Embed Size (px)
Citation preview

Recurrent Stress and Sport Injuries of the Lumbar Spine
Yigal Mirovsky
Assaf Harofeh Medical CenterZerifin, Israel

Function
-Force couple between the upperand lower extremities.
- Absorbs and transmit forces while - Absorbs and transmit forces while providing support and balance.-Transforms lateral bending into axial torque needed to rotate the pelvis.

Structures involved
“ Injuries to the spine affect the limbs and
injuries to the limbs affect the spine”injuries to the limbs affect the spine”

Structures involved
*Bones*Cartilage*Muscles & Ligaments*Nerves*Nerves

Patterns of Injury
*Acute injury*Repetitive activity

Patterns of Injury
Acute injury
-Fractures-Fractures-Tendon ruptures-Disc hernia

Repetitive Activity
- Contact sport- Non contact Sport

Repetitive Activity
*Ballet*Skating*Hockey*Football*Football*Weight Lifting*Rowing*Swimming

Epidemiology
“ 10% of sports injuries are related to the spine”spine”

Epidemiology
Low Back Pain
-82% in elite female rowers.(Howell 1984)
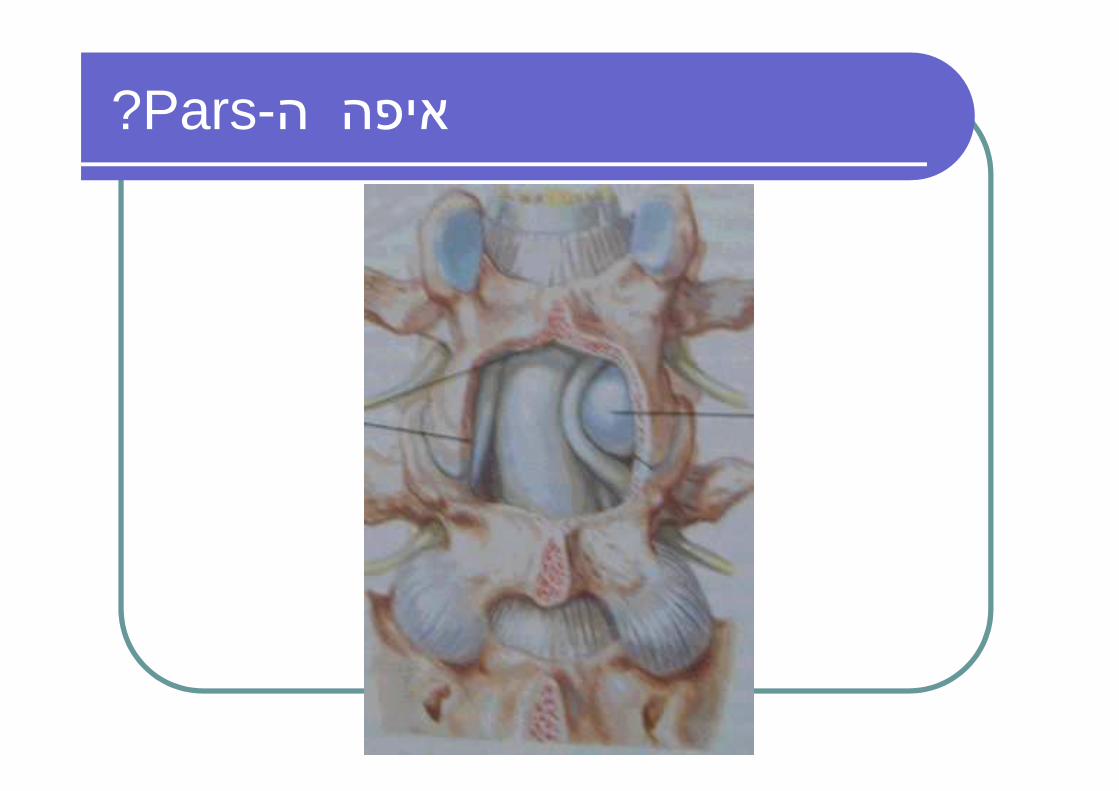
“Recurrent Hyper flexion motion”

