Embed Size (px)
Citation preview

●
(rcirslmslhwh0Cn©
I(
CmcmapbsatiiSoutrcnt
rbccci
A
Regional Citrate Anticoagulation for Continuous VenovenousHemodiafiltration Using Calcium-Containing Dialysate
Monika Gupta, MD, Nand K. Wadhwa, MD, and Rose Bukovsky, RN, BSN, CNN
Background: Regional anticoagulation with trisodium citrate for continuous venovenous hemodiafiltrationCVVHDF) is an effective and safe alternative to heparin, especially in patients at high risk for bleeding. However,egional citrate anticoagulation is not used widely because current protocols are complex, labor intensive, andumbersome. Existing protocols require the use of calcium-free dialysate with a continuous systemic calciumnfusion to prevent hypocalcemia. We evaluated Anticoagulant Citrate Dextrose Formula A (ACD-A) solution foregional anticoagulation in CVVHDF in combination with a commercially available calcium-containing dialysisolution. Methods: Thirty-eight patients in the intensive care units underwent citrate-based CVVHDF usingow-calcium peritoneal dialysis solution (calcium, 5.0 mg/dL [1.25 mmol/L]). ACD-A infusion rate was adjusted to
aintain postfilter ionized calcium (iCa��) levels at 1.0 to 2.0 mg/dL (0.25 to 0.5 mmol/L). Calcium chloride (10%)olution was administered intravenously every 6 hours on an as-needed basis to maintain systemic serum iCa��
evels at 3.5 to 4.0 mg/dL (0.88 to 1.0 mmol/L). Results: CVVHDF was performed for a total of 394 days using 149emofilters. Mean hemofilter life span was 63.5 � 27.1 hours. Seventy-five percent, 61%, and 49% of hemofiltersere patent at 24, 48, and 72 hours, respectively. No patient experienced a change in clinical status caused byypocalcemia and/or signs and symptoms of citrate toxicity. Four patients developed metabolic alkalosis requiring.1 N of hydrochloric acid infusion. Conclusion: Our simplified technique of regional citrate anticoagulation forVVHDF using calcium-containing dialysate is not associated with increased hemofilter clotting and obviates theeed for a continuous systemic calcium infusion and calcium-free dialysate. Am J Kidney Dis 43:67-73.2004 by the National Kidney Foundation, Inc.
NDEX WORDS: Citrate anticoagulation; calcium-containing dialysate; Anticoagulant Citrate Dextrose Formula A
ACD-A); continuous venovenous hemodiafiltration (CVVHDF).brscodflshc
oS
b
oCtP
1
ocBn
ONTINUOUS RENAL replacement therapy(CRRT) has been used increasingly for the
anagement of renal failure in hemodynami-ally unstable and critically ill patients.1-6 Theain disadvantage of CRRT is the need for
nticoagulation to prevent clotting of the extracor-oreal circuit, which further increases the risk forleeding in this patient population. Currently,ystemic heparin is used most commonly fornticoagulation in patients on CRRT.7 However,he major drawback of systemic heparin therapys the risk for life-threatening bleeding episodesn the range of 25% to 30% in these patients.3,8,9
aline flushes have been used to prevent clottingf the extracorporeal circuit, but their efficacy isnclear.3,9,10 Alternative methods for anticoagula-ion, namely, regional anticoagulation with hepa-in,11 low-molecular-weight heparin,12 prostacy-lin,13-15 and the serine protease inhibitorafamostat,16 are not used widely because ofheir limitations.
Regional anticoagulation with citrate has beeneported to be effective and safe, with lowerleeding risk.8,17-19 Citrate chelates ionized cal-ium (iCa��) in the extracorporeal circuit. Thisauses anticoagulation of the extracorporeal cir-uit because iCa�� is required for multiple steps
n the clotting cascade. After citrate enters themerican Journal of Kidney Diseases, Vol 43, No 1 (January), 200
ody, it is diluted by the total blood volume andapidly metabolized to bicarbonate by the liver,keletal muscles, and renal cortex. Regional anti-oagulation with citrate increases the complexityf CRRT because of the need for a calcium-freeialysis solution and/or low-sodium replacementuid to avoid metabolic complications and aystemic calcium infusion to prevent and/or treatypocalcemia. We developed a protocol usingalcium-containing peritoneal dialysis solution
From the Department of Medicine, Division of Nephrol-gy and Division of Nursing, State University of New York attony Brook, Stony Brook, NY.Received April 4, 2003; accepted in revised form Septem-
er 3, 2003.Presented as a poster at the 8th International Conference
n Continuous Renal Replacement Therapies, San Diego,A, March 6-8, 2003, and 35th Annual Meeting and Scien-
ific Exposition of the American Society of Nephrology,hiladelphia, PA, November 1-4, 2002.Published in abstract form in the J Am Soc Nephrol
3:605A, 2002 and Blood Purif 21:199, 2003.Address reprint requests to Nand K. Wadhwa, MD, Division
f Nephrology, Department of Medicine, School of Medi-ine, HSC T-15 Rm-020, State University of NY at Stonyrook, Stony Brook NY 11794. E-mail: [email protected]© 2004 by the National Kidney Foundation, Inc.0272-6386/04/4301-0008$30.00/0
doi:10.1053/j.ajkd.2003.09.0144: pp 67-73 67

itghear
pCsJqm
dfwt(sw
rflmadpL[0iumcioti1bn1S
vtcmtvm
r0
Myldi4frtv
hpfirbmhmep
ptcmaT2s
S
b
GUPTA, WADHWA, AND BUKOVSKY68
n combination with Anticoagulant Citrate Dex-rose Formula A (ACD-A) solution as the re-ional anticoagulant in continuous venovenousemodiafiltration (CVVHDF), consequentlyliminating the need for a customized dialysatend continuous systemic calcium infusion. Weeport our experience.
