Embed Size (px)
Citation preview

Rehabilitative Care Alliance Provincial Stakeholder Webinar
December 11, 2015

Overview of Webinar
2
The teleconference is being recorded for posting with the slides to the RCA website.
Please enter your questions into the chat function in the webinar
We will attempt to answer as many questions as possible, time permitting
All questions entered into the chat function will be used to inform a follow up Q&A document
www.rehabcarealliance.ca

Presenters
3
Dr. Peter Nord – Co-Chair, RCA
Charissa Levy, Executive Director
Sue Balogh, Project Manager
Emmi Perkins, Project Manager
Mark Unwin, Project Coordinator
www.rehabcarealliance.ca
Meeting Objectives
Provide an Overview of the Development/Structure of the Rehabilitative Care Alliance
Provide an Overview of Mandate I Deliverables
Describe the Progress of Mandate II Initiatives
4 www.rehabcarealliance.ca

Development/Structure of the Rehabilitative Care Alliance
The Rehabilitative Care Alliance (RCA) is a provincial collaborative that was established by Ontario’s 14 LHINs in April 2013 with a two-year mandate to effect positive changes in rehabilitative care that focus on supporting
improved patient experiences and clinical outcomes and enhancing the adoption and effectiveness of clinical and
fiscal priorities.
5 www.rehabcarealliance.ca

Alignment With Other System Priorities
Identification of RCA priorities is informed by
evidence and data, as available, and by extensive
provincial stakeholder engagement and input into
the final deliverables.
The work of the RCA aligns with and builds upon
Ministry of Health and Long-Term Care priorities
and directions and other province-wide initiatives.
6 www.rehabcarealliance.ca

First Mandate Deliverables
The RCA’s first mandate was from April 2013 - March 2015
Leadership of the RCA Secretariat brought together
representatives from all LHINs, MOHLTC, HSPs from
hospital and community sectors, patients and caregivers.
Full & summary reports provide an overview of the
recommendations and tools developed for LHINs and
HSPs based on the RCA’s five priority areas of focus.
http://www.rehabcarealliance.ca/news?news_id=94
7 www.rehabcarealliance.ca

Overview of RCA Mandate I
www.rehabcarealliance.ca 8
Priority Area of Focus RCA Solution
Definitions
•Development of common terminology, clear definitions, patient characteristics and resources across all levels of rehabilitative care
•Provides clarity for patients, families and referring professionals and the structure to establish a baseline assessment of current services and inform gap analysis.
• Definitions Framework for Bedded Levels of Rehabilitative Care
• Definitions Framework for Community Based Levels of Rehabilitative Care
• Referral Decision Tree for Rehabilitative Care
Capacity Planning and System Evaluation
• Support monitoring and evaluation of rehabilitative care services, programs and system performance through development of a standard rehabilitative care capacity planning and evaluation toolkit.
• Rehabilitative Care Capacity Planning Framework
• Rehabilitative Care System Evaluation Framework

www.rehabcarealliance.ca 9
Priority Area of Focus RCA Solution
Frail Senior / Medically
Complex
Develop a rehabilitative care approach for frail senior/medically complex populations to support operationalization of priority elements of the "Assess and Restore Framework to Support Aging in Place."
• Standardized ‘Direct Admission Priority Process’ (DAPP) to Bedded Levels of Rehabilitative Care from Community/ED
• DAPP Toolkit • Assessment Urgency Algorithm as
Standardized Provincial Screening Tool • Process and Outcome Indicators • Compendium of Rehabilitative Care
Best Practices
Overview of RCA Mandate I (cont’d)

