Embed Size (px)
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2010) 45, 59–64
Reflectance spectrometry for real-time hemoglobindetermination of placental vessels during endoscopic lasersurgery for twin-to-twin transfusion syndromeSean Currana,b, John W. McMurdyb, Stephen R. Carra,b, Christopher S. Muratorea,b,Barbara M. O'Briena,b, Gregory P. Crawfordb, Francois I. Luksa,b,⁎
aDivision of Pediatric Surgery and Maternal-Fetal Medicine, Program in Fetal Medicine,Alpert Medical School of Brown University, Providence, RI 02905, USAbDivision of Engineering, Brown University, Providence, RI 02905, USA
Received 26 September 2009; accepted 6 October 2009
A
S0
0d
Key words:Endoscopic fetal surgery;Noninvasive monitoring;Anemia;Spectrometry;Hemoglobin
AbstractObjective: The objective of the study was to develop a noninvasive technique to determine hemoglobin(Hb) content through spectral analysis of diffusely reflected broadband visible illumination fromindividual blood vessels during endoscopic fetal surgery for twin-to-twin transfusion syndrome (TTTS).Methods: The reflection of an incoming xenon endoscopic light source was captured through a630-μm–diameter optic fiber coupled to a fixed grating spectrometer (2-nm resolution). A 450- to700-nm wavelength range was used for analysis. Three data-capturing methods were studied: (1) fixed-image spectrum capture with fiber aimed at (but not touching) center of a vessel, (2) no-touch scanningperpendicular to the vessel and dynamic spectral capture, and (3) dynamic spectral capture and analysisof the reflectance spectra during brief vessel touch.Results: Eight controls (elective laparoscopic and thoracoscopic operations in children aged 1-17 years)were enrolled. Four vessels were analyzed in each case. The brief-touch technique with intensity peakanalysis yielded the most reproducible results between multiple vessels in the same patient. Spectrometrywas also applied to 2 TTTS patients. The (anemic) donor and (polycythemic) recipient twin fetuses couldbe differentiated with good correlation between vessels (arteries and vein) of the same fetus.Conclusions: It is possible to differentiate donor from recipient placental vessels by spectral analysis ofthe reflected light through the endoscope using a noninvasive and real-time method. This may improvethe accuracy of endoscopic laser ablation of placental vessels in TTTS and may allow instant endoscopicHb determination for laparoscopic procedures as well.© 2010 Elsevier Inc. All rights reserved.
Presented at the 40th Annual Meeting of the American Pediatric Surgicalssociation, Fajardo, Puerto Rico, May 28-June 1, 2009.⁎ Corresponding author. Division of Pediatric Surgery, Alpert Medical
chool of Brown University, Providence, RI 02905, USA. Tel.: +1 401 228556; fax: +1 401 444 6603.E-mail address: [email protected] (F.I. Luks).
022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2009.10.009
Twin-to-twin transfusion syndrome (TTTS) is a condition
that affects 10% to 15% of all monochorionic/diamniotictwins. When severe and untreated, TTTS leads to dualmortality in a large number of patients; survivors are at highrisk of severe neurologic and cardiac anomalies [1].Endoscopic laser ablation of the communicating placental
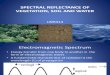
Fig. 1 Inset, Absorbance spectrum of deoxyhemoglobin (Hb)and oxyhemoglobin (HbO2) illuminated with a broadband lightsource. At wavelengths less than 630 nm, the 2 curves are muchmore similar. Main figure, Normalized reflectance spectrum of acapillary vascular bed at 2 different Hb concentrations using aproprietary portable Hb monitoring device (see text for details).
60 S. Curran et al.
vessels can halt the syndrome in the majority of cases, andsurvival of at least 1 twin is seen in 75% to 85% ofpregnancies [2-5]. The procedure involves endoscopicaccess to the amniotic cavity of the recipient twin, whosefluid overload from chronic transfusion results in polyuriaand polyhydramnios. The umbilical cord insertions ofrecipient and donor are mapped out and an avascular planeis identified, perpendicular to the axis between both cordinsertions. Vessels that cross this avascular plane andconnect the 2 fetuses are considered twin-twin anastomosesand must be occluded. Four types are known: arteriovenousconnections from donor to recipient, arteriovenous connec-tions from recipient to donor, and arterioarterial andvenovenous anastomoses.