METHODS
We retrospectively reviewed the medical records of 38atients with renal failure who had undergone citrate-basedVVHDF using calcium-containing dialysate in the inten-
ive care units (ICUs) at our tertiary-care institution fromanuary 2001 to September 2002. We evaluated the fre-uency of hemofilter clotting, hypocalcemia, hypernatremia,etabolic alkalosis, and citrate toxicity.Vascular access was established by insertion of a 12-Fr
ual-lumen catheter (Arrow Int, Reading, PA) in either aemoral, internal jugular, or subclavian vein. Blood flow rateas set and maintained at 150 mL/min throughout the
reatment. The Prisma M100 set with an AN69 hemofilterCobe, Lakewood, CO) was primed with 1 L of normalaline containing 5,000 IU of heparin. The Prisma M100 setas changed every 96 hours.Isotonic saline (sodium, 154 mEq/L [154 mmol/L]; chlo-
ide, 154 mEq/L [154 mmol/L]) was used as replacementuid and infused proximal to the hemofilter at 500 to 1,000L/h. Magnesium sulfate and/or potassium chloride were
dded to the replacement fluid by the pharmacy at theiscretion of the attending nephrologist. A low-calciumeritoneal dialysis solution (sodium, 132 mEq/L [132 mmol/]; calcium, 5.0 mg/dL [1.25 mmol/L]; chloride, 95 mEq/L
95 mmol/L]; lactate, 360 mg/dL [40 mmol/L]; magnesium,.5 mEq/L [0.25 mmol/L]; 1.5% dextrose, pH 5.2; osmolar-ty, 344 mOsm/L; Baxter Healthcare, Deerfield, IL) wassed as dialysate. Dialysate was delivered at 500 to 1,000L/h. ACD-A (3% solution: trisodium citrate, 2.2%; and
itric acid, 0.8%; 112.9 mmol of citrate/L; Baxter) wasnitiated at 150 mL/h through a Y connection at the junctionf the double-lumen hemodialysis catheter and prefilterubing. ACD-A rate was adjusted to maintain posthemofilterCa�� levels at 1.0 to 2.0 mg/dL (0.25 to 0.5 mmol/L; Table). Serum electrolytes, arterial blood gases, and completelood cell count were measured at least twice a day and aseeded. Systemic and posthemofilter iCa�� were measuredhour after initiation of CVVHDF and then every 6 hours.
��
Table 1. Algorithm to Adjust the Rate of ACD-AInfusion
Posthemofilter iCa�� (mg/dL) Change in ACD-A Infusion Rate
�2.00 Increase rate by 10 mL/h1.00-2.00 No change in rate
�1.00 Decrease rate by 10 mL/h
NOTE. To convert iCa�� from mg/dL to mmol/L, multiplyy 0.25.
ystemic iCa samples were drawn from an existing intra- b
enous access. Postfilter iCa�� samples were drawn fromhe blood sampling port distal to the hemofilter. Calciumhloride (10% solution; 13.6 mEq (6.8 mmol) of Ca��/10L) was administered on an as-needed basis as an intermit-
ent intravenous bolus every 6 hours to maintain systemicenous iCa�� levels at 3.5 to 4.0 mg/dL (0.88 to 1.0mol/L; Table 2).Data are presented as mean � SD. t-Test and nonparamet-
ic Wilcoxon’s test were used when appropriate. P less than.05 is considered statistically significant.
