Embed Size (px)
Citation preview
Relationship of Child Psychopathology to ParentalAlcoholism and Antisocial Personality Disorder
SAMUEL KUPERMAN, M.D .. STEVEN S. SCHLOSSER, MAT., ]AMA LIDRAL, BA, AND WENDY REICH, PH.D.
ABSTRACT
Objective: To evaluate the contributions of familial factors, including parental diagnoses of alcoholism andlor antisocial
personality disorder (ASPD), to the risk of developing various child psychiatric diagnoses. Method: Four hundred sixty
three children and their biological parents were interviewed with adult and child versions of the Semi-Structured
Assessment for the Genetics of Alcoholism. Demographic and psychiatric data were compared across 3 groups of chil
dren on the basis of the presence of parental alcoholism and ASPD (no other parental diagnoses were examined).
Generalized estimating equations analyses allowed the inclusion of multiple children from each family in the analyses.
Results: Among offspring, parental alcoholism was associated with increased risks for attention-deficit hyperactivity dis
order, conduct disorder (CD), and overanxious disorder. Parental alcoholism plus ASPD was associated with increased
risk for oppositional defiant disorder. Dysfunctional parenting style was associated with increased risks for CD, alcohol
abuse, and marijuana abuse. Low family socioeconomic status was associated with increased risk for CD. Conclusions:
Parental diagnoses of alcoholism and ASPD were associated with increased risks for a variety of childhood psychiatric
disorders, and dysfunctional parenting style was associated with the diagnoses of CD, alcohol abuse, and marijuana
abuse. J. Am. Acad. Child Ado/esc. Psychiatry, 1999, 38(6):686-692. Key Words: childhood psychopathology, genetics,
alcohol, antisocial personality disorder, children of alcoholic parents.
The rate of behavioral probJems in children of alcoholics(COAs) seems increased compared with the rate ofbehavioral problems in children whose parents are not alcoholic. West and Prinz (1987) reported an increasedfrequency of delinquency, truancy, social inadequacy, andsomatic problems. Roosa et al. (1988) and Tubman(1993) each stated that COAs have more anxiety and lowmood symptoms than children whose parents are notalcoholic. Connolly et aI. (1993) reported that COAs havelower verbal and reading scores and have more schoolrelated behavior problems at age 9 and more home-relatedproblems at age 13. Finally, COAs begin drinking at anearlier age (Fergusson et al., 1994) and have more alcoholrelated problems (Hill and Muka, 1996; Schuckit, 1982).
Accepted December 7. 1998.Dr. Kuperman is Associate Professor and Mr. Schlosser and Ms. Lidral are
Research Assistants. Department of"Psychilltry. University of IOWIl College of
Medicine. 10WI' City. Dr. Reich is ResearchAssociate Professor; Department of
Psychiatry. WllShington University School ofMedicine. St. Louis.
Reprint requests to Dr. Kuperman, Department of Psychiatry. University of
Iowa Hospitals and Clinics. 200 Hau.kins Drive. RM 1873 JPP. Iowa City. IA
52242-1057.
0890-8567/99/.)806-0686101999 by the American Academy of Childand Adolescent Psychiatry.
686
The association of parental alcoholism with the ratesof actual child psychiatric disorders is less clear. Earlystudies of COAs found a positive increase in the rate ofattention-deficit hyperactivity disorder (AOHO) (Earlset al., 1988; Goodwin, 1985; Goodwin et al., 1975;Stewart et al., 1980) and childhood conduct disorder(CD) or oppositional defiant disorder (ODD) (Earlset al., 1988; Merikangas et al., 1985; Steinhausen et al.,1984), but more recent studies have not confirmed thesenndings. Hill and Hruska (1992) examined the rates ofpsychopathology in 53 children from families with multigenerational alcoholism and compared them with ratesin 42 children who had no nrst-degree relatives with aDSM-III diagnosis; the 2 groups did not differ in therates of specific DSM-III diagnoses. Reich et al. (1993)found that the rates of DSM-III diagnoses of ODD,CD, overanxious disorder (OAO), and marijuana abusesignificantly increased as the number of parents withalcohol dependence increased from 0 to 2 in a study of123 children. Finally, Hill and Muka (1996) found that38 adolescents with multiple family members with alcoholism were more likely to have a psychiatric diagnosis(but no specific diagnosis) than 38 matched adolescents
J. AM. ACAD. CHI!.D A[)O!.ESc:. PSYCHIATRY, '>8:6. JUNE 1999

from families without a history of alcoholism in firstand second-degree relatives.
