Embed Size (px)
Citation preview
Redesigning the Acute Coronary Syndrome
(NSTE- ACS) pathway at Morriston Cardiac
Centre - The case for change
4th
July 2012 – Dr D Smith & Dr S Dorman
Introduction ................................................................................................... 2
NSTE-ACS – Where are we now ? ................................................................... 2
NSTE-ACS - Proposed future model of care ................................................... 6
How do we get there ? ................................................................................... 8
The case for change ..................................................................................... 10
Immediate action required .......................................................................... 11
Conclusion ................................................................................................... 11

Introduction
In a recent report by the Office of National Statistics Ischaemic heart disease was recognised to be
the biggest cause of avoidable death in England & Wales as a whole. The report goes on to highlight
that in 2010 whilst the age-standardised avoidable mortality rate for England was 181.4 per 100,000
population, the rate of avoidable mortality in Wales was significant higher at 205.2. Contemporary
management of Acute Coronary Syndromes is a key component in reducing this avoidable mortality
and inequity of access to timely revascularisation in Wales remains a major factor accounting for
this. The situation is particulary acute in Mid & West Wales where patient’s will currently wait an
average of 7 days before they can be transferred to the Morriston Cardiac Centre to undergo
angiography and revascularisation.
Whilst the introduction of a 24/7 region wide Primary PCI service has transformed the care of
patient’s with ST elevation myocardial infarction( STEMI) , these only represent one third of patient’s
with Acute Coronary Syndromes. The Non ST elevation Acute Coronary Syndromes ( NSTE-ACS)
represent the majority of patient’s and the quality of care that this patient group currently receives
in Mid & West Wales is sub standard by all international comparisons. NSTE-ACS does not carry the
same high initial risk of adverse events (such as death, stroke or recurrent heart attack) as STEMI,
but contrary to popular belief, it does carry the same long term risk for adverse events if optimum
treatment is not carried out urgently within a 96 hour time frame from initial admission to hospital
(NICE recommended treatment time target). Therefore our current heart attack service is optimal
for only the minority of our heart attack patients, with the majority of patients with NSTE-ACS having
sub-optimal treatment with the greater likelihood of consequent adverse outcomes.
This paper makes the case for structural changes to our historic model of care for patients with
NSTE-ACS in order to transform the quality of care delivered to this patient group. As a by product it
is likely that significant savings will be realised at a health board level because of the inherent
inefficiencies of the current model of care.
NSTE-ACS – Where are we now ?
Current model of care in Mid & West Wales
Morriston Cardiac Centre serves a secondary and tertiary catchment population of just under 1
million people. As well as the local Swansea population this results in over 800 referrals from
surrounding hospital for patient’s with NSTE-ACS per year.
A patient will typically be risk stratified in the referring hospital using the GRACE scoring system and
then electronically referred after a minimum of 24 hours. The GRACE scoring system is the preferred
tool recommended by NICE & 1000 lives plus for patient risk stratification.
