Embed Size (px)
Citation preview

BIO 510 INTRODUCTION TO BIOMEDICAL INFORMATICS
Registries
Ronda Adkins
12/2/2009

2
What are Registries?
Registries are organized systems used for collecting, storing, retrieving, analyzing, and
circulating information pertaining to a certain disease, condition or risk factor, which can lead
to the occurrence of a health-related event, or previous exposure to something that can cause
harmful health effects.1 The information that is collected for registries is secondary data.
Primary data is collected and entered into a health record during a physician visit and is patient-
identifiable. Secondary data, which usually is not patient-identifiable, originates from the
primary health record. Other resources for collecting health related information include lab
reports, public health surveillance systems for notifiable diseases, hospital discharge records,
surveys, and vital statistics.
Registries have some distinguishing characteristics from their information sources. First, they
focus on a specific disease or group of diseases, or exposure. Second, the data collected comes
from various sources. Third, cases are actively discovered by going through referral sources. For
example, to find cases with trauma diagnoses, a Hospital Information System (HIS) system can
query the trauma register, looking for cases with ICD-9-CM (International Classification of
Diseases, Ninth edition, Clinical Modification) codes pertaining to trauma.2 Registries also
conduct follow-up investigations and data collection on people enrolled in the registry; an
example in this case would be determining the status of cancer registrants by examining vital
statistics.3 Finally, registries are very expensive because data must be found and linked to
multiple sources.
3
Registry Examples
Registries can be constructed for any kind of disease or condition. There is even a registry that
was developed for health care administrative purposes called the National Provider Registry.
Other examples include these:
Immunization Registries –The focus of immunization registries is to help clinicians
evaluate immunization status of their patients. The registries are computerized and help
facilitate vaccination reminders. They also allow public health officials who are reviewing
vaccination coverage in a community to target groups of people who might need priority
treatment. On a national level, registries help in immunizing people so that they are protected
against vaccine-preventable diseases. The success of these immunization registries involves
data exchange through interoperable Immunization Information systems (IIS), or Immunization
Registries, building partnerships with and between current partner organizations, and creating
new public/private partnership opportunities with other national organizations on common
issues related to IIS.4
Trauma Registries –Trauma registries are typically based in the health care facility, but
may include regional or state data. Traumatic injury cases are identified from the health record
and entered into the database, providing baseline estimates on current injury information. This
data meets the needs of trauma care assessment on a national level, clinical outcomes
research, and injury surveillance.5
National Exposure Registry – Operated by the Agency for Toxic Substances and Disease
Registries (ATSDR), this registry identifies individuals who may have been exposed to hazardous

