Embed Size (px)
Citation preview

Relationship Between the Inflammation and Coagulation Pathways in Patients withSevere SepsisImplications for Therapy with Activated Protein C
Peter E. Morris, R. Duncan Hite and Christopher OhlDivisions of Pulmonary and Critical Care Medicine and Infectious Diseases, Wake Forest University School of Medicine,Winston Salem, North Carolina, USA
Contents Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4031. Microvascular Thrombus Formation in Patients with Severe Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 405
1.1 The Coagulation Cascade: Clot Formation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4051.2 Inhibitors of the Coagulation Pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 405
1.2.1 Antithrombin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4051.2.2 Tissue Factor Pathway Inhibitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4051.2.3 Activated Protein C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4051.2.4 Fibrinolytic Pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 407
1.3 Pro- and Anti-Inflammatory Characteristics of the Coagulation Pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4071.3.1 Pro-Inflammatory Effects of Fibrin and Fibrin-Degradation Products . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4071.3.2 Direct Pro-Inflammatory Effects of Thrombin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4081.3.3 In Vitro and In Vivo Anti-Inflammatory Properties Attributed to Activated Protein C . . . . . . . . . . . . . . . . . . . 408
2. Evidence Linking a Low Protein C Level with Poor Outcome in Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4082.1 Protein C Specifically Reduced in Severe Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4092.2 Acquired Protein C Deficiency Precedes Clinical Symptoms of Severe Sepsis/Septic Shock . . . . . . . . . . . . . . . . . 4102.3 Protein C Levels Correlate with the Outcome of Patients with Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4102.4 Acquired Protein C Deficiency in Sepsis Occurs with a Wide Range of Infectious Micro-Organisms . . . . . . . . . . . . . . 410
2.4.1 Gram-Negative Infection-Induced Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4102.4.2 Gram-Positive Infection-Induced Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4112.4.3 Parasitic Infection-Induced Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 411
2.5 Protein C as a Prognostic Marker for Related Diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4113. Use of Recombinant Activated Protein C in Humans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 412
3.1 Administration of Protein C and Activated Protein C in Severe Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4123.2 Phase II Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4123.3 Protein C Pharmacokinetics and Pharmacodynamics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4123.4 Phase III Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4123.5 Serious Adverse Events during the PROWESS Study and Implications for Future Administration . . . . . . . . . . . . . . . . . 414
4. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 414
Abstract In patients with severe sepsis, thrombin has been implicated in the interrelationship between the coagulationand inflammation pathways. Thrombin is responsible for conversion of fibrinogen to fibrin (thrombus forma-tion). Thrombin also activates endothelial cells, white blood cells and platelets. Regulation of both the coagu-lation and inflammation pathways is in part through the interaction of thrombin and activated protein C.Activated protein C has particular attributes that may inhibit microvascular thrombi, promote fibrinolysis anddirectly dampen the pro-inflammatory aspect of infection. In patients with severe sepsis, many investigatorshave demonstrated an active coagulopathic state, with low protein C levels. A phase III clinical trial has nowdemonstrated reduced mortality in patients with severe sepsis receiving activated protein C.
DRUG MECHANISMS AND TARGETS Biodrugs 2002; 16 (6): 403-4171173-8804/02/0006-0403/$25.00/0
© Adis International Limited. All rights reserved.

In the practice of medicine, successful outcomes followingtreatment with antibiotics have become routine when an infectionis limited in severity. On the other hand, patients’ lives are per-sistently placed at risk when an acute infection advances to organdysfunction. Mortality for patients with severe sepsis ranges from30 to 50%. Over the last two decades, many experimental thera-pies have been studied with the hope that an additional decreasein mortality would be achieved for patients with severe sepsis.Unfortunately, despite many efforts during this period, no com-pound was found to reduce mortality in severe sepsis. A recentlycompleted phase III study with activated protein C was able toshow a decrease in the severe sepsis mortality rate.[1] Activatedprotein C, a component of the natural anticoagulant system, is apotent antithrombotic serine protease with suspected indirect anddirect anti-inflammatory properties.
Previous clinical trials in patients with severe sepsis evaluatedpharmacological agents designed to attenuate the pro-inflammatoryevents in sepsis. These included glucocorticoids and drugs designedto neutralise endotoxin, tumour necrosis factor (TNF) or interleu-kin (IL)-1, or other agents intended to dampen the inflammatorycascade. Reasons cited in the medical literature for lack of mor-tality reduction in previous sepsis trials include: the inability of themolecule to achieve its theoretical mechanism (e.g. antiendotoxinclearing endotoxin); the inability to administer the study drug atthe appropriate time in relation to the onset of inflammation [i.e.failing to achieve the equivalent of an ‘off’ switch for inflamma-tion (e.g. IL-1–receptor antagonist)]; and study design flaws thatincluded inaccurate power analysis and loose exclusion criteria(e.g. the inclusion of underlying disease states resulting in a sub-population of patients with significant nonsepsis mortality).[2,3]
What was perhaps not widely recognised until more recently wasthe prominence of an activated coagulation pathway that is tem-porally related to the onset of organ dysfunction in patients withsevere sepsis. Since the mid 1990s, when an activated coagulationsystem in patients with severe sepsis was recognised on a largescale, the coagulation cascade has emerged as a therapeutic targetin severe sepsis.
In 1992, the results of the sepsis definitions consensus confer-ence of the American College of Chest Physicians (ACCP) andthe Society of Critical Care Medicine (SCCM) were published.[4]
The definitions that were agreed were an attempt to categorisesepsis along a continuum of disease severity. The ACCP/SCCMConsensus Conference defined sepsis as a systemic inflammatoryresponse to infection associated with more than one disturbancein homeostasis manifest as abnormal body temperature, elevatedheart rate, tachypnoea or hyperventilation, and altered whiteblood cell count (table I). These clinical manifestations were re-quired to be part of a systemic response to an infectious process, in
the absence of other known causes for such abnormalities. Severesepsis was defined as sepsis associated with acute organ dysfunc-tion, hypoperfusion or hypotension. Septic shock was defined assevere sepsis and sepsis-induced hypotension persisting despiteadequate fluid resuscitation. A patient could be considered to bein septic shock without hypotension if maintenance of blood pres-sure required inotropic support.
This review discusses the coagulation cascade and the natu-rally occurring anticoagulant factors. The pro- and anti-inflam-matory properties of the coagulation cascade are reviewed. Inaddition, the coagulopathy seen in severe sepsis is described, asis the history of protein C and activated protein C administration tohumans with infection. We explain the theory behind why ananticoagulant protein may be appropriate in severe sepsis. Theresults of a phase III trial have led to approval from the US Foodand Drug Administration (FDA) for administration of activatedprotein C to a highly defined group of patients with severe sepsis.Interpretation of the phase III data and the guidelines set by theFDA are explained.
Table I. American College of Chest Physicians (ACCP) and the Society ofCritical Care Medicine (SCCM) Consensus Conference definitions[4]
Condition Definition
Systemic inflammatoryresponse syndrome
Systemic inflammatory response to a variety ofclinical insults manifested by 2 or more of thefollowing:
(i) temperature >38°C or <36°C (>100.4°F or<96.8°F)
(ii) elevated heart rate (>90 beats/min)
(iii) tachypnoea (>20 breaths/min) orhyperventilation (PaCO2 <32mm Hg)
(iv) WBC count >12 000 cells/mm3 or <4000cells/mm3 or >10% immature neutrophils
Sepsis Systemic response to infection associated with2 or more of the following:
(i) temperature >38°C or <36°C (>100.4°F or<96.8°F)
(ii) elevated heart rate (>90 beats/min)
(iii) tachypnoea (>20 breaths/min) orhyperventilation (PaCO2 <32mm Hg)
(iv) WBC count >12 000 cells/mm3 or <4000cells/mm3 or >10% immature neutrophils
Severe sepsis Sepsis associated with 1 of the following:
(i) acute organ dysfunction
(ii) hypoperfusion (e.g. lactic acidosis, oliguria)
(iii) sepsis-induced hypotension
Septic shock Sepsis-induced hypotension persisting despitefluid resuscitationa
a Patients receiving inotropics or vasopressors may not be hypotensivewhen hypoperfusion is measured.
PaCO2 = partial pressure of carbon dioxide in arterial blood; WBC = whiteblood cell.
404 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