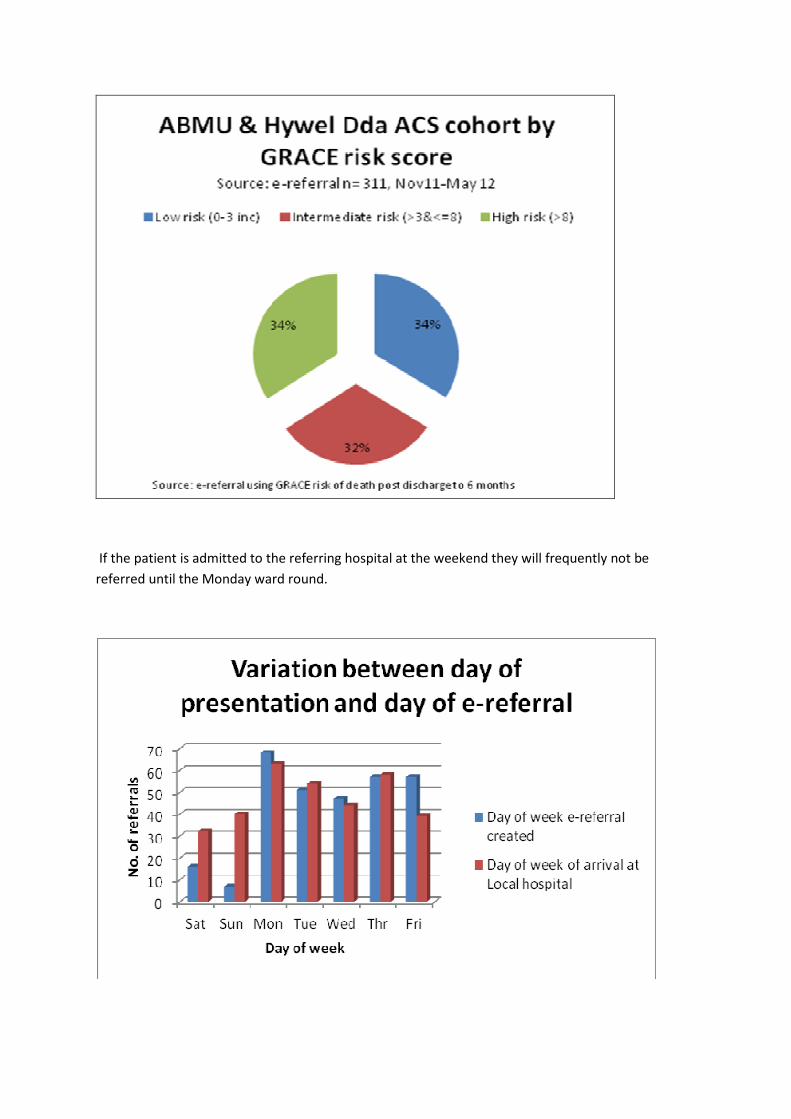
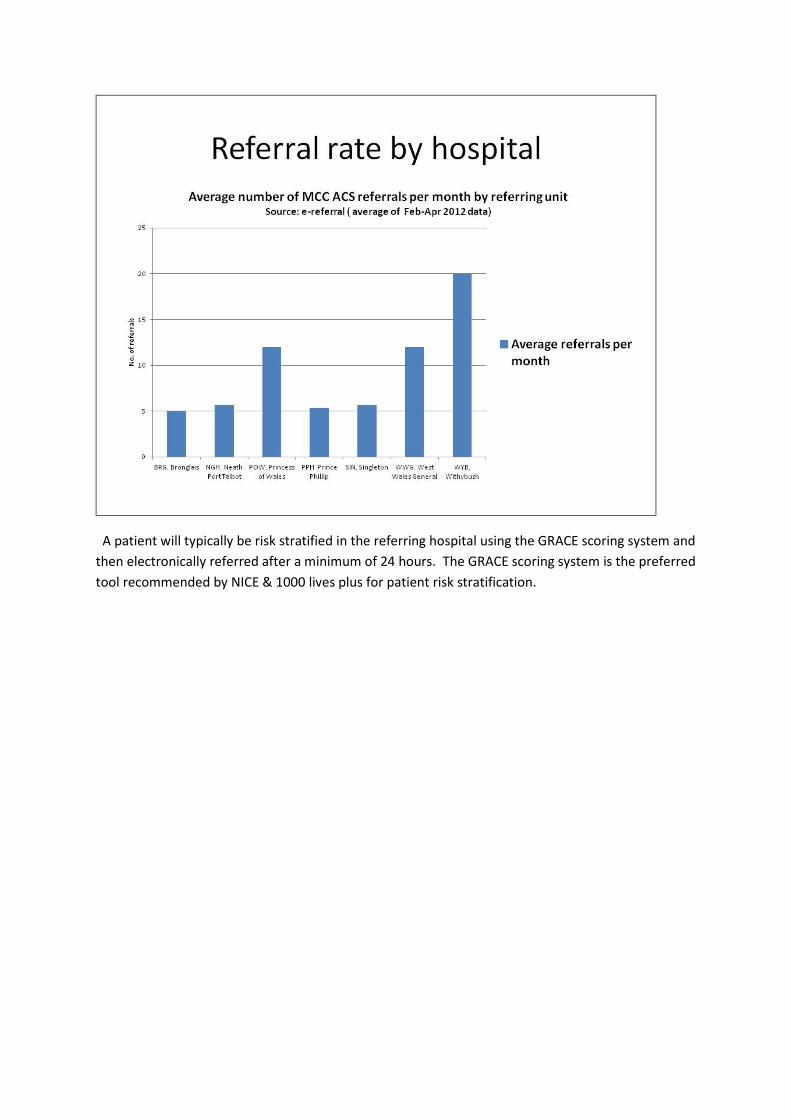
If the patient is admitted to the referring hospital at the weekend they will frequently not be
referred until the Monday ward round.
