Embed Size (px)
Citation preview
Disclosures: Geert Dom ! Speakers fee: J&J, Lundbeck, GSK, Astrazeneca,
Pfizer, Merck, Eli Lily.
! Scientific Advisory Board: Lundbeck
Inhoud presentatie ! Behandeling alcohol: problemen
! Reductie gebruik een nieuw concept ?
! Reductie haalbaar ?
! Reductie waar best inzetbaar
Inhoud presentatie ! Behandeling alcohol: problemen
! Reductie gebruik een nieuw concept ?
! Reductie haalbaar ?
! Reductie waar best inzetbaar
! Kennis vooral gebaseerd op kleine subgroep van alcohol afhankelijke patienten in behandeling.
! Effectiviteit behandelingen matig
! Treatment-gap
Problemen alcohol behandeling
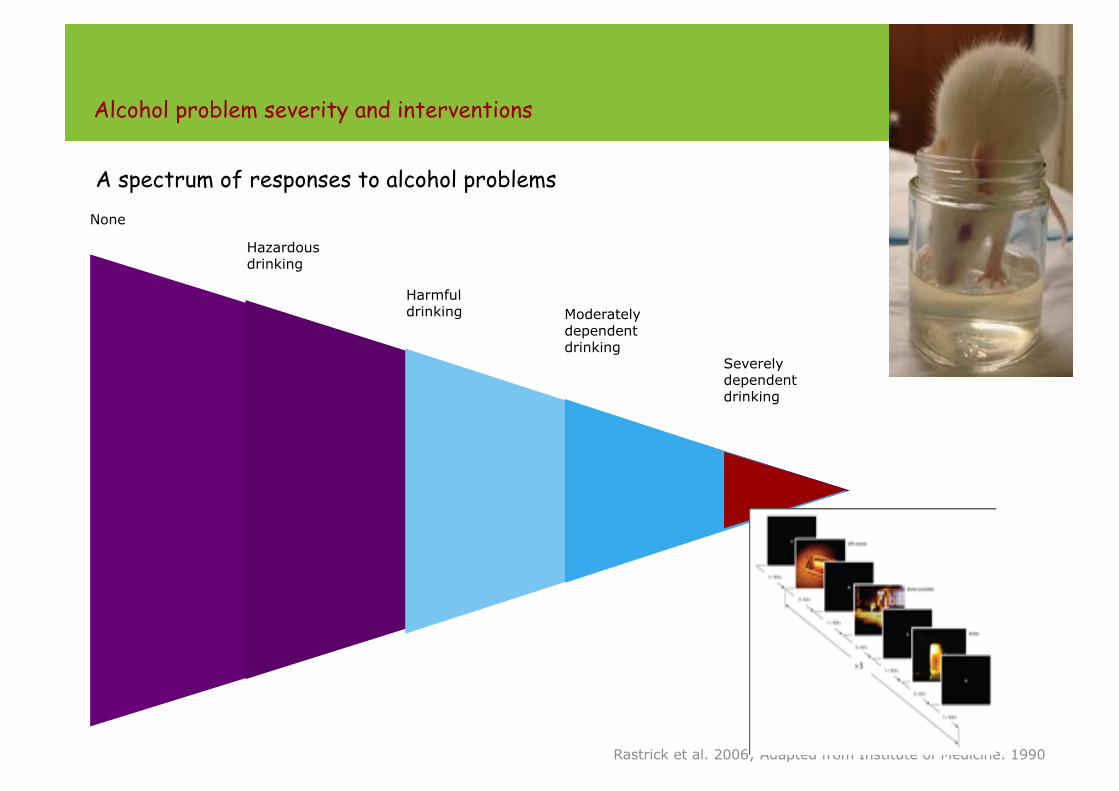
Alcohol problem severity and interventions
A spectrum of responses to alcohol problems None
Hazardous drinking
Harmful drinking Moderately
dependent drinking
Severely dependent drinking
Rastrick et al. 2006; Adapted from Institute of Medicine. 1990
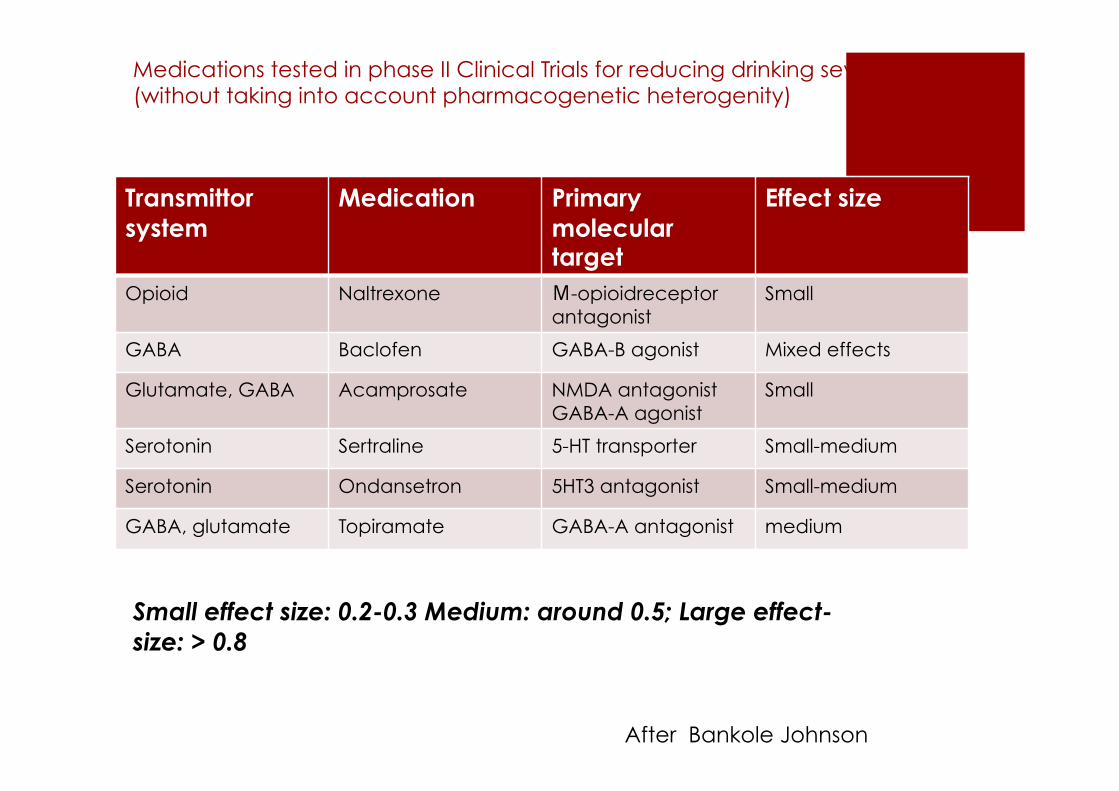
Medications tested in phase II Clinical Trials for reducing drinking severity (without taking into account pharmacogenetic heterogenity)
Transmittor system
Medication Primary molecular target
Effect size
Opioid Naltrexone Μ-opioidreceptor antagonist
Small
GABA Baclofen GABA-B agonist Mixed effects
Glutamate, GABA Acamprosate NMDA antagonist GABA-A agonist
Small
Serotonin Sertraline 5-HT transporter Small-medium
Serotonin Ondansetron 5HT3 antagonist Small-medium
GABA, glutamate Topiramate GABA-A antagonist medium
Small effect size: 0.2-0.3 Medium: around 0.5; Large effect-size: > 0.8
After Bankole Johnson
! Treatment gap: “To little to late”
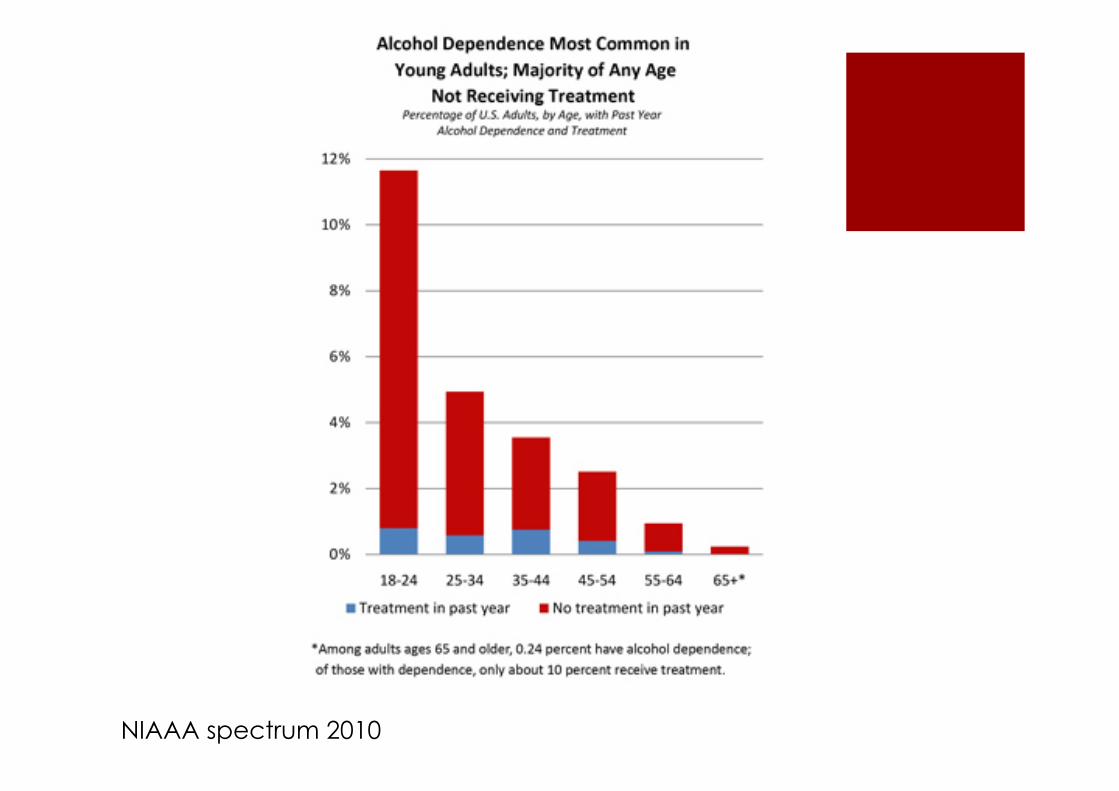
NIAAA spectrum 2010
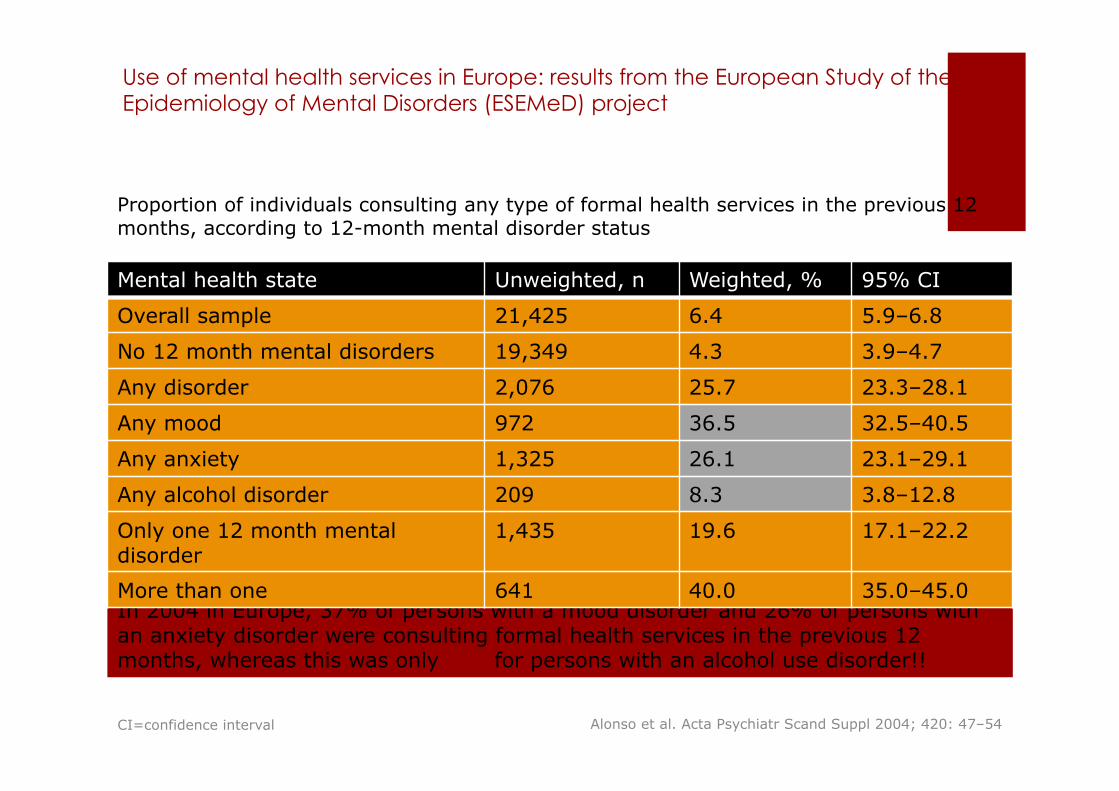
Use of mental health services in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project
In 2004 in Europe, 37% of persons with a mood disorder and 26% of persons with an anxiety disorder were consulting formal health services in the previous 12 months, whereas this was only 8% for persons with an alcohol use disorder!!
