Embed Size (px)
Citation preview

Reducing Adverse Drug Events: Strategies to Accelerate Improvement Webinar - Opioid Safety
Frank FedericoVice President
August 17, 2017
This presenter has no conflicts of interest to
disclose
ObjectivesDescribe the elements of a safe systemList three interventions to improve opioid safetyDescribe two measures to determine if your efforts to improve opioid safety have succeededList the benefits to patients
Starting Your Journey to Improved Opioid Safety
Understand the principles of a safe systemPrevent errors and harmIdentify errors and harm before each progresses to more serious eventMitigate intervene to minimize the impact of the error or harm
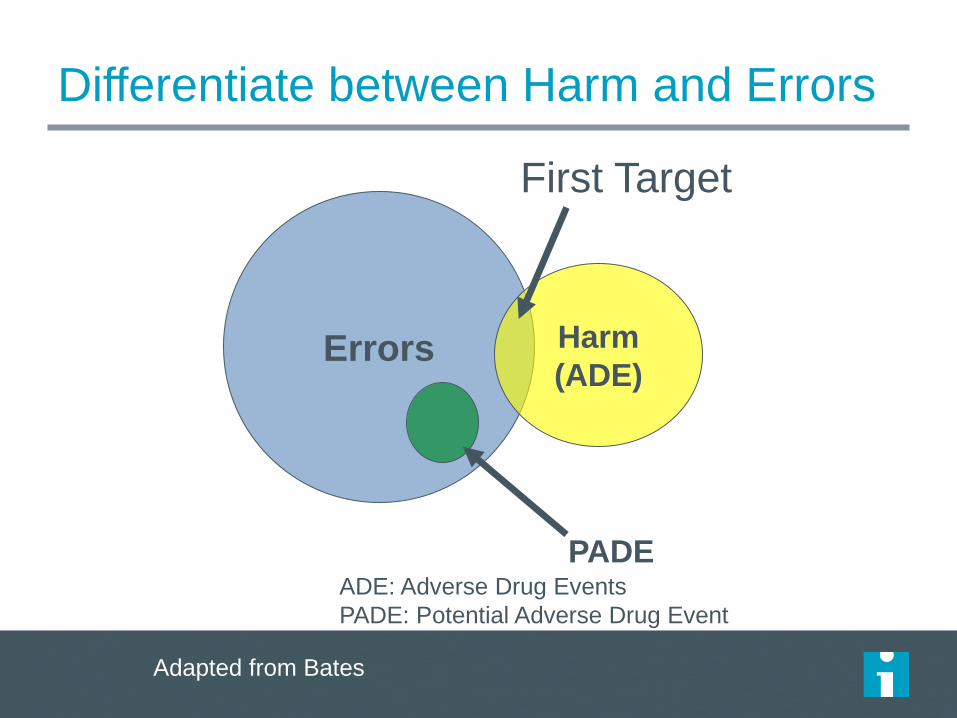
Differentiate between Harm and Errors
Errors Harm(ADE)
PADE
First Target
Adapted from David Bates, MD
ADE: Adverse Drug EventsPADE: Potential Adverse Drug Event
Adapted from Bates
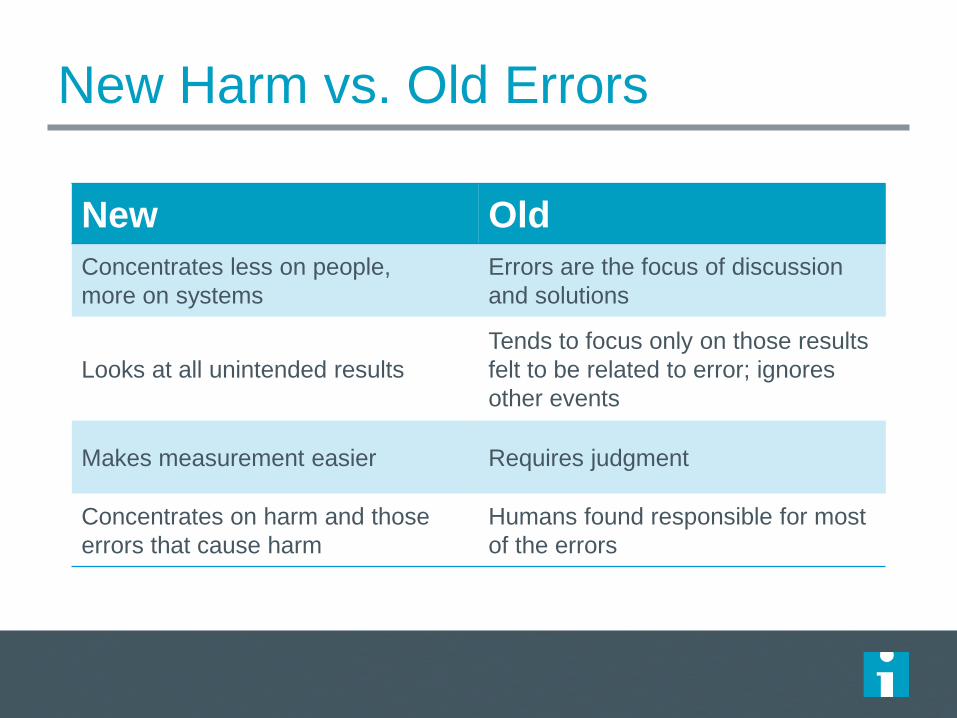
New Harm vs. Old Errors
5
New OldConcentrates less on people, more on systems
Errors are the focus of discussion and solutions
Looks at all unintended resultsTends to focus only on those results felt to be related to error; ignores other events
Makes measurement easier Requires judgment
Concentrates on harm and those errors that cause harm
Humans found responsible for most of the errors
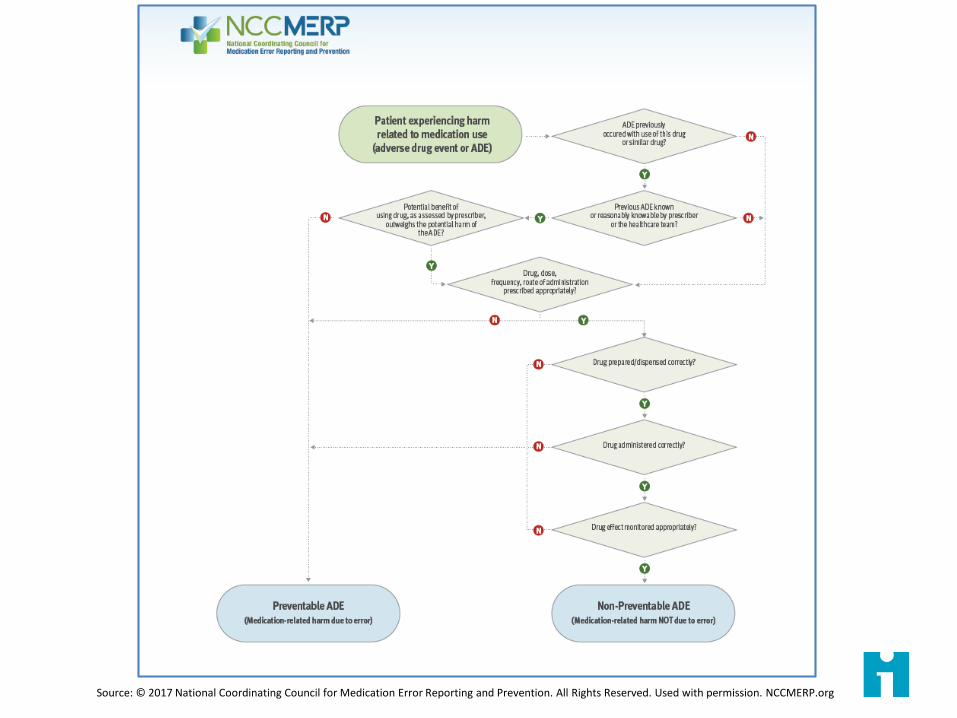
Source: © 2017 National Coordinating Council for Medication Error Reporting and Prevention. All Rights Reserved. Used with permission. NCCMERP.org