1. Microvascular Thrombus Formation in Patientswith Severe Sepsis
1.1 The Coagulation Cascade: Clot Formation
The extrinsic pathway of coagulation is initiated when bloodis exposed to tissue factor in the subendothelial space or whentissue factor is expressed on monocytes in the circulation. Tissuefactor is a membrane-bound glycoprotein and has been referredto as thromboplastin. Tissue factor activates factor VII (figure 1).The resulting VIIa/tissue factor complex then activates factor Xof the common pathway and factor IX of the intrinsic pathway.Factor IX, activated by the tissue factor pathway, in turn activatesadditional factor X, in a reaction that is greatly accelerated by acofactor, factor VIII. Thrombin circulates in the inactive form ofprothrombin. It is activated factor X that converts prothrombinto thrombin (factor IIa) and factor Va accelerates this reaction.Thrombin, once generated, operates in a feedback loop and acti-vates factors VIII and XI. In the final step of the process, throm-bin cleaves fibrinogen to generate fibrin monomers. These fibrinmonomers become the clot by becoming cross-linked by factorXIIIa.[5,6] Thrombin may then bind to either fibrin, where it mayremain active, or thrombomodulin, a receptor on endothelial cells.
It is suspected that in patients with severe sepsis, tissue factorbecomes expressed on monocytes and macrophages, because ofthe pro-inflammatory cytokine generation following an endo-toxaemic event.[5] Tissue factor may also become exposed to theblood from subendothelial sources. It is currently unclear whichof these two sources of tissue factor is the more prevalent expres-sion in patients with severe sepsis.
1.2 Inhibitors of the Coagulation Pathway
1.2.1 AntithrombinAntithrombin is a plasma protein that inhibits the serine pro-
teases of the intrinsic and common coagulation pathways. Therate at which antithrombin inactivates thrombin is increased by afactor of several thousand in the presence of endogenous heparansulfate. Antithrombin is the principal inhibitor of thrombin (fac-tor IIa) [figure 2]. Antithrombin levels in patients with severesepsis become low because of the continuous consumption by theongoing formation of thrombin and other activated proteases thatare susceptible to antithrombin deactivation. Antithrombin is de-graded by elastase, which is released from activated neutrophils.Also, production of antithrombin by the liver is impaired in pa-tients with sepsis, and antithrombin levels in the circulating bloodare lowered as a result of capillary leakage of proteins throughdamaged endothelial structures. Antithrombin has been reportedto be as low as 30% of normal levels in patients with severe
sepsis.[7,8] In a recently completed phase III study of antithrombinadministration in 2314 patients with sepsis, baseline antithrom-bin III levels were below 60% of normal functional levels in morethan 50% of randomised patients.[9]
1.2.2 Tissue Factor Pathway InhibitorThe tissue factor pathway inhibitor (TFPI) is a lipoprotein-
associated plasma protein that binds to tissue factor and activatedfactors VII and X (figure 2). The resultant complex inhibits theextrinsic coagulation pathway. Once factor VIIa activates a smallamount of factor X, the ‘tissue factor/factor VIIa/factor Xa’ com-plexes are rapidly neutralised by the TFPI. Most TFPI is boundto the vessel wall, and only 10 to 25% is found in the circulatingblood.[10]
1.2.3 Activated Protein CProtein C is a plasma serine protease, although it is not inhib-
ited by antithrombin. In the presence of thrombomodulin boundto endothelial cells, thrombin activates protein C, which in turncleaves activated factors VIII and V, leaving them inactivated(figure 2). Protein S is a cofactor that accelerates this reaction.Thrombomodulin is a proteoglycan composed of a protein coreand chondroitin sulphate moiety, which is expressed on mono-cytes and endothelial cells.[11] Protein C is activated by the throm-bin/thrombomodulin complex on the endothelial cell surface.When thrombin binds to thrombomodulin, it undergoes a confor-mational change at its active site that converts it from a procoag-ulant enzyme to a potent activator of protein C. When thrombinbinds to the endothelial cell surface via thrombomodulin, thebinding of thrombin to thrombomodulin increases the conversionof protein C to activated protein C. Activated protein C inhibits
Intrinsic pathway Extrinsic pathway
Commonpathway
XII/XIIa
XI/XIa
Surfacecontact
IX IXa
VIIIa
Injury
Tissuefactor
VIIa
X
XaVa
Prothrombin (II) Thrombin (IIa)
Fibrinogen Fibrin
Fig. 1. The coagulation cascade. a = activated form; II to XII = clotting factors.
Activated Protein C in Severe Sepsis 405
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

the ability of thrombin to further activate factor XIII, endothelialcells and platelets, and ultimately to convert fibrinogen to fibrin.
Therefore, thrombomodulin acts as a molecular switch convert-ing thrombin from a procoagulant to an activator of the anticoag-ulant protein C pathway (figure 3).[12,13] The glycosaminoglycanchondroitin sulfate is an integral component of thrombomodulinon the endothelial cell surface and vital for thrombin-dependentprotein C activation.[14,15]
There is growing evidence to suspect that thrombomodulin isimpaired on endothelial cell membranes in severe sepsis, and thatthis impairment, together with reduced protein C, may cause re-duced generation of functional activated protein C. It has beendemonstrated in vitro that soluble thrombomodulin may be re-leased as a result of endothelial cell damage.[17] In experimentalmodels, thrombomodulin expression is down-regulated in thepresence of pro-inflammatory stimuli, including endotoxin andcytokines.[18,19] In experimental models of sepsis, thrombomo-dulin messenger RNA has been shown to be up-regulated.[20,21]
Monocyte thrombomodulin may be important in the activation ofprotein C in vivo, although there are no data available to supportthis notion in humans with severe sepsis.[22]
In vitro studies suggest that pro-inflammatory mediators suchas TNF may be able to down-regulate the expression of thrombo-modulin, which would result in less activation of protein C bysparing the deactivation of thrombin.[23,24] Also, activated poly-morphonuclear leucocytes that are adhered to the surface of anendothelial cell have been suspected of being able to oxidise throm-bomodulin and cause shedding of thrombomodulin from the en-dothelial cell, reducing the potential ability to clear thrombinfrom the microcirculation.[22]
In a study that may give the most direct information in thismatter, Faust and colleagues[25] indicated that the cellular machineryneeded to convert protein C to activated protein C is down-regulatedin patients with sepsis. This reasoning suggests that activated proteinC might be the appropriate replacement therapy for the acquiredprotein C deficiency in sepsis, rather than the native (unactivated)protein C. In the study by Faust et al.,[25] the expression ofthrombomodulin and endothelial protein C receptor was deter-mined in the dermal microvasculature of children with severemeningococcaemia and purpuric or petechial lesions. Skin speci-mens were obtained by punch biopsy in 21 patients with severemeningococcal sepsis. Biopsies were taken within 24 hours of thefirst antibiotic dose.
A very important finding of this study was that comparativelyweak staining for thrombomodulin and endothelial protein C recep-tor was also observed in areas with little thrombosis. Plasma levelsof thrombomodulin antigen were significantly higher in all pa-tients with meningococcal disease on day 1 after the initiation ofantibiotic and supportive treatments than in the non-meningococcalcontrols. The investigators found a marked reduction in the expres-
FactorVa
Cellsurface
Factor XIa
Factor IXa
Factor Xa
Factor IIa Factor IIa
Fibrin
Plasmin
Antithrombin III, heparan
Tissue-factorpathway inhibitor
Tissue factor
Factor VIIa
FactorVIIIa
Thrombomodulin
Protein SProtein C
Fibrinogen
Plasminogenu-PAt-PA
Fig. 2. Coagulation is initiated by the exposure of blood to tissue factor boundto cell membranes. Tissue factor interacts with factor VIIa to convert factorIX to factor IXa and factor X to factor Xa (only the activated forms are shown).Factor IXa converts factor X to factor Xa. Factor Xa generates factor IIa(thrombin) from factor II (prothrombin). Each of these reactions takes placeon an activated cell surface. Once factor IIa is generated, it cleaves plasmafibrinogen to generate fibrin. The tissue factor pathway inhibitor forms aquaternary structure with tissue factor, factor VIIa and factor Xa. Thethrombomodulin/protein C/protein S pathway inactivates factors Va andVIIIa. Antithrombin III inactivates factors XIa, IXa, Xa, and IIa in a reactionthat is accelerated by the presence of heparan sulfate. In the fibrinolyticpathway, tissue-type plasminogen activator (t-PA) and urokinase-type plas-minogen activator (u-PA) convert plasminogen to plasmin. Once generated,plasmin proteolytically degrades fibrin (reproduced from Rosenberg andAird,[6] with permission).
406 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