10
1Living Longer, Living well. Highlights and Key Recommendations from the Report Submitted to the Minister of Health and Long-Term Care and the Minister Responsible for Seniors on recommendations to inform a Seniors Strategy for Ontario
(December, 2012)
Assess and Restore Framework to Support Aging in Place1
www.rehabcarealliance.ca

www.rehabcarealliance.ca 11
Priority Area of Focus RCA Solution
Outpatient / Ambulatory
Inform evaluation/ planning at the provincial, regional, organizational & program levels through development of a comprehensive and standardized MDS for OP/AMB rehabilitation.
• OP/AMB Evaluative Framework • Rehabilitative Care Minimum Data
Set (MDS) • Comprehensive Review of Existing
Functional Outcome Measures • Preliminary Measure of Patient
Experience • Outpatient/Ambulatory MDS
Implementation Toolkit
Planning Considerations
for Re-Classification of CCC/Rehab Beds
Identify current issues related to the reclassification of CCC to inpatient rehabilitation beds across the province.
Comprehensive toolkit that outlines considerations in a systemic and standardized manner to support the process of completing due diligence if a potential need to re-classify beds is identified.
Overview of RCA Mandate I (cont’d)

Second Mandate Goals/Objectives
12
A briefing note describing the RCA’s first mandate deliverables and a proposed second mandate work plan was submitted to and approved/endorsed by the LHIN CEOs in February, 2015.
This approval/endorsement positions the RCA’s first mandate deliverables for full provincial implementation by LHINs by March 2017.
RCA playing a coordinating/supporting role as LHINs implement the deliverables.
www.rehabcarealliance.ca

LHIN CEOs MOHLTC
Rehabilitative Care Alliance Steering Committee
Co-Chairs – Donna Cripps and Peter Nord
ENABLERS
GTA Rehab Network Secretariat Support (Communication, Stakeholder Engagement, Coordination/Administration, Decision Support etc.)
Accountable to LHIN CEOs through
Alliance Co-Chairs
GTA Rehab Network
Secretariat
Contextual/Influencing Initiatives (Assess & Restore, Health System Funding Reform, Integrated
Funding Pilots, Coordinated Access, etc.)
QBP TJR Task & Advisory
Groups
Debra Carson Trillium Health
Partners
QBP Hip Fracture Task & Advisory
Groups
Roy Butler St. Joseph’s Health Care,
London
Outpatient / Ambulatory Task
& Advisory Groups
Marie Disotto-Monastero, Sunnybrook
Michael Gekas, Sinai Health System
Chris Sulway, TC LHIN
Definitions & CP Task & Advisory Groups
Dale Clement WW CCAC
Mark Edmonds CW LHIN
LHIN & HSP
Leads Advisory
Group
Mark Edmonds, CW LHIN & Andrea Lee,
Health Sciences North
FS/MC / A&R Task & Advisory
Groups
Dr. Jo-Anne Clarke,
North East SGS Carol Halt,
NE LHIN
Patient/Caregiver Advisory Group
Charissa Levy, RCA Executive Director
System Eval Task &
Advisory Groups
Imtiaz Daniel, OHA
Michelle Collins,
MH LHIN & Marilee Suter,
CE LHIN
Mandate II Governance

Second Mandate Goals/ Objectives
14
5 Key Priority Initiatives in Mandate II
• Definitions & Capacity Planning
• Outpatient/Ambulatory
• System Evaluation
• Assess & Restore/Frail Senior Medically Complex
• QBP – Total Joint and Hip Fracture
www.rehabcarealliance.ca

Definitions & Capacity Planning
15

RCA Definitions Framework
16
The overall intent of developing the Definitions Frameworks is to:
Establish provincial standards for levels of rehabilitative care across the continuum
Provide consistency and clarity for patients, families & referring professionals on the focus & clinical components of rehabilitative care programs
Provide a foundation to support system and local capacity planning through a common understanding of rehabilitative care services

Definition Frameworks for Rehabilitative Care Support …
services provided in the community.
www.rehabcarealliance.ca 17
A S
har
ed U
nd
erst
and
ing
o
f
Restorative potential and who is eligible for rehabilitative care
The levels of rehabilitative care (both bedded and community-based) and for each level of care, the:
• Goals of care • Characteristics of patients/clients who would be served
within each level (including estimated average length of stay and discharge indicators)
• Medical and healthcare professional resources and intensity of therapy that would be available within each level of rehabilitative care*
*As the framework is not population-specific, the specialized tertiary services provided by some Health Service Provider organizations are beyond the resource thresholds outlined within the framework.