Errors that Contribute to HarmMix-ups between morphine and HYDROmorphone outnumbered all other medication-pair errorsDosing errorPump errorsAdministration errorsPrescribing errorsConfusion between immediate- and sustained-release formulations.Of the 41,727 events involving opioids, 11.9% (n = 4,958) were reported as wrong-drug events.
http://www.ncbi.nlm.nih.gov/pubmed/17957978
Common RisksLook-alike drug names and packages Concentration errors Use of dangerous abbreviations Dosing errors Line confusion Adverse drug reactions Mislabeled syringes Patient monitoring problems Unintended use
Definition of Harm
In the IHI Global Trigger Tool, the definition used for harm is as follows:
Unintended physical injury resulting from or contributed to by medical care that requires additional monitoring, treatment or hospitalization, or that results in death.
9
Accepting the Harm Burden
Concept of moving from a focus on error and the preventable to the measurement
of global institutional harm, whether preventable or not
10
Common Opioid-related HarmDeath Due To Opioids– Intentional and Unintentional
Unintentional Opioid Poisoning Opioid Induced Respiratory Depression (OIRD)FallsFracturesOversedation
John Kruger Source
Opioids in The Hospital Setting: Increased Risk of Cardio-Pulmonary ArrestOpioids Induced ConstipationOpioids and Fracture Risk in the ElderlyOpioids and Fall Risks in Younger Persons
Second Victim PhenomenaNewborns
– Neonatal Abstinence Syndrome– Possible impact on future addiction and health1
Children– Risk for harm and abuse– May lead to inadvertent substance use/abuse and poisoning.
