which supplies the which supplies the proximal proximal rectumrectum. .
The terminal branches of each artery form The terminal branches of each artery form anastomoses with the terminal branches of the anastomoses with the terminal branches of the adjacent artery and communicate via the adjacent artery and communicate via the marginal artery of Drummondmarginal artery of Drummond. .

Venous DrainageVenous Drainage
Except for the Except for the inferior mesenteric veininferior mesenteric vein, the , the veins of the colon parallel their corresponding veins of the colon parallel their corresponding arteries and bear the same terminology arteries and bear the same terminology
The inferior mesenteric vein ascends in the The inferior mesenteric vein ascends in the retroperitoneal plane over the psoas muscle retroperitoneal plane over the psoas muscle and continues posterior to the pancreas to join and continues posterior to the pancreas to join the splenic vein. the splenic vein.
During a colectomy, this vein is often mobilized During a colectomy, this vein is often mobilized independently and ligated at the inferior edge of independently and ligated at the inferior edge of the pancreas.the pancreas.

LYMPHATIC DRAINAGELYMPHATIC DRAINAGE

lymphatic drainagelymphatic drainage
The lymphatic drainage of the colon originates in The lymphatic drainage of the colon originates in a network of lymphatics in the muscularis a network of lymphatics in the muscularis mucosa.mucosa.
Lymphatic vessels and lymph nodes follow the Lymphatic vessels and lymph nodes follow the regional arteries. regional arteries.

lymphatic drainagelymphatic drainage
Lymph nodes are found on:Lymph nodes are found on:
1. The bowel wall (epicolic)1. The bowel wall (epicolic)
2. Inner margin of the bowel adjacent to the 2. Inner margin of the bowel adjacent to the
arterial arcades (paracolic)arterial arcades (paracolic)
3. Around the named mesenteric vessels 3. Around the named mesenteric vessels (intermediate)(intermediate)
4. Origin of the superior and inferior mesenteric 4. Origin of the superior and inferior mesenteric arteries (main). arteries (main).

lymphatic drainagelymphatic drainage
The The sentinel lymph nodessentinel lymph nodes are the first one to are the first one to four lymph nodes to drain a specific segment of four lymph nodes to drain a specific segment of the colon, and are thought to be the first site of the colon, and are thought to be the first site of metastasis in colon cancer. The utility of metastasis in colon cancer. The utility of sentinel lymph node dissection and analysis in sentinel lymph node dissection and analysis in colon cancer remains controversial.colon cancer remains controversial.

Anorectal LandmarksAnorectal Landmarks The rectum is approximately The rectum is approximately 12 to 15 12 to 15 cm in length. cm in length.
Three distinct submucosal folds:Three distinct submucosal folds:
1.Valves of Houston1.Valves of Houston, extend into the rectal lumen., extend into the rectal lumen.
2. Posteriorly, the 2. Posteriorly, the presecral fasciapresecral fascia separates the separates the rectum from the presacral venous plexus and the rectum from the presacral venous plexus and the pelvic nerves. pelvic nerves.
3. At S4, the 3. At S4, the rectosacral fascia rectosacral fascia ((Waldeyer's fasciaWaldeyer's fascia) ) extends forward and downward and attaches to the extends forward and downward and attaches to the fascia propria at the anorectal junction. fascia propria at the anorectal junction.

ANORECTAL ANATOMYANORECTAL ANATOMY
Rectosigmoid (fusion of taenia coli) to anal canalRectosigmoid (fusion of taenia coli) to anal canal
3 distinct intraluminal curves 3 distinct intraluminal curves (Valves of Houston)(Valves of Houston)
- Proximal & distal curves convex to the right- Proximal & distal curves convex to the right
- Middle curve marks the - Middle curve marks the anterior peritoneal anterior peritoneal
reflectionreflection
- Posterior peritoneal reflection - Posterior peritoneal reflection 12-15 cm from 12-15 cm from
anal vergeanal verge

Anorectal LandmarksAnorectal Landmarks Anteriorly, Anteriorly, Denonvilliers' fasciaDenonvilliers' fascia separates the rectum separates the rectum
from the prostate and seminalfrom the prostate and seminal vesicles in men and vesicles in men and from the vagina in womenfrom the vagina in women
The The lateral ligamentslateral ligaments support the lower rectum. support the lower rectum.
The The surgical anal canal surgical anal canal measures 2 to 4 cm in measures 2 to 4 cm in length and is generally longer in men than in length and is generally longer in men than in women. It women. It beginsbegins at the at the anorectal junction anorectal junction and and terminatesterminates at the at the anal vergeanal verge. .

Anorectal LandmarksAnorectal Landmarks
The The dentatedentate or or pectinate linepectinate line marks the marks the transition transition pointpoint between between columnar rectal mucosa and columnar rectal mucosa and squamous anoderm.squamous anoderm.
The 1 to 2 cm of mucosa just proximal to the The 1 to 2 cm of mucosa just proximal to the dentate line shares histologic characteristics of dentate line shares histologic characteristics of columnar, cuboidal, and squamous epithelium columnar, cuboidal, and squamous epithelium and is referred to as the and is referred to as the anal transition zoneanal transition zone. .

Anorectal LandmarksAnorectal Landmarks The dentate line is surrounded by longitudinal The dentate line is surrounded by longitudinal
mucosal folds, known as the mucosal folds, known as the columns of columns of MorgagniMorgagni, into which the anal crypts empty. , into which the anal crypts empty. These crypts are the source of cryptoglandular These crypts are the source of cryptoglandular abscesses abscesses
In the distal rectum, the inner smooth muscle is In the distal rectum, the inner smooth muscle is thickened and comprises the thickened and comprises the internal anal internal anal sphinctersphincter that is surrounded by the that is surrounded by the subcutaneoussubcutaneous, , superficialsuperficial, and , and deep external deep external sphinctersphincter. .

Anorectal LandmarksAnorectal Landmarks The The deep external anal sphincterdeep external anal sphincter is an extension is an extension
of the of the puborectalis musclepuborectalis muscle. .
MusclesMuscles that form the that form the levator ani musclelevator ani muscle of the of the pelvic floor:pelvic floor:
1. Puborectalis1. Puborectalis
2. Iliococcygeus2. Iliococcygeus
3. Pubococcygeus3. Pubococcygeus

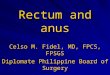
THE ANORECTUMTHE ANORECTUM
VALVES OF HOUSTON
DENTATE LINE
ANAL SPHINCTERS
ANAL VERGE
HEMORRHOIDAL Plx.

Anorectal Vascular SupplyAnorectal Vascular Supply
The The superior rectal artery superior rectal artery arises from the arises from the terminal terminal branch of the inferior mesenteric artery branch of the inferior mesenteric artery and and supplies the upper rectum. supplies the upper rectum.
The The middle rectal artery middle rectal artery arises from the arises from the internal internal iliaciliac; the presence and size of these arteries ; the presence and size of these arteries are highly variable.are highly variable.

Anorectal Vascular SupplyAnorectal Vascular Supply
The The inferior rectal artery inferior rectal artery arises from the arises from the internal internal
pudendal arterypudendal artery, which is a branch of the , which is a branch of the internal iliac artery. internal iliac artery.
A A rich network of collaterals connects the terminal rich network of collaterals connects the terminal arterioles of each of these arteriesarterioles of each of these arteries, thus making , thus making the rectum relatively resistant to ischemia the rectum relatively resistant to ischemia

ARTERIAL SUPPLYARTERIAL SUPPLYMCA IMA
SMA LCA
SRA Sig. A
ICA
RCA

Anorectal Vascular SupplyAnorectal Vascular Supply
The venous drainage of the rectum parallels the The venous drainage of the rectum parallels the arterial supply.arterial supply.
1.1. The The superior rectal veinsuperior rectal vein drains into the drains into the portal portal system system via the via the inferior mesenteric veininferior mesenteric vein..
2.2. The The middle rectal vein middle rectal vein drains into the drains into the internal internal iliac vein.iliac vein.
3.3. The The inferior rectal vein inferior rectal vein drains into the drains into the internal internal pudendal veinpudendal vein, and subsequently into the , and subsequently into the internal iliac veininternal iliac vein. .