Epidemiology
Low Back Pain
-30% in elite female competitive -30% in elite female competitive gymnasts.
(Jackson 1976)
“Recurrent Hyper flexion motion”

Biomechanics
Forces involved.
-Heperflexion-Heperflexion-Hyperextension-Compression- Torsion

Mechanism of injury
�Poor Technique�Poor Conditioning�Abnormal Anatomy�Abnormal Anatomy

Mechanism of injury
�Poor Technique
1. Warm up
“Stretching exercises.”
Amateurs are injured > Professionals-Limited accessibility-Limited facilities
Mechanism of injury
�Poor Technique
2. Lack of supervision
-Advancement to difficult exercises without proper attention to strength.
-Correcting seat height.-Personal adjacements of the facility.

Mechanism of injury
�Poor Conditioning
“Abnormal compensatory lordotic positioning (weight lifting and positioning (weight lifting and gymnastics)”
- Strengthening the abdominalmuscles
- Pelvic tilt and sit-up exercises

Mechanism of injury
�Anatomical Susceptibility
-Adolescent growth spurt.-Muscles.-Congenital anomalies.

Physical Activity
* LBP is more common in less physically active men.
Svensson et al 1988.Svensson et al 1988.
*Sports activity in general is not a risk factor.
Frymoyer 1983.

Physical Activity
937 former Athletes vs. 620 Referents(Ages 36-64).
Videman 1994

Physical Activity

Physical Activity

Physical Fitness
*Lesser risk for chronic LBP.
*More rapid recovery after LBP episode.

Physical Fitness
1652 Fire Fighters
- Fittest men had fewer injuries than the less fit.
- Less worker compensation claims following fitness program.
Cady et al 1985

Physical Fitness
Fitness training vs. control
*Same amount of injuries
*Quicker recovery in the trained subjects
Dehlin et al 1981

Physical Fitness
Future LBP is not influenced by
*Aerobic capacity Gyntelberg 1974, Troup et al 1987Gyntelberg 1974, Troup et al 1987
*Cardiovascular fitnessBattie’ 1989
Long term disability is associated with lower level of aerobic capacity

Physical Fitness
“Improved conditioning have a significant effect on the recovery rate after acute LBP” rate after acute LBP”
Nachemson 1989

Physical Exercises
739 recreational orienteers (mean age 33)
“The cumulative occurrence of LBP is “The cumulative occurrence of LBP is 47%”
Van Der Linden 1988

Body Response to Injury
�Spondylolytic Response.�Discogenic Response.�Discogenic Response.�Apophyseal Fractures.�Mechanical Low Back Pain.

Biomechanics
Tensile & Shear forces over the Pars articularies in normal Flexion and Extension:
“400-630 Newton over 0.75 cm2 at L5”“400-630 Newton over 0.75 cm2 at L5”

Biomechanics
Experimental Pars fracture in 14 years old model
“570 Newton's for 1536 cycles”“570 Newton's for 1536 cycles”

Biomechanics
POSTURE
“The amount of anteriorshear in the lumbar spineshear in the lumbar spineis related to the amount of postural lordosis”
( Weiss 1975)

Biomechanics
Pars interarticularies defect
- Recurrent hyperextension(Hall 1986 and Jackson 1974)(Hall 1986 and Jackson 1974)
- Recurrent hyperextension andhyperflexion(Letts 1986)

Spondylolytic Response
“Frequent in sports activities that involves recurrent involves recurrent hyperextension”

הסתכלות -בדיקה גופנית

טווחי תנועה

תשובה
* Phalen Dickson sign(Knee bent Hip flexed posture).
* Pelvic tilt* Protrusion of rib cage* Protrusion of rib cage* Sacral kyphosis & Hyperlor.* Loss of trunk height.* Flank creases* Hamstring tightness* Rare neurologic findings


אבחנה מבדלת
� Spondylolisthesis. � Juvenile Disc.� Infection.� Extraspinal Pathology:Extraspinal Pathology:
-Hips (Perthes, Slipped epiphysis)-Knees
� Tumor:-Intradural-Extradural