Families– Increased risk of family stress and possibly suicide
Society– Increased demands on law enforcement and criminal justice system.– Increased costs for insurance and risk management resources. – Increased costs for treatment of addiction and substance use disorders as
well as healthcare resource utilization and healthcare worker burnout. – Increased risks and costs to workplaces and workers– Increased risks and costs to rest of society in form of diverted resources and
reduction in taxpayer base.
Source: 1. BM, Tronick E, Nestler E, et al. Behavioral epigenetics. Ann N Y Acad Sci. 2011;1226:14–33. John Kruger Source
Source: http://patientsafety.pa.gov/pst/Documents/Opioids/assessment.pdf

Finding Harms in Your Health System
The IHI Global Trigger ToolAdverse Event Trigger Tool Data AnalysisOrganizational Assessment of Safe Opioid PracticesGo and See Data AnalyticsPatient Identified HarmsStandardized Mortality Rate (SMR)Population Health Statistics (Community Level)PCA Safety Checklist
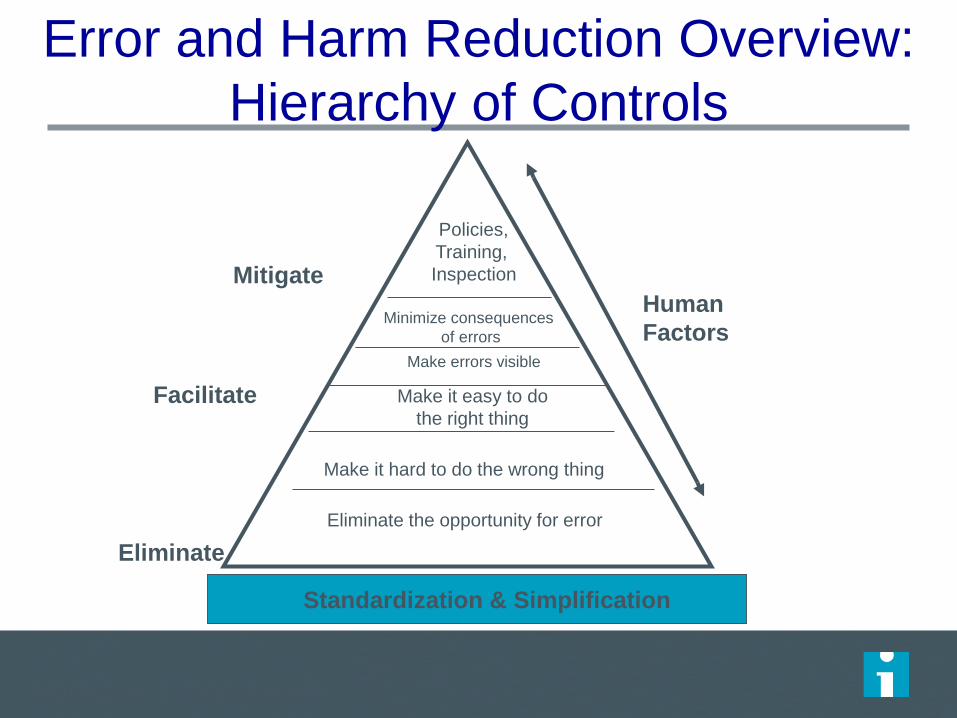
Error and Harm Reduction Overview: Hierarchy of Controls
Standardization & Simplification
Policies,Training, Inspection
Minimize consequencesof errors
Make it easy to do the right thing
Make it hard to do the wrong thing
Eliminate the opportunity for error
HumanFactors
Mitigate
Facilitate
Eliminate
Make errors visible
Adapted by D. Bonacum KP
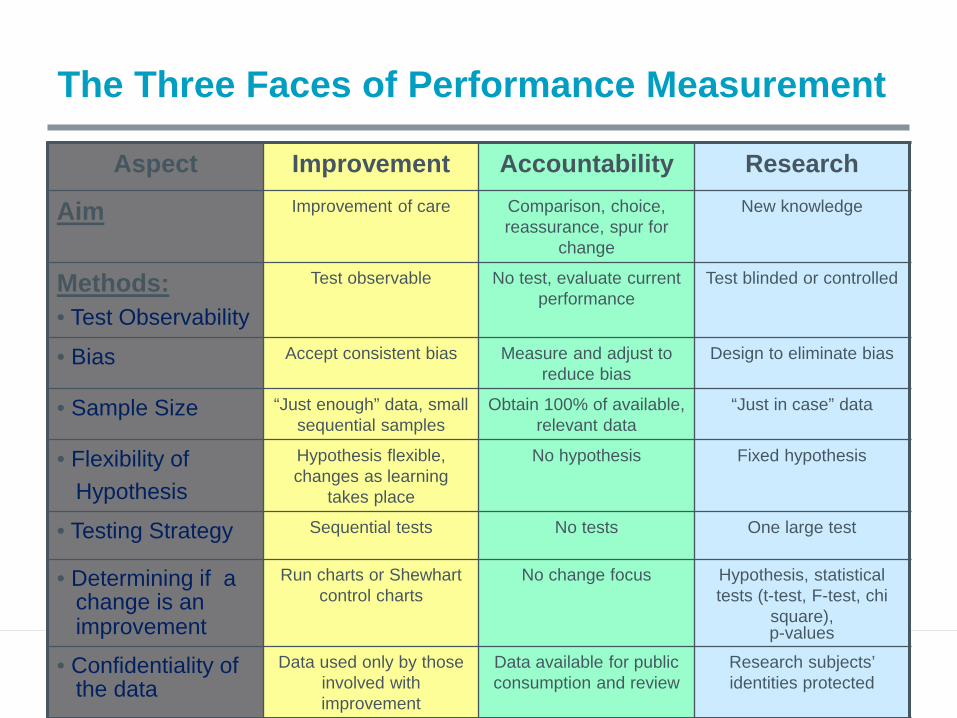
The Three Faces of Performance Measurement
Aspect Improvement Accountability Research
Aim Improvement of care Comparison, choice, reassurance, spur for
change
New knowledge