The differences in published rates of child psychiatricdisorders in COAs have 4 possible explanations. First,the increased rates of parental separation, decreased family income, and a dysfunctional parenting style (DPS)(Connolly et aI., 1993) have not been accounted for instudies of COAs . These factors by them selves are associated with higher rates of child psychopathology (Garmezyand Masten, 1994; Patterson et al., 1989; Patterson andStouthamer-Loeber, 1984). Second, only a few studieshave examined the possibility that the increased rate ofchildhood psychiatric disorders in COAs is due to acomorbid psychiatric diagnosis in the alcoholic parentor to psychiatric illness in the nonalcoholic spouse (Hiller al., 1977; Tubman, 1993).Third, studies have frequentlyused restrictive subject groups (e.g., examining childrenof parents in treatment for alcoholism, or, conversely,examining children with specific psychiatric disordersfollowed by investigation of their parents for alcoholism) with relatively small sample sizes, limiting the ability to generalize findings (Connolly et al., 1993). Fourth,studies have used relatively small sample sizes in comparison to the complex issues being explored.
The Collaborative Study on the Genetics of Alcoholism (COGA) is a National Institute on Alcohol Abuseand Alcoholism-funded study that is able to addressthese concerns. COGA is composed of 6 sites located atthe State University of New York at Brooklyn, the University of Connecticut at Farmington, Indiana Universityin Indianapolis, Washington University in St. Louis, theUniversity of Iowa in Iowa City, and the University ofCalifornia at San Diego. Data collected for COGA arewide-ranging and for each participant include fam ilyand demographic information, laboratory tests, and asemistructured psychiatr ic assessment.
The goal of this study was to use the COGA sampleto assess whether the: risks for specific child psychiatricdiagnoses were increased in COAs , and if so, to determinewhether these increa ses were related to parental diagnoses of alcoholism and antisocial personality disorder(ASPD) and/or DPS and low socioeconomic status (SES).
METHOD
A description of the study design and copies of all interview instruments were approved by the institutional review boards at all 6 sites.Parents provided info rmed con sent and child ren younger th an 18years of age provided informed assent for participation in the stu dy.
J. AM. ACAD . CHILD A D O I. ESC. PSYCHIAT RY, .,8:(" JUN E 1999
PSYCHOPATH OLO GY IN C H ILD REN OF ALCOH OLI C S
Subjects
Three quarters of the children in thi s study were from high-riskCOGA families identified through the following criteria. First, an adultfamily member had to be in treatment for alcoholism. Second, according to the Semi-Structured Assessment for the Genetics of Alcoholism(SSAGA) (Bucholz er al., 1994). th is individual was determi ned to haveboth a DSM-lll-R diagn osis of alcohol dependence and a Feighnerdiagnosis of definite alcoho lism (Feighner et al., 1972) . Third, thisinde x person gave perm ission to contact all his/her immediate andextended relatives, includ ing children. for enrollment into the study.The remaining children came from low-risk CO GA families whose parents were recruited from dental and family practice clinics, businesses,churches, and driver's license renewal centers. The parents of these children were also interviewed with the SSAGA.T he presence or absence ofany psychiatric disorder, including alcohol dependence, was not used toexclude low-risk families.
Indiv iduals in this study younger th an the age of 18 were interviewed using the Child Semi-Structured Assessment for the Geneticsof Alcoholism (C- SSAGA). which closely follows the D iagnosticInterview for Children and Adolescents (Reich er al., 1982) andallows the identification of DSM-lll-R diagno ses. Three versions ofthe C-SSAGA exist: the C-SSAGA-C for ch ildren aged 7 to 12 years,the C-SSAGA-A for children aged 13 to 17 years (both versions haveage-app ropr iate wording and examples), and a parent corroboratingversion, the C-SSAGA-P.
To be included in th is study a family had to have at least 4 completed semistructu red interviews; both biological parents had to havecompleted SSAGAs, each child had to have completed a C-SSAGA,and a parent (most likely the biological mother) had to complete a CSSAGA-P for each child . Research assistants who had extens ive training gave all interviews . Furthermore. all inte rviewers part icipated inmonthly conference calls to review subject data and reduce the likelihood of int erviewer d rift. Different research assistants int erviewedparents and children , which minimized potential int erviewer biasdu e to a priori knowledge of parent or child symptomatology.