Anorectal Vascular SupplyAnorectal Vascular Supply
A submucosal plexus deep to the columns of A submucosal plexus deep to the columns of Morgagni forms the Morgagni forms the hemorrhoidal plexushemorrhoidal plexus and and drains into all three veins.drains into all three veins.HEMORRHOIDAL PLEXUSHEMORRHOIDAL PLEXUS- Subepithelial vascular cushion- Subepithelial vascular cushion
a. a. INTERNAL HINTERNAL H – – aboveabove dentate line; insensate dentate line; insensate mucosamucosa
b. b. EXTERNAL H EXTERNAL H –– below below dentate line; lined by dentate line; lined by richly innervated anodermrichly innervated anoderm

Anorectal Vascular SupplyAnorectal Vascular Supply
Lymphatic drainage of the rectum parallels the Lymphatic drainage of the rectum parallels the vascular supply.vascular supply.
1.1. Lymphatic channels in the upper and middle Lymphatic channels in the upper and middle rectum drain superiorly into the inferior rectum drain superiorly into the inferior mesenteric lymph nodes.mesenteric lymph nodes.
2.2. Lymphatic channels in the lower rectum drain Lymphatic channels in the lower rectum drain both superiorly into the inferior mesenteric both superiorly into the inferior mesenteric lymph nodes and laterally into the internal iliac lymph nodes and laterally into the internal iliac lymph nodes. lymph nodes.

Anorectal Vascular SupplyAnorectal Vascular Supply
The anal canal has a more complex pattern of The anal canal has a more complex pattern of lymphatic drainage. lymphatic drainage.
1. Proximal to the dentate line, lymph drains into 1. Proximal to the dentate line, lymph drains into both the inferior mesenteric lymph nodes and both the inferior mesenteric lymph nodes and the internal iliac lymph nodes. the internal iliac lymph nodes.
2. Distal to the dentate line, lymph primarily 2. Distal to the dentate line, lymph primarily drains into the inguinal lymph nodes, but can drains into the inguinal lymph nodes, but can also drain into the inferior mesenteric lymph also drain into the inferior mesenteric lymph nodes and internal iliac lymph nodes.nodes and internal iliac lymph nodes.

Anorectal Anorectal Nerve SupplyNerve Supply
Both sympathetic and parasympathetic nerves Both sympathetic and parasympathetic nerves innervate the anorectum. innervate the anorectum.
1.Sympathetic nerve fibers from 1.Sympathetic nerve fibers from L1-L3L1-L3 join the join the preaortic plexus whose nerve fibers then extend preaortic plexus whose nerve fibers then extend below the aorta to form the below the aorta to form the hypogastric plexushypogastric plexus, , which subsequently joins the parasympathetic which subsequently joins the parasympathetic fibers to form the pelvic plexus.fibers to form the pelvic plexus.
2. Parasympathetic nerve fibers known as the 2. Parasympathetic nerve fibers known as the nervi erigentesnervi erigentes and originate from and originate from S2-S4. S2-S4. These These fibers join the sympathetic fibers to form the fibers join the sympathetic fibers to form the pelvic plexus. pelvic plexus.

Anorectal Anorectal Nerve SupplyNerve Supply
Sympathetic and parasympathetic fibers then Sympathetic and parasympathetic fibers then
supply the anorectum and adjacent urogenital supply the anorectum and adjacent urogenital organs.organs.

Anorectal Anorectal Nerve SupplyNerve Supply
The The internal anal sphincter internal anal sphincter is innervated by is innervated by sympathetic and parasympathetic nerve fibers; sympathetic and parasympathetic nerve fibers; both types of fibers inhibit sphincter contraction.both types of fibers inhibit sphincter contraction.
The The external anal sphincter external anal sphincter and puborectalis and puborectalis muscles are innervated by the muscles are innervated by the inferior rectal inferior rectal branchbranch of the of the internal pudendal nerveinternal pudendal nerve..

Anorectal Anorectal Nerve SupplyNerve Supply
The The levator ani levator ani receives innervation from both the receives innervation from both the
internal pudendal nerveinternal pudendal nerve and direct branches of and direct branches of S3 to S5. S3 to S5.
Sensory innervation to the anal canal is provided Sensory innervation to the anal canal is provided by the by the inferior rectal branchinferior rectal branch of the of the pudendal pudendal nervenerve..
The The rectum is relatively insensaterectum is relatively insensate, the anal canal , the anal canal below the dentate line is sensate.below the dentate line is sensate.

congenital congenital anomaliesanomalies
Perturbation of the embryologic development of Perturbation of the embryologic development of the midgut and hindgut the midgut and hindgut may result in anatomic may result in anatomic abnormalities of the colon, rectum, and anus abnormalities of the colon, rectum, and anus
Incomplete descent of the urogenital septum Incomplete descent of the urogenital septum may result in imperforate anus and associated may result in imperforate anus and associated fistulas to the genitourinary tractfistulas to the genitourinary tract

Motility, Defecation, and ContinenceMotility, Defecation, and Continence
MotilityMotility
Unlike the small intestine, the large intestine Unlike the small intestine, the large intestine does not demonstrate cyclic motor activity does not demonstrate cyclic motor activity characteristic of the migratory motor complexcharacteristic of the migratory motor complex
Bursts of "rectal motor complexes" Bursts of "rectal motor complexes" also have also have been described. In general, cholinergic been described. In general, cholinergic activation increases colonic motility.activation increases colonic motility.

Motility, Defecation, and ContinenceMotility, Defecation, and Continence
DefecationDefecation
Defecation is a complex, coordinated mechanism Defecation is a complex, coordinated mechanism involving: involving:
1. Colonic mass movement1. Colonic mass movement
2. Increased intra-abdominal and rectal pressure2. Increased intra-abdominal and rectal pressure
3. Relaxation of the pelvic floor. 3. Relaxation of the pelvic floor.

Motility, Defecation, and Continence Motility, Defecation, and Continence
DefecationDefecation
Distention of the rectum causes a reflex Distention of the rectum causes a reflex relaxation of the internal anal sphincter (the relaxation of the internal anal sphincter (the rectoanal inhibitory reflex) that allows the rectoanal inhibitory reflex) that allows the contents to make contact with the anal canal.contents to make contact with the anal canal.
This "sampling reflex" allows the sensory This "sampling reflex" allows the sensory epithelium to distinguish solid stool from liquid epithelium to distinguish solid stool from liquid stool and gas. If defecation does not occur, the stool and gas. If defecation does not occur, the rectum relaxes and the urge to defecate passes rectum relaxes and the urge to defecate passes (the (the accommodation responseaccommodation response

Motility, Defecation, and Continence Motility, Defecation, and Continence
DefecationDefecation
Defecation proceeds Defecation proceeds
1. By coordination of increasing intra-abdominal 1. By coordination of increasing intra-abdominal
pressure via the Valsalva maneuverpressure via the Valsalva maneuver
2. Increased rectal contraction2. Increased rectal contraction
3. Relaxation of the puborectalis muscle3. Relaxation of the puborectalis muscle
4. Opening of the anal canal.4. Opening of the anal canal.

Motility, Defecation, and ContinenceMotility, Defecation, and Continence
ContinenceContinence
The maintenance of fecal continence is at least The maintenance of fecal continence is at least as complex as the mechanism of defecation. as complex as the mechanism of defecation. Continence requires:Continence requires:
1.1. Adequate rectal wall compliance to Adequate rectal wall compliance to accommodate the fecal bolusaccommodate the fecal bolus
2.2. Appropriate neurogenic control of the pelvic Appropriate neurogenic control of the pelvic floor and sphincter mechanism floor and sphincter mechanism
3.3. Functional internal and external sphincter Functional internal and external sphincter muscles. muscles.

Motility, Defecation, and ContinenceMotility, Defecation, and Continence
ContinenceContinence
4. At rest, the puborectalis muscle creates a 4. At rest, the puborectalis muscle creates a "sling" around the distal rectum, forming a "sling" around the distal rectum, forming a relatively acute angle that distributes relatively acute angle that distributes intraabdominal forces onto the pelvic floor.intraabdominal forces onto the pelvic floor.
5. With defecation, this angle straightens, 5. With defecation, this angle straightens, allowing downward force to be applied along allowing downward force to be applied along the axis of the rectum and anal canal. the axis of the rectum and anal canal.
6.The internal and external sphincters are 6.The internal and external sphincters are tonically active at rest. tonically active at rest.

