Embed Size (px)
Citation preview

Refugee
Health
and
Chronic
Disease
What is a Chronic Disease?
WHO Definitions
Cardiovascular
Respiratory
Cancers
Diabetes
Other (kidney;
neurological;
cerebrovascular)
Risk Factors in 2014
Alcohol intake
Cigarette smoking
Hypertension
Obesity
2

In Context…
3
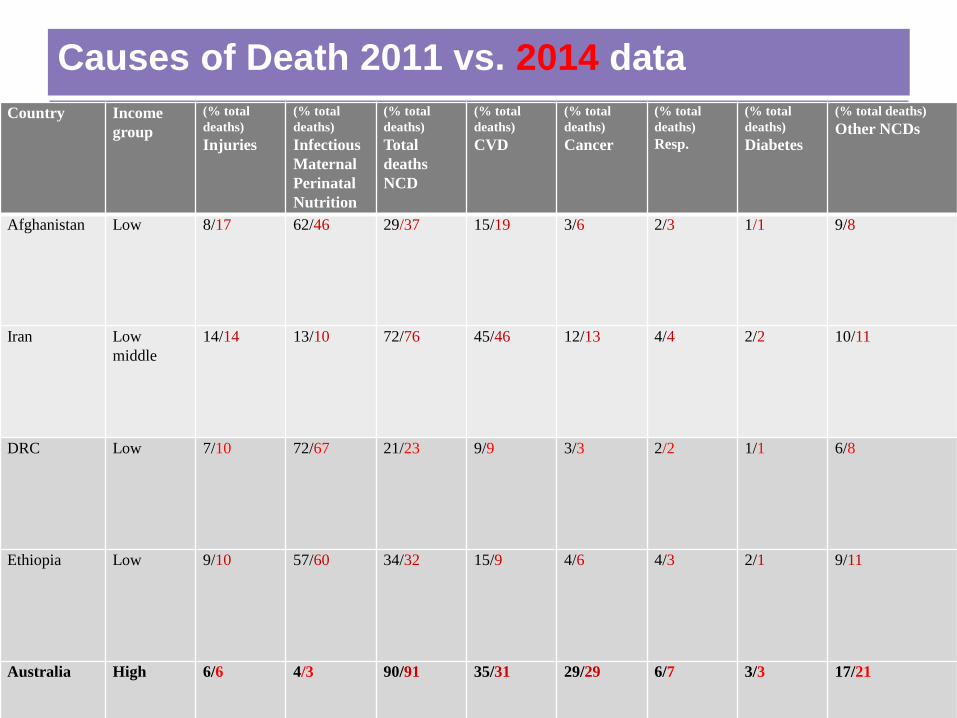
Causes of Death 2011 vs. 2014 data
4
Country Income
group
(% total
deaths)
Injuries
(% total
deaths)
Infectious
Maternal
Perinatal
Nutrition
(% total
deaths)
Total
deaths
NCD
(% total
deaths)
CVD
(% total
deaths)
Cancer
(% total
deaths)
Resp.
(% total
deaths)
Diabetes
(% total deaths)
Other NCDs
Afghanistan Low 8/17 62/46 29/37 15/19 3/6 2/3 1/1 9/8
Iran Low
middle
14/14 13/10 72/76 45/46 12/13 4/4 2/2 10/11
DRC Low 7/10 72/67 21/23 9/9 3/3 2/2 1/1 6/8
Ethiopia Low 9/10 57/60 34/32 15/9 4/6 4/3 2/1 9/11
Australia High 6/6 4/3 90/91 35/31 29/29 6/7 3/3 17/21

CVD Risk Factors 2011 vs 2014 data
Country Smoking Alcohol L. per
head
Physical
inactivity
High BP High blood
glucose
Obesity
Iraq 13.7/18 0.5 55.2 24.4 10.6 27/27
Afghanistan (2008)
- 0.7 - 22.5 - 2.2
Iran 10.4/14 (2011)
1.0 (2010)
35.7 33.7/
24.3
8.3 19.4/
19.4
DRC 4.5/10 (2011)
3.6 (2010)
42.5 37.6/ 29.4 (2008)
- 1.7/1.7 (2008)
Ethiopia 2.4 4.2 17.9 35.2/
25.9
- 1.1/1.1
Australia 16.8/20 12.2 (2010) 40.3 36.4/
21.4
9.4 26.8/
26.8