C hild ren in the sample were separated into groups based on thepr esen ce or absence of parental DSM-lll-R diagnoses of alcoholdependence (alcoholism) and/or ASPO. To more clearly define "alcoholism," i.e., a DSM-1I1-Rdiagnosis of alcohol dependence, 10 families in which any parent had a DSM-Ill-R diagnosis of alcohol abusewere dropped from further analysis. Furthermore, because of smallnumbers, 3 children whose parents had ASPO but no alcohol diagnoseswere also excluded from the analysis. T his resulted in the 3 parenttype (PT) groups: 118 children from 67 families in the "no parentalalcoholism or ASPO " (NPAA) group, 266 children from 165 familiesin the "parental alcoholism only" (PAO ) group, and 79 children from50 families in the "both parental alcoholism and ASPO" (BPAA)group .
The relationships of 2 different types of variables were examinedacross the 3 PT groups. The first consisted of the actual DSM-lll-Rdiagnoses of the children and the second consisted of family variables,which had the possihiliry of influencing these psychiatri c diagnoses.The diagnoses examined in this study were the disruptive behavior disorders of AOHO, ODD, and CD; the internalizing disorders of OADand separation anxiety disorder (SAD); and the substance abuse disorders of alcohol abuse and marijuana abuse. (Because of potential difficulties associated with the more episodic diagnosis of major depressivedisorder in children, it was not included in this study.) These diagnoseswere obtained in a mann er similar to that of Bird er al. (1992 ) andShaffer et a1. (1996); computer algorithm s were used to combine symptoms from both the child and parent versions of the C-SSAGA. thoughident ical symptoms reported by both were counted only once.
687

KUPERMAN ET AL.
Family variables were divided into 2 clusters. The first cluster, asshown in Table I, was based on the suggestion by Patterson er al.(1989) that dysfunctional parenting led to disruptive behavior inchildhood. Twelve C-SSAGA questions were selected as indicators ofOPS for inclusion in this cluster. Four C-SSAGA questions, as shownin Table I, were selected to form a second cluster based on some ofthe risk factors for child psychopathology proposed by Garmezy andMasten (1994). These consisted of items pertaining to low familyincome, failure of parents to complete a high school education, andmarital breakdown and were generally considered to be an indicatorof family SES. A Cronbach a score was calculated on each of theclusters to determine whether the individual items within the clustershad sufficient internal consistency to allow the formation of a clustersum scale score. Cronbach a scores of .70 for cluster 1 and .60 forcluster 2 indicated that sufficient internal consistency existed, andthe scores for these 2 clusters were subsequently used in the statisticalmodels below. Cluster 1 mean ± SO scores for the NPAA, PAO, andBPAA groups were 1.50 ± 1.8, 2.00 ± 2.1, and 1.80 ± 2.3, respectively. Similarly, cluster 2 mean ± SO scores were 0.14 ± 0.4, 0.80 ±
1.0, and 1.3 ± 1.2 for the respective PT groups.