Proportion of individuals consulting any type of formal health services in the previous 12 months, according to 12-month mental disorder status
Alonso et al. Acta Psychiatr Scand Suppl 2004; 420: 47–54
Mental health state Unweighted, n Weighted, % 95% CI
Overall sample 21,425 6.4 5.9–6.8
No 12 month mental disorders 19,349 4.3 3.9–4.7
Any disorder 2,076 25.7 23.3–28.1
Any mood 972 36.5 32.5–40.5
Any anxiety 1,325 26.1 23.1–29.1
Any alcohol disorder 209 8.3 3.8–12.8
Only one 12 month mental disorder
1,435 19.6 17.1–22.2
More than one 641 40.0 35.0–45.0
CI=confidence interval
! Stigma
! Kultuur
! Verzekering en betalingssystemen
! Behandel systeem ! Splitsing verslavingszorg - ggz
! Splitsing eertse lijn versus gespecialiseerde zorg
! Beschikbaarheid & toegankelijkheid
! Focus abstinentie
Treatment gap: factoren ?
11

! Stigma ……….> destigmatizing
! Culture …………> changes in policies alcohol
! Insurance & reimbursement systems ……..> parity act !
! Treatment system: ! Splitting addiction care from (mental) health care. ……>integration
(e.g. Flemish initiative). ! First line versus specialized care. ……….> shifting towards first line ! Availability ………> shifting from specialised care only to shared
responsability of all health sysetem ! Focus abstinence ……..> paradigm shift moderation as a valid
treatment goal.
Treatment gap: opportunities
12
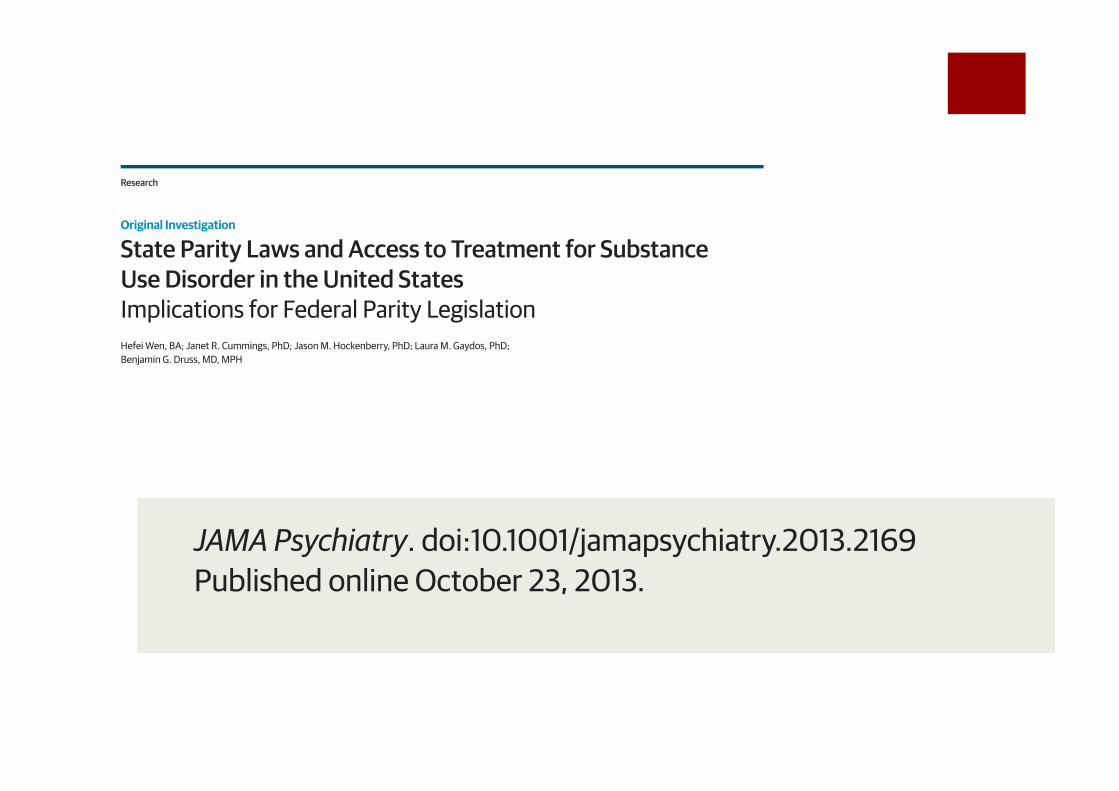
State Parity Laws and Access to Treatment for SubstanceUse Disorder in the United StatesImplications for Federal Parity LegislationHefei Wen, BA; Janet R. Cummings, PhD; Jason M. Hockenberry, PhD; Laura M. Gaydos, PhD;Benjamin G. Druss, MD, MPH
IMPORTANCE The passage of the 2008 Mental Health Parity and Addiction Equity Act and the2010 Affordable Care Act incorporated parity for substance use disorder (SUD) treatmentinto federal legislation. However, prior research provides us with scant evidence as towhether federal parity legislation will hold the potential for improving access to SUDtreatment.
OBJECTIVE To examine the effect of state-level SUD parity laws on state-aggregate SUDtreatment rates and to shed light on the impact of the recent federal SUD parity legislation.
DESIGN, SETTING, AND PARTICIPANTS We conducted a quasi-experimental study using a2-way (state and year) fixed-effect method. We included all known specialty SUD treatmentfacilities in the United States and examined treatment rates from October 1, 2000, throughMarch 31, 2008. Our main source of data was the National Survey of Substance AbuseTreatment Services, which provides facility-level information on specialty SUD treatment.
INTERVENTIONS State-level SUD parity laws during the study period.
MAIN OUTCOMES AND MEASURES State-aggregate SUD treatment rates in (1) all specialty SUDtreatment facilities and (2) specialty SUD treatment facilities accepting private insurance.
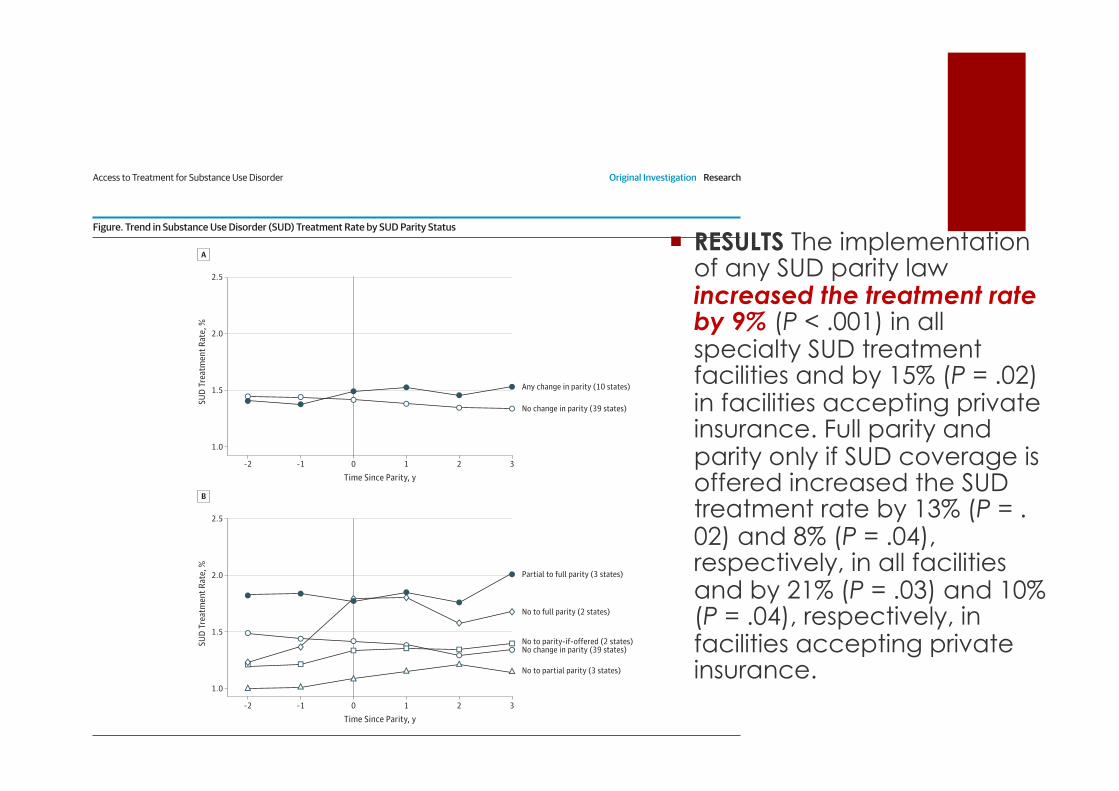
RESULTS The implementation of any SUD parity law increased the treatment rate by 9%(P < .001) in all specialty SUD treatment facilities and by 15% (P = .02) in facilities acceptingprivate insurance. Full parity and parity only if SUD coverage is offered increased the SUDtreatment rate by 13% (P = .02) and 8% (P = .04), respectively, in all facilities and by 21%(P = .03) and 10% (P = .04), respectively, in facilities accepting private insurance.
CONCLUSIONS AND RELEVANCE We found a positive effect of the implementation of stateSUD parity legislation on access to specialty SUD treatment. Furthermore, the positiveassociation is more pronounced in states with more comprehensive parity laws. Our findingssuggest that federal parity legislation holds the potential to improve access to SUDtreatment.
JAMA Psychiatry. doi:10.1001/jamapsychiatry.2013.2169Published online October 23, 2013.
Supplemental content atjamapsychiatry.com
Author Affiliations: Department ofHealth Policy and Management,Rollins School of Public Health,Emory University, Atlanta, Georgia(Wen, Cummings, Hockenberry,Gaydos, Druss); currently with Centerfor Comprehensive Access andDelivery Research and EvaluationCenter, Iowa City Veterans AffairsHealth Care System, Iowa City, Iowa(Hockenberry).
Correspondence: Hefei Wen, BA,Department of Health Policy andManagement, Rollins School of PublicHealth, Emory University, 1518 CliftonRd NE, Room 623, Atlanta, GA 30322([email protected]).
Research
Original Investigation
E1
Downloaded From: http://archpsyc.jamanetwork.com/ by a Universiteit Antwerpen User on 10/28/2013
State Parity Laws and Access to Treatment for SubstanceUse Disorder in the United StatesImplications for Federal Parity LegislationHefei Wen, BA; Janet R. Cummings, PhD; Jason M. Hockenberry, PhD; Laura M. Gaydos, PhD;Benjamin G. Druss, MD, MPH
IMPORTANCE The passage of the 2008 Mental Health Parity and Addiction Equity Act and the2010 Affordable Care Act incorporated parity for substance use disorder (SUD) treatmentinto federal legislation. However, prior research provides us with scant evidence as towhether federal parity legislation will hold the potential for improving access to SUDtreatment.
OBJECTIVE To examine the effect of state-level SUD parity laws on state-aggregate SUDtreatment rates and to shed light on the impact of the recent federal SUD parity legislation.
DESIGN, SETTING, AND PARTICIPANTS We conducted a quasi-experimental study using a2-way (state and year) fixed-effect method. We included all known specialty SUD treatmentfacilities in the United States and examined treatment rates from October 1, 2000, throughMarch 31, 2008. Our main source of data was the National Survey of Substance AbuseTreatment Services, which provides facility-level information on specialty SUD treatment.
INTERVENTIONS State-level SUD parity laws during the study period.
