Embed Size (px)
Citation preview
AORN JOURNAL AUGUST 1990, VOL. 52, NO 2
Reduced-Size Liver Transplantation HOPE FOR PEDIATRIC PATIENTS WITH END-STAGE LIVER DISEASE
E. Steve Woodle, MD; Joan Budzinski, RN; Margaret Pitman, R N Laurie Flanagan, RN; Pamela Boone, RN; Cassandra Smith, RN; Peter F. Whitington, MD; Jean C. Emond, MD; Christoph E. Broelsch, MD
iver transplantation is now an established means of therapy for end-stage liver disease L in children. Pediatric liver transplantation
continues to be plagued, however, by a shortage of donor organs, particularly from the very small donor. As a result, pretransplant mortality rates in children with end-stage liver disease remain unacceptably high, even exceeding mortality rates after transplantation at some medical centers.’ The shortage of donor organs becomes more pro- nounced when transplantation is required on an urgent basis, as in a child with fulminant hepatic failure or chronic liver disease with acute deterioration.
Reduced-size liver transplantation (RSLT) initially was employed as a means to lessen intraabdominal space problems in experimental heterotopic liver transplantation? In heterotopic
liver transplantation, the allograft liver is placed within the recipient abdomen without removal of the diseased native liver. With RSLT, the recipient’s diseased liver is removed, and a portion of the donor’s liver is placed in the recipient.
Initial clinical success with RSLT was reported in 1984.3 Reduced-size liver transplant procedures are now being performed in several centers in Europe and the United States! More than 70 RSLT procedures have been performed at the University of Chicago Hospitals.
Candidate Selection and Evaluation
ven though morbidity and mortality rates associated with RSLT have been compar- E able to those obtained with whole organ
E. Steve Woodle, MD, was a fellow in kidney, liver, and pancreas transplantation at the Universiiy of Chicago when this artide was written. He currently is a transplant surgeon and assistant professor of surgery, Washington University School of Medicine, St Louis. He earned‘ his medical degree from the Universiiy of Texas Medical Branch. Galveston.
Joan Budzinski, RN, BSN is a staff nurse in the OR, Wyler Children’s Hospital, University of Chicago Hospitals. She received her associate degree in nursing from Prairie State College, Chicago Heights, Ill and her BSN from the
University of Illinois Medical Center, Chicago.
Margaret Pitman, RN, is a staff nurse in the OR, Wyler Children’s Hospital, University of Chicago Hospitals. She received her diploma in nursing from Westchester School of Nursing Valhalla NI:
Laurie Flanagan, RN, BSN is a staff nurse in the OR, Wyler Children’s Hospital, University of Chicago Hospitals. She received her diploma in nursing from St Vincent Charity Hospital School of Nursing, Cleveland and her BSNfrom St Xavier College, Chicago.
252

AUGUST 1990, VOL 52, NO 2 AORN J O U R N A L
transplants? RSLT has been applied primarily in
children who are in urgent need of a liver transplant. Children who are critically ill from fulminant hepatic failure, primary hepatic allograft nonfunction, or acute deterioration superimposed on chronic liver failure can benefit from RSLT. More recently, RSLT has been used in children with end-stage liver disease who have demon- strated ongoing deterioration while awaiting a donor organ.
The pediatric hepatologist conducts a pretrans- plantation evaluation that includes an extensive patient medical history and physical examination. Routine testing includes
complete blood count (CBC), serum electrolytes, blood urea nitrogen, creatinine, liver enzymes, serum bilirubin, vitamin A, D, E, and K serum levels, prothrombin time, chest x-ray, abdominal ultrasound with Doppler exam- ination, and echocardiogram. psychosocial evaluation is performed by the
transplant clinical social worker. After the preoperative evaluation is complete, the pediatric hepatologist and the transplant surgeon review each patient and reach a decision regarding transplantation. Other than an active infection or
incurable cancer, few contraindications to liver transplantation for children exist.