sion of thrombomodulin and endothelial protein C receptor onthe endothelium of both thrombosed and nonthrombosed dermalvessels in children with early meningococcal disease. Ultrastruc-tural studies showed that this reduction could not be explainedsimply by the loss of endothelial cells.
Plasma levels of activated protein C were low or undetectablein children with meningococcal sepsis, and activated protein Clevels failed to rise after the administration of unactivated proteinC concentrate (in two patients). These findings suggest that thereduction in the endothelial expression of thrombomodulin andendothelial protein C receptor results in the impairment of proteinC activation.
Protein SThe factors Va and VIIIa are critical in the activation of
thrombin. Protein S is an essential cofactor for the action of ac-tivated protein C on Va and VIIIa. Once protein C becomes acti-vated, it binds to its cofactor protein S on the surface of activatedcells. This complex is then able to inactivate factors Va and VIIIa.The anticoagulant capacity of protein C is enhanced by the freefraction of protein S. The activation of protein C in a response tothrombin generation is itself inhibited by plasma inhibitors. Dur-ing acute inflammation and the proliferation of acute phase pro-teins, it has been suspected that specific acute phase proteins canshorten the measured half-life activity of activated protein C. α1-Antitrypsin and α2-macroglobulin are considered to be inhibitorsof activated protein C.[26]
Protein C can bind directly to C4b binding protein, which isa regulatory protein in the complement cascade. In plasma, 60%of the cofactor protein S is complexed to the complement regu-latory protein C4b binding protein. Increased plasma levels ofC4b binding protein, as a consequence of the acute phase reactionin sepsis, may result in a relative protein S deficiency contribut-ing to a further procoagulant condition.[27]
1.2.4 Fibrinolytic PathwayA series of enzymatic reactions generates plasmin, a serine
protease that acts on fibrin to dissolve preformed clots. A tryp-sin-like protease, plasmin degrades fibrin into soluble fibrin deg-radation products. Tissue-type plasminogen activator (t-PA), whichis synthesised and secreted by endothelial cells, mediates intra-vascular plasminogen activation. Plasminogen activation is tar-geted to fibrin because plasminogen and t-PA bind to fibrin and theenzymatic activity of t-PA is enhanced by fibrin (see figure 2).
The fibrinolytic system is regulated at two levels. Plasmino-gen activator inhibitors, the most important of which is endothe-lial cell–derived type 1 plasminogen activator inhibitor (PAI-1),block t-PA, whereas antiplasmin inhibits plasmin. Recently, a pro-carboxypeptidase B that serves as a link between coagulation and
fibrinolysis, was identified in plasma.[28] This carboxypeptidaseB-like enzyme, known as thrombin activatable fibrinolysis inhib-itor (TAFI), is activated by the thrombin/thrombomodulin complexand attenuates fibrinolysis by cleaving carboxyl-terminal lysineresidues from fibrin.[28] Removal of these lysine residues decreasesplasminogen and plasmin binding to fibrin, thereby retarding thelytic process.[29]
Contribution of Activated Protein C to Clot LysisIn addition to its direct effect on microvascular clot prolifer-
ation via tissue factor expression on monocytes, endotoxin alsoincreases PAI-1 levels. Activated protein C can enhance fibrino-lytic activity by binding to PAI-1,[30] thus blocking its ability tobind t-PA (figure 4). When activated, protein C is available tobind PAI-1; the process keeps t-PA free to activate plasminogento plasmin, and thus helps cleave microvascular clots.
1.3 Pro- and Anti-Inflammatory Characteristics of theCoagulation Pathway
1.3.1 Pro-Inflammatory Effects of Fibrin and Fibrin-Degradation ProductsSeveral studies suggest a direct effect of fibrin on inflamma-
tory activity. Fibrinogen interacts with bacteria and modulates
VIlla Va
IXa X XaII
IIa
EPCRPC IIa
TM
ViVa
APC
PSVIlliVIIIa
APC
PS
a
b
Fig. 3. Protein C (PC) activation and the anticoagulant action of activatedprotein C (APC). (a) The tenase complex [formed by activated factor IX (IXa),activated factor VIII (VIIIa), calcium ions and negatively charged membranephospholipids] activates factor X. Activated factor X (Xa) then forms withactivated factor V (Va), calcium ions and a negatively charged phospholipidsurface, the prothrombinase complex, which converts prothrombin (II) tothrombin (IIa). Thrombin can either promote clotting and activate cells, or itcan bind to thrombomodulin (TM), leading to PC conversion to the antico-agulant APC. PC activation by the thrombin/thrombomodulin complex isfacilitated by the transmembrane protein endothelial protein C receptor(EPCR). (b) Protein S (PS) facilitates APC binding to cell surfaces andenhances APC-mediated cleavage of coagulant factors VIIIa and Va. Theinactivated forms of these cofactors (VIIIi and Vi) are no longer capable ofsustaining thrombin generation (reproduced from Alberio et al.,[16] with per-mission).
Activated Protein C in Severe Sepsis 407
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

their activity. Fibrin serves to encapsulate bacteria and fibrin deg-radation products may trigger the release of pro-inflammatorycytokines.[31] Thus, in extravascular spaces such as the intra-peritoneal cavity or pulmonary tissue, it is suspected that fibrinis involved in the regulation of inflammatory activity and tissuedamage.[32]
1.3.2 Direct Pro-Inflammatory Effects of ThrombinThrombin has been shown to be particularly capable of aug-
menting platelet activating factor (PAF) synthesis.[33] The pres-ence of thrombin, especially in the microcirculation, is associatedwith an increase in adhesion molecule expression.[27] Thrombinacts as a chemotactic factor for neutrophils. Thrombin, therefore,may have the capacity to work directly to amplify the inflamma-tory response. Thrombin has been suspected of contributing tosome of the complications of sepsis, including the activation andadhesion of white blood cells and vascular cell dysfunction.
1.3.3 In Vitro and In Vivo Anti-Inflammatory Properties Attributedto Activated Protein CMany experiments have supported the notion that the anti-
inflammatory activity of activated protein C may be distinct fromits anticoagulant activity. In rodent models, activated protein Cwas shown to decrease TNF response to endotoxin, which minim-ised leucocyte activation and thus pulmonary injury.[33,34] In aseries of experiments that emphasised the use of an agent chosento isolate only anticoagulant effects in an inflammation model, ahighly specific agent that blocked the active site of factor Xafailed to protect the animals from the endotoxin challenge andfailed to prevent cytokine elaboration. Esmon[27] has reviewedmechanisms to account for the ability of activated protein C to
modulate the inflammatory response to endotoxin. One theory isthat a binding site on mononuclear cells appeared to be respon-sible for decreasing the calcium flux in response to endotoxin andalso for blocking TNF elaboration.[34] More recently, Murakamiand colleagues[35] have shown that activated protein C blocksnuclear factor-kappa B (NF-κB) nuclear translocation. NF-κBnuclear translocation is one of the major mechanisms involved incytokine elaboration by mononuclear cells and endothelium.Thus, it is possible that this mechanism accounts, in part, for theability of activated protein C to dampen the inflammatory cyto-kine cascades that are associated with endotoxic shock. The spe-cific monocyte receptor remains to be characterised.
Joyce et al.[36] used transcript profiling (the simultaneous mon-itoring of gene expression for a significant portion of a genome),to show that activated protein C inhibited pro-inflammatory cyto-kine signalling, including TNF induction of cell surface adhesionmolecules (vascular cell adhesion molecule [vCAM], intracellu-lar adhesion molecule [ICAM] and E selectin). Activated proteinC also modulated apoptosis pathways including up-regulation ofthe endothelial Bcl-2 homologue.[37] Activated protein C mayalso decrease the production of IL-1 and TNF from monocytesand uncouple lipopolysaccharide interaction with the CD14 re-ceptor on monocytes.[38]
Activated protein C has the potential for regulating the in-flammatory response by means of at least three mechanisms: itprevents thrombus formation and stimulates fibrinolysis, therebydiminishing ischaemic tissue damage; it blocks thrombin gener-ation, thereby preventing amplification of the inflammatory re-sponse induced by thrombin itself; and it may have a direct effecton monocytes that dampens elaboration of cytokines, such asTNFα, IL-6 and IL-8 (figure 5).[16]
2. Evidence Linking a Low Protein C Level with PoorOutcome in Sepsis
All major physiological anticoagulants, antithrombin III, pro-tein C and TFPI, appear to be affected in patients with dissemin-ated intravascular coagulation (DIC).[39] A large body of literaturegives support to the notion that severe infection is associated witha coagulopathic state. The studies are mostly descriptive of smallpopulations of patients. When these reports are considered to-gether, however, they do form a very compelling argument thatthe coagulation system becomes activated in patients with severeinfection.
Correlations between protein C levels and morbidity and mor-tality have been seen in studies of DIC in patients with sepsis.Fourrier et al.[8] linked the influence of DIC on the mortality rateand the occurrence of multiple organ failure in 60 patients with
Plasminogen
Plasmin
APC
APC
t-PA
t-PA t-PA
or
or
PAI-1 PAI-1
PAI-1
PAI-1
Fig. 4. The role of the protein C pathway in regulating fibrinolysis. Tissue-type plasminogen activator (t-PA) converts plasminogen to plasmin. t-PA israpidly inactivated by plasminogen activator inhibitor 1 (PAI-1). PAI-1 alsoforms tight complexes with activated protein C (APC). Thus, when APClevels are relatively high, they serve to decrease PAI-1, thereby preventinginhibition of t-PA and increasing fibrinolysis (reproduced from Esmon,[27] withpermission).
408 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