MAIN OUTCOMES AND MEASURES State-aggregate SUD treatment rates in (1) all specialty SUDtreatment facilities and (2) specialty SUD treatment facilities accepting private insurance.
RESULTS The implementation of any SUD parity law increased the treatment rate by 9%(P < .001) in all specialty SUD treatment facilities and by 15% (P = .02) in facilities acceptingprivate insurance. Full parity and parity only if SUD coverage is offered increased the SUDtreatment rate by 13% (P = .02) and 8% (P = .04), respectively, in all facilities and by 21%(P = .03) and 10% (P = .04), respectively, in facilities accepting private insurance.
CONCLUSIONS AND RELEVANCE We found a positive effect of the implementation of stateSUD parity legislation on access to specialty SUD treatment. Furthermore, the positiveassociation is more pronounced in states with more comprehensive parity laws. Our findingssuggest that federal parity legislation holds the potential to improve access to SUDtreatment.
JAMA Psychiatry. doi:10.1001/jamapsychiatry.2013.2169Published online October 23, 2013.
Supplemental content atjamapsychiatry.com
Author Affiliations: Department ofHealth Policy and Management,Rollins School of Public Health,Emory University, Atlanta, Georgia(Wen, Cummings, Hockenberry,Gaydos, Druss); currently with Centerfor Comprehensive Access andDelivery Research and EvaluationCenter, Iowa City Veterans AffairsHealth Care System, Iowa City, Iowa(Hockenberry).
Correspondence: Hefei Wen, BA,Department of Health Policy andManagement, Rollins School of PublicHealth, Emory University, 1518 CliftonRd NE, Room 623, Atlanta, GA 30322([email protected]).
Research
Original Investigation
E1
Downloaded From: http://archpsyc.jamanetwork.com/ by a Universiteit Antwerpen User on 10/28/2013
cialty SUD treatment facilities and 1.10 percentage points in fa-cilities accepting private insurance, changes of 0.13 and 0.16percentage points, respectively, can be translated into a 9% in-crease in the overall SUD treatment rate (ie, 9% = 0.13 ÷ 1.40),and a 15% increase in the SUD treatment rate for facilities ac-cepting private insurance (ie, 15% = 0.16 ÷ 1.10).
When considering the comprehensiveness of the parity leg-islation (Table 3), full parity and parity-if-offered increased theSUD treatment rate by 13% (model 1.2, ME = 0.18 percentagepoints [95% CI, 0.03-0.33]) and 8% (model 1.2, 0.12 [0.00-0.23]), respectively, in all facilities and by 21% (model 2.2, 0.23[0.03-0.43]) and 10% (model 2.2, 0.11 [0.00-0.22]), respec-tively, in those accepting private insurance. The influence ofpartial parity on the treatment rate was not statistically sig-nificant across models.
Discussion
Our findings indicate that the implementation of state SUD par-ity legislation results in a significant improvement in accessto specialty SUD treatment. The implementation of any SUDparity law increased the treatment rate by 9% in all specialtySUD treatment facilities and by 15% in facilities accepting pri-vate insurance. Our study contributes to the existing litera-ture by using state-level panel data on a nearly complete enu-meration of all treatment counts in specialty SUD treatmentfacilities, harnessing all legislative changes in state-level SUDparity laws during the study period, and tailoring a rigorousquasi-experimental design to this series of state experi-ments.
Figure. Trend in Substance Use Disorder (SUD) Treatment Rate by SUD Parity Status
1.5
2.0
1.5
1.0
2.5
2.0
SUD
Trea
tmen
t Rat
e, %
Time Since Parity, y
A
–2 –1 0 1 2 3
No change in parity (39 states)
Any change in parity (10 states)
1.0
2.5
SUD
Trea
tmen
t Rat
e, %
Time Since Parity, y
B
–2 –1 0 1 2 3
No change in parity (39 states)No to parity-if-offered (2 states)
No to partial parity (3 states)
Partial to full parity (3 states)
No to full parity (2 states)
A, Any change in parity compared with no change. B, All changes in parityranging from none to full. State-aggregate SUD treatment rates reflect thepreparity and postparity periods. We centered the year each state started toimplement the law at time 0. The vertical line represents the year during whicheach state started to implement or extend the law, and it corresponds with theperiod covered in National Survey of Substance Abuse Treatment Services(N-SSATS) from April 2001 to March 2002 (N-SSATS 2002) for Delaware andMichigan; April 2002 to March 2003 (N-SSATS 2003) for Montana and RhodeIsland; April 2003 to March 2004 (N-SSATS 2004) for Maine and NewHampshire; April 2004 to March 2005 (N-SSATS 2005) for Wisconsin and WestVirginia; and April 2006 to March 2007 (N-SSATS 2007) for Oregon. Kentucky
implemented parity during the gap year between N-SSATS 2000 and 2002, sotime 0 consisted of 9 data points instead of 10. For the other states with nochange in parity, the treatment rates during N-SSAT 2002, 2003, 2004, 2005,and 2007 were weighted by 2/9, 2/9, 2/9, 2/9, and 1/9, respectively, to matchthe proportions of the states that implemented parity in a given year. Followingthe same procedure, we determined times −2, −1, 1, 2, and 3 for the states withany change in parity, and then transferred states with no change in parity to thecorresponding time in accord with the parity states. Only 7 states with anychange in parity were included for time −2 (no data for Kentucky, Deleware, orMichigan), time 2 (no data for Oregon), and time 3 (no data for Oregon).
Access to Treatment for Substance Use Disorder Original Investigation Research
jamapsychiatry.com JAMA Psychiatry Published online October 23, 2013 E5
Downloaded From: http://archpsyc.jamanetwork.com/ by a Universiteit Antwerpen User on 10/28/2013
! RESULTS The implementation of any SUD parity law increased the treatment rate by 9% (P < .001) in all specialty SUD treatment facilities and by 15% (P = .02) in facilities accepting private insurance. Full parity and parity only if SUD coverage is offered increased the SUD treatment rate by 13% (P = .02) and 8% (P = .04), respectively, in all facilities and by 21% (P = .03) and 10% (P = .04), respectively, in facilities accepting private insurance.
Abstinence can be a barrier to treatment
“Refusing to offer treatment for patients who are unable or unwilling to commit to abstinence
sets up a high-threshold barrier”
Owen & Marlatt. Am J Addict 2001;10:289–295
Inhoud presentatie ! Behandeling alcohol: problemen
! Reductie gebruik een nieuw concept ?
! Reductie haalbaar ?
! Reductie waar best inzetbaar
Nieuw idee ?? ! Miller, W.R. (1983). Motivational interviewing with
problem drinkers. Behavioural Psychotherapy, 11, 147-172.
