Embed Size (px)
Citation preview
Reducing the Risk of Adverse Drug Events in Older Patients
Nicole Slater, PharmD, BCACPJuly 14, 2018Consultant Certification and Geriatric Pharmacotherapy

DISCLOSURE/CONFLICT OF INTEREST
I, __Nicole Slater________, have no actual or potential conflict of interest in relation to this program.

OBJECTIVES
At the completion of this knowledge-based activity, the participant will be able to: Define polypharmacy.
Identify common errors made when prescribing medications for the elderly population.
Recognize key recommendations in the BEER’s Criteria guidelines.
Optimize the patient’s drug therapy, given a case scenario.

MEDICATION REVIEWS IN THE OLDERPOPULATION…WHY ARE THEY NEEDED?
Increase in co-morbid disease states
Physiological changes
Increased susceptibility to: Polypharmacy
Drug interactions
Adverse drug reactions
Poor compliance
Potentially inappropriate prescribing

INAPPROPRIATE PRESCRIBING
Under-prescribing Not giving clinically indicated therapies despite no contraindication
to use
Mis-prescribing Unfavorable choice of medication therapies, dose, or duration for
use
Over-prescribing Excessive medication use
Higher doses than necessary
Longer durations than needed
Polypharmacy

SOME EXAMPLES OF OVER-PRESCRIBING
NSAID HTN Anti-HTN med
HCTZ Gout Allopurinol
Amlodipine Edema Diuretics

HOW MANY IS TOO MANY?
How many medications must an older adult take in order to put him or her at risk for polypharmacy? 3 5 10 15

POLYPHARMACY
There is no set definition of how many medications constitute polypharmacy but some studies suggest more than 5, while others suggest more than 7 or 10.

COMPLEX MEDICATION REGIMENS
Large number of medications Expensive medications Complex or frequency of dosing schedule Adverse reactions experienced Confusion related to brand/generic Difficult to open containers Other routes of administration (rectal, vaginal, subQ) Limited patient education

“BUT I BOUGHT IT OVER-THE-COUNTER”
Self-medicating complicates Polypharmacy
OTC, Vitamins, and Herbals ARE STILL MEDICATIONS and COUNT
Use of OTC’s are highly prevalent among the older adult population
Generally NOT reported to the providers
Serious drug-interaction potential

OUR BODIES CHANGE!?
Which of the following physiological changes is most likely to cause an adverse drug event in the older patient? Decreased fat tissue Increased hepatic metabolism Decline in renal function Alteration in gastric pH
PHARMACOKINETICS
Absorption Bioavailability: The fraction of a drug dose reaching the systemic
circulation that affects the body
Distribution Locations in the body where a drug penetrates (i.e fat tissue)
Metabolism Conversion of a drug to alternative compounds which may or may
not be pharmacologically active
Elimination The final route of exit for a drug, which is expressed in half-life or
clearance

AGING PHYSIOLOGICAL CHANGES
Important Physiological changes Absorption: Increased gastric pH, delayed gastric emptying
Distribution: Changes in lean body weight and body fat can alter distribution to different body compartments Malnutrition can affect protein binding potential
More body fat and less muscle mass
Hepatic metabolism: Typically decreases by roughly 40% in the older adult A decline in first-pass clearance causes build up of toxic medications
including warfarin and opioids
Renal elimination: Typically decreases up to 50% by age 80, but will differ in each individual
Substance abuse can also effect drug metabolism (mainly alcohol) when the liver is impaired from long-standing use

AGING PHARMACODYNAMIC CHANGES
Dopaminergic (dopamine) Age related decrease in dopamine turnover = increased
parkinsonism
Serotonergic (serotonin) Decreased 5-HT receptors and serotonin = more depression seen
Norepinephrinic (Nor-Epi) Decrease in Nor-Epi leads to sluggishness
Cholinergic (acetylcholine) Decrease in acetylcholine = dementia
Gabanergic (gaba) Decrease in gaba = hyper-excitability

MONITORING PK AND PD CHANGES
Generally result in decreased clearance of drugs which leads to increased sensitivity to many medications
Lower doses, longer intervals, and slower titrations are recommended to prevent intolerance and/or toxicity
Monitor older patients more often and more closely with medication therapies
Consider non-pharmacologic therapy when able
Balance over- vs. under prescribing

CLINICAL TOOLS TO HELP YOU
The BEERS Criteria Accessible on the American Geriatrics Society Website:
http://www.americangeriatrics.org
STOPP and START Criteria Accessible online at
http://www.ncbi.nlm.gov/pmc/articles/PMC2810806/.