septic shock, 44 of whom had DIC. DIC was defined as thrombo-cytopenia (platelet count <100 × 109/L or a decrease in plateletcount of >100 × 109/L over 24 hours), decrease in prothrombinlevel or factor V (<70%), and presence of soluble complexes offibrin and fibrin degradation product. The mortality rate was sig-nificantly higher in the DIC group (77%) than the DIC-negativegroup (32%) [p = 0.001], as was the total number of acquiredorgan failures after admission (p = 0.05). All but two patients hadlow protein C levels; these levels were significantly lower innonsurvivors than survivors (27 ± 4% vs 47 ± 3%; p = 0.001).Overall, this study found that an initial protein C level <30% hada specificity of 0.86 and sensitivity of 0.60 (chi-square, 9.26; p =0.005) as a prognostic marker for sepsis.
In another study, 28 patients with sepsis were seen at the onsetof sepsis.[40] They were shown to have high levels of throm-bin/antithrombin complexes, PAI-1, neopterin and IL-6. Anti-thrombin III, factor XII and protein C were shown to be belownormal levels. Gando et al.[41] studied 35 patients with systemicinflammatory response syndrome (SIRS): 13 survivors and 22nonsurvivors. High levels of PAI-1 and low levels of protein Cand antithrombin II persisted through day 5 only in the non-survivors. In another study, Gando et al.[42] studied 40 traumapatients and grouped them by nonSIRS, SIRS <2 days and SIRS
>3 days. Tissue factor antigen concentration, prothrombin frag-ment F1+2, thrombin/antithrombin complex (TAT), fibrinopep-tide A, and cross-linked fibrin degradation products (D-dimer)were higher in patients with SIRS >3 days. In a subsequent study,the same group studied 19 patients with severe sepsis and ninetrauma patients without infection.[43] Significant correlationswere found between tissue factor antigen measurements and bothDIC score and organ dysfunction. In a separate study, tissue fac-tor antigen was shown to be higher in a group of 27 patients withacute respiratory distress syndrome (ARDS) compared with 31at-risk or 55 patients without ARDS.[44] Tissue factor levels cor-related with lung injury scores. Additionally, there have beenreports of elevations of soluble thrombomodulin during inflam-matory illness.[45,46]
Considering the sheer volume of reports, and the range ofcritical illness disease states investigated, the literature cited abovedoes support a strong association between the activation of thecoagulation system and severe infection-associated inflammation.
2.1 Protein C Specifically Reduced in Severe Sepsis
Protein C levels had been shown to be reduced in patients withsepsis as early as 1982.[47] Sheth and Carvalho[48] reported thatprotein C levels were depressed in a population of patients with
Fibrinolytic system
Inhibition of PAI
Stimulation of fibrinolysis
Reperfusion
Less ischaemic damage
Inactivation of FVa and FVIIIa
Activated protein C
Coagulation system
Decreased thrombin generation
Prevention of the amplification ofthe inflammatory response
induced by thrombin
Decreasedfibrin formation
Monocytes and endothelium
?
Decreased TNFα, IL-6 and IL-8 production
Less inflammation
Fig. 5. Anti-inflammatory action of activated protein C. Activated protein C has the potential for regulating the inflammatory response by means of at leastthree mechanisms: it prevents thrombus formation and stimulates fibrinolysis, thereby diminishing ischaemic tissue damage; it blocks thrombin generation,thereby preventing amplification of the inflammatory response induced by thrombin itself; and it has a direct effect on monocytes that dampens elaborationof cytokines, such as tumour necrosis factor (TNF)-α, interleukin (IL)-6 and IL-8. FVa = activated factor V; FVIIIa = activated factor VIII; PAI = plasminogenactivator inhibitor (reproduced from Alberio et al.,[16] with permission).
Activated Protein C in Severe Sepsis 409
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

sepsis and trauma. Hesselvik and colleagues[49] studied TAT andprotein C levels in 24 patients with severe infection and 13 pa-tients with septic shock. TAT was significantly elevated in 16 of24 patients with infection and 12 of 13 patients with shock (p =0.001 vs healthy individuals; p = 0.05 infection vs shock). Meanprotein C levels were significantly reduced in all patients (p =0.001 infection and shock vs control; p = 0.01 infection vs shock).
2.2 Acquired Protein C Deficiency Precedes ClinicalSymptoms of Severe Sepsis/Septic Shock
Mesters et al.[7] measured protein C levels in samples col-lected prospectively from a group of 97 adult patients with leu-kaemia. These patients were all at high risk for severe sepsissecondary to chemotherapy-induced neutropenia. There was adramatic drop in protein C levels at the onset of fever in patientswho subsequently developed septic shock. The striking findingof this report is that the fall in protein C occurred well in advanceof clinical signs in patients who developed shock compared withthose who subsequently developed severe sepsis without shock(median protein C levels 23.1 vs 69.5%; p = 0.0003). The medianelapsed times between detection of fever and the diagnosis ofseptic shock or severe sepsis were 12 and 16 hours, respectively.The decrease of protein C levels in the septic shock group at theonset of fever was accompanied by an increase in a marker ofthrombin generation, prothrombin fragment 1 + 2 (3.0 vs 0.95nmol/L in the severe sepsis group; p = 0.009). In contrast, neutro-penic patients who developed ‘fever only’ had protein C levelsin the normal or slightly below normal range. These data suggestthat silent consumptive coagulopathy, characterised by early de-creases in protein C, precedes the overt clinical symptoms ofsevere sepsis and septic shock. The data also support the hypoth-esis that consumption of protein C may lead to multiple organfailure and death in sepsis. The role of protein C administrationwill be an important future area of study in these very ill patients.
2.3 Protein C Levels Correlate with the Outcome ofPatients with Sepsis
Protein C levels have been shown to inversely correlate withmorbidity and mortality in patients with sepsis, regardless of age,infecting micro-organisms, presence of shock, DIC, degree ofhypercoagulation, or severity of illness. For example, Lorente etal.[50] examined the time course of haemostatic abnormalities in48 consecutive patients with septic shock and found that all pa-tients had marked abnormalities in both the coagulation and thefibrinolytic systems, including elevations in levels of D-dimerand TAT. These abnormalities were equally common in patientswith Gram-positive and Gram-negative infections. Most impor-
tantly, the investigators found that protein C levels in patientswith sepsis were significantly different from those in 30 healthyvolunteers on days 1, 4 and 7 after hospital admission and weresignificantly different between survivors and nonsurvivors (p =0.05). The protein C levels remained depressed throughout the 7days in nonsurvivors, but were higher from day 4 onwards insurvivors than in nonsurvivors (p = 0.05).
A retrospective analysis was performed on a subset of a pre-viously published, prospective, randomised, double-blind, pla-cebo-controlled trial (Effects of Ibuprofen on the Physiology andSurvival of Patients with Sepsis; ISS).[51,52] The results werebased on a subset of the total ISS population for whom additionalcoagulation assays were performed on the blood samples ob-tained at baseline and 44 hours. These assays included protein Cantigen, D-dimer and fibrinogen levels. A total of 63 of the 70patients (90%) studied in this report had acquired protein C defi-ciency at entry to the ISS trial (baseline). The presence and se-verity of acquired protein C deficiency were associated with poorclinical outcome, including lower survival rate, higher incidenceof shock, and fewer intensive care unit–free and ventilator-freedays. Although ten of the 70 patients had normal prothrombin time,partial thromboplastin times, platelet count and fibrinogen, nineof these ten patients had acquired protein C deficiency. Theseobservations are consistent with current thinking regarding theprotein C antithrombotic pathway, which assumes that consump-tion of protein C occurs before consumption of other haemostasisfactors such as antithrombin, fibrinogen and factor V.
In general, these studies have shown that protein C levelsremain low for several days in patients with sepsis, especially inpatients who do not survive, but gradually return to normal inpatients who recover.
2.4 Acquired Protein C Deficiency in Sepsis Occurs witha Wide Range of Infectious Micro-Organisms
Clinical reporting has demonstrated that protein C deficiencyoccurs in association with a wide spectrum of infectious micro-organisms, including Gram-negative bacteria (e.g. Neisseriameningitidis, Salmonella typhi, Burkholderia pseudomallei andRickettsia conorii), Gram-positive bacteria (e.g. Streptococcuspneumoniae, S. viridans, and group A haemolytic streptococci)and parasites (e.g. Plasmodium falciparum).[53]
2.4.1 Gram-Negative Infection-Induced SepsisSevere meningococcal infection, an endotoxin-mediated dis-
ease, is well known for its coagulation abnormalities. Activationof the clotting system with intravascular coagulation and micro-vascular thrombosis is a major pathogenic mechanism in menin-gococcal septic shock that is associated with organ failure and
410 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

