Embed Size (px)
Citation preview

REDESIGNING CARE FOR THOSE WHO NEED IT MOST…

Since 1993, CareMore and its founder, CareMore Medical Group, Inc., have been successful in delivering quality care to the Medicare population. CareMore’s only line of business is Medicare Advantage HMO, and its plans are uniquely designed for the frail elderly. We place a strong emphasis on early detection and identification of chronic conditions and co-morbidities and implement preventive and maintenance health care services that help to keep beneficiaries healthy, detect diseases at an early stage, and work to avoid preventable illnesses. CareMore joined the Anthem family of plans in 2011.
California Plans in Los Angeles, Orange, Riverside, San Bernardino, Santa Clara and Stanislaus Counties Offer Standard HMO plans, CSNPs, DSNPs and ISNPs
Nevada Plans in Clark County Offer Standard HMO plans, CSNPs and ISNPs
Arizona Plans in Maricopa and Pima Counties Offer Standard HMO plans, CSNPs and ISNPs
Virginia Plans in Richmond, VA Offer Standard HMO plans, CSNPs and ISNPs
A Brief History

OUR MISSION
Providing innovative and focused healthcare approaches to the complex process of aging.

WHY OUR MISSION
We are here to:
serve our members by prolonging active and independent life
serve caregivers and family by providing support, education, and access to services
protect precious financial resources of seniors and the Medicare Program through innovative methods of managing chronic disease, frailty, and end of life

CAREMORE
Our Members
44% diabetics
40% hypertensive
16% COPD, ESRD, asthma, kidney disease
66% Have co-morbidities
50% at or below $30k annual income
45% Hispanic
A Chronic Care Special Needs Plan

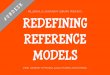
Healthcare Cost and Quality Problems are Concentrated….Not Widespread
Healthy Stable Sick Sickestmostly 1 + Chronic Illness mostly 3 + Chronic Illness
Progressive Illness2010 MedicareSpending Projection = $522 B46 Million BeneficiariesSpending Per Beneficiary = $11,347
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
$80,000
Ann
ual Cos
t/Be
nefi
ciar
y 23 Million Beneficiaries- Spending $1,130 each- Total Spending = 5%
($26 B)
16.1 Million Beneficiaries- Spending $6,150 each- Total Spending = 20%
($104 B)
7 Million Beneficiaries- Spending $55,000 each- Total Spending = 75%
($391 B)
AverageSpending
CHF, DM
85% of Beneficiaries = 25% Spending 15% of Beneficiaries = 75% Spending
ESRD, CANCER

The CareMore Model

Chronic Diseases are Generally Managed Poorly
Patients receive appropriate care only half of the time (EA McGlynn et al)
Diabetic complications could be cut 90% with best care and involved patients (Center for Disease Control and Prevention), yet
• Diabetes related admissions have risen from 3.5 to 6.5 million since 1993 (Dept. HHS)
• Low income diabetics are 80% more likely to be hospitalized (Dept. HHS)
Second heart attacks can be reduced 40% (J.R. Jowers)
More doctors involved in care decreases information exchange and leads to unnecessary hospitalizations (Wennberg/Dartmouth)
But...
• Patients with serious conditions see 11 different doctors
CareMore addresses these problems directly

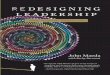
CareMore System Functions in Parallel with Community Physicians
Non-Frail Population
Primary Care Physicians
Extensivists
Member Services
Continuous Frailty Assessment Tools
Provider Relations
CareMore Care Centers
CareMoreExtensivist
CareMore Care Centers
Home Based Services
Specialists
Case Managers
Primary Care Physicians
Close monitoring of non-frail members to proactively identify at-risk members and aggressive management of chronic conditions to prolong the onset of frailty
Intensive management of frail and chronically ill members, identified through predictive models, data scans, PCP referrals or member self-identification
Frail & Chronically Ill Population

The Essentials of CareMore’s Model

CareMore Solution – New Model of Care

Conduct pre-operative exams
Manage patient hospitalization decision
Take control of entire inpatient stay, including specialist consultation, diagnostics, PCP communication, family communication
Create and manage discharge plan
Retain lead physician role during Skilled Nursing stay
Follow patients on an out-patient basis until acute episode or frailty resolves
Manage high-risk outpatient events, such as fall prevention programs, dementia evaluations, transplant evaluations, bariatric surgery evaluations
Create transition to palliative care and end-of-life teams as appropriate
Acute EpisodesTake “ownership” of patient at point
of admission Prepare patient and family for
dischargeDispatch all services necessary to
avoid readmission
Long Term Management“Own” patient for remainder of lifeDispatch home-based servicesFacilitate CCC and other
necessary visitsFacilitate transportation and other
social services
Chronic CareConduct annual health risk
assessments and create care plansMicro-manage chronic conditions and
lead interdisciplinary teams specific to a patient’s needs
Provide all wound care (diabetic, ulcerative, post-surgical)
Staff all home wireless monitoring systems
Available for 24/7 telephonic patient consultation
Frailty and Palliative CarePrimary care provider and case
manager for home-bound patientsAssume primary clinical role for
palliative care patients
Institutional/Custodial/Assisted Living ResidentsMake weekly visitsBecome first point of contact for
facilities and family for ALL care needs
Extensivists Nurse Practitioners Case Managers
CareMore’s Model Allows for Efficient Allocation of Clinical Resources