If the patient is an appropriate candidate, the pediatric hepatologist and transplant surgeon meet with the parents to describe pediatric liver transptantation and RSLT. The physicians answer the parents’ questions and obtain surgical consent. The physicians ensure that the parents realize the procedure is complex, and the child will be ill for some time following transplantation. They also stress that the child must make a lifelong commitment to taking immunosuppressive drugs, and the parents and child must adhere to close medical followup after transplantation. Imme- diately before the transplant procedure, the physicians answer any remaining questions for the parents.
After the decision is reached to proceed with RSLT, the recipient is placed on the transplant list. The weight range of the donor can be between 0.8 and 10 times the recipient’s size. A right lobe graft will reliably accommodate donor-recipient weight ratios of 2:l or less; left lobe grafts will accommodate donor-recipient weight ratios of 4: 1 or less; and left lateral segmental grafts will accommodate donor-recipient weight ratios of 8: 1 or less. Selection of appropriate donor-recipient combinations involves additional considerations. Obese donors, for example, have liver weights that are less than can be predicted based on total body weight alone. Variations exist in size and configuration of liver segments, particularly the
Pamela Boone, RN, MSN, is a nurse associate, Wyler Children ’s Hospital, University of Chicago Hospitals. She received her BSN from Chicago State University, and her MSN from St Xavier College, Chicago.
Cassandra Smith, RN, BSN, is a nurse associate in pediatric hepatology, Wyler Children k Hospital, University of Chicago Hospitals. She received her BSN from the University of Missouri, Columbia.
Peter F. Whitington, MD, is the director of the pediatric liver transplant program and associate professor of pediatrics and medicine, Wvler
Children’s Hospital, University of Chicago Hospitals. He earned his medical degree from the University of Tennessee Center for the Health Sciences, Memphis.
Jean C. Emond, MD, is a liver transplant surgeon and assistant professor of surgery, University of Chicago Hospitals. He earned his medical degree from the University of Chicago.
Christoph E. Broelsch, MD, is the chief of liver transplantation and professor of surgery, Univer- sity of Chicago. He earned his medical degree from the University of Dusseldorf (Germany),
253
AORN JOURNAL AUGUST 1990, VOL. 52, NO 2
Recovery of the donor liver is compatible with recovery of all other solid organs
(ie, heart, heart-lung, pancreas, kidney).
left lateral segment. As a result, we have been able to accommodate donor-recipient weight ratios of up to 12:l for left lateral segmental grafts.
Preparing Donor Grafts
he majority of organ harvest procedures involve procurement of multiple organs. T Recovery of the donor liver is compatible
with recovery of all other solid organs (ie, heart, heart-lung, pancreas, kidney).
The surgeon performs the donor procedure through a midline incision from suprasternal notch to pubis. He or she explores the abdomen and chest for preexisting pathologic conditions and injuries. The surgeon divides the falciform and left triangular ligaments. He or she then divides the common bile duct immediately above the duodenum, and the hepatic artery and portal vein are isolated. The surgeon elevates the right colon and small intestine mesentary from the retroper- itoneum, exposing the inferior vena cava (IVC) and aorta. The surgeon dissects and isolates the left renal vein and superior mesenteric artery. The anesthesiologist administers 200 units/kg body weight heparin through the central venous catheter. The surgeon cannulates the aorta immediately above its bifurcation with a #16 or #20 French aortic cannula. He or she occludes the supraceliac aorta with a vascular clamp and infuses 1 to 1 M L of University of Wisconsin (UW) preservation solution at 4 OC (39 O F ) through the aortic cannula. The solution is a potassium-based preservation solution with hydroxyethyl starch as its colloid component.
The surgeon f& the abdomen with 4 "C (39 O F ) saline slush after the preservation solution infusion is complete and initiates removal of the liver by dividing the portal vein at the junction of the superior mesenteric vein and splenic vein. He or she then removes the arterial supply of
the liver graft, which includes the hepatic artery, the celiac axis, and a segment of donor aorta. The surgeon transects the infrahepatic IVC cephalad to the renal veins and the suprahepatic IVC above the diaphragm. He or she divides the remaining diaphragmatic attachments and removes the hepatic allograft.