SO HOW DO I KNOW WHAT IS BEST FORTHE PATIENT?
Which of the following was designed to assist prescribers in identifying omissions in therapy for an older adult? The Beer’s List The START Criteria The STOPP Criteria The DE-prescribing algorithm

THE BEER’S CRITERIA
Most widely used consensus data for POTENTIALLY inappropriate medication use in the elderly Goal is to help reduce the risk of adverse events
Utilization intended for ambulatory, acute, and institutional settings
Not recommended for hospice or palliative cases
Published first in 1991
Last updated 2015

POCKET CARD
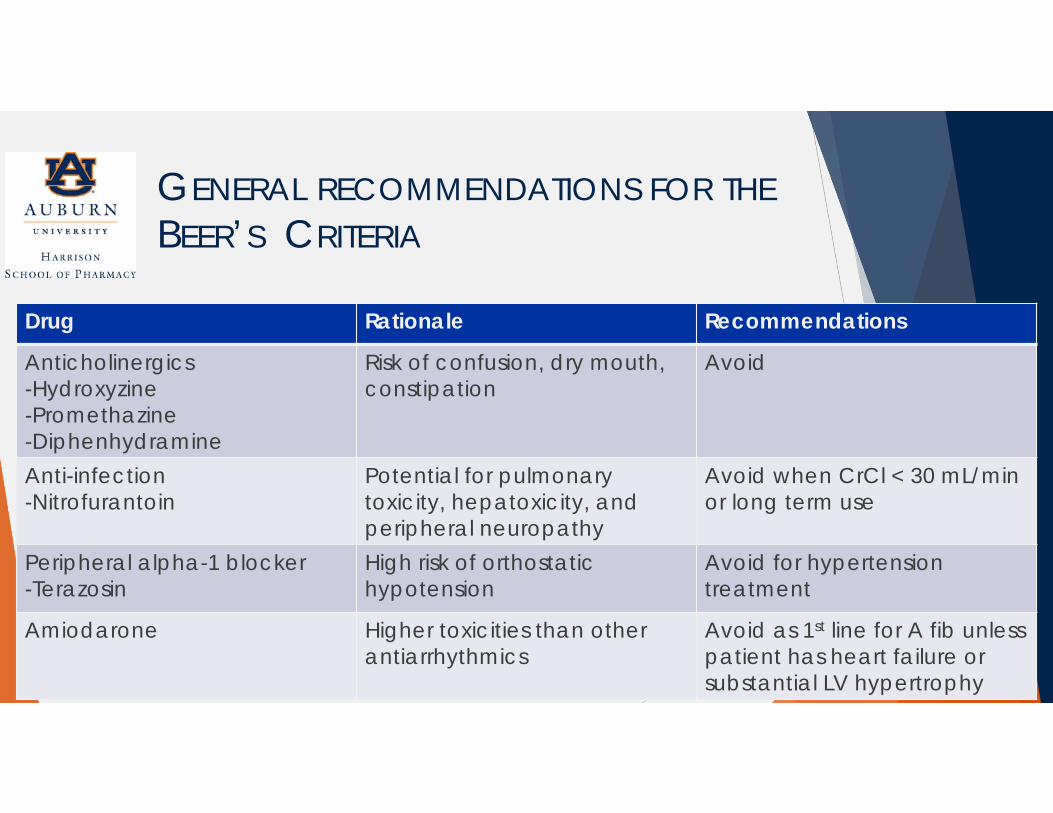
GENERAL RECOMMENDATIONS FOR THEBEER’S CRITERIA
Drug Rationale Recommendations
Anticholinergics-Hydroxyzine-Promethazine-Diphenhydramine
Risk of confusion, dry mouth, constipation
Avoid
Anti-infection-Nitrofurantoin
Potential for pulmonary toxicity, hepatoxicity, and peripheral neuropathy
Avoid when CrCl < 30 mL/min or long term use
Peripheral alpha-1 blocker-Terazosin
High risk of orthostatichypotension
Avoid for hypertension treatment
Amiodarone Higher toxicities than other antiarrhythmics
Avoid as 1st line for A fib unless patient has heart failure or substantial LV hypertrophy

GENERAL RECOMMENDATIONSCONTINUED…
Drug Rationale Recommendation
Antipsychotics-convention and atypical
Increase risk of cerebrovascular accident and greater rate of cognitive decline and mortality in persons with dementia
Avoid, except for schizophrenia, bipolar, or short-term antiemetic in chemotherapy
Benzodiazepines short-acting-Lorazepam-Temazepam
Increase risk of cognitiveimpairment, delirium, falls, fractures and MVA
Avoid
Benzodiazepines long-acting-Clonazepam-Diazepam-Flurazepam
Increase cognitive impairment, delirium, falls, fractures and MVA
May be appropriate for seizure disorders, severe GAD, REM Sleep disorders