Often, the nature of these vessels can be identifiedvisually: arteries carry oxygen-poor blood to the placentaand appear darker than oxygen-rich veins; when paired,arteries tend to cross on top of their companion vein.However, the vascular anatomy can be confusing and hybridanastomoses exist that combine arteries and veins from bothtwins [6]. Ancillary methods to identify the nature and originof placental vessels could allow a more precise mapping ofthe angioarchitecture.
We have developed a spectrophotometric technique topredict the hemoglobin (Hb) concentration from lightreflectance off individual blood vessels, based on earlierwork in noninvasive, real-time Hb determination of theconjunctival vascular bed [7,8].
1. Materials and methods
The principle of reflectance (or transmission) spectro-metry for blood oxygen saturation is based on a difference inlight absorption between oxyhemoglobin and deoxyhemo-globin. This difference is greatest at wavelengths greater than630 nm and into the near-infrared regime, which is why mostpulse oximetry devices compare absorbance or reflectance inthe red and infrared portions of the light spectrum. However,the absorption and reflectance spectra of oxyhemoglobin anddeoxyhemoglobin are much more similar at wavelengths lessthan 630 nm (Fig. 1, inset).
The Division of Engineering at Brown Universitypreviously described a device for real-time, noninvasiveHb determination based on this principle. It uses a broadbandwhite light source to illuminate the palpebral conjunctiva,and diffuse reflectance from the tissues (including bloodvessels) is collected with a fiber-optic–based gratingspectrometer. When curves are normalized for light intensityand analyzed using a nonlinear regression technique, aninverse correlation can be found between Hb concentrationand the amount of light reflected in the 440- to 680-nmwindow of the spectrum. Fig. 1 illustrates this: the Hbreflectance curve in a patient with a serum Hb concentrationof 8.1 g/dL is clearly different from that in a patient with an
Hb concentration of 16.7 g/dL [8,9]. This principle wasadapted for endoscopic use. Institutional Review Boardapproval was obtained for the study.
1.1. Laparoscopy patients
In the first part of the experiment, feasibility was testedusing otherwise healthy pediatric volunteers who wereundergoing elective laparoscopic or thoracoscopic surgeryat Hasbro Children's Hospital. With Institutional ReviewBoard approval and after obtaining parental consent andpatient assent, a 4- to 5-minute study was performed at thebeginning of the laparoscopic procedure. After induction ofgeneral anesthesia, a blood sample was obtained for Hbdetermination (reference value). In preparation for its use inendoscopic fetal surgery, the same telescope setup was usedfor both the laparoscopic and fetal parts of the experiment. A1.9-mm semirigid telescope (Karl Storz Endoscopy, CulverCity, CA) housed in a 10F metal sheath was introducedthrough one of the 5-mm cannulas in the patient's abdomenor thoracic cavity. A standard light source (175-W XenonLight Source, model # 20132020, Karl Storz Endoscopy)was connected through a fiber-optic light cable to thetelescope. A 630-μm–diameter optic fiber used for endo-scopic laser (ForTec Medical, Streetsboro, OH) wasintroduced through the side port of the sheath. Small omentaland mesenteric blood vessels (0.5-1.5 mm in diameter) werechosen to mimic placental vessels (Fig. 2A). The camera wasplaced on the 1.9-mm telescope, which was brought to within1 cm of the blood vessel. The laser fiber was advanced withthe tip just beyond the telescope. Three different capturetechniques were used: (a) real-time recording of the

Fig. 2 A, Setup for spectral Hb measurement in control patients.A 3-mm–diameter telescope sheath containing a 1.9-mm telescopeand 630-μm–diameter optic fiber, pointed at a mesenteric vesselduring laparoscopy. B, Same fiber and telescope during endoscopicfetal surgery. Fiber is aimed at a placental vessel (see text for details).
61Reflectance spectrometry for real-time Hb determination
reflectance spectrum during 10 seconds while the fiber wascentered on the blood vessel; (b) scanning of the fiberperpendicular to the vessel, starting on the surroundingtissues on one side of the vessel wall, through the anteriorwall of the vessel to the contralateral side; and (c) touchtechnique, whereby the tip of the fiber was slightly tapped onthe anterior wall of the vessel.