4
material. Long term consequences of exposures are identified by conducting follow-up
monitoring.
Cancer Registries –Data that is collected for cancer registries includes, but is not limited
to, diagnosis methods, treatment, trends, and pathological data. Skin cancers that do not
metastasize are excluded from the registry; however, benign and borderline brain/central
nervous system tumors must be collected by the National Program of Cancer Registries (CDC
2008).6
Data Collection
The terminology, case definition, is used to define how registries collect uniform and
meaningful patient data, and is the first step in data collection.7 The second step in collecting
data is called case finding. Case finding involves patient identification pertinent to a specific
health concern and extrapolating data from their paper-based health record into the registry.
There is a means of collected information from other databases by electronic data capture, a
computerized system that collects clinical data.
Typical information collected from a patient record includes: demographics, patient’s diagnosis,
ICD-9-CM diagnosis and procedure codes; however, other collected data may include lab
reports, tracked patient visits and follow-up. Once data is entered into the registry from the
multitude of sources, the aggregated data can be used to identify patterns and trends in patient
care, determine the magnitude of the medical problem at hand, and identify high risk groups.
5
The importance of this data is measured by the accuracy and completeness of data to local,
state, national, and international organizations. Reports resulting from the registries provide
knowledge to make important public health decisions. The cancer registry, for example,
provides an aggregate of data in a formal annual report that includes the number of cancer
cases in the past year, site and type of cancer. In the case of trauma registries, the American
college of Surgeons certifies hospitals by trauma level based on which center receives the most
serious cases and provides the best level of trauma care. Diabetes registries may provide the
incidence of diabetes in a particular geographic location. The Food and Drug Administration
receives reports from implant registries to track specific product performances, including
recalls. Transplant registries track donor registries and potential donors.
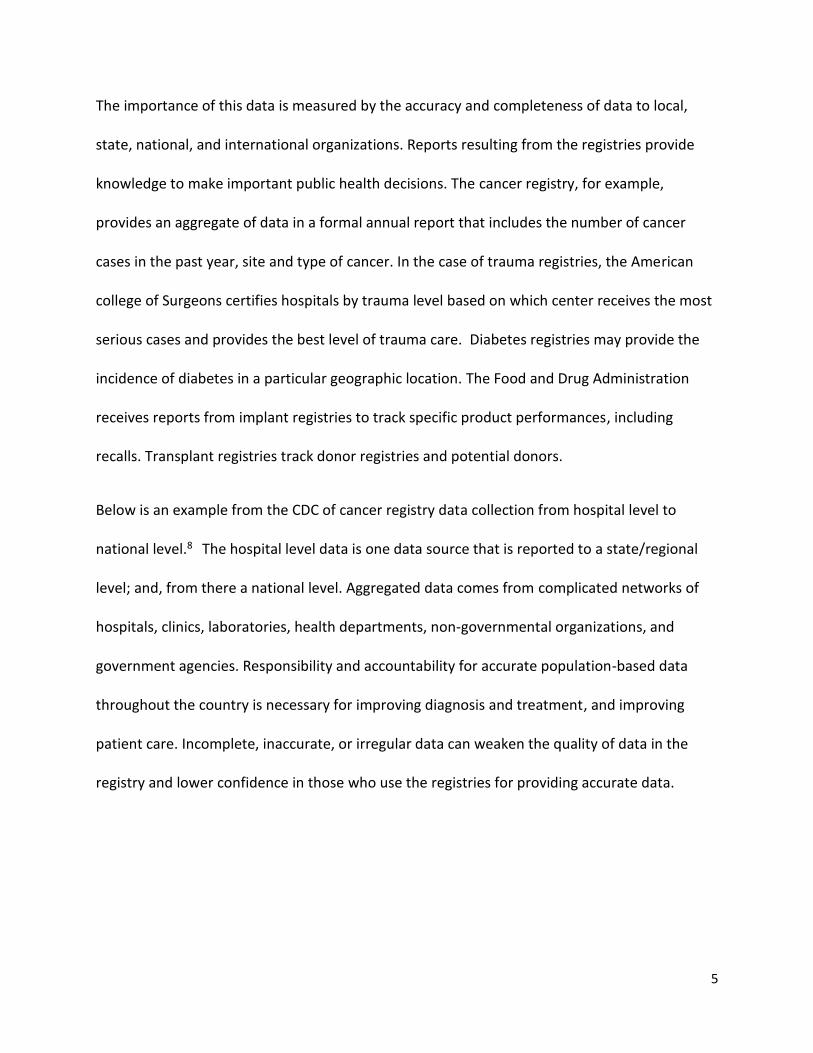
Below is an example from the CDC of cancer registry data collection from hospital level to
national level.8 The hospital level data is one data source that is reported to a state/regional
level; and, from there a national level. Aggregated data comes from complicated networks of
hospitals, clinics, laboratories, health departments, non-governmental organizations, and
government agencies. Responsibility and accountability for accurate population-based data
throughout the country is necessary for improving diagnosis and treatment, and improving
patient care. Incomplete, inaccurate, or irregular data can weaken the quality of data in the
registry and lower confidence in those who use the registries for providing accurate data.

