Embed Size (px)
Citation preview
1Department of Physical Therapy, University of Pittsburgh 2UPMC Rehabilitation Services, Pittsburgh, PA 3Department of Orthopaedic Surgery, Division of Physical Therapy, Duke University School of Medicine 4Wolff Center, UPMC, Pittsburgh, PA
Aileen Chou1 PT, DPT, Tracey Euloth2 MPT, Beth Matcho2 PT, Amy Pastva3 PT, MA, PhD, Andrew Bilderback4, MS, Janet Freburger1 PT, PhD
INTRODUCTION
Rehabilitation therapists’ discharge recommendations and hospital readmissions in patients with congestive heart failure
• > 6 million American adults have CHF1• Costs > $39 billion in care per year1• Readmissions within 30 days for 1 in 4 patients2• Physical (PT) and Occupational therapists (OT)
make discharge recommendations based on5:• Physical and cognitive impairments• Capacity to perform basic activities of daily living• Environmental barriers• Caregiver support availability and competence• Patient/family preference• Fall risk
Discharge discordance (defined as discharge to a setting that is less intensive than recommended by the therapist) may be associated with poorer outcomes
1. Describe the degree of discharge discordance for patients discharged from the acute care setting with a diagnosis of CHF
2. Examine the association between discharge discordance and 30-day all-cause hospital readmission
3. Identify sociodemographic and clinical predictors of discharge discordance
• EHR data from 12 acute care hospitals during Jan 2016 – Mar 2018
• Inclusion Criteria: 18 years+, survived acute care stay, received at least one PT or OT visit during hospital stay
• Exclusion Criteria: Transferred to another hospital, died within 30 days after discharge, missing discharge destinations, missing or unclear therapist-discharge recommendations
Sample (N=25,500)• 55% female, 89% white, 79.5% were 65 years old + • Median hospital length of stay= 6.7 days • Median number of comorbidities= 7 • Moderate or greater: mobility limitations (64%) and
activities of daily living limitations (57%)
OBJECTIVES
MATERIALS & METHODS
RESULTS RESULTS RESULTS
CONCLUSIONS
REFERENCES
CONTACT
1. Virani, S. S., Alonso, A., Benjamin, E. J., Bittencourt, M. S., Callaway, C. W., Carson, A. P., ... & Djousse, L. (2020). Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation, E139-E596.
2. Suter, L. G., Li, S. X., Grady, J. N., Lin, Z., Wang, Y., Bhat, K. R., ... & Drye, E. E. (2014). National patterns of risk-standardized mortality and readmission after hospitalization for acute myocardial infarction, heart failure, and pneumonia: update on publicly reported outcomes measures based on the 2013 release. Journal of general internal medicine, 29(10), 1333-1340.
3. Shoemaker MJ, Gutowski A, Mallgren M, et al. Physical Therapist Determination of Discharge Disposition in the Acute Care Setting. Journal of Acute Care Physical Therapy. 2019;10(3):93-106.
4. Smith BA, Fields CJ, Fernandez N. Physical therapists make accurate and appropriate discharge recommendations for patients who are acutely ill. Physical therapy. 2010;90(5):693-703.
5. Jette DU, Grover L, Keck CP. A qualitative study of clinical decision making in recommending discharge placement from the acute care setting. Physical Therapy. 2003;83(3):224-236.
6. Andrews AW, Li D, Freburger JK. Association of rehabilitation intensity for stroke and risk of hospital readmission. Physical therapy. 2015;95(12):1660-1667.
7. Jette DU, Stilphen M, Ranganathan VK, Passek SD, Frost FS, Jette AM. AM-PAC “6-Clicks” functional assessment scores predict acute care hospital discharge destination. Physical therapy. 2014;94(9):1252-1261.
8. Averill RF, Goldfield N, Hughes JS, et al. All patient refined diagnosis related groups (APR-DRGs) version 20.0: methodology overview. Wallingford, CT: 3M Health Information Systems. 2003;91.
9. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Medical care. 1998:8-27.