1.2. Fetal patients
In the second part of this study, spectrometric Hbdetermination was performed in patients undergoing endo-scopic laser ablation of placental vessels for severe TTTS.The operative technique has been described in detailelsewhere [1,10]. Briefly, the amniotic cavity of the recipienttwin is accessed using a Seldinger technique and a 14F peel-away sheath (Cook Medical, Bloomington, IN). Thetelescope and sheath described above are used to explore
the amniotic cavity and the placental surface, whereindividual communicating blood vessels are obliteratedusing a diode laser through a 630-μm–diameter laser fiber(ForTec Medical). Before laser application, the same laserdelivery fiber was connected to the spectrometer and laptopcomputer for spectral analysis. The tapping fiber collectionmethod was used, based on observed results from thelaparoscopy portion of the study. Fig. 2B illustrates the fiberpointed at one of the placental vessels just before analysis.
1.3. Signal processing
The fiber was connected to a miniature visible fixedgrating spectrometer (dimensions, 3.5” × 2.5” × 1”) with a2-nm resolution and dynamic range from 200 1100 nm(USB400; Ocean Optics, Dunedin, FL), itself plugged into alaptop/desktop via a USB cable for both data analysis andpower. Major modifications in the setup were dictated by thestrong light source used in laparoscopy and endoscopic fetalsurgery, and the direct reading off a single blood vessel,rather than a capillary bed. The integration time to collectsamples from each individual vessel was well under 1second, making a real-time determination possible. Toextract a quantitative parameter correlated with total Hbconcentration, reflectance spectra were normalized by theirradiation source and normalized to the peak reflectanceintensity at 625 nm. An estimation of the amount of total Hbcan be calculated by the intensity ratio at 2 spectral pointswith significantly different absorption coefficients, specifi-cally 625 and 575 nm. Ideally, 2 isosbestic points for oxy-and deoxyhemoglobin would be compared; however, thesimilarity of absorption coefficients of 5 isosbestic points inthe working spectral range (400-700 nm from sourceillumination) makes this comparison less precise. The errorintroduced by varying oxy- and deoxyhemoglobin absorp-tion coefficients at 625 and 575 nm is significant, but likelytolerable in preliminary experimentation. This artificiallygenerated ratio value is termed the hemoglobin ratioparameter (HRP) and correlates with total Hb concentration.
2. Results
Eight patients, aged 1 to 17 years, who underwent alaparoscopic or thoracoscopic procedure for unrelatedindications were enrolled in the first part of the study.Procedures included 2 cholecystectomies, 1 fundoplication,1 colectomy, 2 interval appendectomies, 1 resection of aparaspinal ganglioneuroma, and 1 resection of a pulmonarysequestration. There were no complications. Data capturerequired less than 5 minutes in all patients. The 3 capturetechniques were used to determine the most stable andreproducible method. The single point and scanningcollection methods proved to be too unstable and producedtoo much scatter and background noise.

62 S. Curran et al.
Data were collected from the last 3 laparoscopic patientsusing rapid spectral acquisition with tapping the bloodvessel of interest. The touch technique guarantees that theblood vessel is sampled with minimal interference fromsurrounding tissues, and allows minimal variation fromvessel to vessel. The integration time was approximately 10milliseconds per spectrum over 10 seconds of datacollection. Fig. 3 (A and B) shows the HRP as a functionof time, with maximum intensity at fiber contact (4 taps foreach vessel). An HRP at vessel contact of 2.7 ± 0.06corresponds with an Hb concentration of 10.7 (Fig. 3A); anHRP of 3.2 ± 0.24 corresponds with an Hb concentration of14.0 (Fig. 3B). The reflectance spectra at 1 vessel contactpoint for each of these 2 patients are shown in Fig. 3C.
Two patients undergoing endoscopic fetal procedures forsevere TTTS were enrolled in the study. In each patient, atleast 4 placental vessels from each fetus were sampled. A plotof the spectra of all 4 vessel types (donor A and V, recipientA and V) at the point of maximum HRP is shown in Fig. 4.As anticipated, the anemic donor had a lower absorbance and,therefore, higher reflection than the recipient. There weresmall, but real differences between arteries and veins of thesame fetus, suggesting variation in the absorption coefficientsof oxy- and deoxyhemoglobin at the 2 ratio points becausethey are nonisosbestic for these 2 proteins. This is consistentwith the reflectance spectrum in Fig. 1, which shows that theratio of absorption coefficients at 625 and 575 nm is greaterfor oxyhemoglobin. The HRP is therefore greater for thevessel with higher concentration of total Hb (recipient Ndonor) and higher oxygen saturation (vein N artery).