The surgeon places the hepatic allograft in a basin containing cold UW solution. The gall- bladder is removed, and the biliary tree is flushed thoroughly with preservation solution. The liver is packaged in a sterile plastic bag and placed in an self-sealing plastic container. The container is placed on ice in an ice chest for transportation. The UW preservation solution reliably extends liver preservation times to between 16 and 24 hours, which easily accommodates the additional two to three hours required for preparation of the reduced-size liver graft?
Preoperative Care
he circulating nurse meets the recipient and his or her family in the preoperative holding
questions and provides emotional support. The nurse ensures that the surgical consent, patient's identification bracelet, blood identification numbers, and patient history are complete. At the time of admission, the nurse ensures that the patient's blood is drawn for a type and cross match, CBC, prothombin time, and serum electrolytes.
The nursing team begins room set-up one hour before the scheduled procedure time. Because children can have difficulty with thermoregulation, the perioperative nurse raises the room temper- ature and places a hyperthermia mattress on the OR bed and sets the thermostat at 38 OC (101 OF). The nurse covers the mattress with foam padding to ensure the patient's skin integrity. The circulating nurse obtains blood and fresh frozen plasma from the blood bank and places them in
T area. He or she answers any additional
254
AORN JOURNAL AUGUST 1990, VOL. 52, NO 2
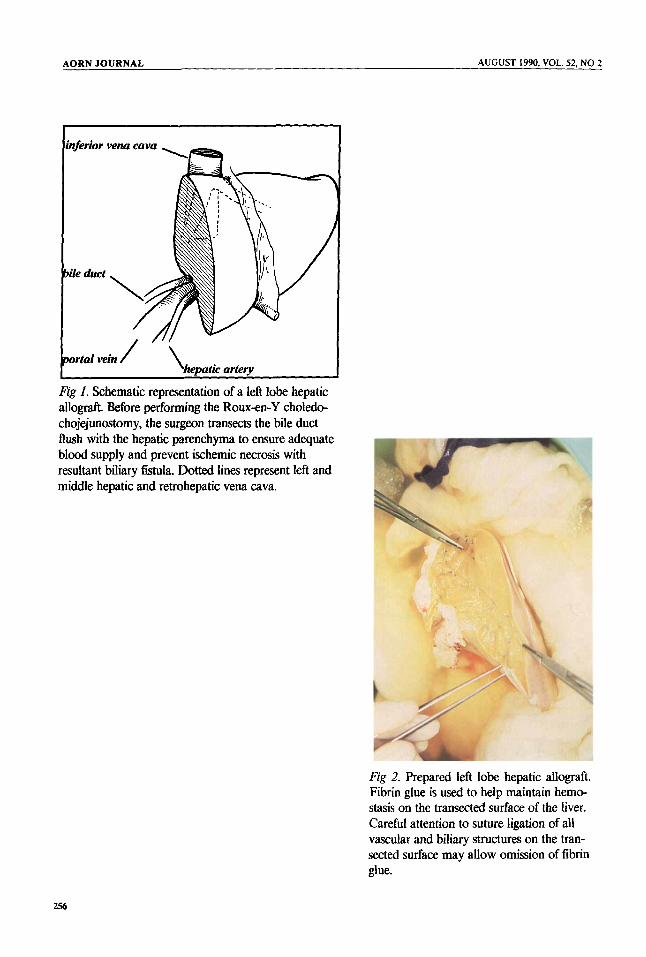
Fig I. Schematic representation of a left lobe hepatic allograft. Before performing the Rouen-Y choledo- chojejunostomy, the surgeon transects the bile duct flush with the hepatic parenchyma to ensure adequate blood supply and prevent ischemic necrosis with resultant biliary fistula. Dotted lines represent left and middle hepatic and retrohepatic vena cava.