Motility, Defecation, and ContinenceMotility, Defecation, and Continence
ContinenceContinence
. The internal sphincter is responsible for most of . The internal sphincter is responsible for most of the resting, involuntary sphincter tone (resting the resting, involuntary sphincter tone (resting pressure). pressure).
The external sphincter is responsible for most of The external sphincter is responsible for most of the voluntary sphincter tone (squeeze the voluntary sphincter tone (squeeze pressure). pressure).
Branches of the pudendal nerve innervate both Branches of the pudendal nerve innervate both the internal and external sphincter the internal and external sphincter

Motility, Defecation, and ContinenceMotility, Defecation, and Continence
ContinenceContinence
Finally, the hemorrhoidal cushions may contribute Finally, the hemorrhoidal cushions may contribute to continence by mechanically blocking the anal to continence by mechanically blocking the anal canal. Thus, impaired continence may result canal. Thus, impaired continence may result from poor rectal compliance, injury to the from poor rectal compliance, injury to the internal and/or external sphincter or internal and/or external sphincter or puborectalis, or nerve damage or neuropathypuborectalis, or nerve damage or neuropathy

Clinical EvaluationClinical Evaluation
A A complete history and physical examination complete history and physical examination is is
the starting point for evaluating any patient with the starting point for evaluating any patient with suspected disease of the colon and rectum.suspected disease of the colon and rectum.
Special attention should be paid to the patient's Special attention should be paid to the patient's past medical and surgical history past medical and surgical history to detect to detect underlying conditions that might contribute to a underlying conditions that might contribute to a gastrointestinal problem.gastrointestinal problem.
If patients have had prior intestinal surgery, it is If patients have had prior intestinal surgery, it is essential that one understand the essential that one understand the resultant resultant gastrointestinal anatomy gastrointestinal anatomy

Clinical EvaluationClinical Evaluation
In addition, family history of colorectal disease, In addition, family history of colorectal disease, especially inflammatory bowel disease, polyps, and especially inflammatory bowel disease, polyps, and colorectal cancer, is crucial.colorectal cancer, is crucial.
Medication use must be detailed as many drugs Medication use must be detailed as many drugs cause gastrointestinal symptoms. cause gastrointestinal symptoms.
Before recommending operative intervention, the Before recommending operative intervention, the adequacy of medical treatment must be ascertained. adequacy of medical treatment must be ascertained.
In addition to examining the abdomen, visual In addition to examining the abdomen, visual inspection of the anus and perineum and careful inspection of the anus and perineum and careful digital rectal exam are essential.digital rectal exam are essential.
EndoscopyEndoscopy

Clinical EvaluationClinical Evaluation
EndoscopyEndoscopy
1.1.AnoscopyAnoscopy
The anoscope is a useful instrument for The anoscope is a useful instrument for examination of the anal canal. Anoscopes are examination of the anal canal. Anoscopes are made in a variety of sizes and measure made in a variety of sizes and measure approximately 8 cm in length. A larger approximately 8 cm in length. A larger anoscope provides better exposure for anal anoscope provides better exposure for anal procedures such as rubber band ligation or procedures such as rubber band ligation or sclerotherapy of hemorrhoids. sclerotherapy of hemorrhoids.
22. Proctoscopy. Proctoscopy

Clinical EvaluationClinical Evaluation
ImagingImaging
Plain X-Rays and Contrast StudiesPlain X-Rays and Contrast Studies
Computed TomographyComputed Tomography
Virtual ColonoscopyVirtual Colonoscopy
Magnetic Resonance ImagingMagnetic Resonance Imaging
Positron Emission TomographyPositron Emission Tomography
AngiographyAngiography
Endorectal and Endoanal UltrasoundEndorectal and Endoanal Ultrasound

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
Anorectal physiologic testing uses a variety of Anorectal physiologic testing uses a variety of techniques to investigate the function of the techniques to investigate the function of the pelvic floor. These techniques are useful in the pelvic floor. These techniques are useful in the evaluation of patients with incontinence, evaluation of patients with incontinence, constipation, rectal prolapse, obstructed constipation, rectal prolapse, obstructed defecation, and other disorders of the pelvic defecation, and other disorders of the pelvic floorfloor

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
11. Manometry. Manometry
2. Neurophysiology2. Neurophysiology
3, Rectal Evacuation Studies3, Rectal Evacuation Studies

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
ManometryManometry
Anorectal manometry is performed by placing a Anorectal manometry is performed by placing a pressure-sensitive catheter in the lower rectum. pressure-sensitive catheter in the lower rectum. The catheter is then withdrawn through the anal The catheter is then withdrawn through the anal canal and pressures recorded.canal and pressures recorded.

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
ManometryManometry
A balloon attached to the tip of the catheter also A balloon attached to the tip of the catheter also can be used to test anorectal sensation.can be used to test anorectal sensation.
The The resting pressureresting pressure in the anal canal reflects the in the anal canal reflects the function of the internal anal sphincter (normal: function of the internal anal sphincter (normal: 40 to 80 mm Hg )40 to 80 mm Hg )

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
ManometryManometry
The The squeeze pressuresqueeze pressure, defined as the , defined as the maximum voluntary contraction pressure minus maximum voluntary contraction pressure minus the resting pressure, reflects function of the the resting pressure, reflects function of the external anal sphincter (normal: 40 to 80 mm external anal sphincter (normal: 40 to 80 mm Hg above resting pressure). Hg above resting pressure).

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
ManometryManometry
The The high-pressurezonehigh-pressurezone estimates the length of the estimates the length of the anal canal (normal: 2.0 to 4.0 cm).anal canal (normal: 2.0 to 4.0 cm).
The The rectoanal inhibitory reflexrectoanal inhibitory reflex can be detected by can be detected by inflating a balloon in the distal rectum; absence of inflating a balloon in the distal rectum; absence of this reflex is characteristic of this reflex is characteristic of Hirschsprung's Hirschsprung's diseasedisease

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
NeurophysiologyNeurophysiology
Neurophysiologic testing assesses function of the Neurophysiologic testing assesses function of the pudendal nerves and recruitment of pudendal nerves and recruitment of puborectalis muscle fibers. Pudendal nerve puborectalis muscle fibers. Pudendal nerve terminal motor latency measures the speed of terminal motor latency measures the speed of transmission of a nerve impulse through the transmission of a nerve impulse through the distal pudendal nerve fibers (normal: 1.8 to 2.2 distal pudendal nerve fibers (normal: 1.8 to 2.2 msec); msec);

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
NeurophysiologyNeurophysiology
Needle EMG has been used to map both the Needle EMG has been used to map both the pudendal nerves and the anatomy of the pudendal nerves and the anatomy of the internal and external sphincters. However, this internal and external sphincters. However, this examination is painful and poorly tolerated by examination is painful and poorly tolerated by most patients. most patients.
Needle EMG has largely been replaced by Needle EMG has largely been replaced by pudendal nerve motor-latency testingpudendal nerve motor-latency testing to assess to assess pudendal nerve function and pudendal nerve function and endoanal endoanal ultrasound to map the sphincters.ultrasound to map the sphincters.

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
Rectal Evacuation StudiesRectal Evacuation Studies
Rectal evacuation studies include the balloon Rectal evacuation studies include the balloon expulsion test and video defecography. Balloon expulsion test and video defecography. Balloon expulsion assesses a patient's ability to expel expulsion assesses a patient's ability to expel an intrarectal balloon. Video defecography an intrarectal balloon. Video defecography provides a more detailed assessment of provides a more detailed assessment of defecation. In this test, barium paste is placed defecation. In this test, barium paste is placed in the rectum and defecation is then recorded in the rectum and defecation is then recorded fluoroscopically. fluoroscopically.

Clinical EvaluationClinical Evaluation
Physiologic and Pelvic Floor InvestigationsPhysiologic and Pelvic Floor Investigations
Rectal Evacuation StudiesRectal Evacuation Studies
Defecography is used to differentiate Defecography is used to differentiate nonrelaxation of the puborectalis, obstructed nonrelaxation of the puborectalis, obstructed defecation, increased perineal descent, rectal defecation, increased perineal descent, rectal prolapse and intussusception, rectocele, and prolapse and intussusception, rectocele, and enterocele. The addition of vaginal contrast and enterocele. The addition of vaginal contrast and intraperitoneal contrast is useful in delineating intraperitoneal contrast is useful in delineating complex disorders of the pelvic floorcomplex disorders of the pelvic floor

laboratory studieslaboratory studies
1. Fecal Occult Blood Testing1. Fecal Occult Blood Testing
2. Stool Studies2. Stool Studies
3. Serum Tests3. Serum Tests
4. Tumor Markers4. Tumor Markers
5. Genetic Testing5. Genetic Testing

laboratory studieslaboratory studies
1. Fecal Occult Blood Testing1. Fecal Occult Blood Testing
Fecal occult blood testing (FOBT) is used as a Fecal occult blood testing (FOBT) is used as a screening test for colonic neoplasms in screening test for colonic neoplasms in asymptomatic, average-risk individuals. The asymptomatic, average-risk individuals. The efficacy of this test is based upon serial testing efficacy of this test is based upon serial testing because the majority of colorectal malignancies because the majority of colorectal malignancies will bleed intermittently. FOBT has been a will bleed intermittently. FOBT has been a nonspecific test for peroxidase contained in nonspecific test for peroxidase contained in hemoglobinhemoglobin

laboratory studieslaboratory studies
Stool StudiesStool Studies
Stool studies are often helpful in evaluating the Stool studies are often helpful in evaluating the etiology of diarrhea. Wet-mount examination etiology of diarrhea. Wet-mount examination reveals the presence of fecal leukocytes, which reveals the presence of fecal leukocytes, which may suggest colonic inflammation or the may suggest colonic inflammation or the presence of an invasive organism such as presence of an invasive organism such as invasive invasive E. coliE. coli or or ShigellaShigella. Stool cultures can . Stool cultures can detect pathogenic bacteria, ova, and parasites. detect pathogenic bacteria, ova, and parasites. C. difficileC. difficile colitis is diagnosed by detecting colitis is diagnosed by detecting bacterial toxin in the stool. Steatorrhea may be bacterial toxin in the stool. Steatorrhea may be diagnosed by adding Sudan red stain to a stool diagnosed by adding Sudan red stain to a stool sample.sample.