! >> conflict residentiele zorg
! Eigen ervaring: ! 1992-1994: opname afdeling:
! harmreduction
! 1997-2013: dagbehandeling (+/- 750 )
! “beter gekaderde patient”
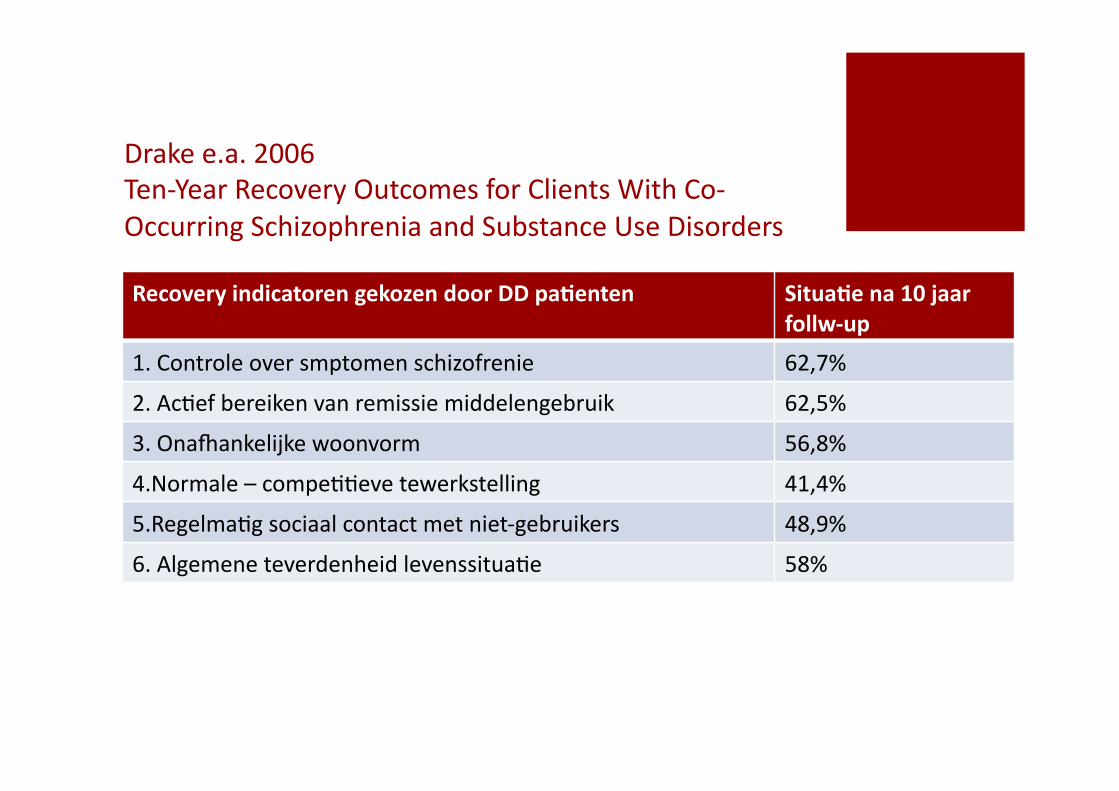
Drake e.a. 2006 Ten-‐Year Recovery Outcomes for Clients With Co-‐Occurring Schizophrenia and Substance Use Disorders
Recovery indicatoren gekozen door DD pa3enten Situa3e na 10 jaar follw-‐up
1. Controle over smptomen schizofrenie 62,7%
2. AcKef bereiken van remissie middelengebruik 62,5%
3. OnaNankelijke woonvorm 56,8%
4.Normale – compeKKeve tewerkstelling 41,4%
5.RegelmaKg sociaal contact met niet-‐gebruikers 48,9%
6. Algemene teverdenheid levenssituaKe 58%
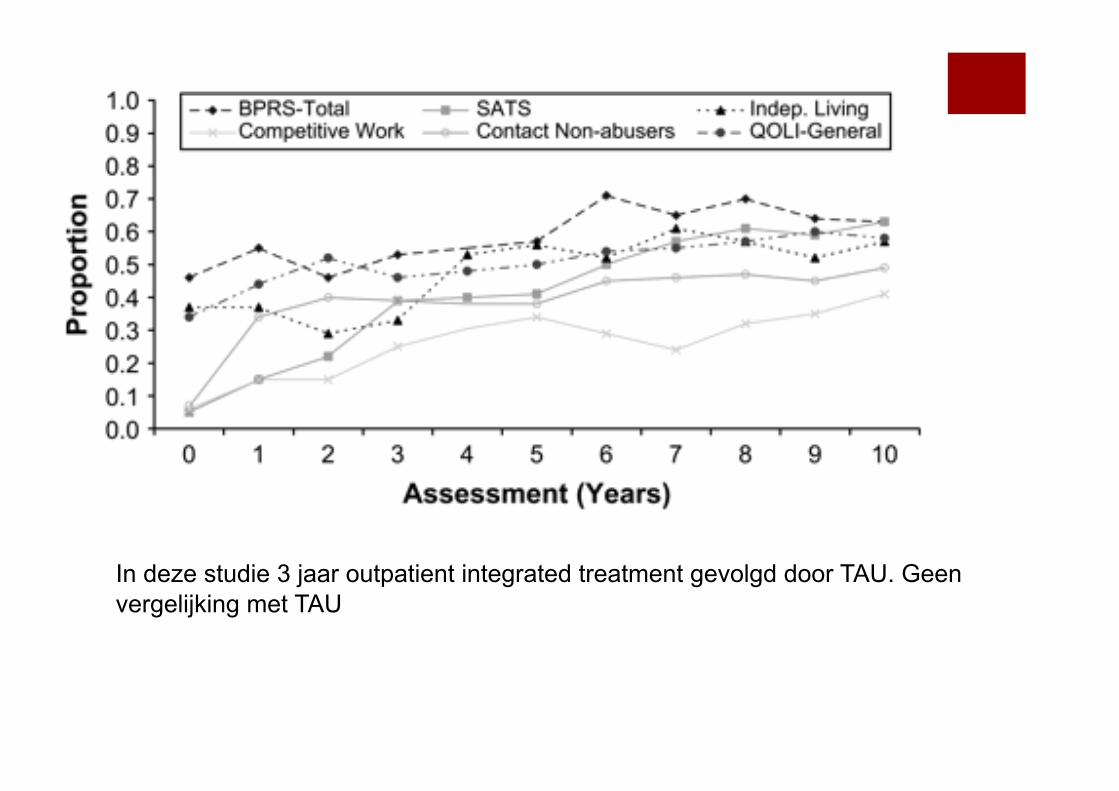
In deze studie 3 jaar outpatient integrated treatment gevolgd door TAU. Geen vergelijking met TAU
! Voordelen niveau volksgezondheid
! Beter aansluiten keuze van patient
! Aanvaard binnen het professionele werkveld
! Haalbaar en werkbaar
! Psychosocial interventions
! Pharmacologic interventions
Reductie als behandeldoel
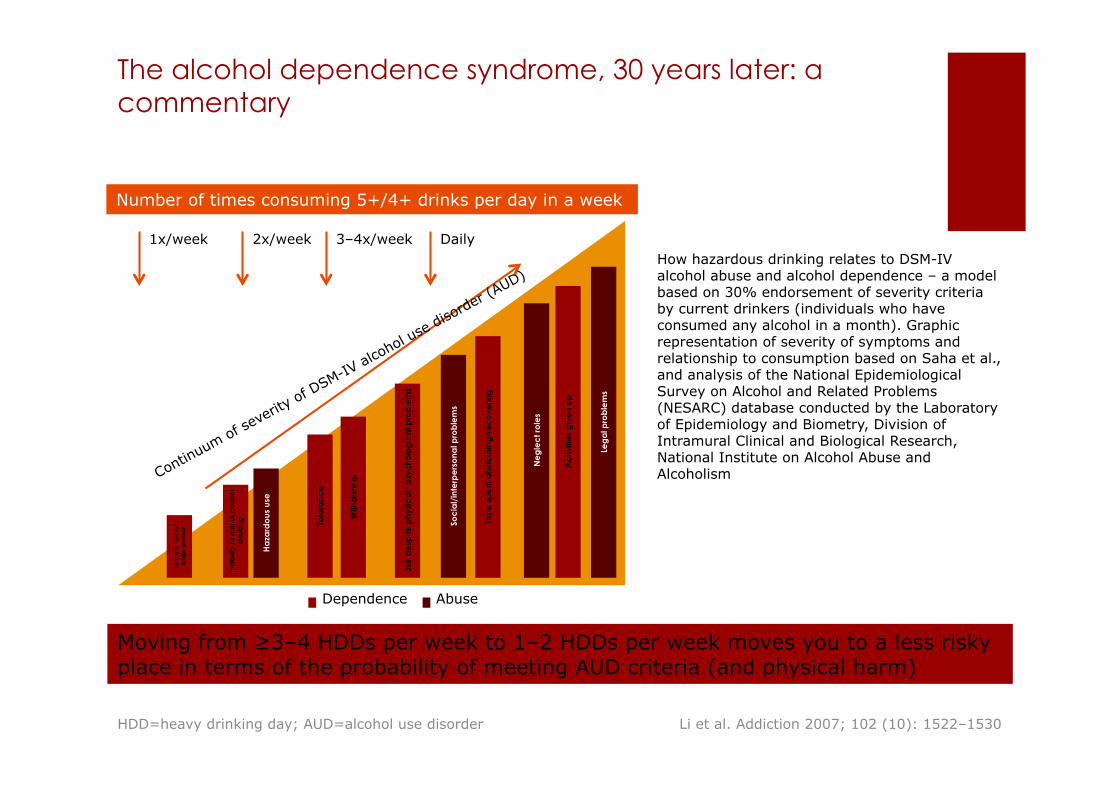
The alcohol dependence syndrome, 30 years later: a commentary
Moving from ≥3–4 HDDs per week to 1–2 HDDs per week moves you to a less risky place in terms of the probability of meeting AUD criteria (and physical harm)
Li et al. Addiction 2007; 102 (10): 1522–1530
How hazardous drinking relates to DSM-IV alcohol abuse and alcohol dependence – a model based on 30% endorsement of severity criteria by current drinkers (individuals who have consumed any alcohol in a month). Graphic representation of severity of symptoms and relationship to consumption based on Saha et al., and analysis of the National Epidemiological Survey on Alcohol and Related Problems (NESARC) database conducted by the Laboratory of Epidemiology and Biometry, Division of Intramural Clinical and Biological Research, National Institute on Alcohol Abuse and Alcoholism
Number of times consuming 5+/4+ drinks per day in a week
1x/week 2x/week 3–4x/week Daily
Larg
er a
mo
unts
/ lo
nge
r pe
riod
s
Ina
bili
ty to
qui
t or c
ont
rol
drin
king
Tole
ranc
e
With
dra
wa
l
Use
de
spite
phy
sic
al/
psy
cho
log
ica
l pro
ble
ms
Tim
e s
pe
nt a
bst
ain
ing
/re
co
verin
g
Ac
tiviti
es
giv
en
up
Ha
zard
ous
use
Soc
ial/
inte
rpe
rso
nal p
rob
lem
s
Ne
gle
ct r
ole
s
Leg
al p
rob
lem
s Dependence Abuse
HDD=heavy drinking day; AUD=alcohol use disorder
NATIONAL HEALTH AND MEDIC AL RESEARCH COUNCIL | 45
AUSTRALIAN GUIDELINES TO REDUCE HEALTH RISKS FROM DRINKING ALCOHOL
Guideline 1: Reducing the risk of alcohol-related harm over a lifetime
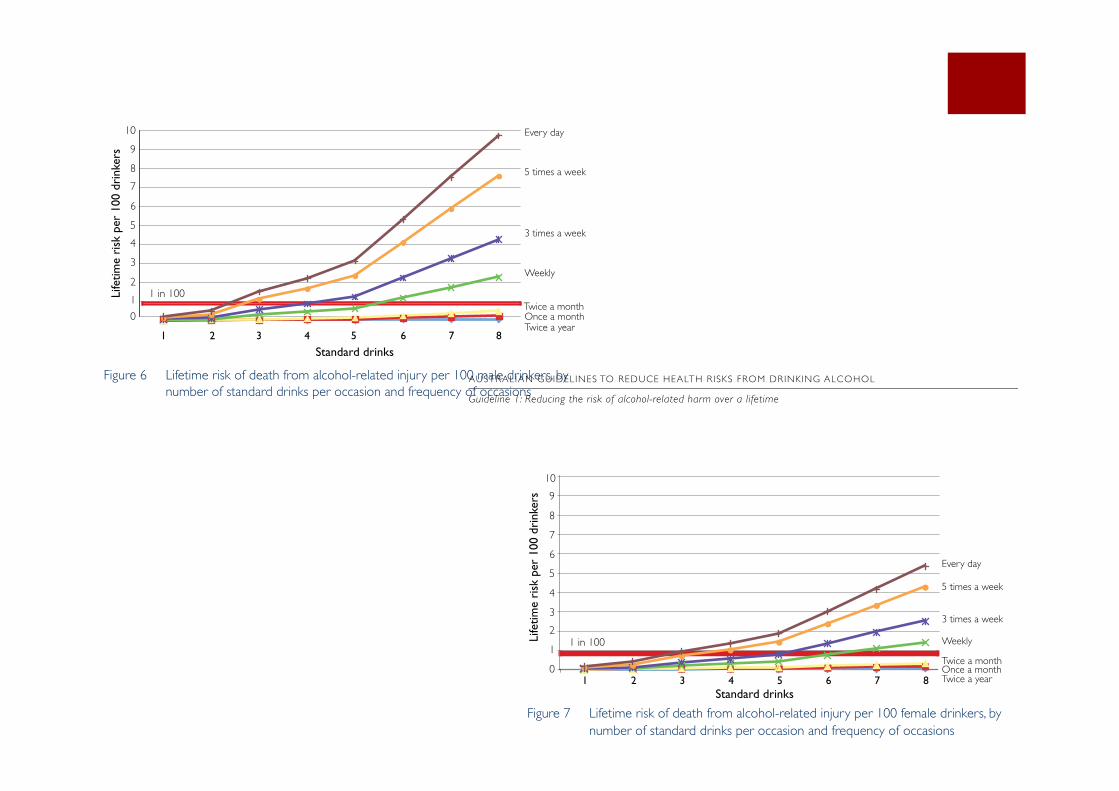
Risk of hospitalisation for alcohol-related injuryMethods similar to those applied to the injury analysis were used in investigating the risk of hospitalisation for alcohol-related injury. The risk of being hospitalised for injury at different frequencies of drinking specific amounts on an occasion was investigated using data for hospitalised injuries from the Victorian Admitted Episode Database for fiscal year 2001–2002. The database includes only cases admitted to a hospital; that is, it does not include cases treated in an emergency department without admission to the hospital. The data can include more than one ‘admission’ for a single injury, in case of transfers to another hospital; and some hospitalised injuries result in death and will also be counted in the injury deaths. These factors are small; thus the proportion of hospitalisations analysed here for injury that ends in death is 1.1 per cent. Around Australia there will be variations between the rate of injuries and the rate of hospitalisations, for example between urban and remote settings due to access of hospitals.
Summary of the evidenceFor both men and women, the lifetime risk of death or hospitalisation due to alcohol-related injury increases with the frequency of drinking occasions. The model incorporated a range of patterns of drinking, based on the number of drinking occasions (see page 35).
Risk of death from alcohol-related injuryFigures 6 and 7 show the risk curves for different frequencies of drinking the specified amounts.
Standard drinks
Life
time
risk
per
100
dri
nker
s
01
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8
Every day
5 times a week
3 times a week
Weekly
Twice a monthOnce a monthTwice a year
1 in 100
Lifetime risk per 100 drinkers
Figure 6 Lifetime risk of death from alcohol-related injury per 100 male drinkers, by number of standard drinks per occasion and frequency of occasions
AUSTRALIAN GUIDELINES TO REDUCE HEALTH RISKS FROM DRINKING ALCOHOL
Guideline 1: Reducing the risk of alcohol-related harm over a lifetime
46 | NATIONAL HEALTH AND MEDIC AL RESEARCH COUNCIL
Standard drinks
Life
time
risk
per
100
dri
nker
s
Every day
5 times a week
3 times a week
Weekly
Twice a monthOnce a monthTwice a year
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 55 6 7 8
1 in 100
Figure 7 Lifetime risk of death from alcohol-related injury per 100 female drinkers, by number of standard drinks per occasion and frequency of occasions
The figures show that:
for both men and women, risk of death increases with frequency of drinkingrisks of death for men are higher than those for women at all levels of drinkingthe risk of death from injury remains below 1 in 100 for both men and women if they always drink two drinks or less on an occasion, even if the occasions are every day.
Men are at a higher risk per day than women because injury mortality per se is higher among men than among women, based on higher rates of risk behaviour at a given level of drinking by men. However, both men and women show similar patterns of increasing risk of injury mortality as both the lifetime drinking occasions and the number of drinks consumed increase.
Risk of hospitalisation due to alcohol-related injuryInvestigation of the risk of being hospitalised for injury at different frequencies of drinking specific amounts on an occasion showed that the lifetime chance of injury related to drinking is an order of magnitude higher than the lifetime chance of death from injury except at the most harmful drinking levels. The ratio of the odds of hospitalisation to the odds of death from injury was much higher at lower amounts of drinking (eg two standard drinks or less on a day) than at higher amounts of drinking. This reflects that the chances of dying from an alcohol-related injury that is serious enough to require hospitalisation increases for higher levels of drinking.