6
Methods of Data Collection
Although registries and databases are mostly computerized, the data collection is typically done
by hand, a daunting task. Collecting and identifying data is time consuming, demanding of
resources, and poses a risk for transcription errors. Data must be interpreted or translated
before entering into the computer much of the time; sometimes because of free text form
which is not standardized, unlike coding that is classified and standardized.9 Coding, unlike
free text, can also be incorrectly entered. Error identification is very difficult. As mentioned in
Connecting for Health’s Common Framework, “data problems represent the dark side of the
tremendous potential offered by the adoption of health IT systems.”10

7
As for ways in which data can be collected, Jan Walker, et al (2005) conducted a study that
resulted in four classifications on how health care units share information11:
Level 1: Nonelectronic data – No use of IT, such as phone and mail
Level 2: Machine –Transportable data - Nonstandardized information transmitted by
basic IT; the document information is not capable of being electronically manipulated (fax
or PC based exchange of scanned documents, pictures, or portable document format
(PDF) files
Level 3: Machine-organizable data - Structured messages having nonstandardized data
and requires interfaces that translate data from the sending organization’s vocabulary to
the receiving organization’s vocabulary; the translations usually result in flawed
translations due to incompatible vocabularies, i.e. e-mail of free text, or PC-based
exchange of files in incompatible/proprietary file formats, HL-7 messages)
Health level 7, HL-7, is a standard
interface format for healthcare
messages; and, is called level 7
because its message format is
layered on the seventh level of the Open Systems Interconnection (OSI) protocol
of the International Standards Organization (ISO).12
Level 4: Machine-interpretable data - Transmission of structured messages consisting of
standardized and coded data; idealized state in which all systems exchange information
using the same formats and vocabularies, i.e. automated exchange of coded results from
8
an external lab into a provider’s electronic medical record (EMR), automated exchange of
a patient’s problems.
Data Collection Challenges
Because data collection is primarily conducted by manual chart review, data acquisition
presents challenges on several levels:
Time consumption of scarce staff resources,
Variations in data collection, data quality, and
Reporting requirements.
Time consumption of scarce staff resources: Staff abstracting data may require special
knowledge and experience in this area. Accuracy and completeness is medically crucial. The
Society of Thoracic Surgeons (STS) National Database, as an example, requires surgical care
nurse reviewers for the American college of Surgeons’ NSQIP activities.13 This is time
consuming, labor intensive and stressful. Staff members typically add these responsibilities to
other duties, such as patient care, coding, and management responsibilities. Quality and safety
may be jeopardized if the execution of collecting data is neither reliable nor timely.
Data Collection Variations: There are multiple avenues for data collection and reporting,
publicly and privately. Individual health care facilities, regional, state and national organizations
use different nomenclature and data elements, causing extreme difficulties in transmitting and
viewing reliable data. Criterion for including a patient in a registry is defined differently across
Registry organizations. For example, in a cancer registry, the stage of the neoplasm must be

9
recorded accurately for statistical information on survival rates by stage as are commonly
reported.14 A bone marrow registry must record HLA tissue typing. Strategies differ, as do
forms, and most importantly, health information systems, bringing us to data quality.
Data Quality: Factors that determine data quality include completeness, timeliness, validity,
and reliability. Conversely, contrasting electronic systems within the same organization,
breakdown in coding and performance measurement requirements, reliance on manual data
abstraction, and inconsistent policies and procedures for using secondary data as a data source
jeopardize data quality.
Data Security: The discussion of data quality requires consideration of data security. Here are
some Registries’ privacy and security concerns around knowing what to report and what not
to15:
• Provider rights to privacy - The concern over where a person’s medical records may end up or
who they may end up with is especially threatening when comparing the paper health record to
the electronic health record.
• Non-identifiable patient data for performance measurement activities – For clinicians,
unspecific health data does not allow the recording of specific patient’s experience, treatment,
visits and follow-up.
• People who try to do the right thing may be legally challenged.
• Performance measurement systems minimize why the data is needed and why certain efforts
are occurring.
• There is fear that data collected may be used or released for unintended purposes.