death.[54] The meningococcal-associated procoagulant activity isthought to be triggered by meningococcal endotoxins that eitherdirectly or indirectly cause tissue factor expression on monocytesor subendothelial surfaces, with subsequent tissue factor pathwaystimulation.[55-59]
Decreased protein C levels have been widely reported in me-ningococcal septic shock and appear to be inversely associatedwith the morbidity and mortality of this disease. Powars and col-leagues[60] suggested that the development of purpura fulminansin meningococcal septic shock results from an acquired proteinC deficiency. This hypothesis is supported by findings from a1993 study demonstrating that low levels of protein C were sta-tistically correlated (p = 0.0017) with death or purpura fulminansin patients with N. meningitidis.[61] Further evidence was pro-vided when protein C activity levels were shown to be subnormalin all but one meningococcal septic shock patient enrolled in astudy (mean activity 19%).[62] The investigators also found thatprotein C levels were significantly lower in nonsurvivors thansurvivors (5 vs 23%; p = 0.0001) and demonstrated a strong neg-ative correlation between the mean size of the skin lesions andprotein C activity (r2 = 0.50; p = 0.001).
Leclerc and colleagues[63] examined protein C levels in 40children with severe infectious purpura and found that protein Cdeficiency was universally present in this patient population,even in the absence of shock and DIC. Children with shock (p =0.05) and children with DIC (p = 0.0005) had reduced protein Cantigen and protein C activity. Brandtzaeg et al.[64] reported me-dian admission levels of protein C at 29% of the normal (range10 to 47%) in patients with fulminant meningococcal septicae-mia.
Similarly low levels of protein C were found in two othertrials. One reported protein C levels of 21% in patients with me-ningococcal sepsis compared with 77% in healthy children (p =0.001).[65] The other examined microvascular coagulopathy in 79children with septic shock and purpura fulminans and reportedprotein C levels of 13% in nonsurvivors versus 22% in survivors(p = 0.001 for both groups compared with normal values).[66]
Haemostatic abnormalities are common in typhoid fevercaused by S. typhi, and systemic complications resulting frommultidrug-resistant enteric fever are being reported with increas-ing frequency.[67] Haemostatic abnormalities were studied in 25patients with multidrug-resistant enteric fever. DIC was presentin 84% and protein C activity was low at onset of illness (mean45.6%), but increased steadily with therapy to 69.6% of normallevels at day 8 (p = 0.05) and 103.0% of normal levels at day 21(p = 0.001).
Recently, Larosa et al.[68] reported results from a study ofacute septicaemic B. pseudomallei infection (melioidosis), a dis-
ease associated with substantial release of endotoxin, TNF andIL-1. Baseline and continued acquired deficiency of protein Cwere predictive of mortality (p = 0.01 and p = 0.004, respec-tively) in this group of patients.
2.4.2 Gram-Positive Infection-Induced SepsisAbnormalities in the coagulation and fibrinolytic systems
were reported to be present equally in patients with Gram-positiveand Gram-negative bacterial infections.[50] In Gram-positive bac-terial infections such as S. pneumoniae, S. viridans and group Ahaemolytic streptococci, the relationship between severity of ill-ness and protein C levels has been documented.[69,70]
2.4.3 Parasitic Infection-Induced SepsisP. falciparum malaria has been associated with thrombocyto-
penia and haemostatic abnormalities suggesting a procoagulantstate.[71] TNF, TAT and protein C were determined in 47 patientswith P. falciparum malaria.[72] The serum TNF was elevated (me-dian 38.6 ng/L) in all patients, but was significantly higher inpatients with complications (median 142 ng/L) compared withthose without complications (median 29.5 ng/L; p = 0.001). Pro-tein C activity was depressed in all patients (mean 34.2%), butwas significantly lower in patients with complications (mean30.2%) than in patients without complications (mean 49.2%; p =0.001). These reductions in protein C activity levels correlatedsignificantly (p = 0.001) with greater parasitaemia and higherTNF.
2.5 Protein C as a Prognostic Marker for Related Diseases
Protein C levels may serve as a prognostic marker for diseasesother than sepsis, including multiple organ dysfunction syndromeafter bone marrow transplantation. In a study of 199 consecutivepatients admitted for bone marrow transplant, protein C activitywas determined in patients with and without organ dysfunctionand in patients who died after transplantation.[73] Both mean andnadir protein C activity were significantly different in patientswho died compared with survivors (p = 0.01 and p = 0.005, respec-tively). Similarly, mean and nadir activities were significantlyassociated with organ dysfunction, pulmonary dysfunction (p <0.001 and p < 0.001, respectively), hepatic veno-occlusive dis-ease (p = 0.008 and p < 0.001, respectively) and central nervoussystem dysfunction (p = 0.01 and p = 0.005, respectively).
The finding of low protein C levels as a predictor of veno-occlusive disease in patients undergoing bone marrow transplanthas been confirmed in other studies.[74,75] Additionally, in pa-tients who were recipients of solid organ transplants, protein Clevels were also found to be inversely associated with thromboticcomplications and organ rejection.[76,77]
Activated Protein C in Severe Sepsis 411
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

3. Use of Recombinant Activated Protein C in Humans
Changes of coagulation along with inflammation in patientswho are severely infected have been recognised for several de-cades, but a more complete relationship of these characterisationsin patients with severe sepsis has only recently begun to emerge.In particular, a great volume of information generated over thepast several years has highlighted the role of the protein C path-way in regulating antithrombotic and profibrinolytic activities,as well as providing new appreciation of its anti-inflammatoryproperties. Several studies have shown that acquired protein Cdeficiency is prevalent in the majority of patients with sepsis.Investigators have suggested that protein C deficiency may beused as a clinical marker of sepsis, because of the data that linka low protein C level with the morbidity (shock status, DIC status,organ failure and severity of disease state) and mortality of sepsis.
Based on these and similar data, the following hypotheticalquestion was raised. Does replacement therapy with activatedprotein C or protein C improve morbidity and mortality in acutelyprotein C–deficient patients with severe sepsis and septic shock?The studies discussed in this section suggest that administrationof activated protein C or protein C reverses haemostatic alter-ations and organ dysfunction in patients with sepsis.
3.1 Administration of Protein C and Activated Protein Cin Severe Sepsis
One of the hallmark articles in the development of thought touse protein C as a therapy for severe sepsis was the work byTaylor et al.[24] In this study, human-derived activated protein Cwas administered to baboons under general anaesthesia who hadbeen given a lethal dose (LD100) of Escherichia coli. The admin-istration of protein C converted an expected 100% mortality to100% survival.
Plasma-derived protein C has been used in nonblind studiesin patients with infection-induced purpura fulminans.[70] The col-lective medical thought to use protein C as therapy received a greatcontribution from the paediatric and adult literature on adminis-tering protein C to patients with meningococcaemia.[60,61,78-87] Inanecdotal reports, protein C treatment in humans with meningo-coccal sepsis claimed a reduction in microvascular coagulation.The value of these reports in the development of activated proteinC as a viable therapy for severe sepsis cannot be overemphasised.
The development of activated protein C as a therapeutic agentresulted from brilliant work with recombinant technology.[37]
The initial laboratory work strove to achieve the recombinantprotein C with all the necessary three-dimensional relationshipsnecessary for its active sites to be functional.
3.2 Phase II Study
A phase II study of recombinant human activated protein C(rhAPC) in patients with severe sepsis was structured to assessthe safety and effect on coagulopathy of a range of doses.[37] Inaddition, the study was designed to determine an effective doseand duration of rhAPC for use in future clinical trials. The phaseII study was a double-blind, randomised, placebo-controlled,multicentre, dose-ranging (sequential) trial. It was conducted in40 community or academic medical institutions; 131 adult pa-tients with severe sepsis were enrolled. They were randomised to re-ceive an intravenous infusion of rhAPC (12, 18, 24 or 30 μg/kg/h)or placebo for 48 or 96 hours.
In the course of the study, no significant differences betweenrhAPC- and placebo-treated patients in incidence of seriousbleeding events (4 vs 5%; p > 0.999) or incidence of serious ad-verse events (39 vs 46%; p = 0.422) were detected. A significantdose-dependent decrease in both D-dimer (p < 0.001) and end-of-infusion IL-6 levels (p = 0.021) was demonstrated. No statis-tically significant effects on fibrinogen or platelet counts wereobserved. There was a trend toward a reduction in mortality withrhAPC- compared with placebo-treated patients.
3.3 Protein C Pharmacokinetics and Pharmacodynamics
Most protein C exists as an inactive zymogen at about 4 μg/ml.The inactive zymogen protein C is a vitamin K-dependent serineprotease that is converted to its activated form by thrombin whenit is complexed with thrombomodulin on the endothelial cell sur-face. Low levels of activated protein C (1 to 2 μg/L) are found inthe healthy human bloodstream. The half-life of activated proteinC is estimated at 15 minutes[27] (table II). Data from the phase IIstudy of activated protein C in severe sepsis showed that thepharmacokinetics of rhAPC were linear over the range of infu-sion rates and durations from 12 to 30 μg/kg/h for 48 to 96 hours.Steady-state plasma activated protein C concentrations wereachieved within 2 hours of starting infusion. Concentrations de-clined rapidly after stopping infusion and were generally belowthe assay’s detection limit of 5 μg/L within 4.5 hours.[88]
3.4 Phase III Study
Overall, the phase III study was tightly controlled and admin-istered.[1] It was a large, randomised, double-blind internationalstudy of 1690 patients. The baseline characteristics and risk fac-tors of the patients were well matched between the two treatmentarms. As had been seen in the phase III antithrombin trial, thisstudy also documented the presence of an ongoing activation ofcoagulation in patients with severe sepsis. Protein C deficiency
412 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