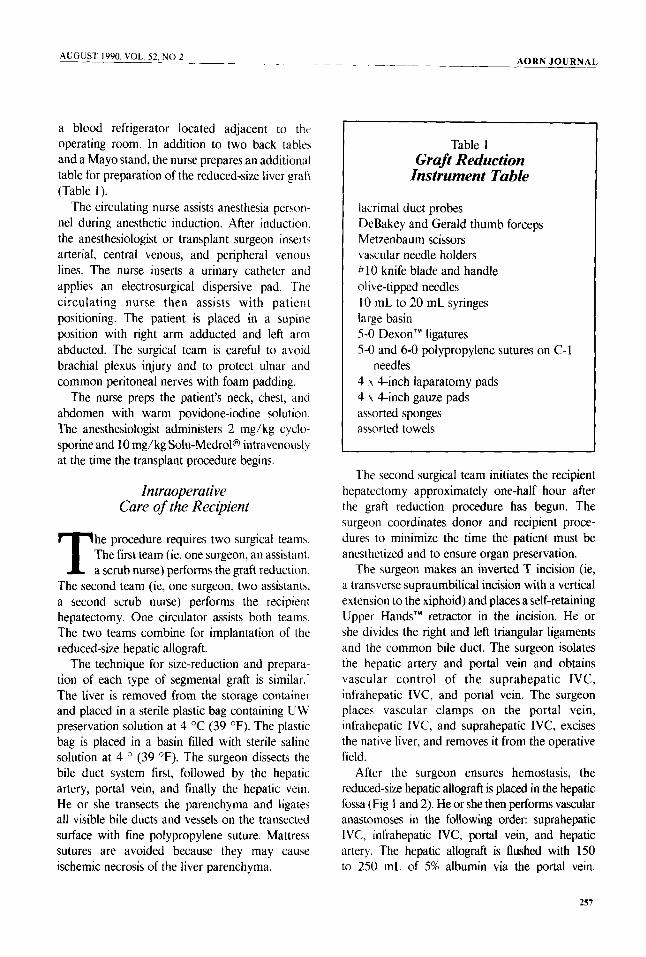
Fig 2. Prepared left lobe hepatic allograft. Fibrin glue is used to help maintain hemo- stasis on the transected surface of the liver. Careful attention to suture ligation of all vascular and biliary structures on the tran- sected surface may allow omission of fibrin glue.
256
AUGUST 1990. VOL. 52. NO 2
a blood refrigerator located adjacent to the operating room. In addition to two back tables and a Mayo stand, the nurse prepares an additional table for preparation of the reduced-size liver graft (Table 1).
The circulating nurse assists anesthesia person- nel during anesthetic induction. After induction. the anesthesiologist or transplant surgeon inserts arterial, central venous, and peripheral venous lines. The nurse inserts a urinary catheter and applies an electrosurgical dispersive pad. The circulating nurse then assists with patient positioning. The patient is placed in a supine position with right arm adducted and left arm abducted. The surgical team is careful to avoid brachial plexus injury and to protect ulnar and common peritoneal nerves with foam padding.
The nurse preps the patient’s neck, chest, and abdomen with warm povidone-iodine solution The anesthesiologist administers 2 mg/kg cyclo- sporine and 10 mg/kg Soh-Medrol@ intravenously at the time the transplant procedure begins.
In traoperative Care of the Recipient
he procedure requires two surgical teams The first team (ie, one surgeon, an assistant. T a scrub nurse) performs the graft reduction
The second team (ie, one surgeon, two assistants. a second scrub nurse) performs the recipient hepatectomy. One circulator assists both teams The two teams combine for implantation of the reduced-size hepatic allograft.
The technique for size-reduction and prepara- tion of each type of segmental graft is similar.- The liver is removed from the storage container and placed in a sterile plastic bag containing UW preservation solution at 4 OC (39 O F ) . The plastic bag is placed in a basin filled with sterile saline solution at 4 O (39 OF) . The surgeon dissects the bile duct system first, followed by the hepatic artery, portal vein, and finally the hepatic vein. He or she transects the parenchyma and ligates all visible bile ducts and vessels on the transected surface with fine polypropylene suture. Mattress sutures are avoided because they may cause ischemic necrosis of the liver parenchyma.