RESULTS
Patient characteristics are listed in Table 3.ean age was 55 � 16 years (range, 23 to 83
ears). All patients were mechanically venti-ated, hemodynamically unstable, and pressorependent. Fluid overload was the most commonndication for initiating CVVHDF. Thirty-three,, and 1 patients had a dual-lumen catheter in theemoral, internal jugular, and subclavian veins,espectively. CVVHDF was performed for a to-al of 394 days using 149 M 100 sets. Treatmentariables during CVVHDF are listed in Table 4.The hemofilter lasted a mean of 63.5 � 27.1
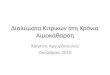
ours. Twenty-six percent of hemofilters wereatent at 96 hours. Twenty-six percent of hemo-lters were discontinued before 96 hours foreasons other than clotting, and 25% were lostecause of catheter malfunction. The censoredean survival of hemofilters was 74.2 � 24.3
ours (excluding filters lost because of catheteralfunction or reasons other than clotting). Sev-
nty-five percent and 61% of hemofilters wereatent at 24 and 48 hours, respectively (Fig 1).Eight patients had coagulopathy defined as a
latelet count less than 75,000/�L and/or interna-ional normalized ratio greater than 2.5. To ex-lude an artificial effect of coagulopathy on he-ofilter survival, we performed a separate
nalysis of data from the remaining 30 patients.he censored hemofilter life span was 64.36 �5.99 hours. This was not different in compari-on to the group as a whole. There was no effect
Table 2. Schemata for Calcium Administration
erum iCa�� (mg/dL) 10% Calcium Chloride (mL)
3.5-4.0 03.0-3.4 10�3.0 20
NOTE. To convert iCa�� from mg/dL to mmol/L, multiply
y 0.25.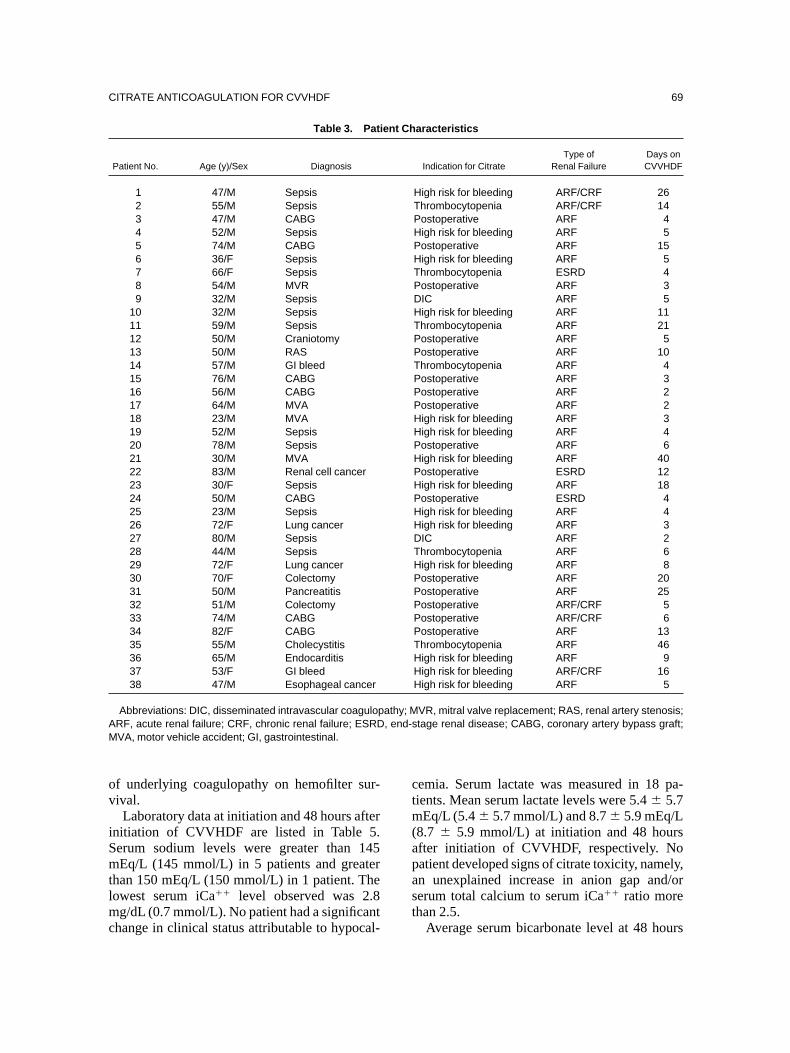
ov
iSmtlmc
ctm(apast
AM
CITRATE ANTICOAGULATION FOR CVVHDF 69
f underlying coagulopathy on hemofilter sur-ival.Laboratory data at initiation and 48 hours after
nitiation of CVVHDF are listed in Table 5.erum sodium levels were greater than 145Eq/L (145 mmol/L) in 5 patients and greater
han 150 mEq/L (150 mmol/L) in 1 patient. Theowest serum iCa�� level observed was 2.8g/dL (0.7 mmol/L). No patient had a significant
Table 3. Pati
Patient No. Age (y)/Sex Diagnosis
1 47/M Sepsis2 55/M Sepsis3 47/M CABG4 52/M Sepsis5 74/M CABG6 36/F Sepsis7 66/F Sepsis8 54/M MVR9 32/M Sepsis
10 32/M Sepsis11 59/M Sepsis12 50/M Craniotomy13 50/M RAS14 57/M GI bleed15 76/M CABG16 56/M CABG17 64/M MVA18 23/M MVA19 52/M Sepsis20 78/M Sepsis21 30/M MVA22 83/M Renal cell cancer23 30/F Sepsis24 50/M CABG25 23/M Sepsis26 72/F Lung cancer27 80/M Sepsis28 44/M Sepsis29 72/F Lung cancer30 70/F Colectomy31 50/M Pancreatitis32 51/M Colectomy33 74/M CABG34 82/F CABG35 55/M Cholecystitis36 65/M Endocarditis37 53/F GI bleed38 47/M Esophageal cancer
Abbreviations: DIC, disseminated intravascular coagulopRF, acute renal failure; CRF, chronic renal failure; ESRDVA, motor vehicle accident; GI, gastrointestinal.