Humanitarian Program (2)
Rank 2003-2004 2007-2008 2012-2013
1 Sudan Burma Iraq
2 Iraq Iraq Afghanistan
3 Afghanistan Afganistan Myanmar
4 Ethiopia Sudan Bhutan
5 Iran Liberia Congo (DRC)
6 Liberia Congo (DRC) Iran
7 Fmr Yugoslavia Burundi Somalia
8 Sierra Leone Iran Sudan
9 Congo (DRC) Sierra Leone Eritrea
10 Somalia Sri Lanka Ethiopia
6

Refugee Health Conditions in Post Arrival Screening
17 Australian studies/reports, ~ 7000 people and ~ 7000 detainees; 4000 children 7
Problem Prevalence No. Studies Informing
Anaemia 9-30% all groups 8
Iron Deficiency 13-34% all groups 6
Low Vitamin D 60-90% African, 37% Karen 6 African, 2 Karen,
Low Vitamin A 40% African NT 2, Rohingya in QLD
Hepatitis B sAg +ve 2-16%, sAb –ve 60% 12, 5
Hepatitis C 1-3% 8
HIV <1% (0/3 studies) 7
Syphilis 0-5% 9
Other STI Very low 4
Schistosoma 2-39% African, 0-7% Karen 11
Strongyloides 1-21% 8
Malaria 5-10% African, changed with DHC 1
Faecal parasites 16-40% all groups 11
Mantoux positive 3-63%, 18-63% 7 studies 9,7
H. pylori 82% African 1
Need for immunisation Close to 100%

8
Nutritional Deficiencies
Prolonged deprivation and severe hunger
Lack of clean water and nutritious food causes long-term vitamin and mineral
deficiency, especially iron.
Menstruation and breastfeeding – women prone to iron and folate deficiency
Diseases endemic eg: malaria, schistosomiasis, strongyloides
Micro-nutrient deficiency disorders – zinc, manganese, Vitamin A in children
40%), B12 (especially Bhutan/Nepal; no macrocytosis); Vitamin D (90%)
Lead toxicity in some children (Burmese dietary supplements)
Diet-related disorders eg: non-insulin dependent diabetes mellitus
Eating disorders – anorexia/obesity/”Western junk food diet”

Studies have shown…
African Refugees 2010 (Asia Pacific Journal of Clinical Nutrition, vol. 20, no. 3, pp. 397-
403. Prevalence of vitamin D insufficiency and risk factors for type 2 diabetes and cardiovascular
disease among African migrant and refugee adults in Melbourne)
62% overweight/obese
47% insulin resistance
16% hypertension
Journal of Community Health 2/3/2012
Katherine Yun (2006-2010 NE USA Refugee Clinic):
“We found that half of the adult refugees in this sample had at least one chronic
NCD (51.1%), and 9.5% had three or more NCDs. Behavioral health
diagnoses were most common (15.0%), followed by hypertension (13.3%).
Half of adults were overweight or obese (54.6%).”
9

Noncommunicable diseases among urban refugees and asylum-seekers in
developing countries: a neglected health care need
Ahmed Hassan Amara1 * and Syed Mohamed Aljunid2 3
Globalization and Health 2014, 10:24 doi:10.1186/1744-8603-10-24
Major search engines and refugee agency websites were systematically
searched between June and July 2012 for articles and reports on NCD
prevalence among urban refugees.
44,468 refugees and asylum seekers, 75 per cent involved Iraqi refugees.
Most studies were conducted in the Middle East and indicated a high
prevalence of NCDs among urban refugees in this region, but in general, the
prevalence varied by refugees’ region or country of origin.
Hypertension, musculoskeletal disease, diabetes and chronic respiratory
disease were the major diseases observed.
10
Prev Chronic Dis. May 2010; 7(3): A51. Apr 15, 2010.
Chronic Disease and Its Risk Factors Among Refugees and Asylees Massachusetts, 2001-
2005
Nameeta M. Dookeran, MD, MSc, Tracy Battaglia, MD, MPH, Jennifer Cochran, MPH, and
Paul L. Geltman, MD, MPH
Health screening data from 4,239 adult refugees and asylees who arrived in
Massachusetts from January 1, 2001, through December 31, 2005.
We determined prevalence of obesity/overweight, hypertension, coronary artery disease
(CAD), diabetes, and anemia. Almost half of our sample (46.8%) was obese/overweight,
and 22.6% had hypertension.
CAD, diabetes, and anemia were documented in 3.7%, 3.1%, and 12.8%, respectively.
People from the Europe and Central Asia region were more likely than those from other
regions to have CAD.
11

