Embed Size (px)
DESCRIPTION
Broad Evaluation Questions Are the units adhering to the guidelines and adopting the model? Are the units clinically effective?
Citation preview

Reinvention of the CADE units: An individual approach to the care of people
with dementia
Annaliese Blair Katrina Anderson
Michael Bird
Sarah MacPherson
Funded by NSW Ministry of Health MHDAO Older Persons Mental Health Policy Unit

T-BASIS model
Medical Director - Part-time geriatrician or psychogeriatrician Integrated outreach/inpatient service – ensuring:
most cases treated in situ, and capacity building takes place most admissions are appropriate and planned follow-up after patients’ discharge
Weekly multi-disciplinary case reviews All staff involved in developing and implementing care plans 24 hour nurse and medical coverage Main population at least moderate BPSD Median length of stay 8 -12 weeks Regular staff training.

Broad Evaluation Questions
Are the units adhering to the guidelines and adopting the model?
Are the units clinically effective?

Number of patients with primary diagnosis (N=118)
Alzheimer’s disease 35 Vascular dementia 18 LBD 6 Alcohol Related Dementia 6 FTD 4 Other dementia or dementia unspecified 26 Mixed Dementia 6 Parkinson’s Dementia 4 Affective disorder 5 Psychotic disorder 3 Delirium 3 Other 1 Missing 1 % with medical co-morbidities 94.72% % with psychiatric co-morbidities 55.79% % with moderate to severe dementia (CDR) 71.96%

Behaviour No. of patients admitted for behaviour Physical aggression 19 Verbal aggression 11 Wandering 10 Sexual disinhibition/ inappropriate 9 Intrusiveness 8 Agitation 8 Absconding 7 Hallucinations 6 Poor medication compliance 6 Delusions 5 Tearfulness 5 Self-Neglect/Living in Squalor 5 Respite 5 Repetitive behaviours 4 Resistive to care 4 Alcohol withdrawal 4 Pacing 3 Awaiting placement 3 Calling out 2 Behavioural assessment 2 Medical review 2 Delirium 2 Confusion 1

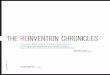
Mean number of behaviour incidents in first two weeks after admission
0
5
10
15
20
25
30
Unit 1(n=12)
Unit 2(n=15)
Unit 3(n=15)
Unit 4(n=14)
Unit 5(n=11)

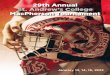
How behaviours were responded to (%)
Figure 1. Psychosocial Figure 2. PRN medication
0
10
20
30
40
50
60
70
80
90
100
Unit 1 (n=12) Unit 2 (n=15) Unit 3 (n=15) Unit 4 (n=14) Unit 5 (n-11)
AdmissionDischarge
0
10
20
30
40
50
60
70
80
90
100
Unit 1 (n=12) Unit 2 (n=15) Unit 3 (n=15) Unit 4 (n=14) Unit 5 (n-11)

‘What would you have done if there wasn’t a T-BASIS unit?’
Number and Percentage
(n=27)
Used sedation 11 (40.70%)
Asked the GP to review medications 5 (18.50%)
Referred to the Psychogeriatric Unit 5 (18.50%)
Taken them to the Emergency Department 2 (7.40%)
Involved the Mental Health Team 2 (7.40%)
Increased staffing levels 2 (7.40%)

Case example
Admitted to hospital after a fall at home – she was not given any pain relief
Multiple physical co-morbidities Continuously wandered into other patients’ rooms
and got into bed with them and frequently had to be removed by security staff
She was given Valium and Haloperidol, restrained using manacles, and specialled for 7 consecutive days.

Case example (cont.)
No incidents of aggression or inappropriate behaviour in the first 48 hours and few thereafter
The design of the T-BASIS units means that doors can be locked but the main ‘treatment’ was redirection by staff
Haloperidol, Temazepam and Valium was ceased She was given substantial pain relief Remained on Risperidone Discharged to residential care after 12 weeks.

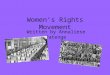
Average number of behavioural incidents per patient at admission and discharge by unit
0
5
10
15
20
25
30
Unit 1 (n=12) Unit 2 (n=15) Unit 3 (n=15) Unit 4 (n=14) Unit 5 (n=11)
Admission
Discharge

Reason for discharge (%)
Discharge reason 1
(n=30) 2
(n=21) 3
(n=25) 4
(n=22) 5
(n=20) Behaviour settled 76.7 61.9 52.0 59.0 75.0 Acute physical illness 0.0 9.5 0.0 4.5 0.0 Moved due to increase in behaviours 0.0 4.8 0.0 0.0 0.0 Physical deterioration 13.3 4.8 12.0 0.0 0.0 Died 0.0 4.7 4.0 4.5 0.0 Still in unit 0.0 9.5 20.0 31.8 15.0 Other 3.3 0.0 0.0 0.0 0.0 Missing data 6.7 4.8 12.0 0.0 10.0 Readmissions 2 3 1 2 2

Where did they go?
Discharge to Percentage of patients (N=103)
Residential care 73.79% Home 3.88% Still in unit 8.74% Other in-patient facility 3.88% Mental Health Ward 0.97% Missing 0.97%

Feedback
Families– I’ve got my mum back. I’m so grateful to them for getting mum
better; it was a God-send– … the staff took mum's behaviours in their stride and worked
with her in a really caring and sensitive way– The social worker was astronomical: she was so attentive to him
[the patient] and she conversed with him as well as with me. Residential Facilities
– RACF staff were asked to rate their satisfaction with the service on a scale of 1 = extremely dissatisfied to 5= extremely satisfied.
– M Score = 3.86 (SD = 0.90).

Acknowledgements
The Nursing Unit Managers and staff who welcomed us so warmly and who also welcomed the fact that there was going to be an evaluation so they could assess their progress.
The families of patients in the T-BASIS units who gave us permission to look at the medical files, and some of whom allowed us to interview them about quality of care.
Richard Fleming and John Bowles, whose commitment to improving the care of people with dementia and challenging behaviour in health services led to the development of the original CADE units.
The NSW Ministry of Health which funded the evaluation and is committed to further improvement of the model and the care of older people with dementia