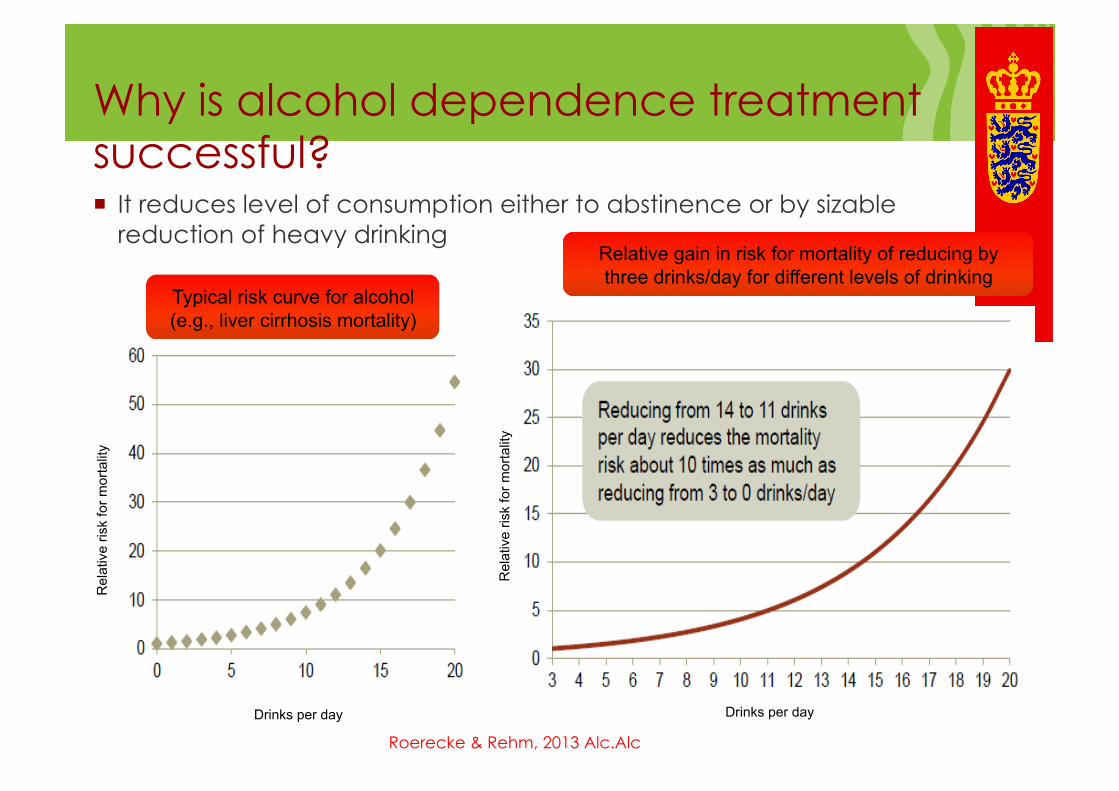
Why is alcohol dependence treatment successful? ! It reduces level of consumption either to abstinence or by sizable
reduction of heavy drinking
Typical risk curve for alcohol (e.g., liver cirrhosis mortality)
Relative gain in risk for mortality of reducing by three drinks/day for different levels of drinking
Rel
ativ
e ris
k fo
r mor
talit
y
Drinks per day Drinks per day
Rel
ativ
e ris
k fo
r mor
talit
y
Roerecke & Rehm, 2013 Alc.Alc
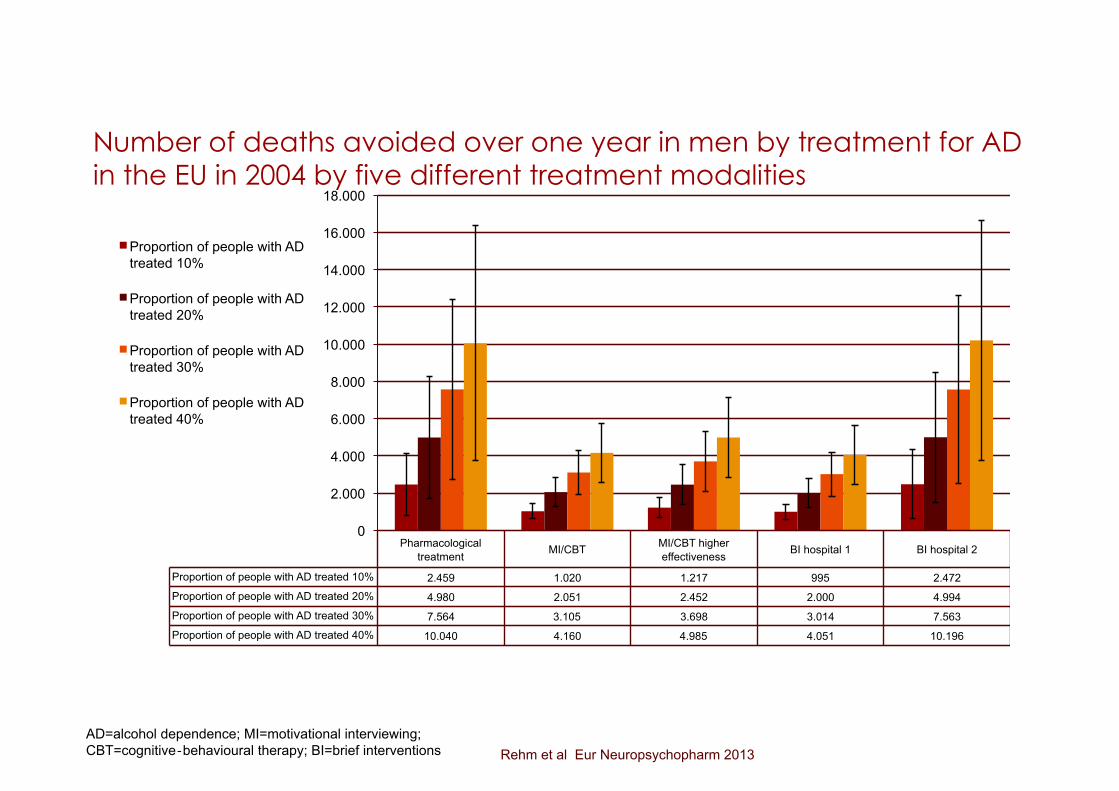
Number of deaths avoided over one year in men by treatment for AD in the EU in 2004 by five different treatment modalities
Pharmacological treatment MI/CBT MI/CBT higher
effectiveness BI hospital 1 BI hospital 2
Proportion of people with AD treated 10% 2.459 1.020 1.217 995 2.472 Proportion of people with AD treated 20% 4.980 2.051 2.452 2.000 4.994 Proportion of people with AD treated 30% 7.564 3.105 3.698 3.014 7.563 Proportion of people with AD treated 40% 10.040 4.160 4.985 4.051 10.196
0
2.000
4.000
6.000
8.000
10.000
12.000
14.000
16.000
18.000
Proportion of people with AD treated 10%
Proportion of people with AD treated 20%
Proportion of people with AD treated 30%
Proportion of people with AD treated 40%
AD=alcohol dependence; MI=motivational interviewing; CBT=cognitive‐behavioural therapy; BI=brief interventions Rehm et al Eur Neuropsychopharm 2013
! Voordelen niveau volksgezondheid
! Beter aansluiten keuze van patient
! Verbreden van de zorg
! Aanvaard binnen het professionele werkveld
! Haalbaar en werkbaar
! Psychosocial interventions
! Pharmacologic interventions
Reductie als behandeldoel
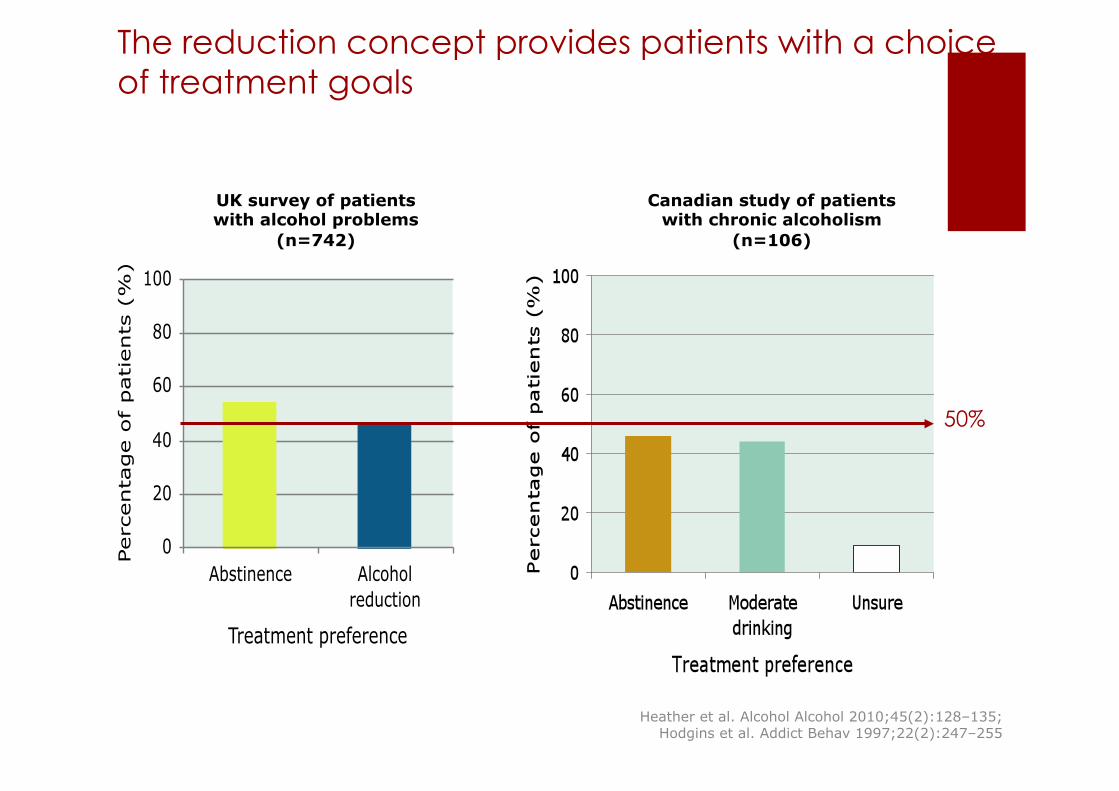
The reduction concept provides patients with a choice of treatment goals
0
20
40
60
80
100
Abstinence Alcoholreduction
Treatment preference
Perc
enta
ge o
f patients
(%
)
UK survey of patients with alcohol problems
(n=742)
Canadian study of patients with chronic alcoholism
(n=106)
50%
Heather et al. Alcohol Alcohol 2010;45(2):128–135; Hodgins et al. Addict Behav 1997;22(2):247–255
! Voordelen niveau volksgezondheid
! Beter aansluiten keuze van patient
! Verbreden van de zorg
! Aanvaard binnen het professionele werkveld
! Haalbaar en werkbaar
! Psychosocial interventions
! Pharmacologic interventions
Reductie als behandeldoel
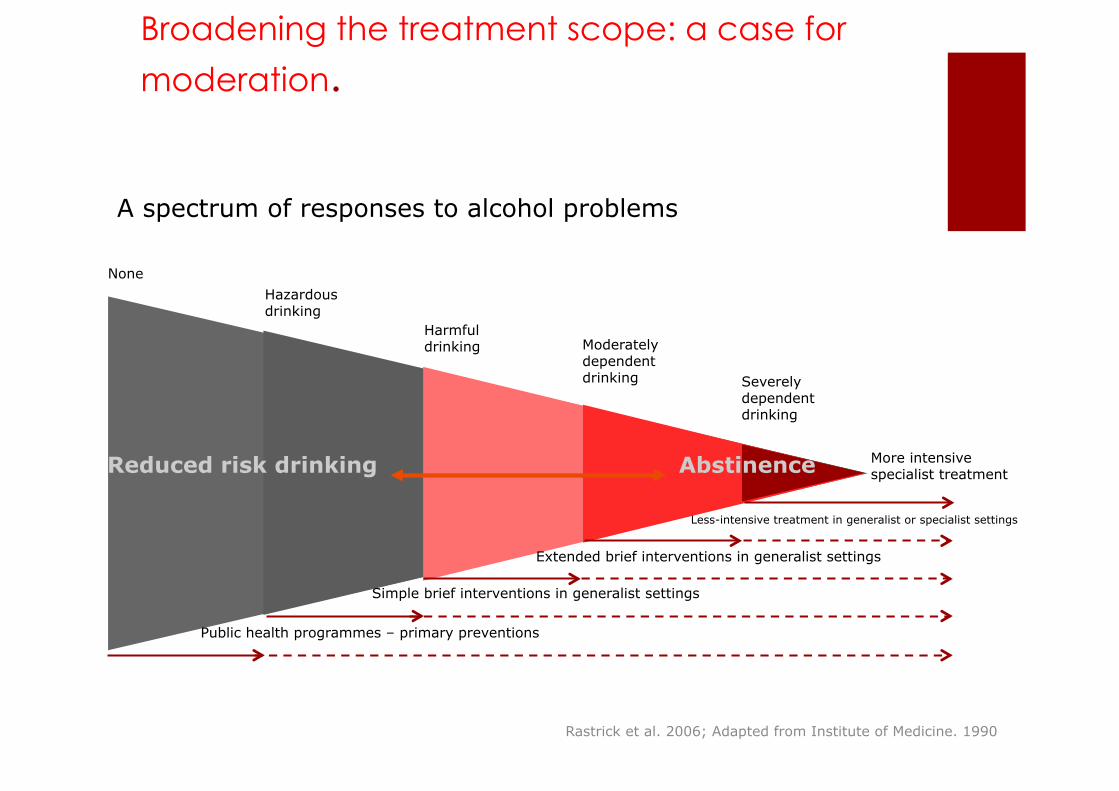
Broadening the treatment scope: a case for
moderation.