www.rehabcarealliance.ca 18
DEFINITIONS FRAMEWORK FOR BEDDED LEVELS OF REHABILITATIVE CARE
Bedded Levels of Rehabilitative Care (i.e. Hospital-based designated inpatient rehab beds and complex continuing care beds as well as convalescent care/restorative care beds within LTCH)
Rehabilitation
(Low to high
intensity)
Activation/ Restoration
Short Term
Complex Medical
Management
Long Term Complex Medical
Management
Functional Trajectory Progression Progression Stabilization &
Progression Maintenance
Level of Care - Goal
Pa
tien
t
Ch
ara
cter
isti
cs Target Population
Functional
Characteristics
Estimated Average LOS
Discharge Indicator
Med
ica
l/A
llied
Hea
lth
Res
ou
rces
Medical Care
Nursing Care
Therapy Care
Intensity of Therapy
Reporting Tools
RCA Definitions Framework for Bedded Levels of Rehabilitative Care Available at http://rehabcarealliance.ca/definitions-1

RCA Definitions Framework for Community-Based Levels of Rehabilitative Care
(Available at http://rehabcarealliance.ca/definitions-1)
www.rehabcarealliance.ca 19

Deliverables of the Second Mandate
Definitions & Capacity Planning
1. LHIN implementation* of the RCA Definitions Frameworks for Bedded & Community-Based Levels of Rehabilitative Care including:
LHIN-level adoption of new terminology, eligibility criteria and re-categorization of rehabilitative care resources according to the levels of rehabilitative care in the Definitions Frameworks
Identification of any challenges/barriers in achieving full alignment with the Definitions Frameworks by March 2017.
Development of an implementation plan* where full re-alignment has not been achieved by the end of this mandate.
* with support as required from the RCA www.rehabcarealliance.ca 20
Deliverables of the Second Mandate
Definitions & Capacity Planning 2. LHIN application of the RCA Capacity Planning Framework. It is recognized that LHINs may have different local needs/priorities and may be at different stages of rehabilitation capacity planning. As such, LHIN application of the RCA Capacity Planning Framework is expected to vary relative to each LHIN’s readiness to undertake a capacity planning exercise. RCA project management support will be provided accordingly.
www.rehabcarealliance.ca 21
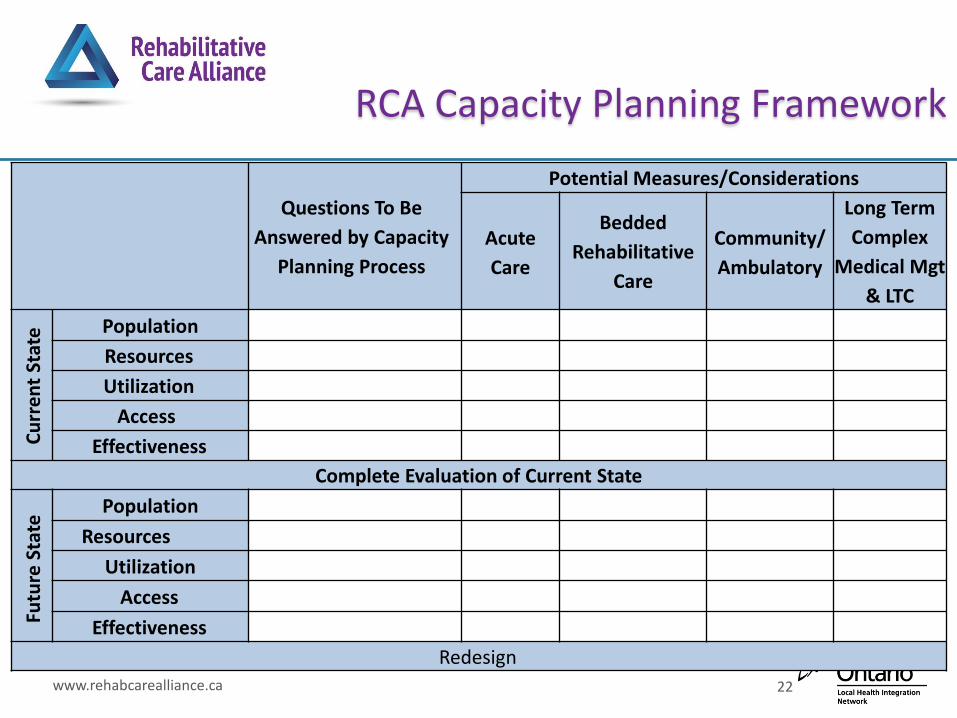
RCA Capacity Planning Framework
22 www.rehabcarealliance.ca
Questions To Be
Answered by Capacity
Planning Process
Potential Measures/Considerations
Acute
Care
Bedded
Rehabilitative
Care
Community/
Ambulatory
Long Term
Complex
Medical Mgt
& LTC
Cu
rre
nt
Stat
e Population
Resources
Utilization
Access
Effectiveness
Complete Evaluation of Current State
Futu
re S
tate
Population
Resources
Utilization
Access
Effectiveness
Redesign