Statistical Analyses
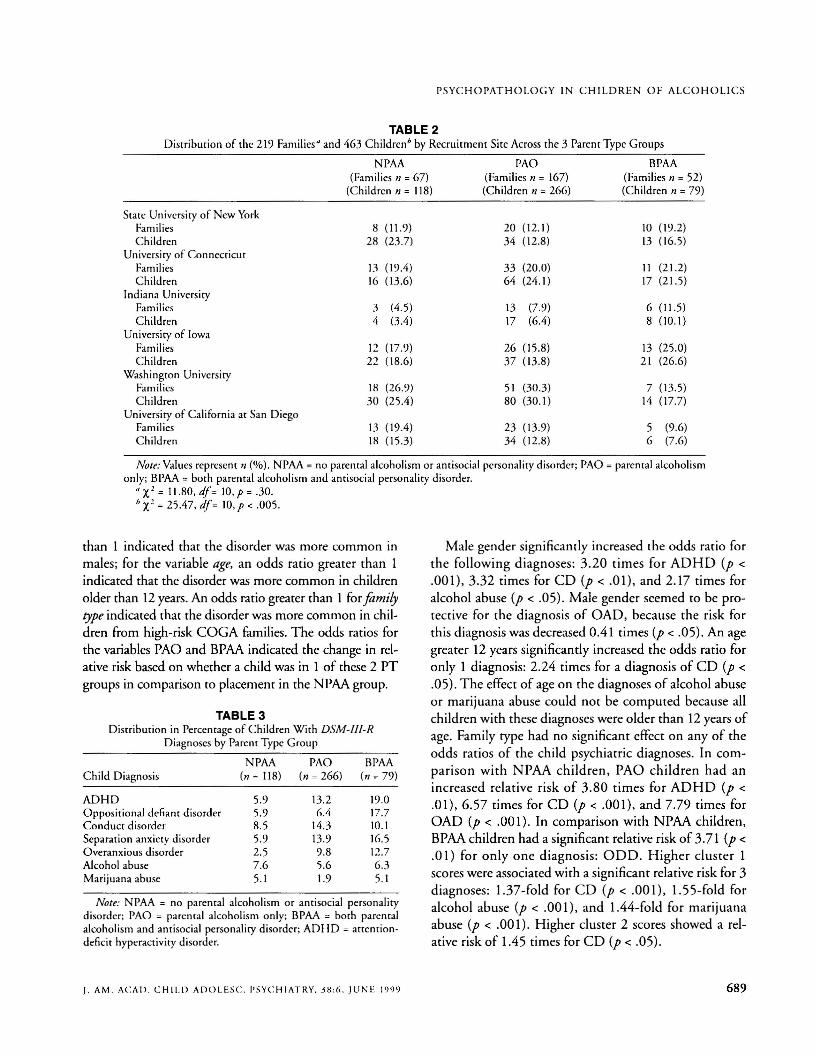
Because COGA families were collected from 6 different sites, itwas possible that the families differed in a variery of ways (ethniciry,education, income, etc.), Unequal contribution of families or childrenfrom the different sites would than have the potential of significantlyinfluencing the data. The distributions of families and children bysite across the 3 different PT groups are shown in Table 2. Preliminarycomparisons indicated no significant differences in the distributionof families by site across the 3 different PT groups. However, the dis-
TABLE 1C-SSAGA Questions That Formed the Basis for Cluster 1
and Cluster 2 Ratings
Cluster 1: Child-Parent Interactions(Cronbach a = .70)
A. Your mother and you do not do things togetherB. Your father and you do not do things togetherC. Your mother does not show that she cares about othersO. Your father does not show that he cares about othersE. Your mother teases you or hurts your feelingsF. Your father teases you or hurts your feelingsG. Your mother frequently criticizes youH. Your father frequently criticizes youI. Your mother does not compliment youJ. Your father does not compliment youK. You do not feel close to your motherL. You do not feel close to your father
Cluster 2: Family Socioeconomic Status(Cronbach a = .60)
A. Lives with only 1 biological parent in the householdB. Family income <$20,OOO/yrC. Mother did not complete high schoolO. Father did not complete high school
Note: C-SSAGA = Child Semi-Structured Assessment for theGenetics of Alcoholism.
688
rriburion of children by site across the 3 PT groups was significantlydifferent (X 2 = 25.47, df= lO,p< .005).
Another potential complicating factor in analyzing the data wasthat on average, each family in the study contributed approximately2 children to the sample. Generalized estimating equations (GEE)modeling was therefore performed to analyze the data because thedata for each child had the potential of not being independent fromthose for other children in the study. The GEE model nested childrenwithin mothers and adjusted for the fact that data from children inthe same family were correlated while examining the effects of independent variables-a child's gender, age (>12 years of age), familyrype (whether the children came from high- or low-risk COGA families), placement in PAO group, placement in BPAA group, cluster 1score, and cluster 2 score---on the dependent variable of a given childpsychiatric diagnosis. Additional independent variables, representingthe effects of recruitment site and recruitment site by PT group interactions, were added to the model based on the uneven distribution ofchildren across sites.The exchangeable working correlation matrix wascalculated in all cases; exchangeable refers to having a value of 1 onthe diagonal and identical off-diagonal elements corresponding to anumber estimated by default in SAS (Proc GenMod). With binarydata, the "Iogit link" function was used corresponding to logisticregression. Goodness of fit was assessed using the measures of scaleddeviance and scaled Pearson X2 provided by the procedure. In allcases the measures were less than I, suggesting a good fit of the model.