Equally at the current time, whilst we provide a 24/7/365 PPCI service for STEMI patients, we do not
provide angiography and angioplasty at the weekend for NSTE-ACS. Therefore if an NSTE-ACS patient
arrives in Morriston after 5pm on a Friday they will not receive angiography until Monday 9am at the
earliest (a gap of 65 hours).
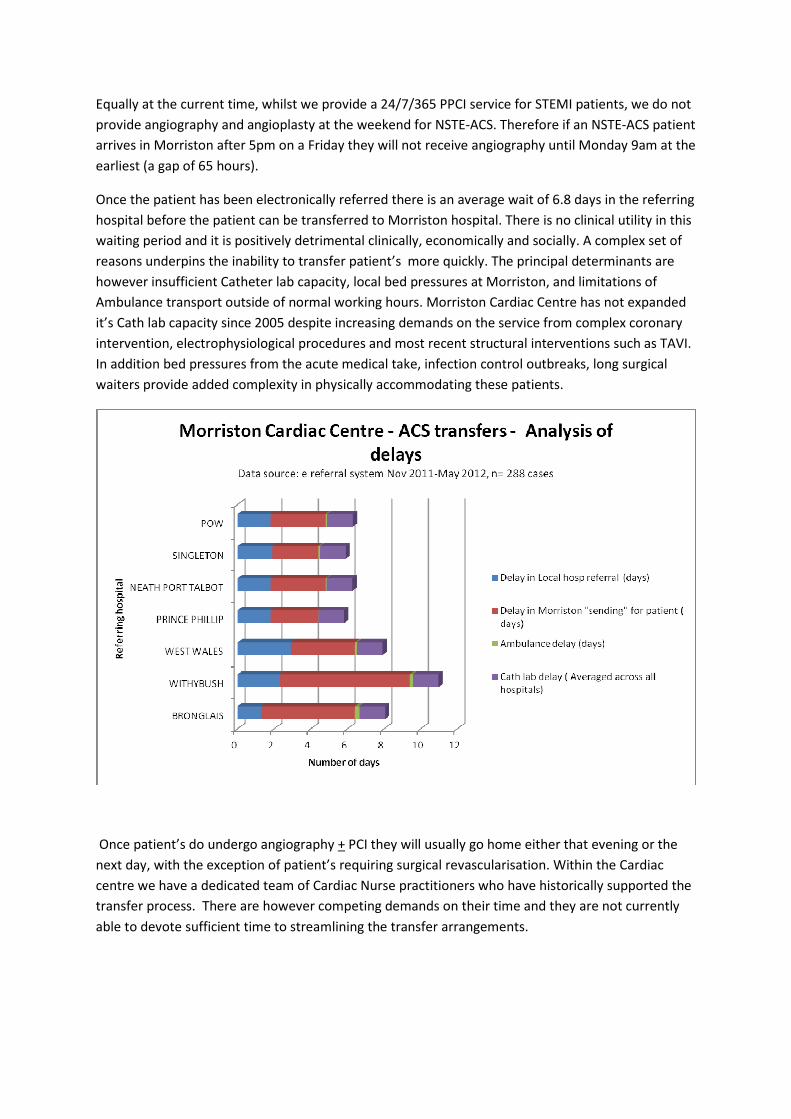
Once the patient has been electronically referred there is an average wait of 6.8 days in the referring
hospital before the patient can be transferred to Morriston hospital. There is no clinical utility in this
waiting period and it is positively detrimental clinically, economically and socially. A complex set of
reasons underpins the inability to transfer patient’s more quickly. The principal determinants are
however insufficient Catheter lab capacity, local bed pressures at Morriston, and limitations of
Ambulance transport outside of normal working hours. Morriston Cardiac Centre has not expanded
it’s Cath lab capacity since 2005 despite increasing demands on the service from complex coronary
intervention, electrophysiological procedures and most recent structural interventions such as TAVI.