Work to date
Definitions & Capacity Planning
Currently supporting LHINs as they work with health service providers to map existing community and bedded rehabilitative care programs relative to the Definitions Frameworks. Completion of the mapping tools is due to the RCA by Dec 21, 2015.
A Definitions & Capacity Planning Communications Toolkit was developed & disseminated to support LHINs in their communications to local stakeholders throughout the implementation of the RCA Definitions Frameworks.
The Secretariat has been providing support on the mapping exercise to the LHINs and HSPs through multiple group teleconferences (10 LHINs) as well as one-on-one support to individual HSPs and consultants involved with completing the mapping survey.
www.rehabcarealliance.ca 23

Next Steps
Definitions & Capacity Planning
Provincial and LHIN-level analysis of the completed mapping
surveys to identify current state alignment with the
Definitions Frameworks for Rehabilitative Care.
Identify and use a LHIN Decision Support strategy to pull
select common data elements from the RCA’s Capacity
Planning Framework to support the LHINs’ regional
rehabilitative care capacity planning efforts. Other data
elements will be obtained from other sources including
OACCAC, MOHLTC, Access to Care.
www.rehabcarealliance.ca 24

Outpatient/Ambulatory Initiative
25

Deliverables of the Second Mandate
Outpatient/Ambulatory
Mandate II Deliverables
Provide leadership and direction to support a provincial pilot of the OP/AMB MDS and a reporting system
Report on results of provincial pilot including recommendations for a potential data collection system and high level implementation plan for provincial operationalization of the Minimum Dataset
Identify a patient classification system for the outpatient /ambulatory rehabilitative care setting.
26

Deliverables of the Second Mandate
Outpatient/Ambulatory
Mandate II Deliverables
Identify and pilot measure(s) of functional change (PROM) for the outpatient/ambulatory rehabilitative care setting
Develop and pilot measure(s) of patient experience (PREM) for the outpatient/ambulatory rehabilitative care setting
27

Work to Date
Outpatient/Ambulatory
Proof of Concept (PoC), using NACRS Clinic Lite, approved by the MOHLTC in July, 2015
In collaboration with CIHI, RCA led the development of the core data elements and rehab patient classification codes within NACRS Clinic Lite
Currently working with potential pilot sites to support participation in the provincial PoC
www.rehabcarealliance.ca 28
Work to Date
Outpatient/Ambulatory
A patient experience measure (PREM) for the OP/AMB rehabilitative care setting has been developed by Drs. J. McMurray and P. Stolee and will be piloted as part of the PoC
A measure of ‘Functional Impact’ (PROM and clinician measured) is being finalized
PoC to start in January 2016 with staggered entry as sites are ready to start
www.rehabcarealliance.ca 29