was detected in nearly 90% of the patients in whom levels weremeasured.
The phase III study showed a reduction in plasma D-dimerlevels, suggesting that the ongoing activation of the coagulationcascade in these patients with severe sepsis was diminished byactivated protein C. The activated protein C treatment group, asa whole, started at a higher average absolute value of IL-6 thanthe placebo group. When the IL-6 data were portrayed as a per-centage change from baseline within the two treatment arms,there appeared to be a greater reduction in IL-6 within the acti-vated protein C group. Whether to place emphasis on the absolutevalues or the percentage change within the groups makes theinterpretation of these data difficult; i.e. it is unclear whether theIL-6 data support the notion that treatment attenuated the inflam-matory cascade.
The absolute reduction in the 28-day mortality rate was 6.1%(30.8% mortality in the placebo group compared with 24.7% inthe group assigned to receive activated protein C), and the rela-tive risk of death in the treated group was reduced by nearly 20%(table III). The statistical analysis reveals a p value of 0.005,making the odds 5 chances out of 1000 that there truly was nodifference between groups. The p value suggests an extremelylow chance of a β error, i.e. rejecting the null hypothesis (nodifference between groups) when there is truly no difference.This p value does tell us with strength that a difference betweenthe treatment groups exists. A p value offers no information aboutthe difference itself, i.e. how large it is. To determine this char-acteristic we use confidence intervals (CI).
The confidence intervals indicate the range in which we mayfind the ‘true’ absolute risk reduction in mortality. The absoluterisk reduction is the characteristic used to generate what is re-ferred to in the pharmaceutical industry as the number needed totreat (NNT) to save one life. The phase III study data demon-strated an NNT of 16. If we try to estimate the worst possiblescenario for the true difference in mortality between the groups,we would use the higher end of the confidence interval of themortality risk reduction as the ‘true’ value. We could then calcu-
late what the NNT would become. In the Recombinant HumanActivated Protein C Worldwide Evaluation in Severe Sepsis(PROWESS) study,[1] the relative risk (RR) of death (mortalitywith treatment/mortality with placebo = 0.247/0.308) was 0.80(CI 0.69 to 0.94). In this example, if the RR is 0.94 (the top endof the confidence interval given in the study), the mortality in theactivated protein C group would have been 28.9% (0.94 × 30.8 =28.9%), and the absolute risk reduction 1.85% (30.8 – 28.9 =1.85%). Therefore, the NNT in the ‘worst case scenario’ trans-lates to 54 (NNT = 1/absolute risk reduction = 1/1.85 = 54). Thatis, 54 patients would need to be treated to move one person des-tined for the nonsurvivor group to the survivor group as a resultof treatment with activated protein C.
The accompanying editorial to the PROWESS study[89] con-cluded that the treatment was effective regardless of age, severityof illness, the number of dysfunctional organs or systems, the siteof infection (pulmonary or extrapulmonary), and the type of in-fecting organism (Gram-positive, Gram-negative or mixed).When the data were reviewed by the FDA, the ad hoc commit-tee’s response differed in interpretation as to the efficacy acrosssubgroups.
The response of the FDA has given rise to much debate as tothe value of subgroup interpretation. There are many referencesin the medical literature to the use of subgroup analyses. Cer-tainly, the overall effect of a study would not be interpreted froman isolated subgroup analysis. Traditionally, it is the justificationof the primary endpoint that determines whether a study is viewedas positive or negative. In the situation where there are many sub-groups pointing to an alternative interpretation and one that canbe viewed as making a reasonable conclusion, then that one sub-group is given attention.
The FDA reviewed the mortality versus Acute Physiologyand Chronic Health Evaluation [APACHE]-II score data and con-cluded that the administration of activated protein C did showremarkable efficacy at the higher end of APACHE II scores, butwas no better than placebo and possibly even more harmful thanplacebo at the lower APACHE II scores[90] (figure 6).
The FDA has since mandated that the product’s package in-sert must reflect this interpretation. The package insert reads that
Table II. Administration information for recombinant human activatedprotein C (drotrecogin alpha activated)
Given by 96-hour continuous infusion
Use dedicated intravenous line (intravenous or multi-lumen)
May be run with 0.9% saline, dextrose 5% in water, or Ringer’s lactatewith up to 40 mEq/L potassium chloride
Comes as a sterile, freeze-dried preparation in glass vials, ready forreconstitution
Dose alteration not required for acute hepatic or acute renal failure
Half-life approximately 15 minutes; undetectable levels in 1 hour
Table III. Summary of Recombinant Human Activated Protein C WorldwideEvaluation in Severe Sepsis (PROWESS) trial efficacy results[1]
Mortality: 30.83% for placebo vs 24.72% for activated protein C (p = 0.0054)
Absolute Risk Reduction (ARR) = 6.11% reduction in absolute mortality
Reduction in relative risk of death = 19.43% (1 – [treatment/placebo] = 1 – (24.7/30.83) × 100)
Number needed to treat to save 1 life (NNT) = 16 (1/ARR = 1/6.11 × 100)
Activated Protein C in Severe Sepsis 413
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

‘Baseline APACHE II score, as measured in PROWESS, wascorrelated with risk of death; among patients receiving placebo,those with the lowest APACHE II scores had a 12% mortalityrate, while those in the 2nd, 3rd, and 4th APACHE quartiles hadmortality rates of 26%, 36% and 49%, respectively. The observedmortality difference between rhAPC and placebo was limited tothe half of patients with higher risk of death, i.e. APACHE IIscore >25, the 3rd and 4th quartile APACHE II scores. The effi-cacy of rhAPC has not been established in patients with lowerrisk of death, e.g. APACHE II score <25.’
The clinical dilemma now faced by critical care practitionersis that the APACHE II system is not designed, nor has it beenvalidated, for use to discriminate any parameter for the individualpatient. The FDA’s response has suggested that in the patients inthe lower quartiles of the APACHE II score rhAPC did notdemonstrate efficacy. That population interpretation does notmake for easy application when dealing with a single patient atthe bedside. The FDA has mandated further studies of activatedprotein C in patients with lower APACHE II scores.
3.5 Serious Adverse Events during the PROWESS Studyand Implications for Future Administration
The incidence of serious bleeding was 3.5% in treated patientsand 2.0% in patients in the placebo group, a difference that almostreached statistical significance (p = 0.06).[1] Activated protein Cdoes produce anticoagulant effects, and there was a clinical trendtowards increased bleeding with activated protein C. Put in per-spective with the reduction in mortality, however, the increasedrisk of bleeding was small. The percentage of patients receivingat least one unit of packed red cell transfusion was similar be-tween the two groups; however, the absolute number of bloodunits administered per patient within each of the two groups wasnot part of the published data.
The study protocol excluded patients with a higher risk ofbleeding, such as those with chronic liver disease, those with chronicrenal failure who were dependent on dialysis, those who had un-dergone recent surgery, organ transplant recipients, patients withthrombocytopenia (defined as a platelet count of <30 000/mm3)and those who had taken aspirin at a dosage of >650 mg/daywithin 3 days before the study. Further studies are needed toassess the safety of activated protein C in these groups of patients.
4. Conclusions
In sepsis, the conversion of inactive protein C to activatedprotein C is impaired. This conversion is controlled via the actionof thrombin bound to thrombomodulin, when thrombomodulin ispresent on the cell membrane. During sepsis, an early depletionof protein C seems to be observed and may be a result of a combi-nation of several mechanisms. Protein C is susceptible to degra-dation by neutrophil elastase, which is released during sepsis. Thecontinuous and rapid conversion of protein C to activated protein Ccan lead to depletion of the plasma pool of protein C. The bio-synthesis of protein C to replenish the circulating pool, a processthat is dependent on the liver, may be inadequate because of inhib-itory effects of acute phase proteins or hepatic dysfunction. In addi-tion to the decreased plasma level of protein C, protein C activationmay be reduced by the down-regulation of pro-inflammatorycytokines.
Activated protein C represents a technological and therapeu-tic breakthrough. The phase III study[1] is the culmination of overa decade of reports that link inflammation and coagulation. Im-portantly, the phase III study indicates that administration of ananticoagulant protein reduced mortality in patients with severesepsis. The study was not designed to treat patients with clinicalsigns of mild to moderate sepsis who did not have evidence ofend-organ injury. A trial is needed to show a benefit in thesepatients before practitioners can safely extend administration tothese less ill patients. Furthermore, the risks and benefits of theagent must be studied in patients at a higher risk of bleeding, inchildren, in immunosuppressed patients, and especially thosewith thrombocytopenia or neutropenia. Currently, the inclusionand exclusion criteria stipulated in the phase III trial are usefulguidelines for clinical use in choosing patients for activated pro-tein C therapy.
How to apply the FDA’s stipulation regarding the APACHEII data to individual bedside practice is unclear, since theAPACHE II system was not designed for such bedside distinc-tions. Current recommendations therefore would certainly in-clude the group of patients with severe sepsis who, at presenta-tion, fulfil the phase III study’s entry criteria and who do not
01020
30405060
7080
10 15 20 25 30 35 40 45 50
APACHE II score (intervals of 5 units)
Mor
talit
y (%
)
PlaceborhAPC
Fig. 6. Acute Physiology and Chronic Health Evaluation (APACHE)-II scoreversus mortality. rhAPC = recombinant human activated protein C (repro-duced from the US Food and Drug Administration web site[90]).
414 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