Methods:• Test Observability
Test observable No test, evaluate current performance
Test blinded or controlled
• Bias Accept consistent bias Measure and adjust to reduce bias
Design to eliminate bias
• Sample Size “Just enough” data, small sequential samples
Obtain 100% of available, relevant data
“Just in case” data
• Flexibility ofHypothesis
Hypothesis flexible, changes as learning
takes place
No hypothesis Fixed hypothesis
• Testing Strategy Sequential tests No tests One large test
• Determining if achange is animprovement
Run charts or Shewhart control charts
No change focus Hypothesis, statistical tests (t-test, F-test, chi
square), p-values
• Confidentiality ofthe data
Data used only by those involved with improvement
Data available for public consumption and review
Research subjects’ identities protected
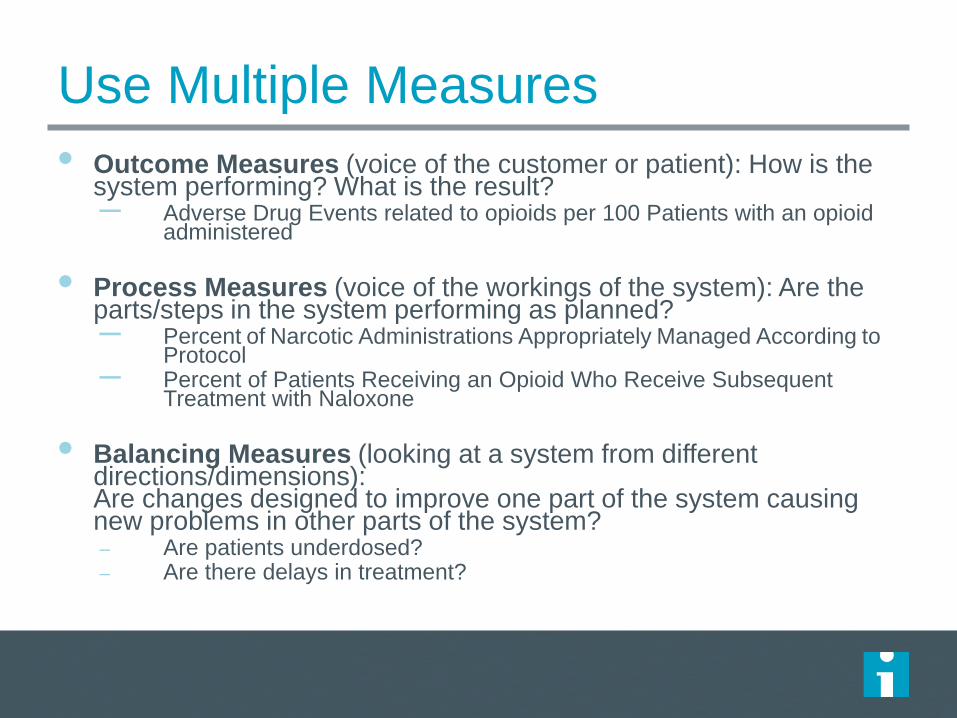
Use Multiple Measures • Outcome Measures (voice of the customer or patient): How is the
system performing? What is the result? – Adverse Drug Events related to opioids per 100 Patients with an opioid administered
• Process Measures (voice of the workings of the system): Are the parts/steps in the system performing as planned? – Percent of Narcotic Administrations Appropriately Managed According to
Protocol– Percent of Patients Receiving an Opioid Who Receive Subsequent Treatment with Naloxone
• Balancing Measures (looking at a system from different directions/dimensions): Are changes designed to improve one part of the system causing new problems in other parts of the system?– Are patients underdosed?– Are there delays in treatment?