Work to Date
Outpatient/Ambulatory
The NACRS Lite data collection system will capture the ‘Access & Transition’ and ‘Financial Performance’ quadrants of the RCA MDS.
The ‘Patient Experience’ and ‘Functional Impact’ quadrants will be collected manually.
www.rehabcarealliance.ca 30

System Evaluation
31

Recent Progress
System Evaluation THINK TANK II
Subject-matter experts were invited to a ‘Think Tank’ meeting in September 2015 to develop a recommendation to the RCA System Evaluation Task Group regarding a methodology to be used to identify targets and benchmarks for indicators within the Rehabilitative Care System Evaluation Framework.
www.rehabcarealliance.ca 32

Think Tank II Recommendations to the System Evaluation Task Group
Recommendations:
1. Identify a 1-3 key indicators from within the RCA Rehabilitative Care System Evaluation framework for benchmarking that are a priority from a QI and data availability perspective
2. Identify a benchmarking methodology to be used for each priority indicator
NOTE: For all others report current performance, previous year performance, provincial median +/- average, top performers (TBD) and/or range to support regions to understand their own performance relative to peers.
3. Develop definitions for 1-3 key undefined indicators from within the RCA Rehabilitative Care System Evaluation framework
4. Develop reporting template and collect data
5. Report data to stakeholders (Fall 2016) www.rehabcarealliance.ca 33
Recent Progress
System Evaluation The Task Group completed an evaluation of the indicators
from within the RCA Rehabilitative Care System Evaluation Framework using the HSII Indicator Validation Tool via the ‘Expert Choice Tool’ with support CE LHIN
Weighted criteria were used: o Strategic Alignment: 40%
o Reliability: 15%
o Actionable (Attribution): 15%
o Timeliness: 15%
o Clarity/Understandability: 15%
www.rehabcarealliance.ca 34
Results of Prioritization Exercise
System Evaluation
Results of the prioritization exercise were recently shared with Task Group members. Five indicators were selected by the group for further exploration.
The RCA Patient Family Advisory Group was also consulted to inform top priority indicators from a patient/caregiver perspective.
www.rehabcarealliance.ca 35

Next Steps
System Evaluation
For short-listed priority indicators, benchmarking methodology will be established and data will be collected to support benchmark setting.
The group will complete a similar prioritization exercise to support identification of the undefined indicators from the RCA framework that should be prioritized to be defined.
www.rehabcarealliance.ca 36

Assess & Restore/Frail Senior Medically Complex
37

Assess & Restore / Frail Senior Medically Complex
Mandate II Deliverables
1. Implementation and evaluation of the standardized tools and indicators developed from the RCA’s first mandate that support the RCA’s ‘Direct Access Priority Process’ to access rehabilitative care from the community as piloted by LHINs with their A&R funding.
2. Revisions (as required) to the standardized tools and indicators developed from the RCA’s first mandate that support the RCA’s ‘Direct Access Priority Process’ to access rehabilitative care from the community as informed by the evaluations/findings from the LHIN funded A&R initiatives
38 www.rehabcarealliance.ca

Second Mandate Goals/Objectives
Assess & Restore/Frail Senior Medically Complex
39
3. Continue to Support LHINs and the MOHLTC with Assess & Restore Related Initiatives:
Work with LHIN leads and Ministry to oversee implementation and support cross-LHIN coordination of Assess and Restore project objectives and learnings.
Facilitate knowledge exchange across LHINs, e.g., facilitation of forums/webinars/teleconferences with LHINs and relevant HSPs
www.rehabcarealliance.ca