צילומים

MRI

דרגת הספונדילוליסטזיסMeyerding

Oblique

Bone scan
-

CT


Classification
Wiltse @ Macnab 1969
1. Dysplastic spondylolisthesis2. Isthmic spondylolisthesis2. Isthmic spondylolisthesis3. Degenerative spondylolisthesis4. Traumatic spondyloisthesis5. Pathologic spondylolisthesis
-Iatrogenic spondylolisthesis

חלוקת הספונדילוליסטזיס

Marcetti-Bartolozzi Classification -1997
� The term “Isthmic” should be avoided.� Pars defect may appear in Acquired and
Developmental conditions� High Dysplastic:
Usually L5-S1, Symptomatic in Adolescents, Wedged L5, Domed and Vertical Sacrum, true Lumbosacral Kyphosis, Progressive
� Low Dysplastic:Young Adults, Associated with Spina Bifida, Slippage Characterized by
translation without angulation or kyphosis



Level
-L/5-S/1: 82%-L/4-L/5: 11%-L/2-L/4: 1%-L/2-L/4: 1%-Other: 6%

Population
4% of the population
Blacks<WhitesWomen<MenWomen<Men
Eskimos 60%

Activity
-Young Sportsman: 11%-35%-Italian gymnastic team: 50%-Weight lifters: 36%-Weight lifters: 36%
Football, Judo,Throwers, Etc.


Risk Factor for Progression
�Clinical.Clinical.�Radiographic.

ClinicalRisk Factor for Progression
� Female.� Prepubescence.
Younger age at presentation.� Younger age at presentation.

RadiographicRisk Factor for Progression
�Dysplastic>Isthmic.�30%-50% of slippage.�Trapezoidal L5 (Lumbar Index).
Slip Angle
�Domed and Vertical Sacrum.�Radiographic Measurements:
-Slip angle>55º (Normal 0º-10º).
-Lumbosacral Kyphosis<100º.
Slip Angle
LumbosacralAngle

Radiographic Measurements
• Sacral Inclination 40°-60°• Lumbosacral Angle 20°-30°