laboratory studieslaboratory studies
Serum TestsSerum Tests
Specific laboratory tests that should be Specific laboratory tests that should be performed will be dictated by the clinical performed will be dictated by the clinical scenario. Preoperative studies generally scenario. Preoperative studies generally include a complete blood count and electrolyte include a complete blood count and electrolyte panel. The addition of coagulation studies, liver panel. The addition of coagulation studies, liver function tests, and blood typing/cross-matching function tests, and blood typing/cross-matching depends upon the patient's medical condition depends upon the patient's medical condition and the proposed surgical procedureand the proposed surgical procedure

laboratory studieslaboratory studies
Tumor MarkersTumor Markers
Carcinoembryonic antigen (CEA) may be Carcinoembryonic antigen (CEA) may be elevated in 60 to 90% of patients with colorectal elevated in 60 to 90% of patients with colorectal cancer. Despite this, CEA is not an effective cancer. Despite this, CEA is not an effective screening tool for this malignancy. Many screening tool for this malignancy. Many practitioners follow serial CEA levels after practitioners follow serial CEA levels after curative-intent surgery in order to detect early curative-intent surgery in order to detect early recurrence of colorectal cancer. However, this recurrence of colorectal cancer. However, this tumor marker is nonspecific, and no survival tumor marker is nonspecific, and no survival benefit has yet been proven . benefit has yet been proven .

laboratory studieslaboratory studies
Tumor MarkersTumor Markers
Other biochemical markers (ornithine Other biochemical markers (ornithine decarboxylase, urokinase) have been decarboxylase, urokinase) have been proposed, but none has yet proven sensitive or proposed, but none has yet proven sensitive or specific for detection, staging, or predicting specific for detection, staging, or predicting prognosis of colorectal carcinoma prognosis of colorectal carcinoma

laboratory studieslaboratory studies
Genetic TestingGenetic Testing
Although familial colorectal cancer syndromes, Although familial colorectal cancer syndromes, such as familial adenomatous polyposis (FAP) such as familial adenomatous polyposis (FAP) and hereditary nonpolyposis colon cancer and hereditary nonpolyposis colon cancer (HNPCC) are rare, information about the (HNPCC) are rare, information about the specific genetic abnormalities underlying these specific genetic abnormalities underlying these disorders has led to significant interest in the disorders has led to significant interest in the role of genetic testing for colorectal cancer. role of genetic testing for colorectal cancer.

laboratory studieslaboratory studies
Genetic TestingGenetic Testing
Tests for mutations in the adenomatous Tests for mutations in the adenomatous polyposis coli (APC) gene responsible for FAP, polyposis coli (APC) gene responsible for FAP, and in mismatch repair genes responsible for and in mismatch repair genes responsible for HNPCC, are commercially available and HNPCC, are commercially available and extremely accurate in families with known extremely accurate in families with known mutations. Although many of these mutations mutations. Although many of these mutations are also present in sporadic colorectal cancer, are also present in sporadic colorectal cancer, the accuracy of genetic testing in average-risk the accuracy of genetic testing in average-risk individuals is considerably lower. individuals is considerably lower.

laboratory studieslaboratory studies
Genetic TestingGenetic Testing
These tests are not recommended for screening. These tests are not recommended for screening. Because of the potential psychosocial Because of the potential psychosocial implications of genetic testing, it is strongly implications of genetic testing, it is strongly recommended that professional genetic recommended that professional genetic counselors be involved in the care of any counselors be involved in the care of any patient considering these tests.patient considering these tests.

evaluation of common symptomsevaluation of common symptoms
Abdominal PainAbdominal Pain
Abdominal pain is a nonspecific symptom with Abdominal pain is a nonspecific symptom with a myriad of causes. Abdominal pain related to a myriad of causes. Abdominal pain related to the colon and rectum can result from the colon and rectum can result from obstruction (either inflammatory or neoplastic), obstruction (either inflammatory or neoplastic), inflammation, perforation, or ischemia. Plain x-inflammation, perforation, or ischemia. Plain x-rays and judicious use of contrast studies rays and judicious use of contrast studies and/or a CT scan can often confirm the and/or a CT scan can often confirm the diagnosis. Gentle retrograde contrast studies diagnosis. Gentle retrograde contrast studies (barium or Gastrografin enema) may be useful (barium or Gastrografin enema) may be useful in delineating the degree of colonic obstruction. in delineating the degree of colonic obstruction.

evaluation of common symptomsevaluation of common symptoms
Abdominal PainAbdominal Pain
Sigmoidoscopy and/or colonoscopy performed by Sigmoidoscopy and/or colonoscopy performed by an experienced endoscopist can assist in the an experienced endoscopist can assist in the diagnosis of ischemic colitis, infectious colitis, diagnosis of ischemic colitis, infectious colitis, and inflammatory bowel disease. and inflammatory bowel disease.
However, if perforation is suspected, colonoscopy However, if perforation is suspected, colonoscopy and/or sigmoidoscopy are generally and/or sigmoidoscopy are generally contraindicated. contraindicated.

evaluation of common symptomsevaluation of common symptoms
Abdominal PainAbdominal Pain
..
Evaluation and treatment of abdominal pain from Evaluation and treatment of abdominal pain from a colorectal source should follow the usual a colorectal source should follow the usual surgical principles of a thorough history and surgical principles of a thorough history and physical examination, appropriate diagnostic physical examination, appropriate diagnostic tests, resuscitation, and appropriately timed tests, resuscitation, and appropriately timed surgical intervention surgical intervention

evaluation of common symptomsevaluation of common symptoms
Pelvic PainPelvic Pain
Pelvic pain can originate from the distal colon Pelvic pain can originate from the distal colon and rectum or from adjacent urogenital and rectum or from adjacent urogenital structures. Tenesmus may result from proctitis structures. Tenesmus may result from proctitis or from a rectal or retrorectal mass. Cyclical or from a rectal or retrorectal mass. Cyclical pain associated with menses, especially when pain associated with menses, especially when accompanied by rectal bleeding, suggests a accompanied by rectal bleeding, suggests a diagnosis of endometriosis. Pelvic inflammatory diagnosis of endometriosis. Pelvic inflammatory disease also can produce significant abdominal disease also can produce significant abdominal and pelvic pain. and pelvic pain.

evaluation of common symptomsevaluation of common symptoms
Pelvic PainPelvic Pain
The extension of a peridiverticular abscess or The extension of a peridiverticular abscess or periappendiceal abscess into the pelvis may periappendiceal abscess into the pelvis may also cause pain. CT scan and/or MRI may be also cause pain. CT scan and/or MRI may be useful in differentiating these diseases. useful in differentiating these diseases. Proctoscopy (if tolerated) also can be helpful. Proctoscopy (if tolerated) also can be helpful. Occasionally, laparoscopy will yield a Occasionally, laparoscopy will yield a diagnosis.diagnosis.

evaluation of common symptomsevaluation of common symptoms
Anorectal PainAnorectal Pain
Anorectal pain is most often secondary to an Anorectal pain is most often secondary to an anal fissure or perirectal abscess and/or fistula. anal fissure or perirectal abscess and/or fistula. Physical examination can usually differentiate Physical examination can usually differentiate these conditions. Other, less common causes these conditions. Other, less common causes of anorectal pain include anal canal neoplasms, of anorectal pain include anal canal neoplasms, perianal skin infection, and dermatologic perianal skin infection, and dermatologic conditions. Proctalgia fugax results from levator conditions. Proctalgia fugax results from levator spasm and may present without any other spasm and may present without any other anorectal findings. anorectal findings.

evaluation of common symptomsevaluation of common symptoms
Anorectal PainAnorectal Pain
Physical exam is critical in evaluating patients Physical exam is critical in evaluating patients with anorectal pain. If a patient is too tender to with anorectal pain. If a patient is too tender to examine in the office, an examination under examine in the office, an examination under anesthesia is necessary. MRI may be helpful in anesthesia is necessary. MRI may be helpful in select cases where the etiology of pain is select cases where the etiology of pain is elusive.elusive.

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal BleedingLower Gastrointestinal Bleeding
The first goal in evaluating and treating a patient The first goal in evaluating and treating a patient with gastrointestinal hemorrhage is adequate with gastrointestinal hemorrhage is adequate resuscitation.resuscitation.
The principles of ensuring a patent airway, The principles of ensuring a patent airway, supporting ventilation, and optimizing supporting ventilation, and optimizing hemodynamic parameters apply and hemodynamic parameters apply and coagulopathy and/or thrombocytopenia should coagulopathy and/or thrombocytopenia should be corrected. be corrected.