hange in clinical status attributable to hypocal-
emia. Serum lactate was measured in 18 pa-ients. Mean serum lactate levels were 5.4 � 5.7Eq/L (5.4 � 5.7 mmol/L) and 8.7 � 5.9 mEq/L
8.7 � 5.9 mmol/L) at initiation and 48 hoursfter initiation of CVVHDF, respectively. Noatient developed signs of citrate toxicity, namely,n unexplained increase in anion gap and/orerum total calcium to serum iCa�� ratio morehan 2.5.
aracteristics
Indication for CitrateType of
Renal FailureDays onCVVHDF
High risk for bleeding ARF/CRF 26Thrombocytopenia ARF/CRF 14Postoperative ARF 4High risk for bleeding ARF 5Postoperative ARF 15High risk for bleeding ARF 5Thrombocytopenia ESRD 4Postoperative ARF 3DIC ARF 5High risk for bleeding ARF 11Thrombocytopenia ARF 21Postoperative ARF 5Postoperative ARF 10Thrombocytopenia ARF 4Postoperative ARF 3Postoperative ARF 2Postoperative ARF 2High risk for bleeding ARF 3High risk for bleeding ARF 4Postoperative ARF 6High risk for bleeding ARF 40Postoperative ESRD 12High risk for bleeding ARF 18Postoperative ESRD 4High risk for bleeding ARF 4High risk for bleeding ARF 3DIC ARF 2Thrombocytopenia ARF 6High risk for bleeding ARF 8Postoperative ARF 20Postoperative ARF 25Postoperative ARF/CRF 5Postoperative ARF/CRF 6Postoperative ARF 13Thrombocytopenia ARF 46High risk for bleeding ARF 9High risk for bleeding ARF/CRF 16High risk for bleeding ARF 5
VR, mitral valve replacement; RAS, renal artery stenosis;tage renal disease; CABG, coronary artery bypass graft;
ent Ch
athy; M, end-s
Average serum bicarbonate level at 48 hours

wLrsctamlCind0slCgbihf
emptVsaflrbia1ssiad
cnS46cw
airCrcm
ADPC
b
pe
GUPTA, WADHWA, AND BUKOVSKY70
as 26.83 � 6.54 mEq/L (26.83 � 6.54 mmol/). Four patients developed metabolic alkalosis
equiring 0.1 N of hydrochloric acid (HCl) infu-ion. This was observed in our early attempts atitrate-based CVVHDF. There was no correla-ion between degree of alkalosis, hypernatremia,nd citrate dose. The first patient developedetabolic alkalosis with a serum bicarbonate
evel of 36 mEq/L (36 mmol/L) after being onVVHDF therapy for 10 days. This was related
n part to acetate present in the total parentalutrition solution. Alkalosis was reversed byiscontinuation of acetate and administration of.1 N of HCl, 100 mL/h, for 36 hours. Theecond patient developed a serum bicarbonateevel of 34 mEq/L (34 mmol/L) after 6 days ofVVHDF therapy. This was related to nasalastric aspiration in this patient with small-owel obstruction. Alkalosis was corrected bynfusion of HCl for 24 hours and the addition ofistamine2 blockers (famotidine). The third andourth patients developed serum bicarbonate lev-
Table 4. Treatment Variables During CVVHDF
Variable Mean � SD
CD-A infusion rate (mL/h) 159 � 10.78*ialysate infusion rate (mL/h) 679.6 � 63.2ostfilter iCa�� (mg/dL) 1.5 � 0.20alcium administered per day(mEq/d [mmol/d]) 10.8 � 8.7 (5.4 � 4.35)
NOTE. To convert Ca�� from mg/dL to mmol/L, multiplyy 0.25.*Equals 0.97 � 1.22 mmol of citrate per hour and
rovides 1.99 � 0.14 mmol of citrate per/L of blood in thextracorporeal circuit.