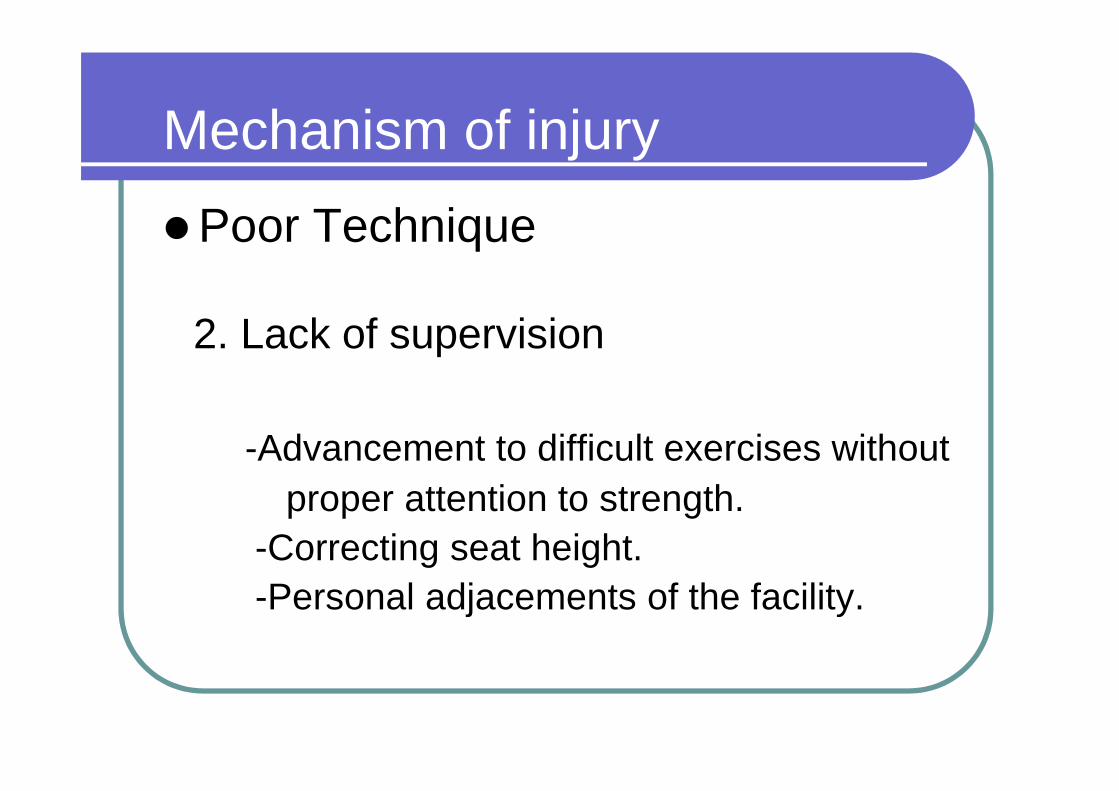
?Pars-איפה ה

Parsinterarticularis defect

Mechanism of Injury
Hyperlordosis
* Shear stresses over the pars are * Shear stresses over the pars are greatest in extension.
* Frequent in Scheuermann.* Frequent in sports that are associated
with hyperextension.

Mechanism of Injury
Repetitive Extension


Symptoms – Back Pain
* Disc Degeneration.* Facet Arthrosis.* Nerve root impingement.* Nerve root impingement.* Ligament Tension.
Wiltse 1977

Symptoms- Leg Pain
-Radicular Pain 14%
* Disc above.* Fibrocartilagenous mass.* Fibrocartilagenous mass.* Stretching of nerves.


Conservative
- Rest.- Bracing.- Medication.- Rehabilitation.- Rehabilitation.

WHO SHOULD BE FUSED
Intractable PainHigh Grade and younger than 10y.Isthmic L4-L5?Neurologic signs.


LEVELS
� M.R.I� Discography


APPROACH
� POSTERIOR.� ANETRIOR.� COMBINED.

No instrumentation
� Children.� Less than 50% of listhesis.� One level.

REDUCTION

REDUCTION

REDUCTION
� Cauda Equina.� Slip > 50%.� Major clinical deformity.
Anterior global sagital imbalance.� Anterior global sagital imbalance.� Following failed in situ fusion.� Surgeon experience.� patient acceptance of risk.

Reduction - Stages
� Laminectomy.� Screws insertion.� Post.Lat. Fusion.� Clamps & Rods.� Clamps & Rods.� Reduction device.� Reduction.

EXAMPLE NO. 1

EXAMPLE NO. 3

Spondylolytic Response
Variants:-Stress fracture of the Transverse process.-Stress fracture of the lamina.

Spondylolytic Response
Variants/Symptoms and Findings
-LBP radiating to the thighs.-Painful extension.-Tight Hamstrings.-Normal Neurology.

Spondylolytic Response
Variants/Treatment
-Brace if warm Tc.-Rest.-Stretching.-Laminectomy.

Discogenic Response.
“Frequent in truck drivers”

Discogenic Response.
Associated with increased risk for DD:
-Gymnastics-Weight lifting-Soccer

Discogenic Response.
Disc Degeneration

Discogenic Response.
Disc Degeneration/Symptoms and Findings
-Mechanical LBP.-Decreased motion.-No neurologic deficit.

Discogenic Response.
Disc Degeneration/Treatmenr
-Limited rest/NSAID/Limited Bracing.-Physiotherapy.-Physiotherapy.-Muscle Strengthening.-Surgery:
*Minimal (IDET, Ablasion,RF)*Fusion*Artificial Disc.