Rastrick et al. 2006; Adapted from Institute of Medicine. 1990
A spectrum of responses to alcohol problems
None Hazardous drinking
Harmful drinking Moderately
dependent drinking Severely
dependent drinking
More intensive specialist treatment
Less-intensive treatment in generalist or specialist settings
Extended brief interventions in generalist settings
Simple brief interventions in generalist settings
Public health programmes – primary preventions
Reduced risk drinking Abstinence
! Voordelen niveau volksgezondheid
! Beter aansluiten keuze van patient
! Verbreden van de zorg
! Aanvaard binnen het professionele werkveld
! Haalbaar en werkbaar
! Psychosocial interventions
! Pharmacologic interventions
Reductie als behandeldoel
NIAAA, 2005
This is the view of recently revised clinical guidelines issued by the National
Institute on Alcohol Abuse and Alcoholism (2005):
“… The safest course is abstinence, and that would be the usual clinical
recommendation. Still, it is best to determine individualised goals with each
patient. Some patients may not be willing to endorse abstinence as a goal,
especially at first. If an alcohol-dependent patient agrees to reduce drinking
substantially, it is best to engage them in that goal while continuing to note
that abstinence remains the optimal outcome.”
Helping Patients Who Drink Too Much - A Clinician's Guide 2005
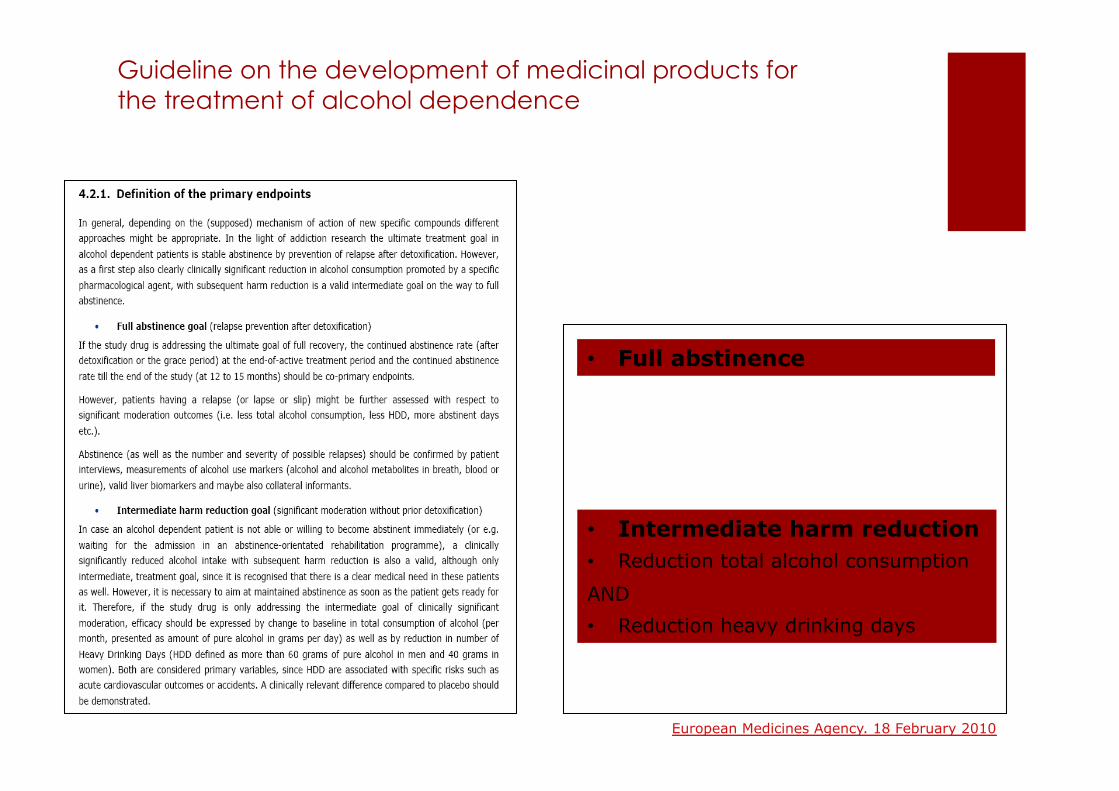
Guideline on the development of medicinal products for the treatment of alcohol dependence
• Full abstinence
• Intermediate harm reduction • Reduction total alcohol consumption
AND
• Reduction heavy drinking days
European Medicines Agency. 18 February 2010
Reduced-risk drinking is accepted as a treatment goal in France (50%), Britain (76%), Australia (72%), Switzerland (22–70%), Canada (27–62%), but not (yet) in the USA (17%)
Acceptance reduced-risk drinking by professionals
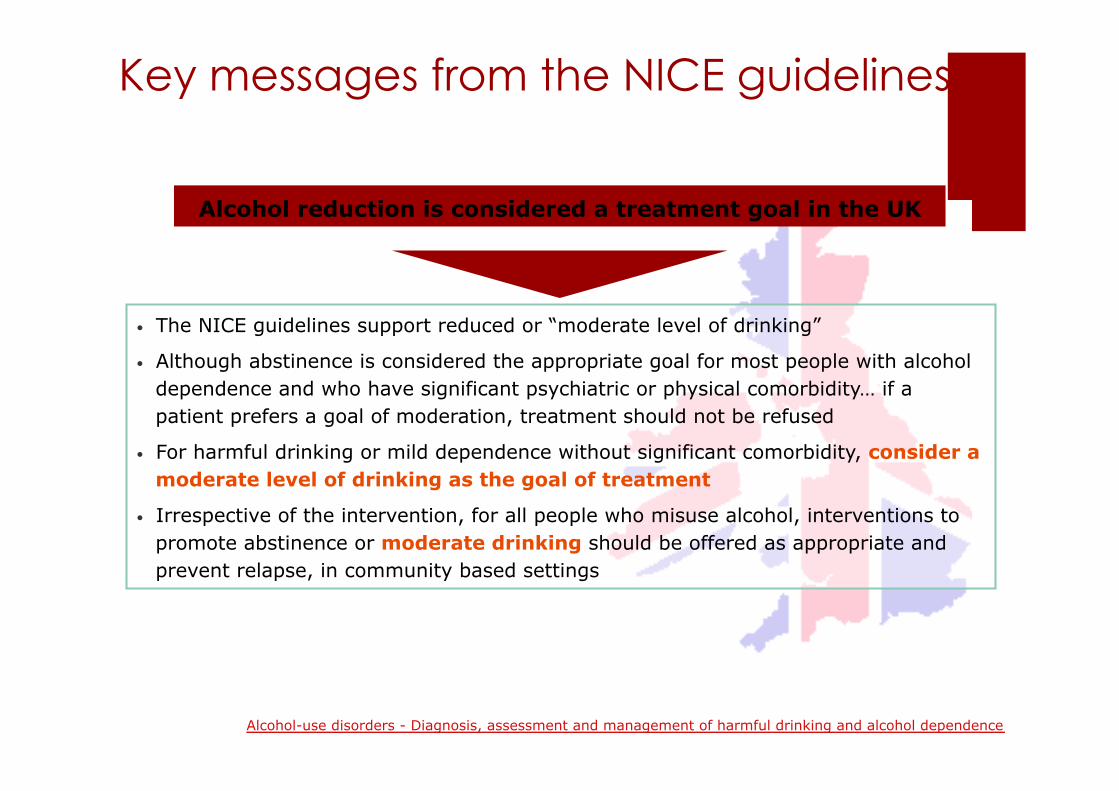
Alcohol reduction is considered a treatment goal in the UK
• The NICE guidelines support reduced or “moderate level of drinking”
• Although abstinence is considered the appropriate goal for most people with alcohol dependence and who have significant psychiatric or physical comorbidity… if a patient prefers a goal of moderation, treatment should not be refused
• For harmful drinking or mild dependence without significant comorbidity, consider a moderate level of drinking as the goal of treatment
• Irrespective of the intervention, for all people who misuse alcohol, interventions to promote abstinence or moderate drinking should be offered as appropriate and prevent relapse, in community based settings
Key messages from the NICE guidelines
Alcohol-use disorders - Diagnosis, assessment and management of harmful drinking and alcohol dependence
! Voordelen niveau volksgezondheid
! Beter aansluiten keuze van patient
! Verbreden van de zorg
! Aanvaard binnen het professionele werkveld
! Haalbaar en werkbaar
! Psychosocial interventions
! Pharmacologic interventions
Reductie als behandeldoel
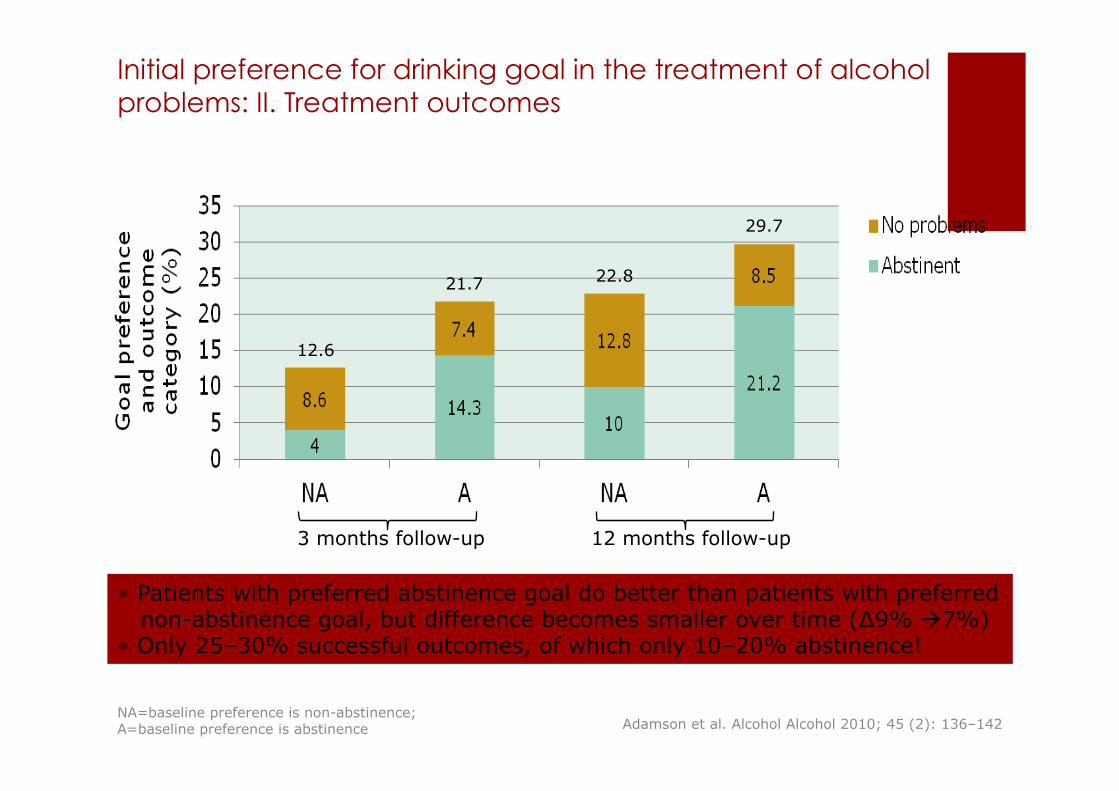
Initial preference for drinking goal in the treatment of alcohol problems: II. Treatment outcomes
• Patients with preferred abstinence goal do better than patients with preferred non-abstinence goal, but difference becomes smaller over time (∆9% !7%) • Only 25–30% successful outcomes, of which only 10–20% abstinence!