The GEE model revealed that of a total possible 35 recruitmentsite and 70 recruitment site by PT group interactions, only 2 significant recruitment site effects were noted (each .04 < P < .05). Thisoccurrence was well below the expected rate of 5 in 100 based on aprobabiliry value of .05. Therefore, the data were reanalyzed with siteand site by PT group interactions eliminated from the GEE model.
RESULTS
Of the 167 families in the PAO group, a family withonly an alcoholic father was the most common means ofentry into this group (60.9%), followed by families whohad 2 alcoholic parents (21.1 %) and families in whichonly the mother had alcoholism (18.0%). Of the 52 families in the BPM group, the distribution of alcoholismamong the parents was similar: only alcoholic fathers(70.9%), 2 parents with alcoholism (24.0%), and onlyalcoholic mothers (5.1%). The distribution pattern ofparental ASPD in this group was also similar: having onlyan ASPD father (91.1%),2 parents with ASPD (6.4%),and only an ASPD mother (2.5%).
As shown in Table 3, the percentage of children withthe disruptive diagnoses of ADHD and ODD increasedwith parental alcoholism and ASPD. The internalizingdiagnoses of SAD and OAD showed a similar patternacross the 3 PT groups. Surprisingly, the diagnoses ofalcohol abuse and marijuana abuse showed no pattern to
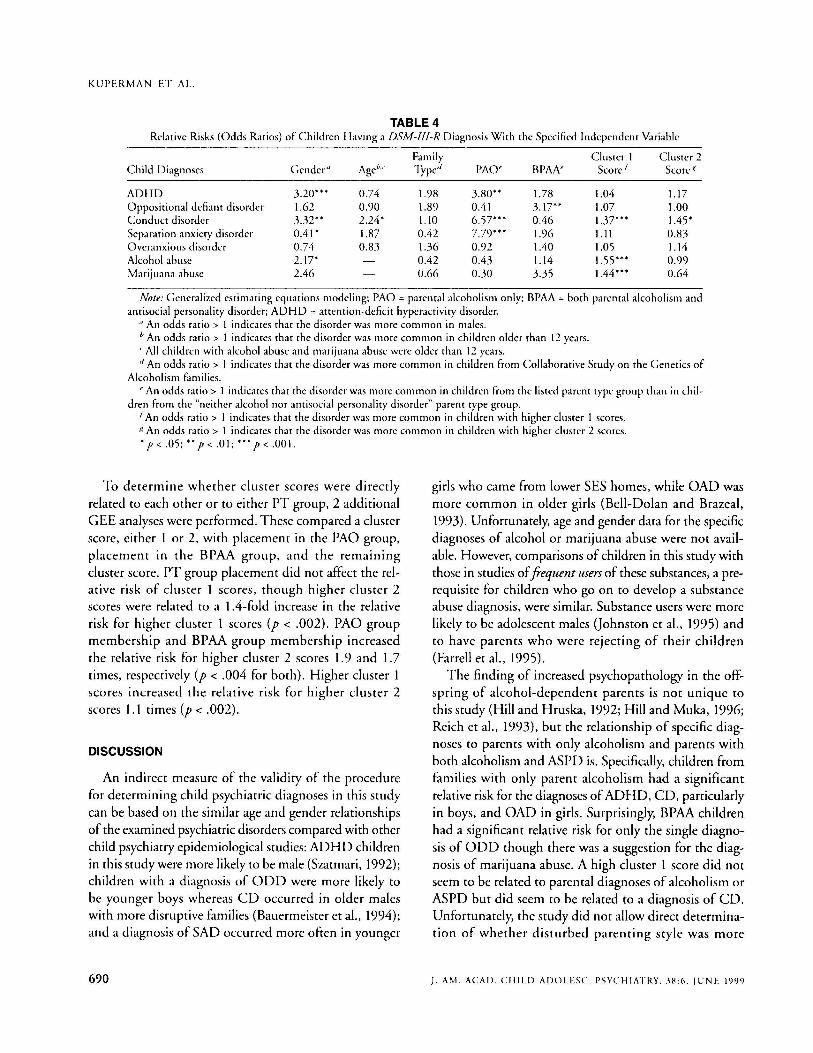
increasing parental alcoholism or ASPD.Table 4 presents the odds ratios and significance levels
for the variables in the GEE model by child psychiatricdiagnosis. For the variable gender, an odds ratio greater
J. AM. ACAD. CHIl.D ADOl.ESC. PSYCHIATRY. j8:6. JUNE 1999
PSYC H O PAT H OLOG Y I N CH I L D REN OF ALCO HO LICS
TABLE 2Distribut ion of the 219 Families" and 463 Children" by Recru itment Site Across the 3 Parent Type Groups
NPAA PAO BPAA(Families n = 67) (Families n = 167) (Families n = 52)
(Childre n n = 118) (C hildren n = 266) (Child ren n = 79)
State University of New YorkFamilies 8 (11.9) 20 (12.1) 10 (19.2)C hildren 21l (23.7) 34 (12.8) 13 (16.5)
University of Co nnecticutFamilies 13 (19.4) 33 (20 .0) 11 (2 1.2)C hild ren 16 (13.6) 64 (24 .1) 17 (21.5)
Ind iana Un iversityFamilies 3 (4.5) 13 (7.9) 6 (11.5)C hildren 4 (3.4) 17 (6.4) 8 (10.1 )
University of IowaFamilies 12 (17.9) 26 (15.8) 13 (25.0)C hildren 22 (18.6) 37 (13.8) 2 1 (26.6)
Washington UniversityFamilies III (26.9) 51 (30.3) 7 (l3.5)C hildren 30 (25.4) 80 (30 .1) 14 (17.7)
University of Ca liforn ia at San DiegoFamilies 13 (19.4) 23 (13.9) 5 (9.6)C hild ren III (15.3) 34 (l2.8) 6 (7.6)