GENERAL RECOMMENDATIONSCONTINUED…
Drug Rationale Recommendation
PPI’s-Omeprazole
Risk of Clostridium difficileinfection, bone loss, and fractures
Avoid schedule use for > 8 weeks unless high risk
Insulin sliding scale Higher risk of hypoglycemia without improvement in hyperglycemia regardless of care setting
Avoid
Testosterone Potential for cardiac problems, contraindicated in prostate cancer
Avoid, unless indicated for confirmed hypogonadism with clinical symptoms

BEERS CRITERIAKEY PRINCIPLES TO GUIDE OPTIMAL USE
1. Medications in the AGS 2015 Beers Criteria are potentially inappropriate, not definitely inappropriate
2. Read the rationale and recommendations statements for each criterion. The caveats and guidance listed there are important
3. Understand why medications are included in the AGS 2015 Beers Criteria, and adjust your approach to those medications accordingly
4. Optimal application of the AGS 2015 Beers Criteria involves identifying potentially inappropriate medications, and where appropriate offering safer non-pharmacologic and pharmacologic therapies
5. The AGS 2015 Beers Criteria should be a starting point for a comprehensive process of identifying and improving medication appropriateness and safety
6. Access to medications included in the AGS 2015 Beers Criteria should not be excessively restricted by prior authorization and/or health plan coverage policies
7. The AGS 2015 Beers Criteria are not equally applicable to all countries

START & STOPP CRITERIA
AIM: to improve medication appropriateness, prevent adverse drug reactions, and reduce drug costs
START: Screening Tool to Alert Doctors to Right Treatments Consider for people over age 65 with certain conditions
where no contraindication exists
Way to identify “omissions” to patient’s med list
STOPP: Screening Tool of Older People’s Potentially Inappropriate Prescriptions Consider for people over age 65 where the medications are
linked to an increase in adverse drug events and hospitalizations
Not comprehensive

START & STOPP CRITERIA
START Cardiovascular system (8) Respiratory system (3) Central Nervous system (2) GI system (2) Musculoskeletal system (3) Endocrine system (4)
STOPP Cardiovascular system (17) Central Nervous system
(13) GI system (5) Musculoskeletal system (8) Respiratory system (3) Urogenital system (6) Endocrine system (4) Analgesics (3) Falling (5) Duplicate classes (1)

CONSIDER STARTING THESE…
Metformin: Patients with Type II diabetes
ACE inhibitor or ARB: Patients with heart failure, post-MI, diabetic nephropathy
Aspirin: Prevention for cardiovascular events in patients with diabetes and one major cardiovascular risk factor
Statin: Patients with cardiovascular disease, cerebrovascular event, or peripheral vascular disease as well as patients with diabetes and one or more additional cardiovascular risk factor
Calcium and vitamin D: Patient with osteoporosis

CONSIDER STOPPING THESE…
Cardiovascular HCTZ with gout history
Aspirin over 150mg
CNS TCA’s
SSRI’s with clinically significant hyponatremia
Musculoskeletal NSAIDS
Falling Benzo’s
First generation antihistamines

CONSEQUENCES OF POLYPHARMACY
Drug-drug interactions Drug-disease interactions Drug-food interactions Drug toxicity Increase hospitalizations/readmissions Increased falls Possible mortality Confusion Side effects/adverse events

ADVERSE DRUG EVENT (ADE)
An injury resulting from medical intervention related to a drug
Unintended effect from a drug that produces symptoms sufficient to cause a person to seek medical attention
May produce symptoms sufficient to affect function or quality of life
Can happen ANYWHERE (hospital, LTCF, outpatient)
Many are preventable
Adverse Drug Reaction (ADR): response to a drug which is noxious and unintended and which occurs at doses normally used in man for prophylaxis, diagnosis, or therapy of disease or for the modification of physiologic function. This is a type of ADE and is different from a side effect

COMMON CULPRITS OF ADE’S
Antipsychotics NSAIDS Insulin Antiplatelet Anticoagulants Diuretics
St. John’s Wort Ginseng Gingko biloba Saw palmetto Kava

COMMON ADVERSE EVENTS IN THEOLDER POPULATION
Falls Fatigue Cognitive decline Constipation/Urinary retention Delirium Pain Insomnia Depression

RECOGNIZING ADVERSE DRUG EVENTS
Many times, these are mistaken for new disease states in elderly patients
Always consider the side effects of the drug
Ask appropriate questions to gather information about the ADE