In addition bed pressures from the acute medical take, infection control outbreaks, long surgical
waiters provide added complexity in physically accommodating these patients.
Once patient’s do undergo angiography + PCI they will usually go home either that evening or the
next day, with the exception of patient’s requiring surgical revascularisation. Within the Cardiac
centre we have a dedicated team of Cardiac Nurse practitioners who have historically supported the
transfer process. There are however competing demands on their time and they are not currently
able to devote sufficient time to streamlining the transfer arrangements.
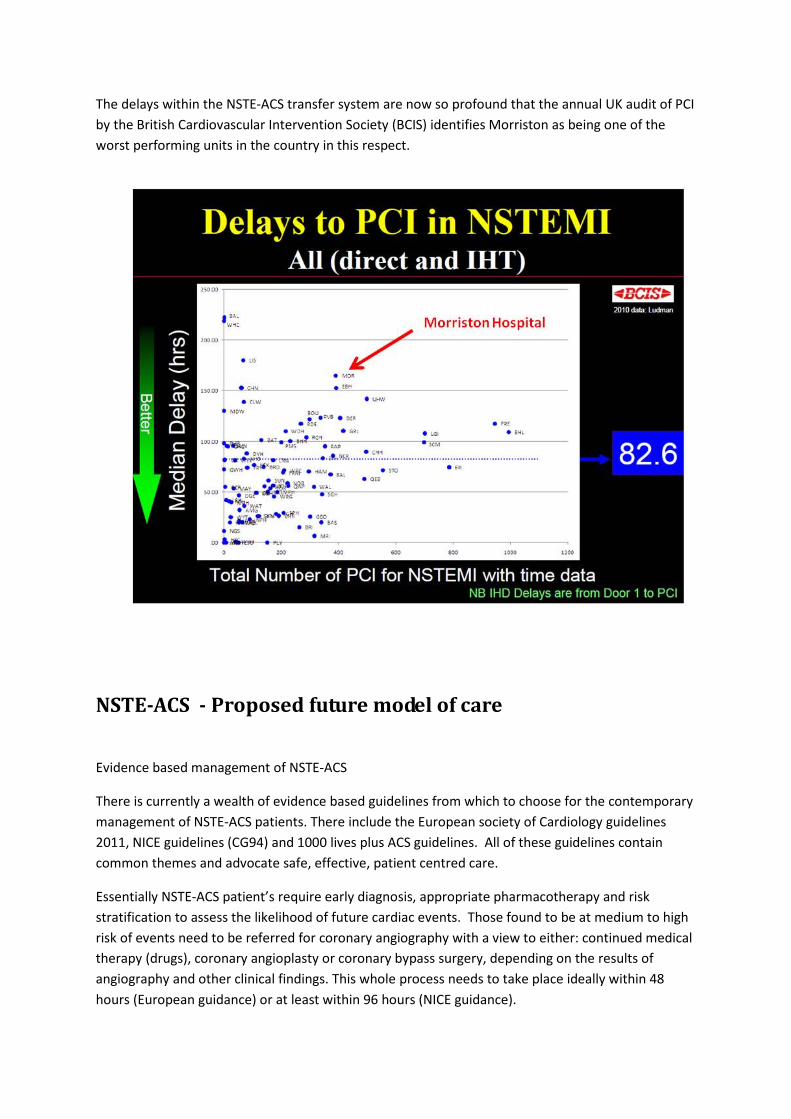
The delays within the NSTE-ACS transfer system are now so profound that the annual UK audit of PCI
by the British Cardiovascular Intervention Society (BCIS) identifies Morriston as being one of the
worst performing units in the country in this respect.