Second Mandate Goals/Objectives
Assess & Restore/Frail Senior Medically Complex Mandate II Deliverables
4. Summary analysis of the system impact of Assess and Restore funding and the RCA’s ‘Direct Access Priority Process’ (DAPP)
5. Development of an annual report describing:
Progress of coordinated LHIN efforts to implement the Assess and Restore Guideline
On-going evaluation of LHIN A&R funded initiatives and the RCA’s ‘Direct Access Priority Process’
Completed knowledge exchange events in support of A&R funded initiatives
Summary and analysis of progress across system and project indicators and lessons learned/successes across LHINs
40 www.rehabcarealliance.ca

Additional Task Group Directions
Assess & Restore/Frail Senior Medically Complex
Promotion/education of a ‘Cross Continuum A&R Pathway’ that clarifies the 5 Essential Elements of A&R, the existing tools to support each element and alignment of these elements and tools with other system initiatives.
www.rehabcarealliance.ca 41

Provincial Webinar(s) Frailty e-modules – “5 Essential Elements of Assess and Restore”
Assess & Restore 5 Essential Elements Pathway (DRAFT)
www.rehabcarealliance.ca 42
1. Screening
• Clinical Judgment
• AUA • AUA Provincial
Implementation Toolkit (WWLHIN)
2. Assessment
• RCA Compendium
• RGP Definition of a CGA
• RGP CGA Core Elements & Competencies (CE/NE LHINs)
• QoL Measure(s)
3. Navigation & Placement
To Bedded & Community Levels of Rehabilitative Care
5. Transition To Home/
Community-Based Program(s)
4. Intervention
• RCA Compendium
• Emerging Practice
• BPGs • SFH Strategies • 2014/15 Assess
& Restore Initiatives Summary
•RCA Definitions Frameworks •RCA Referral Decision Tree •AUA Referral Pathways •RCA Rehab/A&R Definitions Cross-Walk
• RCA Definitions Frameworks
• RCA Referral Decision Tree
• HQO Adopting a Common Approach to Transitional Care Planning
• RCA Transition Checklist
Esse
nti
al E
lem
ents
o
f A
sses
s &
Res
tore
To
ols
an
d B
est/
Emer
gin
g P
ract
ices
Pro
mo
tio
nal
O
pp
ort
un
itie
s

Additional Task Group Directions
Assess & Restore/Frail Senior Medically Complex
Identify the elements of and develop a tool to support “successful transitions” within the rehabilitative care system, as informed by: o Adopting a Common Approach to Transitional Care Planning
(HQO)
o RCA Hip Fracture QBP Transition Checklist
o Research literature & other information as available that describes the unique transitional care needs of frail seniors
www.rehabcarealliance.ca 43

Identification and Evaluation of
Existing Quality of Life Measure(s)
www.rehabcarealliance.ca 44

MOHLTC Evaluation of Assess & Restore Funded Initiatives
www.rehabcarealliance.ca 45
1. Ministry Mandatory Indicators
a) Mandatory System Indicator(s)
% of unplanned readmission to hospital within 30 days of discharge from hospital
% of unplanned, less-urgent ED visit within 30 days of discharge from hospital
% of primary care follow-up visit within 7 days of discharge from hospital
% of LTC placements where home care client could have stayed home/elsewhere in the
community
Annual ALC rate by: post-acute inpatient rehabilitative care services
discharge destination from acute care
a) Mandatory Output Indicator(s)
Number of incremental attendances/visits provided as a result of this funding, & Quality of Life (QoL) measure pre-post intervention
Number of frail seniors served as a result of this funding, & Quality of Life (QoL) measure pre-post intervention
Number of clinicians trained during this funding period