REPORTING ADVERSE EVENTS/REACTIONS
Med watch Voluntary reporting to the FDA by health care providers and patients
Manufacturer Health care providers and patients may report directly to the
manufacturer who then is responsible for submitting to the FDA
What happens? Product recalls or withdrawal
Black Box Warnings formulated
Contraindications are modified
Monitoring recommendations are created
Med Guides are developed
Letters to health care professionals are disseminated

DE-PRESCRIBING
Should be a shared decision Complete a full medication review first Assess adherence Assess appropriateness with BEERS and START/STOPP Discuss the patient’s preferences and values Explain the goals of therapy Prioritize medication discontinuation Obtain buy-in from the patient Seek guidance from healthcare team members (i.e. pharmacist!)

PATIENT CASE
You, the pharmacist, received a discharge letter from a patient in your practice who was discharged from the hospital 5 days ago after being admitted for an exacerbation of chronic obstructive pulmonary disease (COPD) and was also treated for a Urinary Tract Infection (UTI). SJ is 74 year old WF who is an ex-smoker (1 PPD x 45 years). She also has a medical history of diabetes mellitus and hypertension, which are both controlled at this time. All of her labs and blood studies are WNL. You are asked to perform a medication reconciliation on SJ and determine appropriateness of her medications.
Her medications before hospitalization were are as follows: Metformin 1000mg twice daily Glipizide 10mg twice daily Amlodipine 10mg once daily Tiotropium inhaler (18 micrograms) 1 puff once a day Pro-Air HFA 2 puff every 4 to 6 hours as needed for shortness of breath Citalopram 20mg once daily

MEDICATIONS UPON DISCHARGE
Tiotropium inhaler (18 micrograms) 1 puff once a day Advair Diskus 250/50 1 puff twice a day Albuterol nebulizers 1 every 4 – 6 hours as needed Sliding scale insulin: per instructions given at discharge Glipizide 10mg twice daily Ramipril 10 mg once a day Amlodipine 10 mg once a day Citalopram 20 mg once a day Omeprazole 20mg once a day Temazepam 15 mg at night Prednisolone (short course) 30 mg once a day for 7 days Nitrofurantoin (short course) 100 mg four times a day for 7 days

WHAT CHANGES NEED TO BE MADE?
Review the patient’s medication list and make any recommendations that are potentially inappropriate for this patient. Also consider medications that may need to be started based on her PMH.

QUESTIONS?
Thank you for your time!

REFERENCES
Masnoon N, Shakib S, Kalish-Ellett L, et al. What is polypharmacy? A systematic review of definitions. BMC Geriatrics (2017) 17:230
Pretourius R, Gataric G, Swedlund S, et al. Reducing the Risk of Adverse Drug Events in Older Adults. Am Fam Phys 2013:87(5);331-336.
Lavan A, Gallagher P. Predicting risk of adverse drug reactions in older adults. Ther Adv Drug Saf2016:7(1);11-22.
Hajjar ER, Hanlon JT, Artz MB, et al. Adverse Drug reaction risk factors in older outpatients. Am J GerPharmacotherapy 2003;1(2):82-89
Reporting Adverse Drug Events. Available from: https://www.uspharmacist.com/article/reporting-adverse-drug-events US Pharm. 2010;35:HS-15-HS-19.
Adverse Drug Events: Overview. Available from: https://health.gov/hcq/ade.asp. Accessed 25 June 2018. START and STOPP Criteria: Available from: http://www.ncbi.nlm.gov/pmc/articles/PMC2810806/. BEERS Criteria: Available from: http://www.americangeriatrics.org Deprescribing: Available from: https://deprescribing.org/resources/deprescribing-guidelines-algorithms/ BEERS Criteria pocket card: Available from:
https://geriatricscareonline.org/ProductTypeStore/pocketcards/10/ Mortazavi S, Shati M, Keshtkar A, et al. Defining polypharmacy in the elderly: a systematic review protocol.
BMJ Open 2016;6: e010989. Davies EA, O’Mahony MS. Adverse Drug reactins in special populations-the elderly. British J of Pharmcol
2015; 80(4). Available from: https://bpspubs.onlinelibrary.wiley.com/doi/full/10.1111/bcp.12596
![Advers drug reactions in older people: detection and ...drug-drug and drug-disease interactions.[27] As an illustration, patients taking two drugs face a 13% risk of adverse drug-drug](https://img.pdfslide.net/doc/110x75/5ed937ab6714ca7f47695c3a/advers-drug-reactions-in-older-people-detection-and-drug-drug-and-drug-disease.jpg)