NSTE-ACS - Proposed future model of care
Evidence based management of NSTE-ACS
There is currently a wealth of evidence based guidelines from which to choose for the contemporary
management of NSTE-ACS patients. There include the European society of Cardiology guidelines
2011, NICE guidelines (CG94) and 1000 lives plus ACS guidelines. All of these guidelines contain
common themes and advocate safe, effective, patient centred care.
Essentially NSTE-ACS patient’s require early diagnosis, appropriate pharmacotherapy and risk
stratification to assess the likelihood of future cardiac events. Those found to be at medium to high
risk of events need to be referred for coronary angiography with a view to either: continued medical
therapy (drugs), coronary angioplasty or coronary bypass surgery, depending on the results of
angiography and other clinical findings. This whole process needs to take place ideally within 48
hours (European guidance) or at least within 96 hours (NICE guidance).
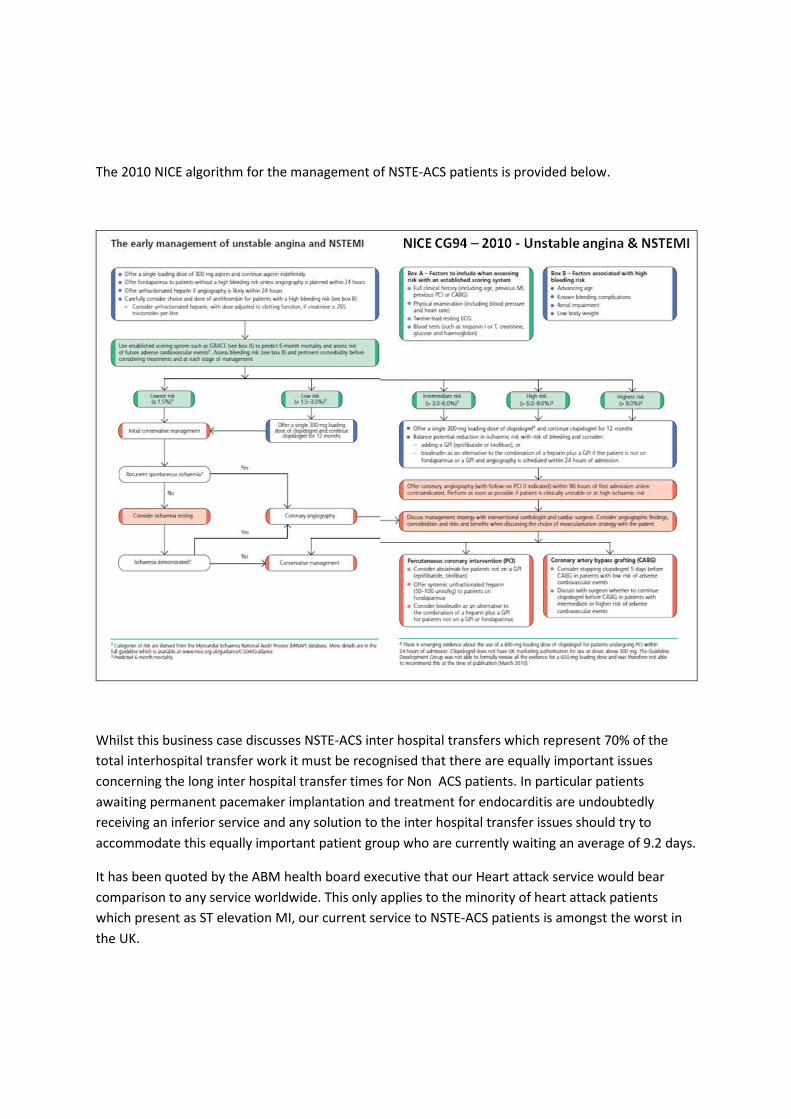
The 2010 NICE algorithm for the management of NSTE-ACS patients is provided below.