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal BleedingLower Gastrointestinal Bleeding
The second goal is to identify the source of The second goal is to identify the source of hemorrhage. Because the most common hemorrhage. Because the most common source of gastrointestinal hemorrhage is source of gastrointestinal hemorrhage is esophageal, gastric, or duodenal, nasogastric esophageal, gastric, or duodenal, nasogastric aspiration should always be performed; return aspiration should always be performed; return of bile suggests that the source of bleeding is of bile suggests that the source of bleeding is distal to the ligament of Treitz. If aspiration distal to the ligament of Treitz. If aspiration reveals blood or nonbile secretions, or if reveals blood or nonbile secretions, or if symptoms suggest an upper intestinal source, symptoms suggest an upper intestinal source, esophagogastroduodenoscopy is performed. esophagogastroduodenoscopy is performed.

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal BleedingLower Gastrointestinal Bleeding
Anoscopy and/or limited proctoscopy can Anoscopy and/or limited proctoscopy can identify hemorrhoidal bleeding.identify hemorrhoidal bleeding.
A technetium-99 (A technetium-99 (99m99mTc)-tagged red blood cell Tc)-tagged red blood cell (RBC) scan is extremely sensitive and is able to (RBC) scan is extremely sensitive and is able to detect as little as 0.1 mL/h of bleeding; detect as little as 0.1 mL/h of bleeding; however, localization is imprecise. however, localization is imprecise.
If the If the 99m99mTc-tagged RBC scan is positive, Tc-tagged RBC scan is positive, angiography can then be employed to localize angiography can then be employed to localize bleedingbleeding

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal BleedingLower Gastrointestinal Bleeding
Infusion of vasopressin or angioembolization may Infusion of vasopressin or angioembolization may be therapeutic. Alternatively, a catheter can be be therapeutic. Alternatively, a catheter can be left in the bleeding vessel to allow localization left in the bleeding vessel to allow localization at the time of laparotomy. If the patient is at the time of laparotomy. If the patient is hemodynamically stable, a rapid bowel hemodynamically stable, a rapid bowel preparation (over 4 to 6 hours) can be preparation (over 4 to 6 hours) can be performed to allow colonoscopy.performed to allow colonoscopy.

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal Bleeding.Lower Gastrointestinal Bleeding.
Colonoscopy may identify the cause of the Colonoscopy may identify the cause of the bleeding, and cautery or injection of bleeding, and cautery or injection of epinephrine into the bleeding site may be used epinephrine into the bleeding site may be used to control hemorrhage. Colectomy may be to control hemorrhage. Colectomy may be required if bleeding persists despite these required if bleeding persists despite these interventionsinterventions

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal Bleeding.Lower Gastrointestinal Bleeding.
Intraoperative colonoscopy and/or enteroscopy Intraoperative colonoscopy and/or enteroscopy may assist in localizing bleeding. If colectomy is may assist in localizing bleeding. If colectomy is required, a segmental resection is preferred if required, a segmental resection is preferred if the bleeding source can be localized. "Blind" the bleeding source can be localized. "Blind" subtotal colectomy may very rarely be required subtotal colectomy may very rarely be required in a patient who is hemodynamically unstable in a patient who is hemodynamically unstable with ongoing colonic hemorrhage of unknown with ongoing colonic hemorrhage of unknown source. It is crucial to irrigate rectum & examine source. It is crucial to irrigate rectum & examine the mucosa by proctoscopy to ensure source of the mucosa by proctoscopy to ensure source of bleeding is not distal to the resection margin bleeding is not distal to the resection margin

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal Bleeding.Lower Gastrointestinal Bleeding.
Intraoperative colonoscopy and/or enteroscopy Intraoperative colonoscopy and/or enteroscopy may assist in localizing bleeding. If colectomy is may assist in localizing bleeding. If colectomy is required, a segmental resection is preferred if required, a segmental resection is preferred if the bleeding source can be localized. "Blind" the bleeding source can be localized. "Blind" subtotal colectomy may very rarely be required subtotal colectomy may very rarely be required in a patient who is hemodynamically unstable in a patient who is hemodynamically unstable with ongoing colonic hemorrhage of unknown with ongoing colonic hemorrhage of unknown source. It is crucial to irrigate rectum & examine source. It is crucial to irrigate rectum & examine the mucosa by proctoscopy to ensure source of the mucosa by proctoscopy to ensure source of bleeding is not distal to the resection margin bleeding is not distal to the resection margin

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal Bleeding.Lower Gastrointestinal Bleeding.
Occult blood loss from the gastrointestinal tract Occult blood loss from the gastrointestinal tract may manifest as iron-deficiency anemia or may may manifest as iron-deficiency anemia or may be detected with fecal occult blood testing. be detected with fecal occult blood testing. Because colon neoplasms bleed intermittently Because colon neoplasms bleed intermittently and rarely present with rapid hemorrhage, the and rarely present with rapid hemorrhage, the presence of occult fecal blood should always presence of occult fecal blood should always prompt a colonoscopy. Unexplained iron-prompt a colonoscopy. Unexplained iron-deficiency anemia is also an indication for deficiency anemia is also an indication for colonoscopy.colonoscopy.

evaluation of common symptomsevaluation of common symptoms
Lower Gastrointestinal Bleeding.Lower Gastrointestinal Bleeding.
Hematochezia is commonly caused by Hematochezia is commonly caused by hemorrhoids or fissure. hemorrhoids or fissure.
Sharp, knife-like pain and bright-red rectal Sharp, knife-like pain and bright-red rectal bleeding with bowel movements suggest the bleeding with bowel movements suggest the diagnosis of fissure. diagnosis of fissure.

evaluation of common symptomsevaluation of common symptoms
Constipation and Obstructed DefecationConstipation and Obstructed Defecation
Constipation is an extremely common Constipation is an extremely common complaint, affecting more than 4 million people complaint, affecting more than 4 million people in the United States. Despite the prevalence of in the United States. Despite the prevalence of this problem, there is lack of agreement about this problem, there is lack of agreement about an appropriate definition of constipation.an appropriate definition of constipation.
Patients may describe infrequent bowel Patients may describe infrequent bowel movements, hard stools, or excessive straining. movements, hard stools, or excessive straining. A careful history of these symptoms often A careful history of these symptoms often clarifies the nature of the problem.clarifies the nature of the problem.

evaluation of common symptomsevaluation of common symptoms
Constipation and Obstructed DefecationConstipation and Obstructed Defecation
Constipation has a myriad of causes.Constipation has a myriad of causes.
1.Underlying metabolic 1.Underlying metabolic
2.Pharmacologic2.Pharmacologic
3.Endocrine 3.Endocrine
4.Psychologic4.Psychologic
5.Neurologic causes often contribute to the 5.Neurologic causes often contribute to the problemproblem

evaluation of common symptomsevaluation of common symptoms
Constipation and Obstructed DefecationConstipation and Obstructed Defecation
A stricture or mass lesion should be excluded by A stricture or mass lesion should be excluded by colonoscopy or barium enema. After these colonoscopy or barium enema. After these causes have been excluded causes have been excluded
Evaluation focuses upon differentiating Evaluation focuses upon differentiating slow-slow-transit constipationtransit constipation from from outlet obstructionoutlet obstruction. . Transit studies, in which radiopaque markers Transit studies, in which radiopaque markers are swallowed and followed radiographically, are swallowed and followed radiographically, are useful for diagnosing slow-transit are useful for diagnosing slow-transit constipation. constipation.

evaluation of common symptomsevaluation of common symptoms
Constipation and Obstructed DefecationConstipation and Obstructed Defecation
Anorectal manometry and electromyography can Anorectal manometry and electromyography can detect nonrelaxation of the puborectalis, which detect nonrelaxation of the puborectalis, which contributes to outlet obstruction. The absence contributes to outlet obstruction. The absence of an anorectal inhibitory reflex suggests of an anorectal inhibitory reflex suggests Hirschsprung's disease and may prompt a Hirschsprung's disease and may prompt a rectal mucosal biopsy.rectal mucosal biopsy.
Defecography can identify rectal prolapse, Defecography can identify rectal prolapse, intussusception, rectocele, or enteroceleintussusception, rectocele, or enterocele

evaluation of common symptomsevaluation of common symptoms
Constipation and Obstructed DefecationConstipation and Obstructed Defecation
Medical management is the mainstay of Medical management is the mainstay of therapy for constipation and includes fiber, therapy for constipation and includes fiber, increased fluid intake, and laxatives. Outlet increased fluid intake, and laxatives. Outlet obstruction from nonrelaxation of the obstruction from nonrelaxation of the puborectalis often responds to biofeedback. 7 puborectalis often responds to biofeedback. 7 Surgery to correct rectocele and rectal prolapse Surgery to correct rectocele and rectal prolapse has a variable effect on symptoms of has a variable effect on symptoms of constipation, but can be successful in selected constipation, but can be successful in selected patients. patients.

evaluation of common symptomsevaluation of common symptoms
Constipation and Obstructed DefecationConstipation and Obstructed Defecation
Subtotal colectomy is considered only for Subtotal colectomy is considered only for patients with severe slow-transit constipation patients with severe slow-transit constipation (colonic inertia) refractory to maximal medical (colonic inertia) refractory to maximal medical interventions. While this operation almost interventions. While this operation almost always increases bowel movement frequency, always increases bowel movement frequency, complaints of diarrhea, incontinence, and complaints of diarrhea, incontinence, and abdominal pain are not infrequent, and patients abdominal pain are not infrequent, and patients should be carefully selected. should be carefully selected.