Examples of MeasuresHave you developed a protocol or order set for all appropriate medications?– Is the protocol or order set being used?
Have you developed dose-conversion charts to minimize errors when changing from one medication to another? For pain medications?– If you have developed dose conversion charts, are
they being used?Are patients monitored using established protocols?

https://www.hqsc.govt.nz/assets/GTT/NEMR-images--files/GTT-workshop-Ashika-Maharaj-April-2013.pdf

Tips for Effective MeasuresUse a sample of, at most, ten patient charts per week on the unit where you are testing the new process Plot data over timeSeek usefulness, not perfectionUse samplingIntegrate measurement into the daily routineUse qualitative and quantitative data
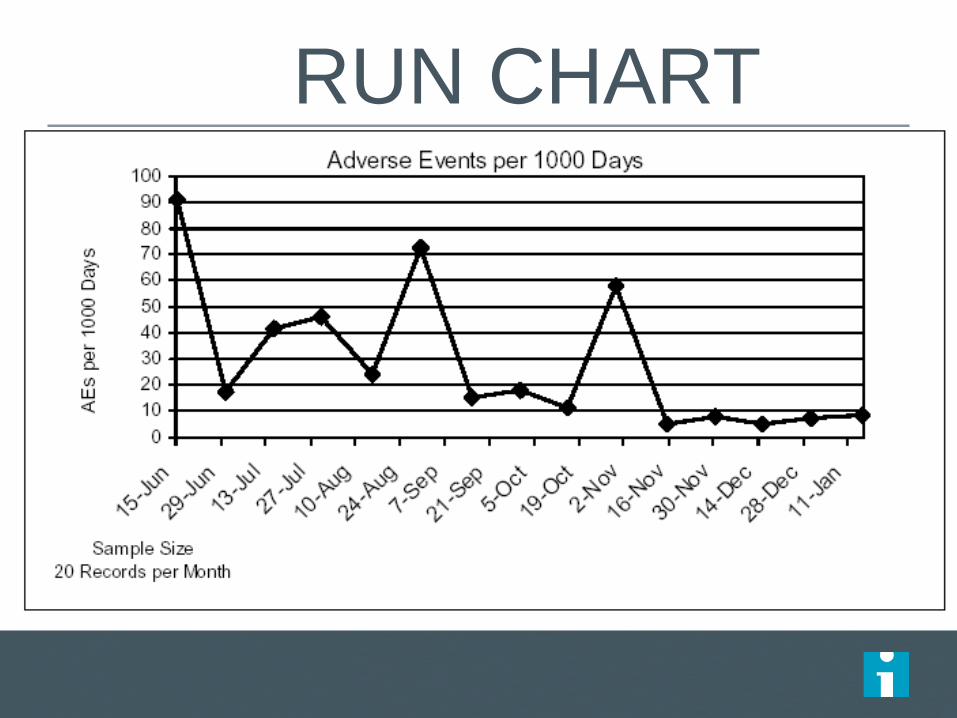
RUN CHART

How long do we measure?Outcomes: ALWAYSProcesses• Daily until stable • Weekly x 6; if stable then: • Biweekly x 4; if stable then:• Monthly x 4; if stable then: • Quarterly, no less.
23
Variation within the clinical area? Manage in the area.Variation across clinical areas? Leadership investigates and manages.