Whilst this business case discusses NSTE-ACS inter hospital transfers which represent 70% of the
total interhospital transfer work it must be recognised that there are equally important issues
concerning the long inter hospital transfer times for Non ACS patients. In particular patients
awaiting permanent pacemaker implantation and treatment for endocarditis are undoubtedly
receiving an inferior service and any solution to the inter hospital transfer issues should try to
accommodate this equally important patient group who are currently waiting an average of 9.2 days.
It has been quoted by the ABM health board executive that our Heart attack service would bear
comparison to any service worldwide. This only applies to the minority of heart attack patients
which present as ST elevation MI, our current service to NSTE-ACS patients is amongst the worst in
the UK.
How do we get there ?
The principal issue for providing safe, effective, patient centred care for our NSTE-ACS cohort is to
improve the currently unacceptable transfer times. The essential requirement is to provide the right
care for the NSTE-ACS patient at the right time in the right place. This will undoubtedly necessitate
changes to current working practices which have historically been organised around a pattern of
Monday to Friday, 9-5 working.
How do we improve transfer times ?
Timely transfer of patient’s with NSTE-ACS is dependent on a number of key variables , and requires
that the service has the potential to operate 24/7 365 days a year. The key variables are:
• Early recognition & prompt referral from surrounding hospitals
• Bed availability at Morriston Cardiac Centre to receive the patients
• Ambulance availability to facilitate patient transfer
• A trained Cath lab team & Cath lab capacity to perform angiography + intervention
• Flexing capacity to deal with the significant variations in weekly referrals
• Volume of Primary PCI workload
Only when deficiencies in all variables are correctly identified and treated and the service is
reorganised around a 7 day working week will significant improvements be made. The dependencies
are now discussed in more detail.
Early recognition & prompt referral
Early recognition is highly dependent on the skill mix and availability of staff in referring units. In an
ideal world all NSTE-ACS patient’s would be seen and risk stratified by a Consultant Cardiologist
within 24 hours of admission. This is a stated requisite of the Welsh National Service Framework for
Cardiovascular disease. This is not however currently practical in many referring units within Mid &
West Wales and so novel solutions will be required involving the use of Cardiac nurse practitioners,
automated scoring systems and early discussion with the Cardiac Centre. The Cardiac network is
currently facilitating this piece of work.
Bed availability at Morriston Cardiac Centre
Availability of limited beds in the cardiac centre is heavily dependent on a number of factors
Ward closures due to D& V & Norovirus outbreaks
Acute medical bed pressures
Upskilling of medical & nursing staff on Ward R
Delays in repatriation
Cardiac surgical workload and CITU bed availability
Bed management policy & practical thereof
In practice it is often the case that when there are hospital wide bed pressures the first group of
patients to suffer are the cardiac interhospital transfers. This is in part related to the current bed
management arrangements and the natural tendency to prioritise the patient who is in front of you.
There have already been 2 cases of cardiac patients who appear to have died whilst awaiting
transfer and it is no longer acceptable for the bed management arrangements to remain as they do
currently
Ambulance transfer
Ambulance transfer arrangements are complicated and have been extensively reviewed previously.