possess an exclusion. For patients with severe sepsis who do not‘fit’ within the entry and exclusion criteria, the decision to ad-minister activated protein C is ultimately based on good clinicaljudgement of the treating physician.
Acknowledgements
Dr Morris is a consultant for Eli Lilly. No sources of funding were directlyused to assist in the preparation of this manuscript, however.
References1. Bernard GR, Vincent J-L, Laterre P-F, et al. , for the Recombinant Human Acti-
vated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) Study
Group. Efficacy and safety of recombinant human activated protein C for se-
vere sepsis. N Engl J Med 2001; 344: 699-709
2. Natanson C, Esposito CJ, Banks SM. The sirens’ songs of confirmatory sepsis
trials: selection bias and sampling error. Crit Care Med 1998; 26 (12): 1927-31
3. Sprung CL, Eidelman LA, Pizov P, et al. The HA-1A Sepsis Study Group. Influ-
ence of alterations in forgoing life-sustaining treatment practices on a clinical
sepsis trial. Crit Care Med 1997; 25: 383-7
4. Bone RC, Balk RA, Cerra FB, et al. , and the ACCP/SCCM Consensus Confer-
ence Committee. Definitions for sepsis and organ failure and guidelines for the
use of innovative therapies in sepsis. Chest 1992; 101: 1644-55
5. Aird WC. Vascular bed-specific hemostasis: role of endothelium in sepsis patho-
genesis. Crit Care Med 2001; 29: S28-35
6. Rosenberg RD, Aird WC. Vascular-bed-specific hemostasis and hypercoagulable
states. N Engl J Med 1999; 340 (20): 1555-64
7. Mesters RM, Mannucci PM, Coppola R, et al. Factor VIIa and antithrombin III
activity during severe sepsis and septic shock in neutropenic patients. Blood
1996; 88: 881-6
8. Fourrier F, Chopin C, Goudemand J, et al. Septic shock, multiple organ failure,
and disseminated intravascular coagulation: compared patterns of antithrombin
III, protein C, and protein S deficiencies. Chest 1992; 101: 816-23
9. Warren BL, Eid A, Singer P, et al. Caring for the critically ill patient: high-dose
antithrombin III in severe sepsis: a randomized controlled trial. JAMA 2001;
286 (15): 1869-78
10. Mann KG, van’t Veer C, Cawthern K, et al. The role of the tissue factor pathway
in initiation of coagulation. Blood Coagul Fibrinolysis 1998; 9 Suppl. 1: S3-7
11. Sadler JE. Thrombomodulin structure and function. Thromb Haemost 1997; 78:
392-5
12. Esmon CT. Thrombomodulin as a model of molecular mechanisms that modulate
protease specificity and function at the vessel surface. FASEB J 1995; 9: 946-55
13. Xu J, Esmon NL, Esmon CT. Reconstitution of the human endothelial cell protein
C receptor with thrombomodulin in phosphatidylcholine vesicles enhances
protein C activation. J Biol Chem 1999; 274: 6704-10
14. Lin JH, McLean K, Morser J, et al. Modulation of glycosaminoglycan addition
in naturally expressed and recombinant human thrombomodulin. J Biol Chem
1994; 269: 25021-30
15. Bourin MC, Ohlin AK, Lane DA, et al. Relationship between anticoagulant ac-
tivities and polyanionic properties of rabbit thrombomodulin. J Biol Chem
1988; 263: 8044-52
16. Alberio L, Lammle B, Esmon CT. Protein C replacement in severe
meningococcemia: rationale and clinical experience. Clin Infect Dis 2001; 32
(9): 1338-46
17. Ishii H, Uchiyama H, Kazama M. Soluble thrombomodulin antigen in conditioned
medium is increased by damage of endothelial cells. Thromb Haemost 1991;
65: 618-23
18. Fukudome K, Esmon CT. Identification, cloning, and regulation of a novel endo-
thelial cell protein C/activated protein C receptor. J Biol Chem 1994; 269:
26486-91
19. Moore KL, Andreoli SP, Esmon NL, et al. Endotoxin enhances tissue factor and
suppresses thrombomodulin expression of human vascular endothelium in
vitro. J Clin Invest 1987; 79: 124-30
20. Bartha K, Brisson C, Archipoff G, et al. Thrombin regulates tissue factor and
thrombomodulin mRNA levels and activities in human saphenous vein endo-
thelial cells by distinct mechanisms. J Biol Chem 1993; 268: 421-9
21. Esmon CT, Xu J, Gu J-M, et al. Endothelial protein C receptor. Thromb Haemost
1999; 82: 251-8
22. Faust SN, Heyderman RS, Levin M. Coagulation in severe sepsis: a central role
for thrombomodulin and activated protein C. Crit Care Med 2001; 29: S62-8
23. Sims PJ, Wiedmer T, Esmon CT, et al. Assembly of the platelet prothrombinase
complex is linked to vesiculation of the platelet plasma membrane: studies in
Scott syndrome: an isolated defect in platelet procoagulant activity. J Biol
Chem 1989; 264: 17049-57
24. Taylor Jr FB, Chang A, Esmon CT, et al. Protein C prevents the coagulopathic
and lethal effects of E. coli infusion in the baboon. J Clin Invest 1987; 79:
918-25
25. Faust SN, Levin M, Harrison OB, et al. Dysfunction of endothelial protein C
activation in severe meningococcal sepsis. N Engl J Med 2001; 345 (6): 408-16
26. Heeb MJ, Gruber A, Griffin JH. Identification of divalent metal ion-dependent
inhibition of activated protein C by a2-macroglobulin and a2-antiplasmin in
blood and comparisons to inhibition of factor Xa, thrombin, and plasmin. J Biol
Chem 1991; 266: 17606-12
27. Esmon CT. Protein C anticoagulant pathway and its role in controlling microvas-
cular thrombosis and inflammation. Crit Care Med 2001; 29: S48-52
28. Bajzar L, Morser J, Nesheim M. TAFI, or plasma procarboxypeptidase B, couples
the coagulation and fibrinolytic cascades through the thrombin-thrombomodulin
complex. J Biol Chem 1996; 271: 16603-8
29. Weitz JI, Hirsh J. New anticoagulant drugs. Chest 2001; 119: 95S-107S
30. Sakata Y, Loskutoff DJ, Gladson CL, et al. Mechanism of protein C-dependent
clot lysis: role of plasminogen activator inhibitor. Blood 1986; 68: 1218-23
31. Tapper H, Herwald H. Modulation of hemostatic mechanisms in bacterial infec-
tious diseases. Blood 2000; 96: 2329-37
32. ten Cate H, Schoenmakers S, Franco R, et al. Microvascular coagulopathy and
disseminated intravascular coagulation. Crit Care Med 2001; 29: S95-8
33. White B, Schmidt M, Murphy C, et al. Activated protein C inhibits lipopolysac-
charide-induced nuclear translocation of nuclear factor kB (NF-kB) and tumour
necrosis factor a (TNF-a) production in the THP-1 monocytic cell line. Br J
Haematol 2000; 110: 130-4
34. Hancock WW, Tsuchida A, Hau H, et al. The anticoagulants protein C and protein
S display potent anti-inflammatory and immuno-suppressive effects relevant
to transplant biology and therapy. Transplant Proc 1992; 24: 2302-3
35. Murakami K, Okajima K, Uchiba M, et al. Activated protein C prevents LPS-in-
duced pulmonary vascular injury by inhibiting cytokine production. Am J Physiol
1997; 272: L197-202
36. Joyce DE, Gelbert L, Ciaccia A, et al. Gene expression profile of antithrombotic
protein c defines new mechanisms modulating inflammation and apoptosis. J
Biol Chem 2001; 276 (14): 11199-203
37. Yan SB, Razzano P, Chao YB, et al. Characterization and novel purification of
recombinant human protein C from three mammalian cell lines. Biotechnology
1990; 8: 655-61
Activated Protein C in Severe Sepsis 415
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