Apophyseal Fractures.
“Recurrent hyperflexion of the spine”
Scheuermann
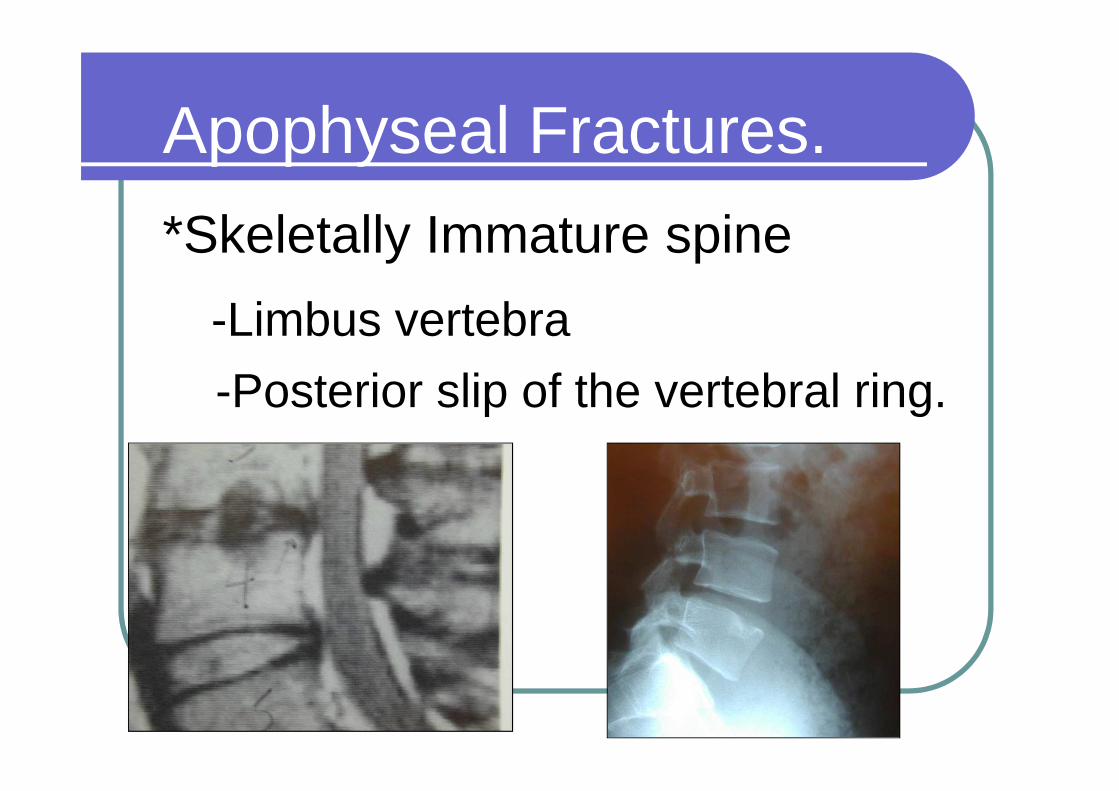
Apophyseal Fractures.
*Skeletally Immature spine
-Limbus vertebra
-Posterior slip of the vertebral ring.-Posterior slip of the vertebral ring.
Apophyseal Fractures.
*Gymnast.*Thoracolumbar Junction.*1-3 Levels.*1-3 Levels.

Apophyseal Fractures.
Predisposing Factor
“Tight Lumbar-Dorsal Fascia that “Tight Lumbar-Dorsal Fascia that resist foreword flexion of the Lumbar spine”



?מה הלאה



Apophyseal Fractures.
Treatment-Semi rigid Thermoplastic brace
(with 15 Degr. Of lumbar lordosis).(with 15 Degr. Of lumbar lordosis).
- For 23 Hours a day until bony
healing.


Apophyseal Fractures.
*Restitution of height over 9-12 months.months.
* Resume sport/dance in brace when become asymptomatic.




Mechanical Low Back Pain.
Cause
“Mechanical strain on ligaments and“Mechanical strain on ligaments andjoints”

Mechanical Low Back Pain.
Symptoms
“Non Specific back pain”“Non Specific back pain”

Mechanical Low Back Pain.
Physical Findings
-Increased Lumbar Lordosis.-Increased Lumbar Lordosis.-Hamstring Spasm.-Tight Lumbar Fascia.

Mechanical Low Back Pain.
Treatment- Stretching of the tight structures.- Strengthening the Abdominal
muscles, pelvic tilt and antilordotic muscles, pelvic tilt and antilordotic posture.
- O degree of anterior opening Brace for 3-4 months if exercises are not effective

Muscles and Ligaments
Muscles1. Rupture.2. Inflammation.2. Inflammation.