-_ AORN J O U R N A L
Table 1 Graft Reduction
Instrument Table
lacrimal duct probes DeBakey and Gerald thumb forceps Metzenbaum scissors vascular needle holders # 10 knife blade and handle olive-tipped needles I0 mL to 20 mL syringes large basin 5-0 DexonTM ligatures 5-0 and 6-0 polypropylene sutures on C-1
4 Y 4-inch laparatomy pads 4 x 4-inch gauze pads assorted sponges assorted towels
needles
The second surgical team initiates the recipient hepatectomy approximately one-half hour after the graft reduction procedure has begun. The surgeon coordinates donor and recipient proce- dures to minimize the time the patient must be anesthetized and to ensure organ preservation.
The surgeon makes an inverted T incision (ie, a transverse supraumbilical incision with a vertical extension to the xiphoid) and places a self-retaining Upper Hands” retractor in the incision. He or she divides the right and left triangular ligaments and the common bile duct. The surgeon isolates the hepatic artery and portal vein and obtains vascular control of the suprahepatic IVC, infrahepatic IVC, and portal vein. The surgeon places vascular clamps on the portal vein, infrahepatic IVC, and suprahepatic IVC, excises the native liver, and removes it from the operative field.
After the surgeon ensures hemostasis, the reduced-size hepatic allograft is placed in the hepatic fossa (Fig 1 and 2). He or she then performs vascular anastomoses in the following order: suprahepatic IVC, infrahepatic IVC, portal vein, and hepatic artery. The hepatic allograft is flushed with 150 to 250 mL of 5% albumin via the portal vein.
257

AUGUST 1990, VOL. 52, NO 2 AORN JOURNAL
Fig 3. Revascularized left lobe hepatic allograft. Minimal bleeding is present from the transected surface of the liver.
The surgeon removes the vascular clamps, and reperfusion is achieved (Fig 3). During the next half-hour, the surgeon ensures hemostasis, and the anesthesiologist rewarms and stabilizes the patient. Biliary tract reconstruction is performed, either with a choledochocystostomy or a Roux- en-Y hepatodocho-jejunostomy. He or she inserts abdominal drains and then closes the abdomen.
Throughout the procedure there is a coordinated effort between the staffs of the OR and the blood bank to maintain an adequate supply of blood products (eg, packed red blood cells, fresh frozen platelets and blood cells).
The surgical team pays careful attention throughout the procedure to the temperature of the irrigation solutions. Before revascularization of the reduced-size liver graft, cold (4 OC [39 O F I )
saline is used to help prevent premature rewarming of the graft. Following reperfusion, warmed imgation is used to help maintain the patient’s body temperature.
During extended procedures, the circulating
nurse periodically informs the family of the patient’s condition and progress of the operation either in person or by telephone. Before conclusion of the procedure, the circulating nurse alerts the pediatric intensive care unit (ICU) nurse of the patient’s impending arrival and gives him or her a brief report.
Postoperative Care
embers of the surgical team transport the child to the ICU. The ICU staff M places the patient in a supine position
on an eggcrate mattress with warming blankets above and below the patient. Mechanical ventilation is maintained for a minimum of eight to 12 hours. A chest x-ray is obtained immediately on arrival in the ICU. The ICU nurse monitors vital signs, drains, and urine output. He or she measures the patient’s abdominal girth hourly to assess the presence of intraabdominal bleeding. The nurse also monitors IV and blood product infusions. He or she ensures that blood is drawn
258
AUGUST 1990, VOL. 52, NO 2 AORN JOURNAL
and sent to the laboratory for arterial blood gas, electrolytes, CBC, prothrombin time, liver enzymes, and bilirubin determinations. Visitation is allowed after the patient’s vital signs are stabilized. Formal protective isolation is not used, however, assiduous attention is placed on handwashing.