Fig. 3 Reflectance intensity during spectral analysis of Hbconcentration in control patients using the “tapping” method(see text for details). A and B, The computed HRP atmaximum reflectance intensity (fiber contact with the bloodvessel) is reproducible with minimal intrapatient variation andcorrelates with serum Hb concentration in 2 patients: (A) HRP3.2 ∼ Hb 14.0 and (B) HRP 2.7 ∼ Hb 10.7. Overlaidreflectance spectra correlating to a peak in the HRP for eachpatient are shown (C).
3. Discussion
Noninvasive optical spectroscopy has been in clinical usefor several decades. The difference in light absorption (andtherefore reflectance) between deoxyhemoglobin and oxy-hemoglobin is the basis for oximetry [11,12] and pulseoximetry [13]. As the spectra of these 2 forms of Hb differ atwavelengths greater than 630 nm, the total reflectance atpredetermined wavelengths in that window can help estimatethe relative concentration of each and, therefore, thepercentage saturation of blood. At less than 630 nm, the 2spectral curves are much more similar. We have previouslydemonstrated that, when vascularized tissues are illuminatedby a light source with known spectral signature, the relativereflectance intensity in the lower end of the visible spectrumcorrelates well with the serum Hb concentration. Thisprinciple has already been applied to design a portablenoninvasive Hb monitor for use in an emergency departmentor office setting [7,9,14].
The present report demonstrates that this principle canalso be applied to estimate Hb concentration duringlaparoscopic and other endoscopic procedures. The ultimategoal of our study was to use Hb concentration as an adjunct

Fig. 4 Reflectance spectra from donor/recipient vein/artery for 2 sets of twins with TTTS. Reflectance intensity normalized for curve peak at630 nm. DA indicates donor artery; DV, donor vein; RA, recipient artery; RV, recipient vein.
63Reflectance spectrometry for real-time Hb determination
in identifying placental vessels in severe TTTS. In thiscondition affecting identical (monochorionic) twin fetuses,one acts as a chronic donor and the other as recipient [1,2]. Insevere cases, the best treatment option is endoscopic fetalintervention to obliterate the connecting placental vessels.The angioarchitecture of the placenta can be complex[6,15,16]; and it is crucial to obliterate all vessels thatconnect both twins, while sparing vessels that belong to 1fetus only [17]. More recent reports further suggest that theorder in which the causative vessels are obliterated impactsoutcome [4,18]. Because the donor is anemic and therecipient polycythemic, the discordant Hb concentrations canbe used to distinguish the vascular territory of each fetus.
The technique was first validated in otherwise normalvolunteers during elective laparoscopic or thoracoscopicprocedures. Three different methods of data capture werecompared, as the circumstances in laparoscopy differ fromthe previously validated spectrometry techniques. In contrastwith the portable monitor used to analyze the conjunctivaltissues [14], the intraoperative setup uses the (strong) lightsource from the endoscopic tower. Furthermore, small- andmedium-sized vessels are interrogated individually, whereasconjunctival analysis captures the reflected light off acapillary bed. Of the 3 sampling methods, the contacttechnique proved to be the most reliable and reproducible: asthe optic fiber nears the target vessel, the intensity of thereflected light increases. The maximum intensity is obtainedas the fiber makes contact with the vessel—this spectrum isthen used to analyze the reflectance curve at predeterminedwavelengths. An artificial quantitative parameter (HRP), theratio of reflected intensity at 625 to 575 nm, was observed tocorrelate with total Hb concentration and was used toobserve the performance of the laparoscopic study.
When used in utero, reflectance spectrometry of theindividual placental vessels clearly demonstrated intratwin
concordance and intertwin discordance in spectral signa-tures. Thus, vessels of donor origin could be distinguishedfrom recipient vessels (Fig. 4). A higher Hb concentration,seen in the recipient, resulted in a lower reflectance (andtherefore higher absorbance) of light at the index wave-length. This trend followed the observations in postnatalendoscopic volunteers and in previous experiments with theconjunctival monitor. However, the waveform was slightlydifferent, reflecting the difference in light source used duringlaparoscopy (xenon) and conjunctival illumination (light-emitting diode). An absolute Hb measurement could notbe obtained, as this would have required a larger numberof normal measurements to construct a nomogram. Further-more, the device cannot yet be used in real time, asthe analysis of the curve was performed post facto.Nevertheless, the results of this preliminary report aresufficiently promising and reproducible that a real-timedevice can be designed with relative Hb value reading forintraoperative use during laser ablation of placental vessels inTTTS. Other uses of this device are conceivable inintraoperative situations where rapid blood loss or fluctua-tions in Hb concentrations are expected, such as trauma.Further studies are under way to combine Hb, oxygensaturation, and blood flow measurements for clinical andresearch purposes.