Muscles and LigamentsRupture-Weightlifters.-Discus Thrower-Football-Football-Handball-Basketball-Volleyball-Wreslers.-Boxers

Muscles and Ligaments
Rupture-Minor rupture.-Usually long back extensors.-Usually long back extensors.
Symptoms-Piercing pain on each motion.
-Local Tenderness

Muscles and Ligaments
Rupture/Treatment-Rest for 3-8 weeks.-Local heat/Analgetics/NSAID-Local heat/Analgetics/NSAID-Controlled muscle trainingafter few days.
Muscles and Ligaments
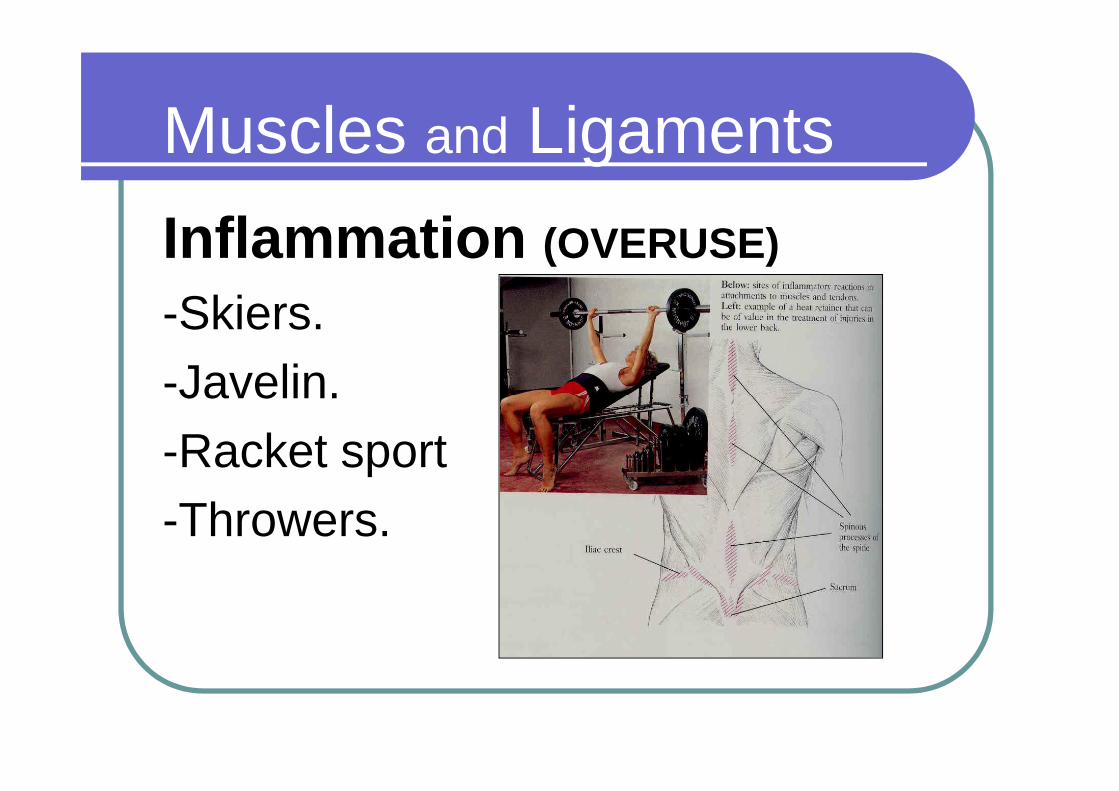
Inflammation (OVERUSE)
-Skiers.-Javelin.-Javelin.-Racket sport-Throwers.
Muscles and Ligaments
Inflammation /Symptoms
-Pain during exertion.-Aching after exertion.-Aching after exertion.-Tenderness over bony attachments.-Pain provocation with triggered
contraction.

Muscles and Ligaments
Inflammation /Treatment
-Limited rest.-Local heat.-Local heat.-Analgetics/NSAID/Creams-Local injection of steroids.

Take Home Message
� Sports activity in general is not a risk factor� Repetitive motion mainly in hyperextension is
the most Dangerous.� Be careful in risky population: Adolescent
growth spurt, Congenital anomalies.growth spurt, Congenital anomalies.� Poor Training Technique, Conditioning and
Fitness increase the risk for LBP.� Bone and Soft tissue injuries have a better
prognosis than Cartilage injuries.� Participation in sport in general is not
associated in general with increased risk to suffer in the future from LBP.