Medical Conditions by Region of Origin of People Who Received Refugee
Health Assessment Services, Massachusetts, 2001-2005 (N = 4,239)a
12
Region Obesity % Overwt % HT % CAD % Diabetes % Anaemia %
Europe
Central Asia (Fmr USSR, Fmr
Yugo.; Albania)
27.3 31.2 32.2 7.8 3.5 9.5
Africa (Somalia, Liberia,
Sudan)
13.3 24.2 16.4 0.5 2.5 19.6
East and SE
Asia (Viet.; Cambodia;
Burma)
3.6 21 9.8 0.6 3.6 5.3
Nr East South
Asia (Afghan.; Iraq;
Iran)
13.6 27.2 11.7 0.5 2.8 12.2
Latin America
and Caribbean (Haiti, Cuba,
Colombia)
18.6 31.2 17.4 0.3 3.3 9.0
All Regions 19.1 27.7 22.6 3.7 3.1 12.8

Prevalence: Refugees and Trauma
Up to 30% of world’s refugee population have
had at least one experience of torture (IRCT,
2011)
80% of refugee women have experienced
sexual abuse or sexual torture (UNHCR)
7/10 refugees on assessment had experienced
physical or psychological violence (Foundation
House, 2010)

Prevalence: Refugees and Psychological
Suffering
PTSD: 32%-100% (various studies 1984-2000:
FH)
Depression: 47-72% (various studies 1987,
1993: FH)
PTSD in up to 20% in children, in some studies
Chronic pain in 65% (of 72 clients in Oslo clinic),
72% of those ‘severe’. Tidsskr Nor Laegeforen. 2006
Feb 23;126(5):608-10.[Chronic pain in traumatized
refugees].Dahl S, Dahl CI, Sandvik L, Hauff E.

Cardiovascular Effects of Traumatic Stress
PTSD – direct relationship to devt of HT (US National Comorbidity
Survey)
Increased activity of SNS and hyperfn of parasympathetic NS
Hyperlipidaemia – Brazilian police officers with PTSD; Croatian
soldiers
Obesity – increased BMI in individuals with PTSD
Coronary heart disease – Dept Vet Affairs USA – normative aging
study
(The Long-term Consequences of Traumatic Stress: Intertwined Physical and
Psychological Consequences. Alexander C. MacFarlane World Psychiatry
2010 Feb v 9(1) 3-10. Supported by NHMRC NHF BeyondBlue)
15

Risk Factors Contributing to Chronic disease
In refugees, changes in diet, physical activity and chronic
stress of poverty, low SES, family separation are factors. 16
Australian Institute of Health and Welfare
Risk Factors for Chronic Disease 2012
•Most Australians have 1 risk factor
•90% reduced veg intake
•50% reduced fruit
•60% reduced physical acitvity (>150mins in 1/52 over 5 sessions)
•80% more than 3 hours each day sitting
•17% males > 5 risk factors cf 11% females
•Increased factors associated with lower SES



















![The “Liberalization” of Refugee Naturalization: Some ......Aug 31, 2016 · 2016] karbasi and refugee naturalization 243 for refugees,”2 for it defines who “refugees” are,](https://img.pdfslide.net/doc/110x75/5f6868f1c373db7227087f6f/the-aoeliberalizationa-of-refugee-naturalization-some-aug-31-2016-.jpg)