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel SyndromeDiarrhea and Irritable Bowel Syndrome
Diarrhea is also a common complaint and is Diarrhea is also a common complaint and is usually a self-limited symptom of infectious usually a self-limited symptom of infectious gastroenteritis. If diarrhea is chronic or is gastroenteritis. If diarrhea is chronic or is accompanied by bleeding or abdominal pain, accompanied by bleeding or abdominal pain, further investigation is warranted. further investigation is warranted.

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel Syndrome. Diarrhea and Irritable Bowel Syndrome.
Bloody diarrhea and pain are characteristic of Bloody diarrhea and pain are characteristic of colitis; etiology can be an infection:colitis; etiology can be an infection:
1.Invasive 1.Invasive E. ColiE. Coli
2. Shigella2. Shigella
3.Salmonella3.Salmonella
4. Campylobacter4. Campylobacter
5.Entamoeba histolytica5.Entamoeba histolytica
6.C. Difficile6.C. Difficile

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel Syndrome. Diarrhea and Irritable Bowel Syndrome.
Inflammatory bowel disease (ulcerative colitis or Inflammatory bowel disease (ulcerative colitis or Crohn's colitis), or ischemia.Crohn's colitis), or ischemia.
Stool wet-mount and culture can often diagnose Stool wet-mount and culture can often diagnose infection. infection.
Sigmoidoscopy or colonoscopy can be helpful in Sigmoidoscopy or colonoscopy can be helpful in diagnosing inflammatory bowel disease or diagnosing inflammatory bowel disease or ischemia. However, if the patient has ischemia. However, if the patient has abdominal tenderness, particularly with abdominal tenderness, particularly with peritoneal signs, or any other evidence of peritoneal signs, or any other evidence of perforation, endoscopy is contraindicated.perforation, endoscopy is contraindicated.

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel Syndrome. Diarrhea and Irritable Bowel Syndrome.
Rarely, carcinoid syndrome and islet cell tumors Rarely, carcinoid syndrome and islet cell tumors (vasoactive intestinal peptide-secreting tumor (vasoactive intestinal peptide-secreting tumor [VIPoma], somatostatinoma, gastrinoma) [VIPoma], somatostatinoma, gastrinoma) present with this symptom. present with this symptom.
Large villous lesions may cause secretory Large villous lesions may cause secretory diarrhea. diarrhea.
Collagenous colitis can cause diarrhea without Collagenous colitis can cause diarrhea without any obvious mucosal abnormality. any obvious mucosal abnormality.

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel Syndrome. Diarrhea and Irritable Bowel Syndrome.
Along with stool cultures, tests for malabsorption, Along with stool cultures, tests for malabsorption, and metabolic investigations, colonoscopy can and metabolic investigations, colonoscopy can be invaluable in differentiating these causes. be invaluable in differentiating these causes. Biopsies should be taken even if the colonic Biopsies should be taken even if the colonic mucosa appears grossly normalmucosa appears grossly normal

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel Syndrome. Diarrhea and Irritable Bowel Syndrome.
Irritable bowel syndromeIrritable bowel syndrome is a particularly is a particularly troubling constellation of symptoms consisting troubling constellation of symptoms consisting
1. Crampy abdominal pain1. Crampy abdominal pain
2. Bloating2. Bloating
3. Constipation3. Constipation
4. Urgent diarrhea. 4. Urgent diarrhea.

evaluation of common symptomsevaluation of common symptoms
Diarrhea and Irritable Bowel Syndrome. Diarrhea and Irritable Bowel Syndrome.
Irritable bowel syndromeIrritable bowel syndrome
Work-up reveals no underlying anatomic or Work-up reveals no underlying anatomic or physiologic abnormality. physiologic abnormality.
Once other disorders have been excluded, Once other disorders have been excluded, dietary restrictions and avoidance of caffeine, dietary restrictions and avoidance of caffeine, alcohol, and tobacco may help to alleviate alcohol, and tobacco may help to alleviate symptoms.symptoms.
Antispasmodics and bulking agents may be Antispasmodics and bulking agents may be helpfulhelpful

evaluation of common symptomsevaluation of common symptoms
IncontinenceIncontinence
The incidence of fecal incontinence has been The incidence of fecal incontinence has been estimated to occur in 10 to 13 individuals per estimated to occur in 10 to 13 individuals per 1000 people older than age 65 years. 1000 people older than age 65 years. Incontinence ranges in severity from Incontinence ranges in severity from
occasional leakage of gas and liquid stool tooccasional leakage of gas and liquid stool to
daily loss of solid stool. daily loss of solid stool.

evaluation of common symptomsevaluation of common symptoms
IncontinenceIncontinence
The underlying cause of incontinence is often The underlying cause of incontinence is often multifactorial and diarrhea is often contributory. multifactorial and diarrhea is often contributory. In general, causes of incontinence can be In general, causes of incontinence can be classifiedclassified
as as neurogenicneurogenic
anatomicanatomic. .
Neurogenic causes include diseases of the Neurogenic causes include diseases of the central nervous system and spinal cord along central nervous system and spinal cord along with pudendal nerve injury.with pudendal nerve injury.

evaluation of common symptomsevaluation of common symptoms
Incontinence.Incontinence.
Anatomic causes include Anatomic causes include
1. congenital abnormalities1. congenital abnormalities
2. procidentia 2. procidentia
overflow incontinence secondary to impaction overflow incontinence secondary to impaction or neoplasm, or neoplasm,

evaluation of common symptomsevaluation of common symptoms
Incontinence.Incontinence.
trauma. trauma.
The most common traumatic cause of The most common traumatic cause of incontinence is injury to the anal sphincter incontinence is injury to the anal sphincter during vaginal delivery.during vaginal delivery.
Other causes includeOther causes include
Anorectal surgery, Anorectal surgery,
Impalement, Impalement,
Pelvic fracture.Pelvic fracture.

evaluation of common symptomsevaluation of common symptoms
After a thorough medical evaluation to detect After a thorough medical evaluation to detect underlying conditions that might contribute to underlying conditions that might contribute to incontinence, evaluation focuses on: incontinence, evaluation focuses on:
1. Assessment of anal sphincter & pudendal 1. Assessment of anal sphincter & pudendal nerves. nerves. Pudendal nerve terminal motor latency Pudendal nerve terminal motor latency testing mtesting may detect neuropathy. ay detect neuropathy. Anal manometry Anal manometry can detect low resting and squeeze pressures. can detect low resting and squeeze pressures. DefecographDefecography can detect rectal prolapse. y can detect rectal prolapse. Endoanal ultrasound Endoanal ultrasound is invaluable in diagnosing is invaluable in diagnosing sphincter defects sphincter defects

evaluation of common symptomsevaluation of common symptoms
Therapy depends upon underlying abnormality. Therapy depends upon underlying abnormality.
1.Diarrhea should be treated medically. Even in 1.Diarrhea should be treated medically. Even in the absence of frank diarrhea the absence of frank diarrhea
2.Addition of dietary fiber may improve 2.Addition of dietary fiber may improve continence.continence.
3.Some patients may respond to biofeedback. 3.Some patients may respond to biofeedback.

evaluation of common symptomsevaluation of common symptoms
Therapy depends upon underlying abnormality. Therapy depends upon underlying abnormality.
4.Many patients with a sphincter defect are candidates 4.Many patients with a sphincter defect are candidates for an overlapping sphincteroplasty. for an overlapping sphincteroplasty.
5.Innovative technologies such as sacral nerve 5.Innovative technologies such as sacral nerve stimulation or artificial bowel sphincter are proving stimulation or artificial bowel sphincter are proving useful in patients who fail other interventionsuseful in patients who fail other interventions

General Surgical ConsiderationsGeneral Surgical Considerations
Anterior ResectionAnterior Resection
High Anterior ResectionHigh Anterior Resection
Low Anterior ResectionLow Anterior Resection
Extended Low Anterior ResectionExtended Low Anterior Resection
Hartmann's Procedure and Mucus FistulaHartmann's Procedure and Mucus Fistula
Abdominoperineal ResectionAbdominoperineal Resection