12.6
21.7 22.8
29.7
NA=baseline preference is non-abstinence; A=baseline preference is abstinence
3 months follow-up 12 months follow-up
Adamson et al. Alcohol Alcohol 2010; 45 (2): 136–142
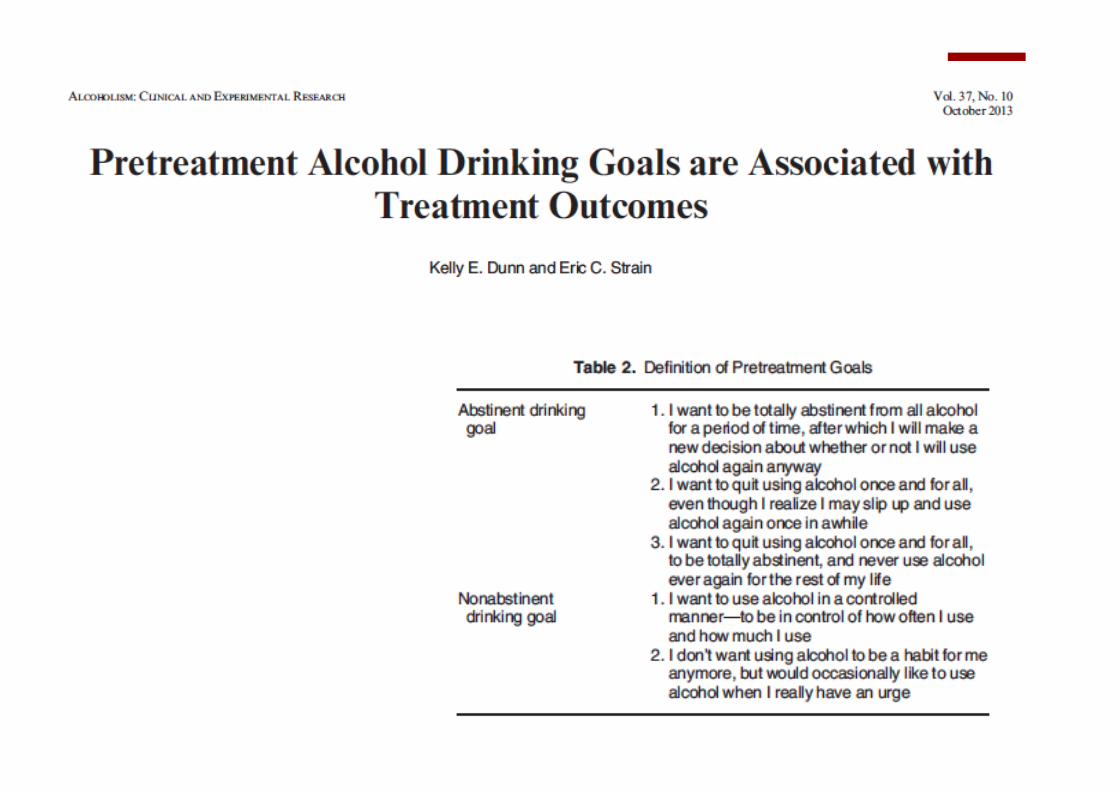
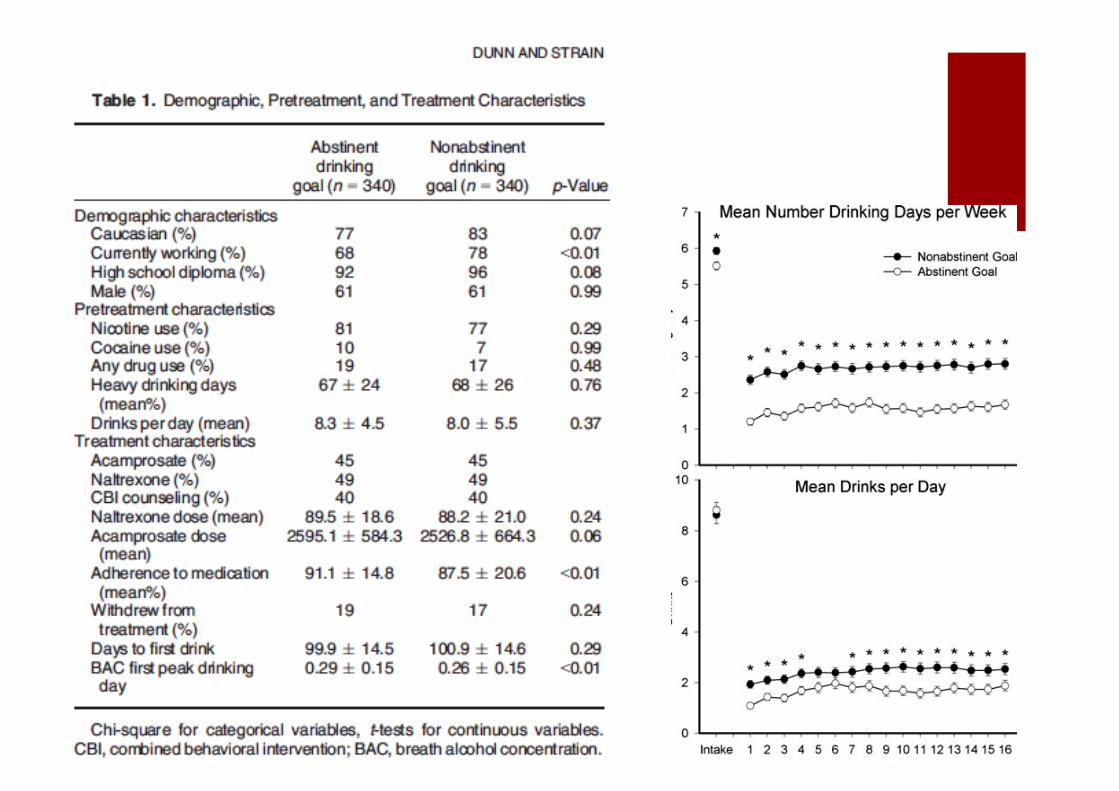
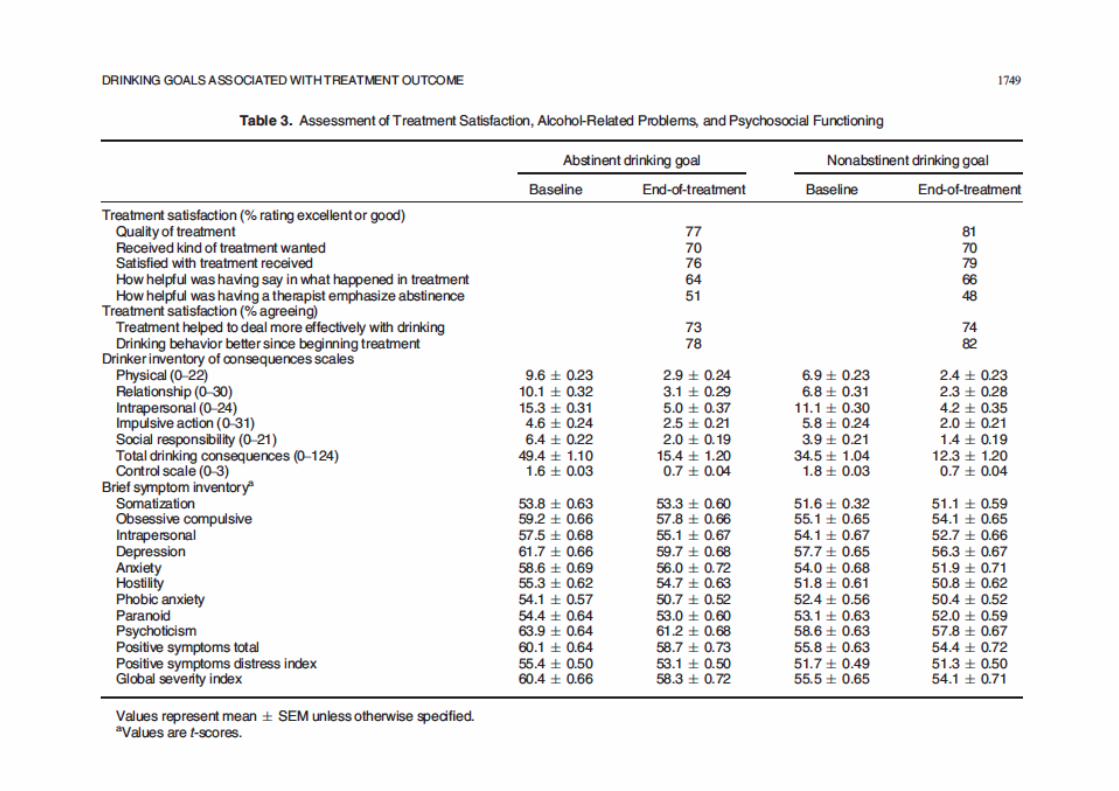
Results ! Approximately 25% of the total COMBINE study sample
endorsed a nonabstinent drinking goal at study intake, which is consistent with other studies that have reported 16 to 46% of participants entering treatment for alcohol use disorders identify a nonabstinent drinking goal
! Participants who chose an abstinent drinking goal had significantly more weeks with no drinking or no heavy drinking, reported fewer heavy drinking days, reported fewer days with >1 drink, and were more likely to have a 50%decrease in drinks per day between baseline and week 16 of the intervention.
! However, both groups reported reductions over time in percent drinking days, mean drinks per day, number of heavy drinking days, and number of drinking days per week, and participants in both groups experienced significant reductions in alcohol-related problems and improvements in psychosocial functioning.
! Voordelen niveau volksgezondheid
! Beter aansluiten keuze van patient
! Verbreden van de zorg
! Aanvaard binnen het professionele werkveld
! Haalbaar en werkbaar
! Psychosocial interventions
! Pharmacologic interventions
Reductie als behandeldoel
PRIORITY COMMUNICATION
Extending the Treatment Options in AlcoholDependence: A Randomized Controlled Study ofAs-Needed NalmefeneKarl Mann, Anna Bladstrom, Lars Torup, Antoni Gual, and Wim van den Brink
Background: There is a large treatment gap in alcohol dependence, and current treatments are only moderately effective in preventingrelapse. New treatment modalities, allowing for reduction of alcohol consumption as a treatment goal are needed. This study evaluatedthe efficacy of as-needed use of the opioid system modulator nalmefene in reducing alcohol consumption in patients with alcoholdependence.
Methods: Six hundred and four patients (placebo ¼ 298; nalmefene ¼ 306), ‡18 years of age, with a diagnosis of alcoholdependence, ‡6 heavy drinking days, and average alcohol consumption ‡ World Health Organization medium drinking risk level in the4 weeks preceding screening, were randomized (1:1) to 24 weeks of as-needed placebo or nalmefene 18 mg.
Results: Patients taking placebo (n ¼ 289) and patients taking nalmefene (n ¼ 290) were included in the efficacy analyses. At Month 6,there was a significant effect of nalmefene compared with placebo in reducing the number of heavy drinking days ("2.3 days [95%confidence interval: "3.8 to ".8]; p ¼ .0021) and total alcohol consumption ("11.0 g/day [95% confidence interval: "16.8 to "5.1]; p ¼.0003). Improvements in Clinical Global Impression and liver enzymes were larger in the nalmefene group compared with placebo atWeek 24. Adverse events (most mild or moderate) and dropouts due to adverse events were more common with nalmefene thanplacebo. The number of patients with serious adverse events was similar in the two groups.
Conclusions: Nalmefene provides clinical benefit, constitutes a potential new pharmacological treatment paradigm in terms of thetreatment goal and dosing regimen, and provides a method to address the unmet medical need in patients with alcohol dependencethat need to reduce their alcohol consumption.
Key Words: Alcohol dependence, as-needed, nalmefene, opioidantagonist, placebo-controlled, reduction
With almost 15 million affected persons in the EuropeanUnion and 8 million affected persons in the UnitedStates, alcohol dependence is a major public health
problem (1,2). At the same time, alcohol dependence remainsseriously underdiagnosed and undertreated (3). In Europe,!10% of the people diagnosed with alcohol dependencereceive any treatment; the corresponding figure for the UnitedStates is approximately 25% (4). Moreover, more than two thirds ofpatients in abstinence-oriented treatments relapse within the first12 months (5,6). Despite encouraging data from studies targetingreduction of alcohol intake (7–9), current pharmacological treat-ments for alcohol dependence are approved only for relapseprevention. However, !30% of patients treated with acamprosatewere continuously abstinent after 12 months of treatment (10),and two thirds of patients treated with naltrexone had experi-enced at least one heavy drinking day after 16 weeks of treatment
(2). Despite all this, prevailing opinions hold abstinence as theprimary treatment goal (11), although abstinence-oriented treat-ments might not be desirable or acceptable to many patients (12).