CAREMORE
Care Center
Community Focus
•Located in the heart of the neighborhood
Social Environment
•Designed for seniors •Resource for family and caregivers
•Frequent classes and activities
Clinical • Disease Management
• Foot Center• Healthy Start
• Pre- Op • Fall Prevention
• Wellness programs
A Newly Defined Medical and Social Home

Healthy Start – Initial EvaluationComplete medical evaluation for all new members
Goals Early identification of chronic diseases; referral to chronic
disease management programs One complete H&P Immediate referral to specialist if needed
Results 80% of members have appt within 30 days 42% referred to prevention or support program 23% referred to a chronic care program 18% diagnosed with depression (previously unknown) 3% diagnosed with Diabetes for the first time
Healthy Start – Initial EvaluationComplete medical evaluation for all new members
Goals High touch evaluation for high acuity patients Ensures at least one complete evaluation per year:
“second pair of eyes” when PCP/member engagement low
Results 70% of SNP members undergo in-person annual
assessment 100% Update to Care Plan and Medication Plan
Johns Hopkins Predictive Modeling Software
Healthy Journey –Ongoing EvaluationComplete medical evaluation for all new members
Goals High touch evaluation for high acuity patients Ensures at least one complete evaluation per year:
“second pair of eyes” when PCP/member engagement low
Results 70% of SNP members undergo in-person annual
assessment 100% Update to Care Plan and Medication Plan
Ascender Predictive Modeling Tool identifies targets based on claims data
Monthly run of claims, Rx, lab data, age correlated to identify 5% most at-risk members
72% plugged into appropriate chronic care of frailty program
CARSIdentifies sick patients through software
CareMore’s Model Allows for Predictive Modeling and Early Intervention

OUTCOMES
Diabetes Programo Members with A1c>9 on initial visit reduced to average of 7.08
when in programo 65% less amputations than Medicare FFS average (8.7
Medicare vs 2.96 Caremore)o Delayed Progression of Chronic Kidney Disease – Medicare
average of 6 years vs Caremore 24 years based on our predictive modeling
o ESRD program members have 37% less admissions and 64% fewer hospital days than Medicare average
Based on 2013 CareMore data and the most recent Medicare information

OUTCOMES
Chronic Heart Failure Program memberso 28% Fewer admissions than Medicare averageo 45% fewer hospital days than Medicare averageo 47% fewer readmissions than Medicare averageo 97% in program record daily weight through a wireless scale
Based on 2013 CareMore data and the most recent Medicare information

OUTCOMES
Chronic Lung Disease Program 48% fewer re-admissions than non-Program members 52% fewer admissions than Medicare average Members with COPD on Oxygen
o 33% fewer admissions than non-Program memberso 47% fewer hospital days than non-Program memberso 47% fewer readmissions than Medicare averageo 97% in program record daily weight through a wireless scale
Based on 2013 CareMore data and the most recent Medicare information

Payers & Providers

Drivers of Payer viability:
Membership/Growth
Patient Satisfaction
HCC Documentation & Coding
HEDIS measures
Specialist utilization
ER Visits
In Patient Utilization
Physician group Impact
Identify patients who benefit from Health Plan products and services
Short wait times; same day appointments; Timely communication-lab/test results; 5 STAR service
Comprehensive patient visit; documentation to the highest level of specificity
Comprehensive patient visit collecting HEDIS measures or referring for HEDIS-related visits
Reduced referrals to specialists where appropriate; utilization of preferred/aligned specialist providers
Short patient wait-times while in office; same day appointments, scheduled follow up visits, utilization of CareMore care center
All of the above
Alignment of Incentives

Primary Care Physicians Quality Bonuses
o HEDISo Patient Satisfaction
HCC documentation bonuseso Patient assessment formso Coding accuracy
Shared savings o Membership panel viewed as stand alone financial statement for Medical Group or
POD
PARTNERING

Specialists Bonuses for HEDIS capture
Retinopathy screenings
Shared savings on admission/re-admission reduction Cardiology COPD Nephrology
Episodic care management/Bundled payment Cardiology Orthopedics
PARTNERING

Hospitals Quality and Patient Satisfaction bonuses Shared savings on admission/re-admission reduction Episodic care management/Bundled payment
Cardiology Orthopedics
PARTNERING

IMPACT OF PATIENT SATISFACTION
GROWTHMEDICARE STARS
MEMBER COMPLAINTS MEMBERS LEAVING THE PLAN
HCC CAPTURECOMPLIANCE WITH CLINICAL PROGRAMS

Getting Care Quickly:• Setting appropriate and realistic expectations• Offering adequate and informative explanations• Acknowledging patient’s presence in the waiting room• Courteous and respectful staff
Getting Needed Care:• Submitting prior authorizations in a timely manner• Ensuring pharmacy receives prescriptions in a timely manner• Collaboration between PCPs and Specialists
Coordination of Care:• Using health plan resources for sharing clinical information• Set appropriate and realistic expectations regarding test results• Offering adequate and informative explanations
Member perception of all of these is KEY!
IMPROVING PATIENT SATISFACTION

HOW DO WE START?
Open the dialogue with payers Understand the quality and financial
issues Get the data Find partners with same goals