The dependencies include the funding arrangements for the Jumbulance, the ability to use “999”
ambulances when needed, and the ability to access private ambulances. The large travel times to
hospitals in West Wales have a particularly profound impact on capacity.
Cath lab capacity
Morriston Cardiac Centre is currently failing to operate a region wide emergency ACS
revascularisation service, elective revascularisation & EP service and a structural heart disease
service for a population of around 1 million from 2 Catheter laboratories and 1 pacing room. It is not
uncommon for a UK district general hospital to have similar facilities for half the size of population
with no EP or structural heart disease service. It is abundantly clear that currently Cath lab capacity
is a major limiting factor in meeting contemporary ACS revascularisation targets. In the long term
there will need to be a significant expansion in the Cardiac Centre however realistically in the short
term extended hours of operation of the existing Cath labs or a mobile facility are likely to be most
appropriate.
Flexing capacity
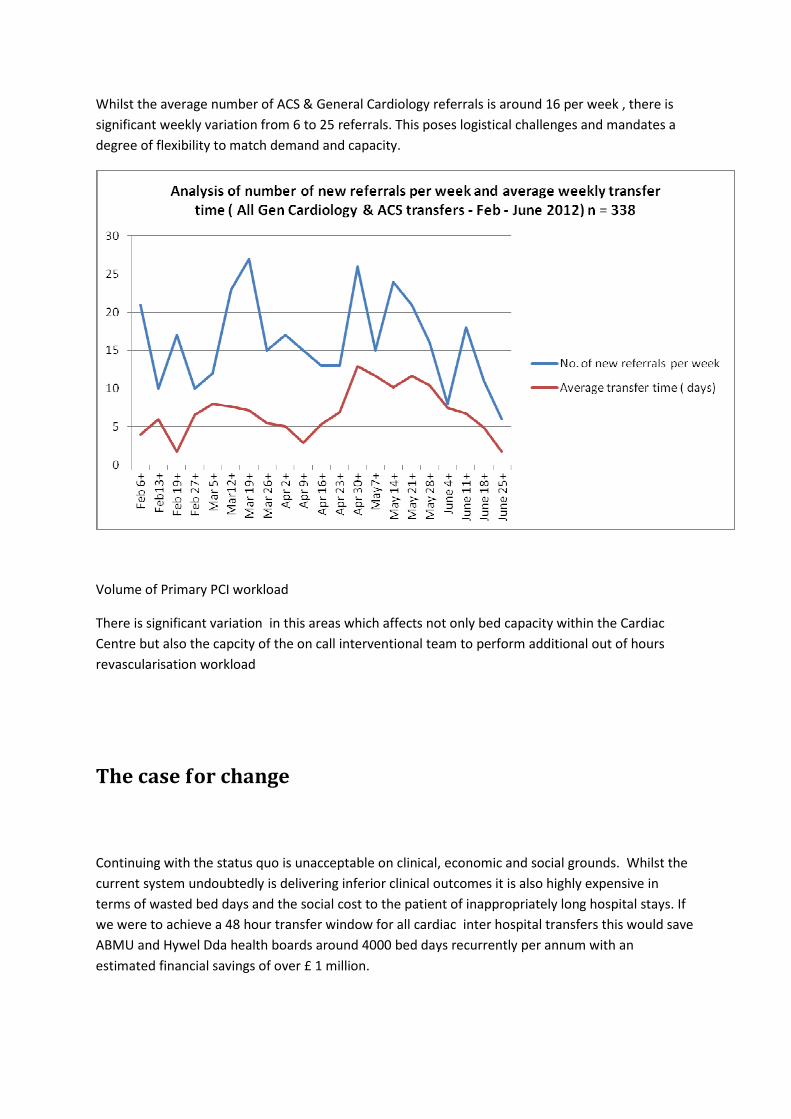
Whilst the average number of ACS & General Cardiology referrals is around 16 per week , there is
significant weekly variation from 6 to 25 referrals. This poses logistical challenges and mandates a
degree of flexibility to match demand and capacity.