In such an unsatisfactory situation, new evidence-basedtreatment modalities are needed (13–15) to address this unmetmedical need in patients at risk of alcohol-related harm. Reduc-tion of alcohol consumption as a treatment goal has been heavilydebated within the scientific community (16,17). Cliniciansincreasingly support reduction of alcohol consumption as avaluable treatment option to reduce the consequences ofharmful alcohol consumption and attract patients who arecurrently not inclined to seek treatment (11,13,18–20).
Reduction of alcohol consumption is associated with reducedrisk of morbidity and mortality in patients with alcohol depen-dence (21). Allowing patients to choose between abstinence orreduction as their treatment goal might enhance engagementwith the treatment, ultimately leading to better treatment out-comes (22,23). Patients might also reconsider abstinence oncethey are engaged in therapy (24), even though abstinence is notalways necessary to benefit from treatment.
Nalmefene is an opioid system modulator, with antagonistactivity at the m and d receptors and partial agonist activity at thek receptor (25). Acute alcohol intake results in mesolimbicdopamine release (facilitated by the release of b-endorphins)(26). After repeated exposure to high doses of alcohol, neuroa-daptations occur in several neurotransmitter/neuropeptide sys-tems, including the opioid receptor system, which might lead tocontinued alcohol intake (27,28). The proposed mechanism ofaction of nalmefene is to reduce the reinforcing effects of alcohol,helping the patient to reduce drinking.
Although Anton et al. (29) was unable to show an effectcompared with placebo, other studies of nalmefene in patientswith alcohol-use disorders indicate that treatment with nalmefene is
Authors AG and WvdB contributed equally to this work.
From the Central Institute of Mental Health (KM), University of Heidelberg,Mannheim, Germany; H. Lundbeck A/S (AB, LT), Copenhagen,Denmark; Neurosciences Institute (AG), Hospital Clinic, Barcelona,Spain; and the Academic Medical Center (WvdB), Department ofPsychiatry, University of Amsterdam, Amsterdam, The Netherlands.
Address correspondence to Karl Mann, M.D., Ph.D., Department ofAddictive Behavior and Addiction Medicine, Ruprecht-Karls-University Heidelberg, Central Institute of Mental Health, Square J5,68159 Mannheim, Germany; E-mail: [email protected].
Received Jul 13, 2012; revised Sep 26, 2012; accepted Oct 12, 2012.
0006-3223/$36.00 BIOL PSYCHIATRY 2013;73:706–713http://dx.doi.org/10.1016/j.biopsych.2012.10.020 Crown Copyright & 2013 Published by Elsevier Inc
on behalf of Society of Biological Psychiatry. All rights reserved.
PRIORITY COMMUNICATION
Extending the Treatment Options in AlcoholDependence: A Randomized Controlled Study ofAs-Needed NalmefeneKarl Mann, Anna Bladstrom, Lars Torup, Antoni Gual, and Wim van den Brink
Background: There is a large treatment gap in alcohol dependence, and current treatments are only moderately effective in preventingrelapse. New treatment modalities, allowing for reduction of alcohol consumption as a treatment goal are needed. This study evaluatedthe efficacy of as-needed use of the opioid system modulator nalmefene in reducing alcohol consumption in patients with alcoholdependence.
Methods: Six hundred and four patients (placebo ¼ 298; nalmefene ¼ 306), ‡18 years of age, with a diagnosis of alcoholdependence, ‡6 heavy drinking days, and average alcohol consumption ‡ World Health Organization medium drinking risk level in the4 weeks preceding screening, were randomized (1:1) to 24 weeks of as-needed placebo or nalmefene 18 mg.
Results: Patients taking placebo (n ¼ 289) and patients taking nalmefene (n ¼ 290) were included in the efficacy analyses. At Month 6,there was a significant effect of nalmefene compared with placebo in reducing the number of heavy drinking days ("2.3 days [95%confidence interval: "3.8 to ".8]; p ¼ .0021) and total alcohol consumption ("11.0 g/day [95% confidence interval: "16.8 to "5.1]; p ¼.0003). Improvements in Clinical Global Impression and liver enzymes were larger in the nalmefene group compared with placebo atWeek 24. Adverse events (most mild or moderate) and dropouts due to adverse events were more common with nalmefene thanplacebo. The number of patients with serious adverse events was similar in the two groups.
Conclusions: Nalmefene provides clinical benefit, constitutes a potential new pharmacological treatment paradigm in terms of thetreatment goal and dosing regimen, and provides a method to address the unmet medical need in patients with alcohol dependencethat need to reduce their alcohol consumption.
Key Words: Alcohol dependence, as-needed, nalmefene, opioidantagonist, placebo-controlled, reduction
With almost 15 million affected persons in the EuropeanUnion and 8 million affected persons in the UnitedStates, alcohol dependence is a major public health
problem (1,2). At the same time, alcohol dependence remainsseriously underdiagnosed and undertreated (3). In Europe,!10% of the people diagnosed with alcohol dependencereceive any treatment; the corresponding figure for the UnitedStates is approximately 25% (4). Moreover, more than two thirds ofpatients in abstinence-oriented treatments relapse within the first12 months (5,6). Despite encouraging data from studies targetingreduction of alcohol intake (7–9), current pharmacological treat-ments for alcohol dependence are approved only for relapseprevention. However, !30% of patients treated with acamprosatewere continuously abstinent after 12 months of treatment (10),and two thirds of patients treated with naltrexone had experi-enced at least one heavy drinking day after 16 weeks of treatment
(2). Despite all this, prevailing opinions hold abstinence as theprimary treatment goal (11), although abstinence-oriented treat-ments might not be desirable or acceptable to many patients (12).
In such an unsatisfactory situation, new evidence-basedtreatment modalities are needed (13–15) to address this unmetmedical need in patients at risk of alcohol-related harm. Reduc-tion of alcohol consumption as a treatment goal has been heavilydebated within the scientific community (16,17). Cliniciansincreasingly support reduction of alcohol consumption as avaluable treatment option to reduce the consequences ofharmful alcohol consumption and attract patients who arecurrently not inclined to seek treatment (11,13,18–20).
Reduction of alcohol consumption is associated with reducedrisk of morbidity and mortality in patients with alcohol depen-dence (21). Allowing patients to choose between abstinence orreduction as their treatment goal might enhance engagementwith the treatment, ultimately leading to better treatment out-comes (22,23). Patients might also reconsider abstinence oncethey are engaged in therapy (24), even though abstinence is notalways necessary to benefit from treatment.
Nalmefene is an opioid system modulator, with antagonistactivity at the m and d receptors and partial agonist activity at thek receptor (25). Acute alcohol intake results in mesolimbicdopamine release (facilitated by the release of b-endorphins)(26). After repeated exposure to high doses of alcohol, neuroa-daptations occur in several neurotransmitter/neuropeptide sys-tems, including the opioid receptor system, which might lead tocontinued alcohol intake (27,28). The proposed mechanism ofaction of nalmefene is to reduce the reinforcing effects of alcohol,helping the patient to reduce drinking.
Although Anton et al. (29) was unable to show an effectcompared with placebo, other studies of nalmefene in patientswith alcohol-use disorders indicate that treatment with nalmefene is
Authors AG and WvdB contributed equally to this work.
From the Central Institute of Mental Health (KM), University of Heidelberg,Mannheim, Germany; H. Lundbeck A/S (AB, LT), Copenhagen,Denmark; Neurosciences Institute (AG), Hospital Clinic, Barcelona,Spain; and the Academic Medical Center (WvdB), Department ofPsychiatry, University of Amsterdam, Amsterdam, The Netherlands.
Address correspondence to Karl Mann, M.D., Ph.D., Department ofAddictive Behavior and Addiction Medicine, Ruprecht-Karls-University Heidelberg, Central Institute of Mental Health, Square J5,68159 Mannheim, Germany; E-mail: [email protected].
Received Jul 13, 2012; revised Sep 26, 2012; accepted Oct 12, 2012.
0006-3223/$36.00 BIOL PSYCHIATRY 2013;73:706–713http://dx.doi.org/10.1016/j.biopsych.2012.10.020 Crown Copyright & 2013 Published by Elsevier Inc
on behalf of Society of Biological Psychiatry. All rights reserved.
Drug and Alcohol Dependence 133 (2013) 15– 29
Contents lists available at ScienceDirect
Drug and Alcohol Dependence
jo ur nal homep ag e: www.elsev ier .com/ locate /drugalcdep
Review
Emerging pharmacotherapies for alcohol dependence: A systematicreview focusing on reduction in consumption!
Henri-Jean Aubina,∗, Jean-Bernard Daeppenb,1
a Hôpital Paul Brousse, INSERM 669, Université Paris-Sud, Villejuif, Franceb Alcohol Treatment Center, Lausanne University Hospital, Lausanne, Switzerland
a r t i c l e i n f o
Article history:Received 7 November 2012Received in revised form 15 March 2013Accepted 22 April 2013Available online 6 June 2013
Keywords:AbstinenceAlcohol dependenceBurdenSystematic reviewTreatmentReduction in consumption
a b s t r a c t
Background: European Medicines Agency guidelines recognize two different treatment goals for alco-hol dependence: abstinence and reduction in alcohol consumption. All currently approved agents areindicated for abstinence. This systematic review aimed to identify drugs in development for alcoholdependence treatment and to establish, based upon trial design, if any are seeking market authorizationfor reduction in consumption.Methods: We searched PubMed and Embase (December 2001–November 2011) to identify agents indevelopment for alcohol dependence treatment. Additional studies were identified by searching Clini-calTrials.gov and the R&D Insight and Clinical Trials Insight databases. Studies in which the primary focuswas treatment of comorbidity, or n ≤ 20, were excluded. Studies were then classified as ‘abstinence’ ifthey: described a detoxification/alcohol withdrawal period; enrolled patients who had undergone detox-ification previously; or presented relapse/abstinence rates as the primary outcome. Studies in patientsactively drinking at baseline were classified as ‘reduction in consumption’.Results: Of 602 abstracts identified, 45 full-text articles were eligible. Five monotherapies were in devel-opment for alcohol dependence treatment: topiramate, fluvoxamine, aripiprazole, flupenthixol andnalmefene. Nalmefene was the only agent whose sponsor was clearly seeking definitive approval forreduction in consumption. Development status was unclear for topiramate, fluvoxamine, aripiprazoleand flupenthixol. Fifteen agents were examined in published exploratory investigator-initiated trials;the majority focused on abstinence. Ongoing (unpublished) trials tended to focus on reduction in con-sumption.Conclusions: While published studies generally focused on abstinence, ongoing trials focused on reductionin consumption, suggesting a change in emphasis in the approach to treating alcohol dependence.
© 2013 Elsevier Ireland Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
2.1. Published literature search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162.2. Proprietary database search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173.1. Published literature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
3.1.1. Sponsored agents in development for alcohol dependence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183.1.2. Agents explored in investigator-initiated trials for alcohol dependence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
3.2. Proprietary databases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203.2.1. Additional trials in ClinicalTrials.gov and CTI without published data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203.2.2. Additional agents identified via R&D Insight . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
! Supplementary material can be found by accessing the online version of this paper at http://dx.doi.org and by entering http://dx.doi.org/10.1016/j.drugalcdep.2013.04.025.∗ Corresponding author at: Addictologie, Hôpital Paul Brousse, 12, avenue Paul-Vaillant-Couturier, 94804 VILLEJUIF Cedex, France. Tel.: +33 145 59 39 51;
fax: +33 145 59 38 63.E-mail addresses: [email protected], [email protected] (H.-J. Aubin).
1 Service d’alcoologie, Avenue de Beaumont 21bis, CHUV 1011 Lausanne, Switzerland.
0376-8716/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.http://dx.doi.org/10.1016/j.drugalcdep.2013.04.025
Vragen ! Reductie valide behandel doel
! Maar voor wie ?
! Klinische criteria ?
conclusie ! Verminderen van alcohol gebruik als behandel
doel aantal belangrijke voordelen:
! Meer aansluiten op vraag van een belangrijk aantal patienten met alcohol afhankelijkheid
! Verlaging drempel behandeling & verhogen behandel bereik.
! Meer patienten bereiken in vroeger stadium
! Destigmatizering.
! Op bevolkingsniveau grote gezondheids winst.