Additional references available upon request
email: [email protected]
a Mixed-effects model with random intercept for hospital, controlling for demographics, insurance, median income, comorbidities9, length of stay, intensive care use, mortality risk8, illness severity8, AM-PAC7 mobility score only, discharge destination, total visits from PT and OTLow Mobility (AM-PAC < 16): N=11,972; High Mobility (AM-PAC > 16): N=12,205Abbreviations: OR, odds ratio; CI, confidence interval
Readmission Risk
Predictors of Discharge DiscordanceAbbreviation: Home: Home without home services, HH: Home with home health services, PAC: Post-acute care facilities, COM: Community setting, Therapist Rec: Therapist RecommendationRed shading: discharge destination discordant with recommendations (mismatched with a lower therapy intensity)Green shading: discharge destination concordant with recommendations (matched or overmatched with a higher therapy intensity
Therapist Rec Discharge Destination
Com
m Community (Comm) Post-Acute Care Facility (PAC)Home Home HH SNF IRFHH Home HH SNF IRF
PAC SNF Home HH SNF IRF
IRF Home HH SNF IRF
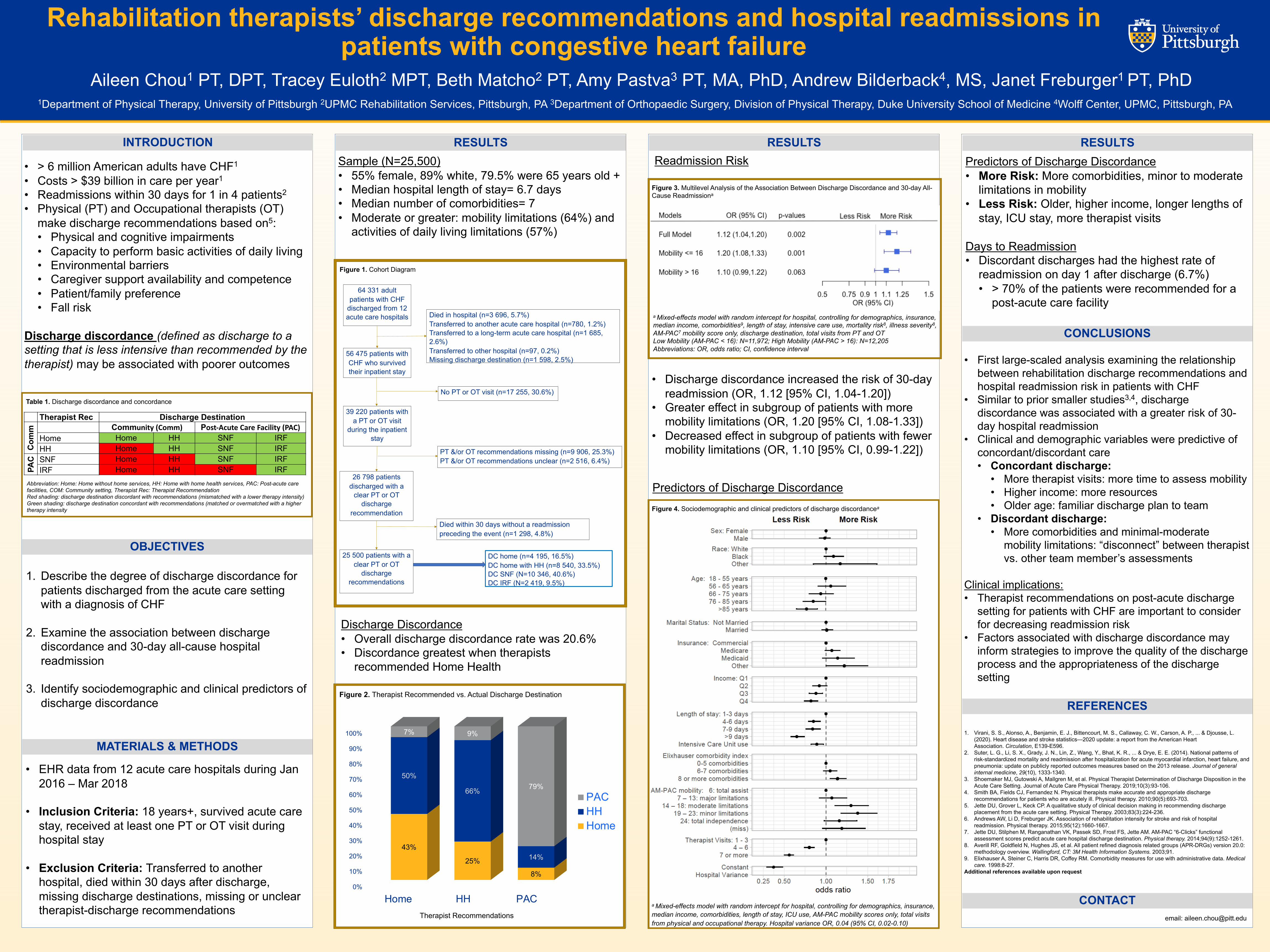
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Home HH PAC
43%
25%
8%
50%
66%
14%
7% 9%
79%
Therapist Recommendations
PACHHHome
Discharge Discordance• Overall discharge discordance rate was 20.6%• Discordance greatest when therapists
recommended Home Health
64 331 adult patients with CHF
discharged from 12 acute care hospitals Died in hospital (n=3 696, 5.7%)
Transferred to another acute care hospital (n=780, 1.2%)Transferred to a long-term acute care hospital (n=1 685, 2.6%)Transferred to other hospital (n=97, 0.2%)Missing discharge destination (n=1 598, 2.5%)
56 475 patients with CHF who survived their inpatient stay
39 220 patients with a PT or OT visit
during the inpatient stay
No PT or OT visit (n=17 255, 30.6%)
PT &/or OT recommendations missing (n=9 906, 25.3%)PT &/or OT recommendations unclear (n=2 516, 6.4%)
26 798 patients discharged with a
clear PT or OT discharge
recommendationDied within 30 days without a readmission preceding the event (n=1 298, 4.8%)
25 500 patients with a clear PT or OT
discharge recommendations
DC home (n=4 195, 16.5%)DC home with HH (n=8 540, 33.5%)DC SNF (N=10 346, 40.6%)DC IRF (N=2 419, 9.5%)