POLYPSPOLYPS
Neoplastic-Tubular, villous, tubulovillousNeoplastic-Tubular, villous, tubulovillous
Hamartomatous- juvenile, Peutz-JeghersHamartomatous- juvenile, Peutz-Jeghers
Hyperlastic - <5mm- >2cmHyperlastic - <5mm- >2cm
Inflammatory- pseudopolypInflammatory- pseudopolyp
Polyps less than 1 cm - Polyps less than 1 cm - 1-10%1-10%
1 to 2 cm – 1 to 2 cm – 7 -10%7 -10%
2 cm – 2 cm – 35 -50%35 -50%

RECTAL POLYPS
SESSILE PEDUNCULATED

CASE: MULTIPLE COLORECTAL POLYPS
CLINICAL PRESENTATION
BARIUM ENEMA

CASE: MULTIPLE COLORECTAL POLYPS
LOCATION OF COLORECTAL POLYPS

Familial polyposis of the colon is most oftenFamilial polyposis of the colon is most often
associated with which of the following associated with which of the following
conditionsconditions
A. Carcinoma of the pancreasA. Carcinoma of the pancreas
B. Carcinoma of the colonB. Carcinoma of the colon
C. Granulomatous disease of the colonC. Granulomatous disease of the colon
D. Pneumatosis cystoides intestinalesD. Pneumatosis cystoides intestinales
E. Sigmoid volvulusE. Sigmoid volvulus

CASE: POST- SURGICAL RESECTION

INFLAMMATORY BOWEL DISEASEINFLAMMATORY BOWEL DISEASE
ULCERATIVE COLITISULCERATIVE COLITIS
Rare in FilipinosRare in Filipinos
Common in caucasians esp. in JewsCommon in caucasians esp. in Jews
Non-specific, idiopathic mucosal Non-specific, idiopathic mucosal inflammation of the colon and the inflammation of the colon and the rectumrectum

INFLAMMATORY BOWEL DISEASEINFLAMMATORY BOWEL DISEASE
ULCERATIVE COLITISULCERATIVE COLITIS
Usually begins at the rectum moving Usually begins at the rectum moving proximally by direct extension (mucosa proximally by direct extension (mucosa and submucosa)and submucosa)
inflammation stops at the ileocolic inflammation stops at the ileocolic junctionjunction
Bloody mucoid diarrheaBloody mucoid diarrhea, abdominal pain, , abdominal pain, tenesmus, fevertenesmus, fever

INFLAMMATORY BOWEL DISEASEINFLAMMATORY BOWEL DISEASE
ULCERATIVE COLITISULCERATIVE COLITIS Treatment:Treatment: Sulfasalazine -4g/day relapse rate 9%/yr.Sulfasalazine -4g/day relapse rate 9%/yr. Rowasa- topical enema of 5-ASA.Rowasa- topical enema of 5-ASA. steroids , azathioprine, cyclosporine, steroids , azathioprine, cyclosporine,
6-mercaptopurine, tacrolimus.6-mercaptopurine, tacrolimus. Total abdominal colectomy with end Total abdominal colectomy with end
ileostomy.ileostomy.

INFLAMMATORY BOWEL DISEASEINFLAMMATORY BOWEL DISEASE
Crohn’s diseaseCrohn’s disease Nonspecific, transmural inflammationNonspecific, transmural inflammation- exacerbation/remissionexacerbation/remission- Mouth to anus, Mouth to anus, bloody diarrheabloody diarrhea- Extraintestinal manifestationExtraintestinal manifestation- Skip lesion , rectal sparing(40%)Skip lesion , rectal sparing(40%)- Terminal ileum and cecum (41%), SI(35%)Terminal ileum and cecum (41%), SI(35%)- Fistula,abscess,obstruction,strictureFistula,abscess,obstruction,stricture

ANORECTAL DISEASESANORECTAL DISEASES
HemorrhoidsHemorrhoids
Ischiorectal AbscessIschiorectal Abscess
Fistula in anoFistula in ano
Fissure in anoFissure in ano
WartsWarts
Fournier’s gangreneFournier’s gangrene
Foreign BodyForeign Body


Right Right AnteriorAnterior
Right Right PosteriorPosterior
Left LateralLeft Lateral3 MAJOR 3 MAJOR PILESPILES

HEMORRHOIDAL DISEASEHEMORRHOIDAL DISEASE
A
P
LRPrimary Locations
3-7-11 o’clock positons
(Left Lateral, Right Anterior and Right Posterior)

HEMORRHOIDAL DISEASEHEMORRHOIDAL DISEASE
Submucosal cushion contains venules, Submucosal cushion contains venules, arterioles, smooth muscle fibers.arterioles, smooth muscle fibers.Part of continence mechanism.Part of continence mechanism.Excessive straing, increase abdominal Excessive straing, increase abdominal pressure, hard stools.pressure, hard stools.Bleeding, thrombosis, prolapse.Bleeding, thrombosis, prolapse.External hemorrhoids distal to dentate lineExternal hemorrhoids distal to dentate lineInternal hemorrhoids proximal to dentate lineInternal hemorrhoids proximal to dentate line

HEMORRHOIDAL DISEASEHEMORRHOIDAL DISEASE
Grading :Grading :1.1. First degree – bulge into anal First degree – bulge into anal
canal ,prolapse beyond dentate linecanal ,prolapse beyond dentate line2.2. Second degree- prolapse through anus, Second degree- prolapse through anus,
reduce spontaneouslyreduce spontaneously3.3. Third degree- require manual reductionThird degree- require manual reduction4.4. Fourth degree- cannot be reduced, Fourth degree- cannot be reduced,
prone to strangulationprone to strangulation

Retrograde View from Colonoscopy
Hemorrhoids Hemorrhoids

Hemorrhoids: ManagementHemorrhoids: Management
MedicalMedical
DietDiet
Sitz BathSitz Bath
SuppositoriesSuppositories
SurgicalSurgical
Milligan MorganMilligan Morgan
Rubber Band Rubber Band LigationLigation
Harmonic ScalpelHarmonic Scalpel

Hemorrhoidectomy
Rubber Band Ligation
Harmonic Scalpel

Hemorrhoidectomy
Stapler Technique Ferguson or Excision

Anorectal Abscess and FAnorectal Abscess and Fiistulastula
What is an anal fistula?What is an anal fistula?
An abnormal communication between An abnormal communication between anal canal &skinanal canal &skin
What is the assoc. bet. Abscess/Fistula?What is the assoc. bet. Abscess/Fistula?
Approx. 50% of abscess occur Approx. 50% of abscess occur secondary to anal fistula. Abscess is the secondary to anal fistula. Abscess is the acute signacute sign..

Anorectal Abscess and FAnorectal Abscess and Fiistulastula
What is the P/E in anorectal abscess?What is the P/E in anorectal abscess?
Inflamed and tender perianal swellingInflamed and tender perianal swelling
Treatment for anorectal abscess/fistula?Treatment for anorectal abscess/fistula?
I & D “asap” for abscess.I & D “asap” for abscess.
Elective surgery for fistula.Elective surgery for fistula.

Salmon Goodsalls rule: Anterior - straight tractsPosterior- curved tracts
Exception: > 3cm curved
Fistula in Ano

Fistula in Ano

COMPLICATED FISTULA IN ANO

Anal FissureAnal Fissure
Anal fissure Anal fissure
Linear ulcer (anal canal) dentate to anusLinear ulcer (anal canal) dentate to anus
Symptoms of anal fissure Symptoms of anal fissure
Bleeding / anal pain during / after BMBleeding / anal pain during / after BM
Physical findings Physical findings
Split in anal canal, posterior midline,Split in anal canal, posterior midline,
sentinel pile, DRE extremely painfulsentinel pile, DRE extremely painful

Fissure in AnoFissure in Ano

Anal Anal FissureFissure
Treatment of acute anal fissure Treatment of acute anal fissure
High fiber diet, wheat bran, steroid High fiber diet, wheat bran, steroid creamcream
Treatment of chronic anal fissure Treatment of chronic anal fissure
Lateral internal sphincterotomyLateral internal sphincterotomy

Incidence of Cancer-PhilippinesIncidence of Cancer-Philippines
MaleMale
1.1. LungsLungs
2.2. LiverLiver
3.3. Colon/RectumColon/Rectum
4.4. StomachStomach
5. Prostate5. Prostate
FemaleFemale
1.1. BreastBreast
2.2. Cervix /UterusCervix /Uterus
3.3. Colon/ RectumColon/ Rectum
4.4. LungsLungs
5.5. ThyroidThyroid
6.6. OvaryOvary
7.7. LiverLiver

Colorectal CarcinomaColorectal Carcinoma
Colon CancerColon Cancer
3rd most common type /Filipino Male3rd most common type /Filipino Male
(11.5 per 100,000) (11.5 per 100,000)
Male : female ratio = 1.21Male : female ratio = 1.21
Incidence in the Philippines is Incidence in the Philippines is lower thanlower than those those elsewhere with the exception of Thailandelsewhere with the exception of Thailand
Incidence among Incidence among Filipino migrantsFilipino migrants to the USA is to the USA is higherhigher than than those observed in the Philippines those observed in the Philippines

Colorectal CarcinomaColorectal Carcinoma
Colon Cancer- Colon Cancer- GlobalGlobal
Highest among western countriesHighest among western countries
15% of all malignancies15% of all malignancies
Age related- 7Age related- 7thth decade; <40y/o (5%) decade; <40y/o (5%)
Rectum(30%) Rectum(30%) sigmoid(28%),cecum(13%),transverse sigmoid(28%),cecum(13%),transverse (11%),ascending/descending(9%).(11%),ascending/descending(9%).
Calcium supplement- (RTC) protective.Calcium supplement- (RTC) protective.