38. Grinnell BW, Hermann RB, Yan SB. Human protein C inhibits selectin-mediated
cell adhesion: role of unique fucosylated oligosaccharide. Glycobiology 1994;
4: 221-5
39. Levi M, ten Cate H. Disseminated intravascular coagulation. N Engl J Med 1999;
341: 586-92
40. Leithauser B, Matthias FR, Nicolai U, et al. Hemostatic abnormalities and the
severity of illness in patients at the onset of clinically defined sepsis: possible
indication of the degree of endothelial cell activation? Intensive Care Med
1996; 22: 631-6
41. Gando S, Kameue T, Nanzaki S, et al. Disseminated intravascular coagulation is
a frequent complication of systemic inflammatory response syndrome. Thromb
Haemost 1996; 75: 224-8
42. Gando S, Kameue T, Nanzaki S, et al. Participation of tissue factor and thrombin
in posttraumatic systemic inflammatory syndrome. Crit Care Med 1997; 25:
1820-6
43. Gando S, Nanzaki S, Sasaki S, et al. Activation of the extrinsic coagulation path-
way in patients with severe sepsis and septic shock. Crit Care Med 1998; 26:
2005-9
44. Gando S, Nanzaki S, Morimoto Y, et al. Systemic activation of tissue-factor
dependent coagulation pathway in evolving acute respiratory distress syn-
drome in patients with trauma and sepsis. J Trauma Injury Infect Crit Care
1999; 47 (4): 719-23
45. Ikegami K, Suzuki Y, Yukioka T, et al. Endothelial cell injury as quantified by
the soluble thrombomodulin level predicts sepsis/multiple organ dysfunction
syndrome after blunt trauma. J Trauma 1998; 44: 789-94
46. Iba T, Yagi Y, Kidokoro A, et al. Increased plasma levels of soluble thrombo-
modulin in patients with sepsis and organ failure. Surg Today 1995; 25: 585-90
47. Griffen JH, Mosher DF, Zimmerman TS, et al. Protein C, an antithrombotic
protein, is reduced in hospitalized patients with intravascular coagulation.
Blood 1982; 60: 261-4
48. Sheth SB, Carvalho AC. Protein S and C alterations in acutely ill patients. Am J
Hematol 1991; 36: 14-9
49. Hesselvik JF, Malm J, Dahlback B, et al. Protein C, protein S and C4b-binding
protein in severe infection and septic shock. Thromb Haemost 1991; 65: 126-9
50. Lorente JA, Garcia-Frade LJ, Landin L, et al. Time course of hemostatic abnor-
malities in sepsis and its relation to outcome. Chest 1993; 103: 1536-42
51. Hartman DL, Bernard GR, Helterbrand JD, et al. Recombinant human activated
protein C (rhAPC) improves coagulation abnormalities associated with severe
sepsis. Intensive Care Med 1998; 24 Suppl. 1: S177
52. Yan SB, Helterbrand JD, Hartman DL, et al. Low levels of protein C are associ-
ated with poor outcome in severe sepsis. Chest 2001; 120 (3): 915-22
53. Fisher Jr CJ, Yan SB. Protein C levels as a prognostic indicator of outcome in
sepsis and related diseases. Crit Care Med 2000; 28 (9): S49-56
54. McManus ML, Churchwell KB. Coagulopathy as a predictor of outcome in me-
ningococcal sepsis and the systemic inflammatory response syndrome with
purpura. Crit Care Med 1993; 21: 706-11
55. Osterud B, Flaegstad T. Increased tissue thromboplastin activity in monocytes of
patients with meningococcal infection: related to an unfavorable prognosis.
Thromb Haemost 1983; 49: 5-7
56. Wuillemin WA, Fijnvandraat K, Derkx BHF, et al. Activation of the intrinsic
pathway of coagulation in children with meningococcal septic shock. Thromb
Haemost 1995; 74: 1436-41
57. Moore KL, Andreoli SP, Esmon NL, et al. Endotoxin enhances tissue factor and
suppresses thrombomodulin expression of human vascular endothelium in
vitro. J Clin Invest 1987; 79: 124-30
58. Bevilacqua MP, Pober JS, Majeau GR, et al. Interleukin 21 induces biosynthesis
and cell surface expression of procoagulant activity in human vascular endo-
thelial cells. J Exp Med 1984; 160: 618-23
59. Warr TA, Rao LV, Rapaport SI. Disseminated intravascular coagulation in rabbits
induced by administration of endotoxin or tissue factor: effect of anti-tissue
factor antibodies and measurement of plasma extrinsic pathway inhibitor ac-
tivity. Blood 1990; 75: 1481-9
60. Powars DR, Rogers ZR, Patch MJ, et al. Purpura fulminans in meningococcemia:
association with acquired deficiencies of proteins C and S. N Engl J Med 1987;
317: 571-4
61. Powars D, Larsen R, Johnson J, et al. Epidemic meningococcemia and purpura
fulminans with induced protein C deficiency. Clin Infect Dis 1993; 17: 254-61
62. Fijnvandraat K, Derkx B, Peters M, et al. Coagulation activation and tissue ne-
crosis in meningococcal septic shock: severely reduced protein C levels predict
a high mortality. Thromb Haemost 1995; 73: 15-20
63. Leclerc F, Hazelzet J, Jude B, et al. Protein C and S deficiency in severe infectious
purpura of children: a collaborative study of 40 cases. Intensive Care Med
1992; 18: 202-5
64. Brandtzaeg P, Kierulf P, Gaustad P, et al. Plasma endotoxin as a predictor of
multiple organ failure and death in systemic meningococcal disease. J Infect
Dis 1989; 159: 195-204
65. Blanco A, Guisasola JA, Solis P, et al. Fibronectin in meningococcal sepsis:
correlation with antithrombin III and protein C. Acta Paediatr Scand 1990; 79:
73-6
66. Hazelzet JA, Risseeuw-Appel IM, Kornelisse RF, et al. Age-related differences
in outcome and severity of DIC in children with septic shock and purpura.
Thromb Haemost 1996; 76: 932-8
67. Koul PA, Quadri MI, Wani JI, et al. Haemostatic abnormalities in multidrug-re-
sistant enteric fever. Acta Haematol 1995; 93: 13-9
68. Larosa SP, Opal SM, Utterback B, et al. Decreased protein C, protein S and
antithrombin III levels are predictive of poor outcome in gram-negative sepsis
caused by Burkholderia pseudomallei. Crit Care 2000; 4 Suppl. 1: S18
69. Smith KJ, Neal J, Winton EF, et al. Purpura fulminans and S. pneumoniae sepsis
with severe acquired protein C deficiency successfully treated with recombi-
nant human activated protein C [abstract 2334]. Thromb Haemost 1999; 82
Suppl Aug: 738
70. Gerson WT, Dickerman JD, Bovill EG, et al. Severe acquired protein C deficiency
in purpura fulminans associated with disseminated intravascular coagulation:
treatment with protein C concentrate. Pediatrics 1993; 91: 418-22
71. Hemmer CJ, Kern P, Radtke KP, et al. P. falciparum malaria with procoagulant
changes and increased TNF-alpha serum level. Klin Wochenschr 1990; 68:
281-5
72. Hemmer CJ, Kern P, Holst FGE, et al. Activation of the host response in human
Plasmodium falciparum malaria: relation of parasitemia to tumor necrosis fac-
tor/cachectin, thrombin-antithrombin III, and protein C levels. Am J Med 1991;
91: 37-4
73. Haire WD, Ruby EI, Gordon BG, et al. Multiple organ dysfunction syndrome in
bone marrow transplantation. JAMA 1995; 274: 1289-95
74. Faioni EM, Krachmalnicoff A, Bearman SI, et al. Naturally occurring anticoag-
ulants and bone marrow transplantation: plasma protein C predicts the devel-
opment of venocclusive disease of the liver. Blood 1993; 81: 3458-62
75. Harper PL, Jarvis J, Jennings I, et al. Changes in the natural anticoagulants fol-
lowing bone marrow transplantation. Bone Marrow Transplant 1990; 5: 39-42
76. Sorensen PJ, Nielsen AH, Knudsen F, et al. Protein C renal allotransplantation
during the perioperative period. J Intern Med 1989; 226: 101-5
77. Harper PL, Edgar PF, Luddington RJ, et al. Protein C deficiency and portal throm-
bosis in liver transplantation in children. Lancet 1988; II: 924-7
416 Morris et al.
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)

78. Rintala E, Seppala O, Kotilainen P, et al. Protein C in the treatment of coagulo-
pathy in meningococcal disease. Lancet 1996; 347: 1767
79. Rintala E, Seppala O, Kotilainen P, et al. Protein C in the treatment of coagulo-
pathy in meningococcal disease. Crit Care Med 1998; 26: 965-8
80. Rivard GE, David M, Farrell C, et al. Treatment of purpura fulminans in
meningococcemia with protein C concentrate. J Pediatrics 1995; 126: 646-52
81. Rivard GE, David M, Farrell C, et al. Treatment of purpura fulminans in
meningococcemia with protein C concentrate. Thromb Haemost 1993; 69: A2339
82. Smith OP, White B, Vaughn D, et al. Use of protein C concentrate, heparin and
haemodiafiltration in meningococcus-induced purpura fulminans. Lancet
1997; 350: 1590-3
83. Veldman A, Escuriola-Ettingshausen C, Beeg T, et al. Treatment of DIC in septic
shock with protein C concentrate. Blood 1997; 90: A3271
84. Kreuz W, Escuriola-Ettingshausen C, Beeg T, et al. Protein C concentrate for
meningococcal purpura fulminans. Lancet 1998; 351: 986-7
85. Betrosian AP, Balla M, Kofinas G, et al. Protein C in the treatment of coagulo-
pathy in meningococcal sepsis. Crit Care Med 1999; 27: 2849-50
86. Darnstadt GL. Acute infectious purpura fulminans: pathogenesis and medical
management. Pediatric Dermatol 1998; 15: 169-83
87. Rintala E, Kauppila M, Seppala OP, et al. Protein C substitution in sepsis-asso-
ciated purpura fulminans. Crit Care Med 2000; 28 (7): 2373-8
88. Bernard GR, Ely EW, Wright TJ, et al. Safety and dose relationship of recombi-
nant human activated protein C for coagulopathy in severe sepsis. Crit Care
Med 2001; 29: 2051-9
89. Matthay MA. Severe sepsis: a new treatment with both anticoagulant and anti-
inflammatory properties. N Engl J Med 2001; 344 (10): 759-62
90. US Food and Drug Administration’s web site. Available from URL: http://www.fda.gov/
ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/sld023.htm [Accessed 2002 Jan 9]
Correspondence and offprints: Dr Peter E. Morris, Divisions of Pulmonaryand Critical Care Medicine and Infectious Diseases, Wake Forest UniversitySchool of Medicine, Winston Salem, NC 27104, USA.E-mail: [email protected]
Activated Protein C in Severe Sepsis 417
© Adis International Limited. All rights reserved. Biodrugs 2002; 16 (6)















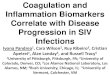
![Critical Care - Mednemolnx.mednemo.it/wp-content/uploads/2009/04/cc7765.pdf · coagulation (DIC) and bear a risk of bleeding diathesis [7]. In severe inflammation, coagulation-regulating](https://img.pdfslide.net/doc/110x75/5e3efa686ed93454ed5dfcab/critical-care-coagulation-dic-and-bear-a-risk-of-bleeding-diathesis-7-in.jpg)