• Discharge discordance increased the risk of 30-day readmission (OR, 1.12 [95% CI, 1.04-1.20])
• Greater effect in subgroup of patients with more mobility limitations (OR, 1.20 [95% CI, 1.08-1.33])
• Decreased effect in subgroup of patients with fewer mobility limitations (OR, 1.10 [95% CI, 0.99-1.22])
a Mixed-effects model with random intercept for hospital, controlling for demographics, insurance, median income, comorbidities, length of stay, ICU use, AM-PAC mobility scores only, total visits from physical and occupational therapy. Hospital variance OR, 0.04 (95% CI, 0.02-0.10)
• First large-scaled analysis examining the relationship between rehabilitation discharge recommendations and hospital readmission risk in patients with CHF
• Similar to prior smaller studies3,4, discharge discordance was associated with a greater risk of 30-day hospital readmission
• Clinical and demographic variables were predictive of concordant/discordant care• Concordant discharge:
• More therapist visits: more time to assess mobility• Higher income: more resources• Older age: familiar discharge plan to team
• Discordant discharge:• More comorbidities and minimal-moderate
mobility limitations: “disconnect” between therapist vs. other team member’s assessments
Clinical implications: • Therapist recommendations on post-acute discharge
setting for patients with CHF are important to consider for decreasing readmission risk
• Factors associated with discharge discordance may inform strategies to improve the quality of the discharge process and the appropriateness of the discharge setting
Predictors of Discharge Discordance• More Risk: More comorbidities, minor to moderate
limitations in mobility • Less Risk: Older, higher income, longer lengths of
stay, ICU stay, more therapist visits
Days to Readmission• Discordant discharges had the highest rate of
readmission on day 1 after discharge (6.7%)• > 70% of the patients were recommended for a
post-acute care facility
Figure 1. Cohort Diagram
Figure 3. Multilevel Analysis of the Association Between Discharge Discordance and 30-day All-Cause Readmissiona
Figure 2. Therapist Recommended vs. Actual Discharge Destination
Table 1. Discharge discordance and concordance
Figure 4. Sociodemographic and clinical predictors of discharge discordancea