RISK FACTORSRISK FACTORS
Familial Adenomatous polyposisFamilial Adenomatous polyposis
Inflammatory bowel diseaseInflammatory bowel disease
Familial Cancer SyndromesFamilial Cancer Syndromes
Family HistoryFamily History
Adenomatous polypsAdenomatous polyps
DietDiet
Colorectal CarcinomaColorectal Carcinoma

Distribution of Cancer : Left side total = 81 %

narrowing

Modified Dukes’ ClassificationModified Dukes’ Classification
Stage A- CA confined to wall of bowelStage A- CA confined to wall of bowel
Stage B- CA spread to pericolonic tissuesStage B- CA spread to pericolonic tissues
Stage C- Mets. present in lymph nodesStage C- Mets. present in lymph nodes
Stage D- Omental implant; peritoneal Stage D- Omental implant; peritoneal seeding; metastasis beyond the confinesseeding; metastasis beyond the confines
of surgical resectionof surgical resection

Colorectal CancerColorectal CancerDukes' Classification / Survival(5 years)Dukes' Classification / Survival(5 years)
Dukes’ A 83 %Dukes’ A 83 %
B 57%B 57%
C 31 %C 31 %
D 0%D 0%

Survival By TNMSurvival By TNM
Stage I T1-2NOMO,75-90%Stage I T1-2NOMO,75-90%
Stage II T3-4NOMO,54-65%Stage II T3-4NOMO,54-65%
Stage III anyTN1-3MO <50 Stage III anyTN1-3MO <50
Stage IV 0-5% Stage IV 0-5%

Colorectal Cancer-ScreeningColorectal Cancer-Screening
FOBTFOBT - low specificity, low sensitivity- low specificity, low sensitivity - test repeated annually >50y/o- test repeated annually >50y/o
Flexible sigmoidoscopeFlexible sigmoidoscope - repeat every 5 years,safe.- repeat every 5 years,safe.
DCBEDCBE - sensitivity 50%-80%(<1cm polyps) , - sensitivity 50%-80%(<1cm polyps) ,
70-90%(>1cm); 55-85% Duke’s A & B. 70-90%(>1cm); 55-85% Duke’s A & B.ColonoscopyColonoscopy
- cecum visualized in 98.6%- cecum visualized in 98.6%

Colorectal Cancer-ScreeningColorectal Cancer-Screening
Guidelines Common to Most Guidelines Common to Most OrganizationsOrganizations::
50 years or more50 years or more
- Annual FOBT- Annual FOBT
- Flexible Sigmoidoscopy - Flexible Sigmoidoscopy
- DCBE q 6 years- DCBE q 6 years

Colorectal Cancer-ScreeningColorectal Cancer-Screening
Guidelines Common to Most Guidelines Common to Most OrganizationsOrganizations::
11stst degree relative w/ cancer/adenoma degree relative w/ cancer/adenoma
- Flex Sig ,DCBE or colonoscopy q 5 - Flex Sig ,DCBE or colonoscopy q 5 years at 50 years oldyears at 50 years old
- relative Dx < 55 y/o, colonoscopy done at - relative Dx < 55 y/o, colonoscopy done at 5050

Proctosigmoidoscopy

ColonoscopyColonoscopy

Screening for HNPCC* and FAP*Screening for HNPCC* and FAP* Genetic consult Genetic consult Annual colonoscopy from age 25Annual colonoscopy from age 25
* * Hereditary Non Polyposis Cancer/ColonHereditary Non Polyposis Cancer/Colon
(Lynch Syndrome I - 5 to 10 %)(Lynch Syndrome I - 5 to 10 %)
* Familial Adenomatous Polyposis* Familial Adenomatous Polyposis
Colorectal Carcinoma / ScreeningColorectal Carcinoma / Screening


Synchronous and Synchronous and Metachronous CAMetachronous CA
Synchronous CarcinomaSynchronous Carcinoma - two or more - two or more sites of cancer .sites of cancer .
Metachronous CarcinomaMetachronous Carcinoma - another - another cancer found two or more years aftercancer found two or more years after

Colorectal Colorectal CA-ClinicalCA-Clinical PresentationPresentation
Rectal bleedingRectal bleeding
Change/bowel habits Change/bowel habits
Tenesmus / fatigueTenesmus / fatigue

Colorectal CA Clinical PresentationColorectal CA Clinical Presentation
Persistent narrowing of stoolsPersistent narrowing of stools
Feeling / incomplete emptying Feeling / incomplete emptying after b.m.after b.m.
Unexplained weight loss/AnemiaUnexplained weight loss/Anemia

An elderly woman is admitted with weaknessAn elderly woman is admitted with weakness
anemia, anemia, weight loss, and a palpableweight loss, and a palpable abdominal abdominal
mass. She has colonic carcinoma. The mostmass. She has colonic carcinoma. The most
likely anatomic site would be:likely anatomic site would be:
A. RectumA. Rectum
B. Sigmoid colonB. Sigmoid colon
C. Left colonC. Left colon
D. Transverse colonD. Transverse colon
E. CecumE. Cecum

RECTALRECTAL CANCERCANCER
Rectal bleedingRectal bleeding( bright red)( bright red)
Altered bowel habits( incomplete Altered bowel habits( incomplete evacuation and unproductiveevacuation and unproductive urge to defecate)urge to defecate)
Rectal massRectal mass


TNM Staging of TNM Staging of Colorectal CancerColorectal Cancer
Definition of TNMDefinition of TNM
Primary Tumor (T)Primary Tumor (T) Tx Cannot be assessedTx Cannot be assessed Tis Carcinoma in situTis Carcinoma in situ T1 Tumor invades submucosaT1 Tumor invades submucosa T2 Tumor invades Muscularis propiaT2 Tumor invades Muscularis propia T3 thru muscularis propia to serosaT3 thru muscularis propia to serosa T4 directly invades other organsT4 directly invades other organs or perforatesor perforates

Regional Lymph Nodes(N)Regional Lymph Nodes(N)
NX cannot be assessedNX cannot be assessed
NO no lymph node metastasisNO no lymph node metastasis
N1 Metastasis in one to three N1 Metastasis in one to three
N2 Metastasis in four or moreN2 Metastasis in four or more
N3 any lymph node along namedN3 any lymph node along named
vascular trunkvascular trunk

Distant Metastasis ( M )Distant Metastasis ( M )
MX Cannot be assessedMX Cannot be assessed
MO No distant metastasisMO No distant metastasis
M1 Distant MetastasisM1 Distant Metastasis

Colorectal CancerColorectal Cancer
Stage Groupings (TNM)Stage Groupings (TNM)
Stage O T1sNOMO N/AStage O T1sNOMO N/A I T1NOMO Stage AI T1NOMO Stage A T2NOMO Stage B1T2NOMO Stage B1
II T3NOMO Stage B2II T3NOMO Stage B2 T4NOMO Stage B3T4NOMO Stage B3
III Any TN1MO Stage CIII Any TN1MO Stage C
IV Any T AnyNM1 StageIV Any T AnyNM1 Stage DD

Colorectal CancerColorectal Cancer
Stage II – High Risk GroupStage II – High Risk Group
- tumor fixation- tumor fixation
- tumor perforation- tumor perforation
- complete obstruction- complete obstruction
- poor histologic grades- poor histologic grades

CEA
• for prognostication
• not for diagnosis or screening
• rising titer postop indicates recurrence

Is there any role for surgery in patients with liver metastasis?
In highly selected patients with less than four metastasis and
no evidence of any other disease ( no local recurrence or further metastasis )

• 5 year survival is 25 to 30 % in patients who undergo a successful resection
• 100 % of patients die within 2 years with untreated liver metastasis

Colostomy

Squamous typeSquamous type
TreatmentTreatmentNigro ProtocolNigro Protocol
5FU chemotherapy5FU chemotherapyRadiotherapyRadiotherapy
ANAL CANCERANAL CANCER