Patients remain in ICU for at least 24 hours. The primary criteria for transfer from the ICU are cardiopulmonary stability and adequate renal function. Patients are monitored for acute rejection during the fmt two postoperative weeks with daily blood tests of levels of bilirubin, serum glutamic pyruvic transaminase (SGPT), alkaline phospha- tase, and serum gamma glutamyl transpeptidase (SGGT).
The patient is allowed to eat when adequate bowel sounds return. This usually occurs by the beginning of the second postoperative week. The patient is converted from intravenous to oral cyclosporine after adequate oral intake is established. The patient is required to take cyclosporine for the remainder of his or her life. An elevation in bilirubin, SGPT, alkaline phosphatase, or SGGT levels may require liver biopsy to diagnose for acute rejection. High-dose corticosteroid therapy (eg, Solu-MedroP 10 mg/kg/day for three days) provides first-line therapy for acute rejection. Corticosteroid- resistant acute rejection requires the administra- tion of OKT3 monoclonal antibody therapy. This commonly used immunosuppressive agent is a murine monoclonal antibody that binds to the T-cell receptor complex on human T lympho- cytes.
Following discharge from the hospital, patients are evaluated in the transplant clinic on a weekly basis. Bilirubin and liver enzymes are determined twice weekly during the first two months following discharge.
Conclusion
Reduced-size liver transplantation in children provides graft and patient survival rates similar to those obtained with whole organ liver transplants. This procedure provides the advantage of major reductions in pretransplant mortality in children. 0
Notes 1. C E Broelsch et al, “Liver transplantation with
reduced-size donor organs,” Tramplantation 45 (March 1988) 519-524; C 0 Esquivel et al, “Liver transplan- tation before one year of age,” Journal of Pediatrics 110 (April 1987) 545-548; J R Lilly, R J Hall, R P Altman, “Liver transplantation and Kasai operation in the first year of life: Therapeutic dilemma in biliary atresia” (Editorial) Journal of Pediatrics 110 (April 1987) 561-562; B J Zitelli et al, “Evaluation of the pediatric patient for liver transplantation,” Pediatrics 78 (October 1987) 559-565.
2. J B Price, Jr, A B Voorhees, Jr, R C Britton, “Partial hepatic autotransplantation with complete revascularization in the dog,” Archives of Surgery 95 (July 1967) 59; M N Van der Heyde, “The role of functional competition in auxiliary liver transplanta- tion,” Transplantation 5 (May 1966) 78.
3. H Bismuth, D Houssin, “Reduced-size orthotopic liver graft in hepatic transplantation in children,” Surgery 95 (March 1984) 367-370; C E Broelsch et al, “Orthotopic transplantation of hepatic segments in infants with biliary atresia,” Chirurgisches Forum 19848 Experim u. Klimhche Forschung Hrsg, L Koslowski, ed (BerWHeidelberg: Verlang/Springer, 1984).
4. Bismuth, Houssin, “Reduced-size orthotopic liver graft in hepatic transplantation in children,” 367-370; R Pichlmayr et al, “Transplantation einer Spenderleber auf zwei Empfanger (Splitting-Transplantation),” Lungenbeck’s Archives Chirurgkhes 383 (1988) 127- 130; J B Otte et al, “Recent developments in pediatric liver transplantation,” Transplantation Proceedings 19 (October 1987) 43614364,
5. C E Broelsch et al, “Liver transplantation, including the concept of reduced-size liver transplants in children,” Annals of Surgery 208 (October 1988) 410-420.
6. S Todo et al, “Extended preservation of human liver grafts with UW solution,” Journal of the American MedicalAssociation 261 (Feb 3, 1989) 711-714.
7. Broelsch et al, “Liver transplantation, including the concept of reduced-size liver transplants in children,” 410-420.
verall, one-year patient survival rates in excess of 75% are obtained by most 0 pediatric liver transplantation programs.
In most programs, retransplantation rates vary between 10% and 25%.