References
[1] Luks FI, Carr SR, De Paepe ME, et al. What—and why—the pediatricsurgeon should know about twin-to-twin transfusion syndrome.J Pediatr Surg 2005;40:1063-9.
[2] Muratore CS, Carr SR, Lewi L, et al. Survival after laser surgery fortwin-to-twin transfusion syndrome: when are they out of the woods?J Pediatr Surg 2009;44:66-9.

64 S. Curran et al.
[3] Middeldorp JM, Sueters M, Lopriore E, et al. Fetoscopic laser surgeryin 100 pregnancies with severe twin-to-twin transfusion syndrome inthe Netherlands. Fetal Diagn Ther 2007;22:190-4.
[4] Quintero RA, Ishii K, Chmait RH, et al. Sequential selective laserphotocoagulation of communicating vessels in twin-twin transfusionsyndrome. J Matern Fetal Neonatal Med 2007;20:763-8.
[5] Senat MV, Deprest J, Boulvain M, et al. Endoscopic laser surgeryversus serial amnioreduction for severe twin-to-twin transfusionsyndrome. N Engl J Med 2004;351:136-44.
[6] Poch M, Luks FI, Carr SR, et al. Intratwin arteriovenous fistula of theplacenta in a case of twin-to-twin transfusion syndrome. Am JPerinatol 2005;22:3-6.
[7] McMurdy JW, Jay GD, Suner S, et al. Diffuse reflectance spectra ofthe palpebral conjunctiva and its utility as a noninvasive indicator oftotal hemoglobin. J Biomed Opt 2006;014019:11.
[8] McMurdy JW, Jay GD. Anemia detection utilizing diffuse reflectanceof the palpebral conjunctiva and tunable liquid crystal filtertechnology. SPIE 2006;61771:C1-C10.
[9] Suner S, Crawford G, McMurdy J, et al. Non-invasive determinationof hemoglobin by digital photography of palpebral conjunctiva.J Emerg Med 2007;33:105-11.
[10] Chang J, Tracy TF, Carr SR, et al. Port insertion and removaltechniques to minimize premature rupture of the membranes inendoscopic fetal surgery. J Pediatr Surg 2006;41:905-9.
[11] Keogh BF, Kopotic RJ. Recent findings in the use of reflectanceoximetry: a critical review. Curr Opin Anaesthesiol 2005;18:649-54.
[12] Bowes III WA, Corke BC, Hulka J. Pulse oximetry: a review of thetheory, accuracy, and clinical applications. Obstet Gynecol 1989;74:541-6.
[13] Rady MY. The role of central venous oximetry, lactic acidconcentration and shock index in the evaluation of clinical shock: areview. Resuscitation 1992;24:55-60.
[14] Jay GD, Racht J, McMurdy J, et al. Point-of-care noninvasivehemoglobin determination using fiber optic reflectance spectroscopy.Conf Proc IEEE Eng Med Biol Soc 2007;2007:2932-5.
[15] De Paepe ME, Friedman RM, Poch M, et al. Placental findings afterlaser ablation of communicating vessels in twin-to-twin transfusionsyndrome. Pediatr Dev Pathol 2004;7:159-65.
[16] De Paepe ME, Burke S, Luks FI, et al. Demonstration of placentalvascular anatomy in monochorionic twin gestations. Pediatr DevPathol 2002;5:37-44.
[17] Quintero RA, Bornick PW, Morales WJ, et al. Selective photocoag-ulation of communicating vessels in the treatment of monochorionictwins with selective growth retardation. Am J Obstet Gynecol 2001;185:689-96.
[18] van Gemert MJ, van den Wijngaard JP, Lopriore E, et al. Simulatedsequential laser therapy of twin-twin transfusion syndrome. Placenta2008;29:609-13.








![A monochorionic diamniotic twin pregnancy with selective ... · fetoscopy, a sequential Laser placental ablation was performed, identifying 6 anastomoses (5 arteriovenous [AV] and](https://img.pdfslide.net/doc/110x75/5f2d79ce00b49e3aa72f885c/a-monochorionic-diamniotic-twin-pregnancy-with-selective-fetoscopy-a-sequential.jpg)