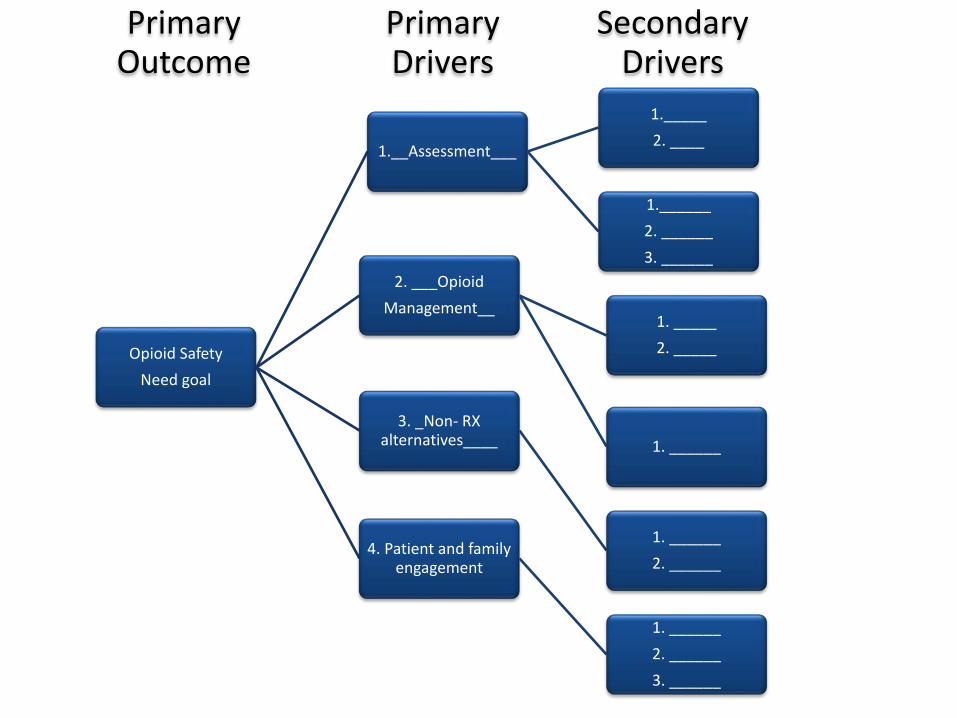
Primary Outcome
Primary Drivers
Secondary Drivers
Opioid Safety Need goal
1.__Assessment___
1._____2. ____
1.______2. ______3. ______
2. ___OpioidManagement__
1. _____2. _____
1. ______3. _Non- RX
alternatives____
1. ______2. ______
4. Patient and family engagement
1. ______2. ______3. ______
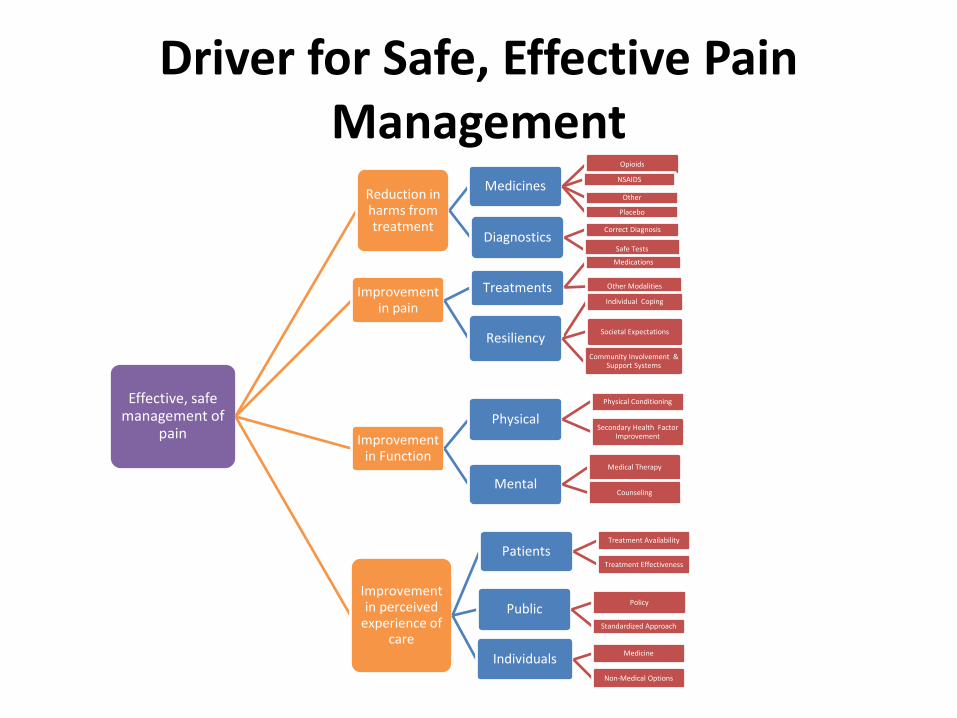
Driver for Safe, Effective Pain Management
Effective, safe management of
pain
Reduction in harms from treatment
Medicines
Opioids
NSAIDS
Other
Placebo
DiagnosticsCorrect Diagnosis
Safe Tests
Improvement in pain
Treatments
Medications
Other Modalities
Resiliency
Individual Coping
Societal Expectations
Community Involvement & Support Systems
Improvement in Function
Physical Physical Conditioning
Secondary Health Factor Improvement
Mental Medical Therapy
Counseling
Improvement in perceived
experience of care
PatientsTreatment Availability
Treatment Effectiveness
Public Policy
Standardized Approach
Individuals Medicine
Non-Medical Options
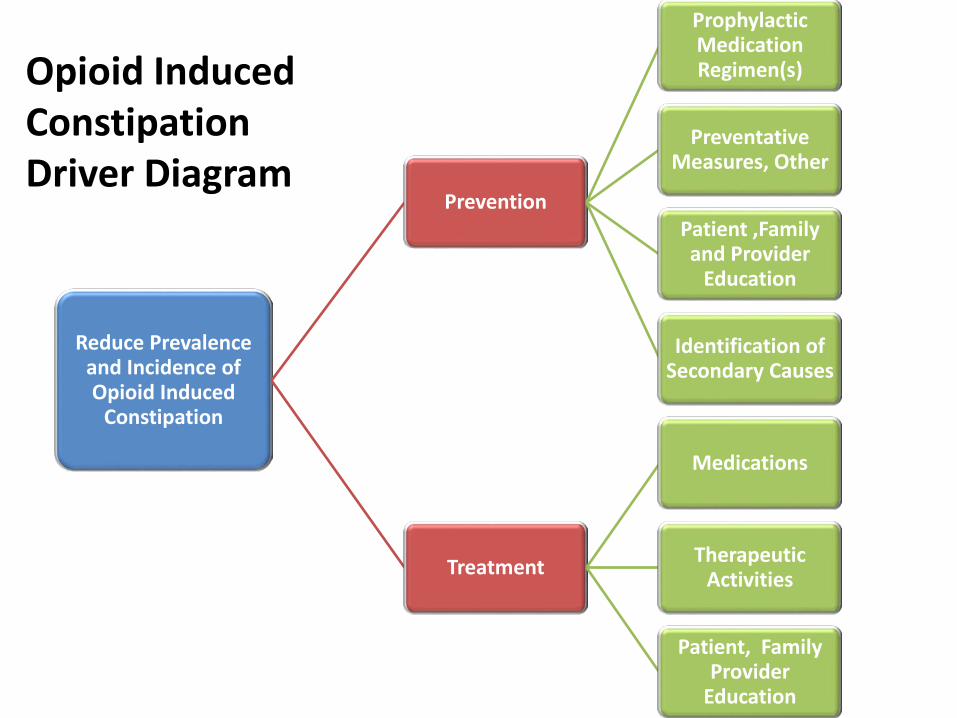
Opioid Induced Constipation Driver Diagram
Reduce Prevalence and Incidence of Opioid Induced
Constipation
Prevention
Prophylactic Medication Regimen(s)
Preventative Measures, Other
Patient ,Family and Provider
Education