ls of 32 mEq/L (32 mmol/L) and 31 mEq/L (31mol/L), probably caused by increased hepatic
roduction of bicarbonate from citrate and lac-ate metabolism. Both patients had been on CV-HDF therapy for 7 days. Mean ACD-A infu-
ion rates were 170 and 180 mL/h for patients 3nd 4, respectively. Dialysate and replacementuid infusion rates were 750 and 500 mL/h,espectively. Metabolic alkalosis was reversedy decreasing the dialysate rate to 500 mL/h andncreasing the replacement fluid rate to 750 mL/h,long with the administration of 0.1 N of HCl for2 hours. Although total exposure to the dialy-ate and replacement fluid remained constant,evere metabolic alkalosis was corrected by anncrease in the convective loss of bicarbonate,long with reduced exposure of lactate from theialysate.
DISCUSSION
We report the use of ACD-A with calcium-ontaining dialysate in CVVHDF, obviating theeed for a continuous systemic calcium infusion.ixty-one percent of hemofilters were patent at8 hours. Mean life span of the hemofilter was3.5 � 27.1 hours. Clinically significant hypocal-emia related to the use of citrate anticoagulationas not observed.Morita et al21 described the use of citrate for
nticoagulation during intermittent hemodialysisn 1961. It was not until the late 1980s thategional citrate anticoagulation was first used forRRT. Despite the simple basic principle behind
egional citrate anticoagulation, current proto-ols are complex, and concerns about potentialetabolic abnormalities exist. This makes hepa-
Fig 1. Percentage of func-
tioning hemofilters over time.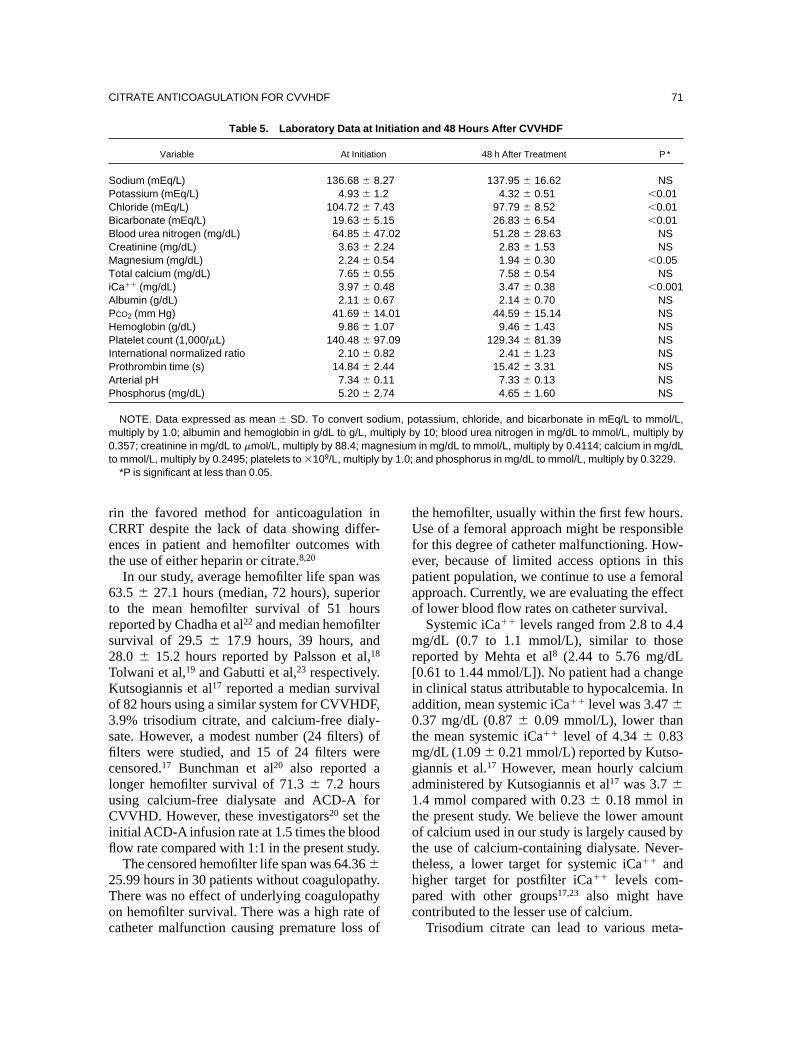
rCet
6trs2TKo3sficluCifl
2Toc
tUfepao
mr[ia0tmga1totthpc
SPCBBCMTiAPHPIPAP
m0t
CITRATE ANTICOAGULATION FOR CVVHDF 71
in the favored method for anticoagulation inRRT despite the lack of data showing differ-nces in patient and hemofilter outcomes withhe use of either heparin or citrate.8,20
In our study, average hemofilter life span was3.5 � 27.1 hours (median, 72 hours), superioro the mean hemofilter survival of 51 hourseported by Chadha et al22 and median hemofilterurvival of 29.5 � 17.9 hours, 39 hours, and8.0 � 15.2 hours reported by Palsson et al,18
olwani et al,19 and Gabutti et al,23 respectively.utsogiannis et al17 reported a median survivalf 82 hours using a similar system for CVVHDF,.9% trisodium citrate, and calcium-free dialy-ate. However, a modest number (24 filters) oflters were studied, and 15 of 24 filters wereensored.17 Bunchman et al20 also reported aonger hemofilter survival of 71.3 � 7.2 hourssing calcium-free dialysate and ACD-A forVVHD. However, these investigators20 set the
nitial ACD-A infusion rate at 1.5 times the bloodow rate compared with 1:1 in the present study.The censored hemofilter life span was 64.36 �
5.99 hours in 30 patients without coagulopathy.here was no effect of underlying coagulopathyn hemofilter survival. There was a high rate of
Table 5. Laboratory Data at In
Variable At Initiatio
odium (mEq/L) 136.68 � 8.otassium (mEq/L) 4.93 � 1.hloride (mEq/L) 104.72 � 7.icarbonate (mEq/L) 19.63 � 5.lood urea nitrogen (mg/dL) 64.85 � 47reatinine (mg/dL) 3.63 � 2.agnesium (mg/dL) 2.24 � 0.otal calcium (mg/dL) 7.65 � 0.
Ca�� (mg/dL) 3.97 � 0.lbumin (g/dL) 2.11 � 0.CO2 (mm Hg) 41.69 � 14emoglobin (g/dL) 9.86 � 1.latelet count (1,000/�L) 140.48 � 97
nternational normalized ratio 2.10 � 0.rothrombin time (s) 14.84 � 2.rterial pH 7.34 � 0.hosphorus (mg/dL) 5.20 � 2.
NOTE. Data expressed as mean � SD. To convert sodultiply by 1.0; albumin and hemoglobin in g/dL to g/L, mu.357; creatinine in mg/dL to �mol/L, multiply by 88.4; mago mmol/L, multiply by 0.2495; platelets to �109/L, multiply
*P is significant at less than 0.05.
atheter malfunction causing premature loss of
he hemofilter, usually within the first few hours.se of a femoral approach might be responsible
or this degree of catheter malfunctioning. How-ver, because of limited access options in thisatient population, we continue to use a femoralpproach. Currently, we are evaluating the effectf lower blood flow rates on catheter survival.
Systemic iCa�� levels ranged from 2.8 to 4.4g/dL (0.7 to 1.1 mmol/L), similar to those
eported by Mehta et al8 (2.44 to 5.76 mg/dL0.61 to 1.44 mmol/L]). No patient had a changen clinical status attributable to hypocalcemia. Inddition, mean systemic iCa�� level was 3.47 �.37 mg/dL (0.87 � 0.09 mmol/L), lower thanhe mean systemic iCa�� level of 4.34 � 0.83
g/dL (1.09 � 0.21 mmol/L) reported by Kutso-iannis et al.17 However, mean hourly calciumdministered by Kutsogiannis et al17 was 3.7 �.4 mmol compared with 0.23 � 0.18 mmol inhe present study. We believe the lower amountf calcium used in our study is largely caused byhe use of calcium-containing dialysate. Never-heless, a lower target for systemic iCa�� andigher target for postfilter iCa�� levels com-ared with other groups17,23 also might haveontributed to the lesser use of calcium.
n and 48 Hours After CVVHDF
48 h After Treatment P *
137.95 � 16.62 NS4.32 � 0.51 �0.01
97.79 � 8.52 �0.0126.83 � 6.54 �0.0151.28 � 28.63 NS2.83 � 1.53 NS1.94 � 0.30 �0.057.58 � 0.54 NS3.47 � 0.38 �0.0012.14 � 0.70 NS
44.59 � 15.14 NS9.46 � 1.43 NS
129.34 � 81.39 NS2.41 � 1.23 NS
15.42 � 3.31 NS7.33 � 0.13 NS4.65 � 1.60 NS
otassium, chloride, and bicarbonate in mEq/L to mmol/L,y 10; blood urea nitrogen in mg/dL to mmol/L, multiply byin mg/dL to mmol/L, multiply by 0.4114; calcium in mg/dL
and phosphorus in mg/dL to mmol/L, multiply by 0.3229.