Volume of Primary PCI workload
There is significant variation in this areas which affects not only bed capacity within the Cardiac
Centre but also the capcity of the on call interventional team to perform additional out of hours
revascularisation workload
The case for change
Continuing with the status quo is unacceptable on clinical, economic and social grounds. Whilst the
current system undoubtedly is delivering inferior clinical outcomes it is also highly expensive in
terms of wasted bed days and the social cost to the patient of inappropriately long hospital stays. If
we were to achieve a 48 hour transfer window for all cardiac inter hospital transfers this would save
ABMU and Hywel Dda health boards around 4000 bed days recurrently per annum with an
estimated financial savings of over £ 1 million.
Immediate action required
Preliminary analysis has suggested that the most significant deficiencies in the system are currently
the Cath lab capacity and ensuring a transfer bed is available. A composite of different solutions is
likely to be required including but not limited to:
• 7 day working week system for the Cath lab team
• Extended opening hours of Cardiac Short stay
• Up skilling and appropriate resourcing of nursing & medical staff on Ward R
• Greater autonomy in bed management of Ward R
• Use of a mobile Catheter lab system
• Ringfencing of prioritised Inter hospital transfer beds
• Greater nurse practitioner involvement in co-ordinating transfers
Due to the complex and dynamic interdependencies described previously we strongly advocate a
move away from the traditional pattern of 9-5 service provision. In order to fine tune the exact
operational requirements we would propose a 6 month pilot of extended Cath lab working including
evening and weekend sessions. This mandates a change in the health board’s approach to bed
management to one that prioritises cardiac inter hospital transfers. By doing this we are more likely
to realise greater bed efficiencies across the whole of this health board as well as Hywel Dda.
Conclusion
Cardiac disease remains the biggest killer in Wales and a significant proportion of this is avoidable.
The current model of service provision for the majority of heart attacks in Mid & West Wales is
inequitable, clinically outdated and financially unsustainable in the current climate. Whilst we have
made successful progress with Primary PCI in treating ST elevation myocardial infarction, NSTE-ACS
remains the elephant in the room in attempting to provide contemporary management of Acute
Coronary Syndromes. Delays in inter hospital transfers remain the single biggest failing of the system

and pose an ongoing and ever present clinical risk to patient’s and the health board. The financial,
emotional and social cost of the current system cannot be allowed to continue any longer. We
strongly advocate a long term structural solution which will involve increasing Cardiac Centre
capacity allied to 7 day working. However an immediate interim solution is required that increases
Cath lab capacity in conjunction with increased bed availability for inter hospital transfers. It should
be recognised that such an interim solution may be necessary for the next couple of years until
sufficient additional capital infrastructure has been realised.
Succesful implementation of this enhanced service will be of undisputed benefit to patients but also
has the potential to save over 4000 bed days recurrently per annum across ABMU & Hywel Dda
health boards.





![#442 NQF 0071: Persistence of Beta-Blocker Treatment After ... · In patients with concomitant NSTE-ACS [non-ST-elevation acute coronary syndrome], stabilized HF [heart failure],](https://img.pdfslide.net/doc/110x75/604263e58c2aca63cf6bb0df/442-nqf-0071-persistence-of-beta-blocker-treatment-after-in-patients-with.jpg)


















![Is heparin sufficient in non-ST-elevation acute coronary ... · acute coronary syndrome (NSTE-ACS) in the setting of PCI [1,2]. This recommendation is primarily based on the ACUITY](https://img.pdfslide.net/doc/110x75/5e789a6996af2f6cfb0c5c48/is-heparin-sufficient-in-non-st-elevation-acute-coronary-acute-coronary-syndrome.jpg)