Identification of Secondary Causes
Treatment
Medications
Therapeutic Activities
Patient, Family Provider
Education
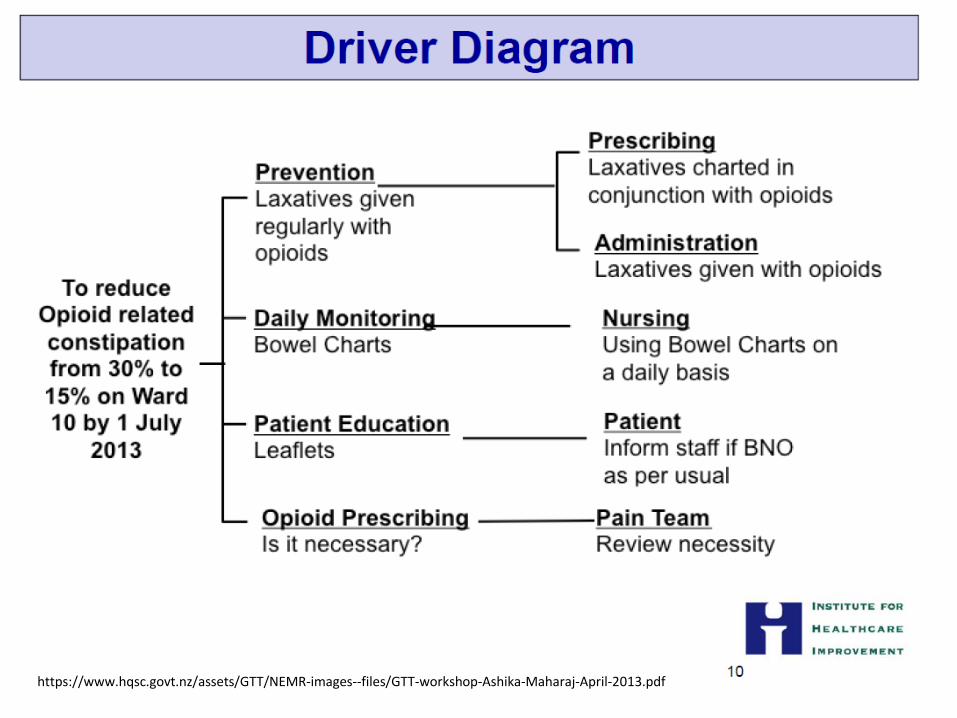
https://www.hqsc.govt.nz/assets/GTT/NEMR-images--files/GTT-workshop-Ashika-Maharaj-April-2013.pdf

Improving Opioid SafetySegment the population. Begin by working with patients whose treatment is initiated in-house. This does not imply that all patients should not receive the same care. Once your team has implemented improvements with this group, spread the improvements to other groups.Start by designing for a homogeneous population and control as many variables as possible to test the design. Use small tests of change to test the design. (See the Model for Improvement.Measure the process; if the science is right, the outcomes will follow.Use standard approaches such as order sets, but remember that these
alone will not accomplish the goal. Develop the order sets using evidence-based medicine and society guidelines
How-to Guide: Prevent Harm from High-Alert Medications Institute for Healthcare Improvement
Postoperative Induced Respiratory Depression (POIRD)
48 million inpatient procedures performed annually in the U.S. Undetected critical POIRD results in respiratory failure and cardiac arrest.– Hypoxic injury or death in 80% of cases.