itiatio
n
2724315.02
2454554867.01
07.09
82441174
ium, pltiply bnesiumby 1.0;
Trisodium citrate can lead to various meta-

bansswmmltaiirsh
ltbbC6bTismtmCl
ilitatptgathl(5oeT
lhthmdhb
Aacdcc
R(IcNp
hos
ac9
ae
v
cof
aiM
r8
gh9
a
GUPTA, WADHWA, AND BUKOVSKY72
olic disturbances, including hypernatremia8,21
nd metabolic alkalosis.24 The incidence of hyper-atremia in our study was similar to that ob-erved by other investigators.17,20,23 Mean serumodium level 48 hours after initiation of CVVHDFas 137.95 � 16.62 mEq/L (137.95 � 16.62mol/L; range, 130 to 154 mEq/L [130 to 154mol/L]). Only 1 patient had a serum sodium
evel greater than 150 mEq/L (150 mmol/L). Inhis patient, serum sodium levels normalizedfter the replacement fluid was switched fromsotonic saline to 0.45% sodium chloride. Thencidence of hypernatremia was lower than thateported by Mehta et al8 because there is lowerodium exposure with ACD-A compared withypertonic citrate.The risk for alkalosis with ACD-A also is
ower compared with hypertonic trisodium ci-rate because the former produces 33% less bicar-onate.25 In the present study, average serumicarbonate level 48 hours after initiation ofVVHDF was 26.83 � 6.54 mEq/L (26.83 �.54 mmol/L). Four patients developed meta-olic alkalosis requiring 0.1 N of HCl infusion.his was seen only in our initial patients undergo-
ng citrate-based CVVHDF. Adjustment of dialy-ate and replacement fluid infusion rates andinimum use of acetate in total parental nutri-
ion subsequently eliminated the development ofetabolic alkalosis in these patients duringVVHDF using ACD-A solution as anticoagu-
ant.No increase in arterial pH was seen despite an
ncrease in serum bicarbonate levels. We calcu-ated anion gap to evaluate for possible coexist-ng metabolic acidosis caused by the accumula-ion of unmeasured acids, namely, lactic acidnd/or citric acid. Citrate can accumulate whenhe citrate infusion rate (ACD-A) exceeds he-atic metabolism and dialysate clearance of ci-rate. This is reflected by an unexplained anionap acidosis, referred to as citrate gap. There wasn increase in mean anion gap from 13.80 � 7.31o 17.75 � 10.14 (P � not significant [NS]) at 48ours after initiation of CVVHDF. Mean serumactate levels increased from 5.4 � 5.7 mEq/L5.4 � 5.7 mmol/L) to 8.7 � 5.9 mEq/L (8.7 �.9 mmol/L; P � NS) at 48 hours after initiationf CVVHDF. This increase in anion gap wasxplained mainly by the degree of lactic acidosis.
here was no evidence of citrate gap. We believe Iactic acidosis was caused primarily by tissueypoperfusion in these critically ill patients, al-hough the lactate in the dialysate also mightave contributed. In addition, all patients wereechanically ventilated. Infusion of 0.9% so-
ium chloride as replacement fluid also mightave counteracted the increase in pH to a degreeecause 0.9% sodium chloride is acidic (pH 5.4).In summary, results from this study show that
CD-A is an effective and safe regional antico-gulant for CVVHDF when used with calcium-ontaining dialysate. Use of calcium-containingialysate allows for the omission of a continuousalcium infusion and eliminates the need for austom-made dialysis solution.
ACKNOWLEDGMENT
The authors thank nurse clinicians Mary J. Longobucco,N, and Christine Teague, RN; dialysis staff; and ICU staff
Cardiovascular Intensive Care Unit, Medical ICU, SurgicalCU, and Coronary Care Unit) at University Hospital Medi-al Center, State University of New York at Stony Brook,Y, for their support in running a successful CVVHDFrogram.