10
Defining and Improving Medical Registries
As previously discussed, registries can be built for any disease or condition. Within each registry
can be multiple ways to collect data, from: primary sources, networks of hospitals, clinics,
laboratories, health departments, and state/regional, and national, public and private agencies.
The goal of registries is providing accurate, timely data that adds to the exploration and
discovery of better health care management. Therefore, we must account for misinterpreted
health data, missing data, lack of interoperable standards, regulatory and legal concerns, and
timeliness. These are familiar issues for medical informatics, of which registries are a part.
Suggestions for Improvement
1. Engage in open clinical data interchange for creating terminology standards -
a. Identify needs and wants
b. Conceptualize, discuss, and implement
c. Continue to reassess results of implementation
Standardization of terminology will help physicians, coders, and many others
who enter and extrapolate data.
2. Stay abreast of technological changes in software and PC peripherals -
Software is always changing and there are many different vendors providing
interoperable options. Keep abreast of what options are available and what is
coming down the pike and discuss with similar organizations. Peripherals, such as
PDAs, will continue to improve and consequently be more accepted by users.

11
3. Be aware of regulatory and legal issues regionally and nationally -
Regulatory and legal issues will continue to evolve around standards and
infrastructure.
Responsibility and accountability for accurate population-based data throughout the country is
necessary for improving diagnosis and treatment and improving patient care. Timely, accurate
and reliable data collection can have a positive effect to the multitude of registries, and
consequently patient care. Over time clinicians and patients will feel more at ease in
disseminating personal health information, making registries reliable and timely resources for
aggregated data and public health information.

12
Bibliography
1. FAQ on Public Health, http://ncvhs.hhs.gov/9701138b.htm
2. Health Information management: Concepts, Principles, and Practice, Third Edition, Kathleen M. LaTour, Shirley Eichenwald Maki, pg 333
3. FAQ on Public Health, http://ncvhs.hhs.gov/9701138b.htm
4. http://www.immregistries.org/about/index.phtml
5. http://www.facs.org/trauma/ntdb/nsp.html
6. Health Information Management: Concepts, Principles, and Practice, Third Edition, Kathleen M. LaTour, Shirley Eichenwald Maki, pg. 332
7. LaTour, ibid, pg 331
8. http://www.cdc.gov/cancer/npcr/informatics/merp2/master.htm
9. Biomedical Informatics: Computer Applications in Health Care and Biomedicine, Shortliffe, Edward H (Editor), and Cimino, James J (Editor), 2006, 3rd Ed., pg 464
10. Connecting for Health. “Background Issues on Data Quality.” April 2006. Available online at www.connectingforhealth.org/commonframework/docs/T5_Background_Issues_ Data.pdf
11. Walker J, Pan E, Johnston D, Adler-Milstein J, Bates DW, Middleton B. The Value of Health Care Information Exchange and Interoperability [Web exclusive]. Accessed at http://content.healthaffairs.org/cgi/content/full/hlthaff.w5.10/DC1 on 11 October 2005
12. http://www.otechimg.com/pdf/hl7messaging_ch1.pdf
13. AHRQ Conference on Health Care Data Collection and Reporting, Collecting and Reporting Performance Measurement: Moving Toward Alignment. Foundation of Research and Education, AHIMA; MGMA Center for Research FORE, AHIMA Report 2/27/07
14. Shortliffe, ibid, pg 343
15. AHRQ Conference on Health Care Data Collection and Reporting, Collecting and Reporting Performance Measurement: Moving Toward Alignment. Foundation of Research and Education, AHIMA; MGMA Center for Research FORE, AHIMA Report 2/27/07
![ebXML Registry Information Model ebXML Registry …€¦ · ebXML Registry Information Model Page 6 of 38 ... ebXML Registry Business Domain Model [4] ... 209 services based on this](https://img.pdfslide.net/doc/110x75/5b5da6d27f8b9aa3048b74c6/ebxml-registry-information-model-ebxml-registry-ebxml-registry-information-model.jpg)