As many as 113 events per 1000 patients. – By strict OIRD diagnostic criteria, incidence may be as
high as 41%!Opioid induced respiratory depression can occur any time a patient has an opioid agent in their system. – Effects occur minutes to days after opioid initiation.
John Kruger Source
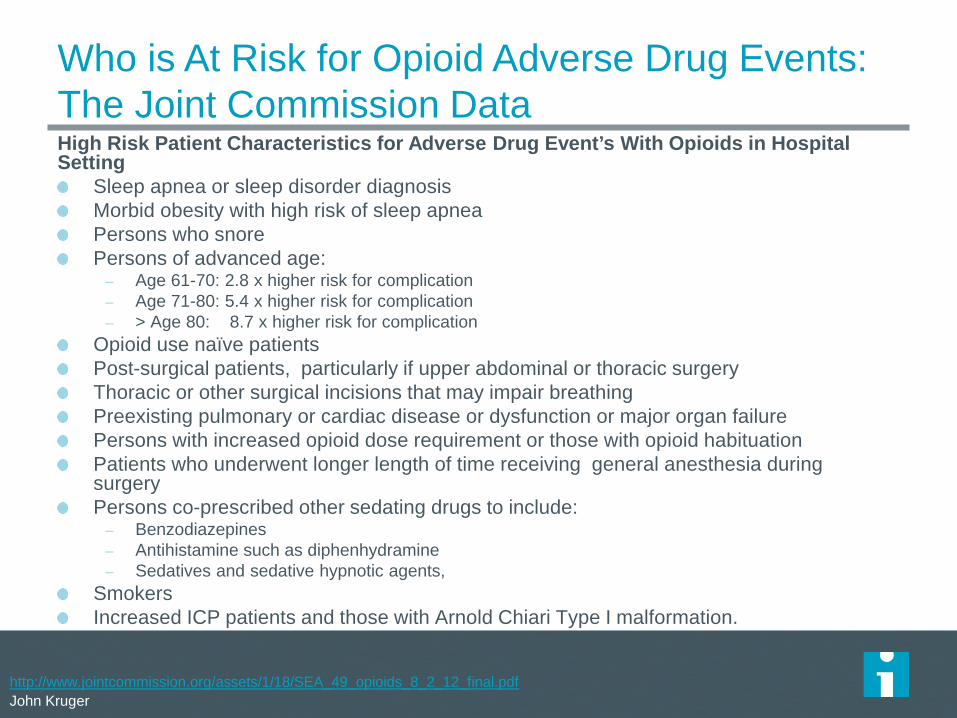
Who is At Risk for Opioid Adverse Drug Events: The Joint Commission DataHigh Risk Patient Characteristics for Adverse Drug Event’s With Opioids in Hospital Setting
Sleep apnea or sleep disorder diagnosisMorbid obesity with high risk of sleep apnea Persons who snorePersons of advanced age:
– Age 61-70: 2.8 x higher risk for complication– Age 71-80: 5.4 x higher risk for complication– > Age 80: 8.7 x higher risk for complication
Opioid use naïve patientsPost-surgical patients, particularly if upper abdominal or thoracic surgery Thoracic or other surgical incisions that may impair breathingPreexisting pulmonary or cardiac disease or dysfunction or major organ failurePersons with increased opioid dose requirement or those with opioid habituation Patients who underwent longer length of time receiving general anesthesia during surgery Persons co-prescribed other sedating drugs to include:
– Benzodiazepines– Antihistamine such as diphenhydramine– Sedatives and sedative hypnotic agents,
SmokersIncreased ICP patients and those with Arnold Chiari Type I malformation.
Source: The Joint Commission Sentinel Event Alert. Issue 49, August 8, 2012(Multiple Contributing Sources Referenced and Found at: http://www.jointcommission.org/assets/1/18/SEA_49_opioids_8_2_12_final.pdf John Kruger SourceJohn Kruger Source






