Quality Based Procedures Total Joint Replacement and Hip
Fracture
46

Quality-Based Procedure Initiatives
Health Quality Ontario has developed Clinical Handbooks for a number of conditions “to serve as a compendium of the evidence-based rationale and clinical consensus driving the development of the policy framework and implementation approach for patients with specific conditions seen in hospitals1.”
While the TJR and Hip Fracture handbooks may include recommendations for rehabilitation, the extent to which these handbooks provide detailed information on rehabilitative care best practices post surgery is limited and requires further development.
47 www.rehabcarealliance.ca
1Health Quality Ontario; Ministry of Health and Long-Term Care. Quality-based procedures: Clinical handbook for primary hip and knee replacement. Toronto: Health Quality Ontario; 2014 February. 95 p.
Hip Fracture & TJR QBP
Quality-Based Procedure Initiatives Mandate II Deliverables
1. Standardized rehabilitative care best practices for Hip Fracture & TJR
2. Standardized rehabilitative models of care (including identification of optimal locations, transitions and processes of care) across bedded and community-based levels of rehabilitative care for the Hip Fracture population
3. Identification of recommendations regarding indicators to support performance monitoring of QBP-related outcomes and system performance for inclusion in the RCA Rehabilitative Care System Evaluative Framework
48 www.rehabcarealliance.ca

Determining Appropriate Rehabilitative Care Destination
49 www.rehabcarealliance.ca
During the RCA’s first mandate, the “Definitions” working group developed the “RCA Decision Referral Tree” to help guide decisions on the most appropriate location for rehabilitative care for all patient populations.
The TJR and Hip Fracture Task Groups endorsed using the RCA’s Decision Referral Tree for hip fracture patients as a starting point for a model of care (second deliverable) while supporting alignment with provincial direction for rehabilitative care.
http://rehabcarealliance.ca/uploads/File/Toolbox/Definitions/Referral_Decision_Tree_for_Rehabilitative_Care_FINAL__Dec_11_2014_.pdf
Hip Fracture & TJR QBP
Best Practice Framework
50 www.rehabcarealliance.ca
To support the first deliverable, a ‘Rehabilitative Care Best Practices Framework’ framework has been created.
The framework is based on existing pathways that identify best practice recommendations specific to the rehabilitative care location (Bedded Levels of Rehabilitation, Community-Based Rehabilitation, In-Home Rehabilitation, Long-Term Care).
The processes of care categories are based on the categories identified in the existing pathways.

Rehab Best Practice Framework for Hip Fracture Patients
www.rehabcarealliance.ca 51

Rehab Best Practice Framework for TJR Patients
52 www.rehabcarealliance.ca
Rehabilitative Care Best Practices for Primary Hip and Knee Replacement Patients
Processes of Care Pre-Operative Care Bedded Levels of
Rehabilitative Care
Community-Based
Rehabilitative Care
In-home
Rehabilitative Care
Screening
Assessments
Treatment/Interventions
• Individual & Group
Exercise Interventions
• Functional Training (e.g.
ADLs & Mobility)
Client & Family Education
Pain
Transition Care Planning
Clinical Outcome Measures

Hip Fracture & TJR QBP
Next Steps
53 www.rehabcarealliance.ca
Nov –Dec: Identify standardized rehabilitative care best practices for Hip Fracture Patients across community levels of rehabilitative care.
Jan – Feb: Identify standardized rehabilitative care best practices for Hip Fracture Patients across in-Home Rehabilitative Care.
March: Identify standardized rehabilitative care best practices for Hip Fracture Patients across Long-Term Care. For TJR - Identification of process indicators to support performance monitoring of recommended QBP-related process/practices for TJR populations

Questions?
54
Please enter your questions into the chat function in the webinar
We will attempt to answer as many questions as possible, time permitting
All questions entered into the chat function will be used to inform a follow up Q&A document
Still have questions? Get in touch with us: [email protected]
www.rehabcarealliance.ca

Help Us Keep You Informed
55
Consider signing up to receive our quarterly newsletter and other news from the Alliance, to keep updated on:
Announcements of new resources and tools supporting best practice in rehabilitative care
Opportunities to engage in and contribute to RCA projects and initiatives
www.rehabcarealliance.ca
To sign up, visit http://rehabcarealliance.ca/subscribe You can choose to unsubscribe at any time.

Thank you
56





