REFERENCES
1. Kramer P, Wigger W, Rieger J, et al: Arteriovenousaemofiltration: A new and simple method for treatment ofver-hydrated patients resistant to diuretics. Klin Wochen-chr 55:1121-1122, 1977
2. Lauer A, Saccaggi A, Ronco C, et al: Continuousrteriovenous hemofiltration in the critically ill patient: Clini-al use and operational characteristics. Ann Intern Med9:455-460, 19833. Kaplan AA, Longnecker RE, Folkert VW: Continuous
rteriovenous hemofiltration. A report of six months’ experi-nce. Ann Intern Med 100:358-367, 1984
4. Schneider NS, Geronemus RP: Continuous arterio-enous hemodialysis. Kidney Int Suppl 33:S159-S162, 19885. Barzilay E, Weksler N, Kessler D, et al: The use of
ontinuous arteriovenous hemodialysis in the managementf patients with oliguria associated with multiple organailure. Intensive Care Med 14:444-445, 1988
6. Bellomo R, Boyce N: Continuous venovenous hemodi-filtration compared with conventional dialysis in criticallyll patients with acute renal failure. ASAIO J 39:M794-
797, 19937. Abramson S, Niles JL: Anticoagulation in continuous
enal replacement therapy. Curr Opin Nephrol Hypertens:701-707, 19998. Mehta RL, McDonald BR, Aguilar MM, et al: Re-
ional citrate anticoagulation for continuous arteriovenousemodialysis in critically ill patients. Kidney Int 38:976-81, 19909. Ward DM, Mehta RL: Extracorporeal management of
cute renal failure patients at high risk of bleeding. Kidney
nt Suppl 43:S237-S244, 1993
s
cT
tcO
av1
(t
tipN
mc1
ct
ip1
fit
ha
aM
ar
am2
ta2
gc
CITRATE ANTICOAGULATION FOR CVVHDF 73
10. Paganini EP: Slow continuous hemofiltration andlow continuous ultrafiltration. ASAIO Trans 34:63-66, 1988
11. Kaplan AA, Petrillo R: Regional heparinization forontinuous arterio-venous hemofiltration (CAVH). ASAIOrans 33:312-315, 198712. Jeffrey RF, Khan AA, Douglas JT, et al: Anticoagula-
ion with low molecular weight heparin (Fragmin) duringontinuous hemodialysis in the intensive care unit. Artifrgans 17:717-720, 199313. Langenecker SA, Felfernig M, Werba A, et al: Antico-
gulation with prostacyclin and heparin during continuousenovenous hemofiltration. Crit Care Med 22:1774-1781,99414. Canaud B, Mion C, Arujo A, et al: Prostacyclin
epoprostenol) as the sole antithrombotic agent in postdilu-ional hemofiltration. Nephron 48:206-212, 1988
15. Davenport A, Will EJ, Davison AM: Comparison ofhe use of standard heparin and prostacyclin anticoagulationn spontaneous and pump-driven extracorporeal circuits inatients with combined acute renal and hepatic failure.ephron 66:431-437, 199416. Ohtake Y, Hirasawa H, Sugai T, et al: Nafamostatesylate as anticoagulant in continuous hemofiltration and
ontinuous hemodiafiltration. Contrib Nephrol 93:215-217,99117. Kutsogiannis DJ, Mayers I, Chin WD, et al: Regional
itrate anticoagulation in continuous venovenous hemodiafil-
ration. Am J Kidney Dis 35:802-811, 2000 218. Palsson R, Niles JL: Regional citrate anticoagulationn continuous venovenous hemofiltration in critically illatients with a high risk of bleeding. Kidney Int 55:1991-997, 199919. Tolwani AJ, Campbell RC, Schenk MB, et al: Simpli-
ed citrate anticoagulation for continuous renal replacementherapy. Kidney Int 60:370-374, 2001
20. Bunchman TE, Maxvold NJ, Barnett J, et al: Pediatricemofiltration: Normocarb dialysate solution with citratenticoagulation. Pediatr Nephrol 17:150-154, 2002
21. Morita Y, Johnson RW, Dorn RE, et al: Regionalnticoagulation during hemodialysis using citrate. Am Jed Sci 242:32-42, 196122. Chadha V, Garg U, Warady BA, et al: Citrate clear-
nce in children receiving continuous venovenous renaleplacement therapy. Pediatr Nephrol 17:819-824, 2002
23. Gabutti L, Marone C, Colucci G, et al: Citrate antico-gulation in continuous venovenous hemodiafiltration: Aetabolic challenge. Intensive Care Med 28:1419-1425,
00224. Mehta RL, McDonald BR, Ward DM: Regional ci-
rate anticoagulation for continuous arteriovenous hemodi-lysis. An update after 12 months. Contrib Nephrol 93:210-14, 199125. Flanigan MJ, Pillsbury L, Sadewasser G, et al: Re-
ional hemodialysis anticoagulation: Hypertonic tri-sodiumitrate or anticoagulant citrate dextrose-A. Am J Kidney Dis
7:519-524, 1996
























![[H. Kawanishi, A. C. Yamashita] Hemodiafiltration (BookFi.org)](https://img.pdfslide.net/doc/110x75/55cf94bf550346f57ba41c26/h-kawanishi-a-c-yamashita-hemodiafiltration-bookfiorg.jpg)