Note: Values represent n (%) . NPAA =no parent al alcoholism or antisocial personality disorder ; PAO =parental alcoholismonly; BPAA =both parental alcoholism and anti social personality disorder.
" X2 = 11.80, df = 10, P = .30.b Xl =25.4 7, df = 10, P < .005 .
than 1 indicated that the disorder was more common inmales; for the variable age, an odds ratio greater than 1indicated that the disorder was more common in childrenolder than 12 years. An odds ratio greater than 1 for familytype ind icated that the disorder was more common in children from high-risk COGA families. T he odds ratios forthe variables PAO and BPAA indicated the change in relative risk based on whether a child was in 1 of these 2 PTgroups in comparison to placement in the NPAA group.
TABLE 3Distributio n in Percentage of Children With DSM -III-R
Diagnoses by Parent Type Gro up
NPAA PAO BPAAC hild Diagnosis (n = 11 8) (n = 266) (n = 79)
ADHD 5.9 13.2 19.0Oppositional defiant d isorder 5.9 6.4 17.7Conduct diso rder 8.5 14.3 10.1Separat ion anxiety disorder 5.9 13.9 16.5O veranxious d isorde r 2.5 9.8 12.7Alcoh ol abuse 7.6 5.6 6.3Marijuana abuse 5. 1 1.9 5.1
Note: N PAA = no parent al alcoholism or ant isocial personalitydisorder; PAO = parent al alcoholism only; BPAA = both parenta lalcoholism and antisoc ial person ality disorder; ADHD = artcnrio ndeficit hyperactivity disorder.
J. AM. ACA D. CHIl. D A D O LESC. PSYC H IAT RY. 38:6 . J UN E 19 99
Male gende r significantly increased the odds ratio forth e follo wing di agn oses: 3.20 times for AOHO (p <
.001) , 3.32 times for CO (p < .0 1), and 2.17 times foralcohol abuse (p < .05). Male gender seemed to be protective for the diagnosis of OAO, because th e risk forthis diagnosis was decreased 0.41 times (p < .05). An agegreater 12 years significantly increased the odds ratio foronly 1 diagnosis: 2.24 times for a diagnosis of CO (p <
.05). The effect of age on the diagnoses of alcohol abuseor mar ijuana abuse could not be computed because allchildren with these diagnoses were older than 12 years ofage. Family type had no significant effect on any of theodds ratios of the ch ild psychiatric diagnoses. In compari son with NPAA child ren, PAO children had anincreased relati ve risk of 3. 80 times for AOHO (p <
.01) ,6.57 times for CD (p < .001), and 7.79 times forOAO (p < .001). In comparison with NPAA children,BPAAchildren had a significant relative risk of 3.7 1 (p <
.0 1) for onl y one d iagnos is: 000. H igher clu ster 1scores were associated with a significant relative risk for 3diagno ses: 1.37-fold for CO (p < .001), 1.5 5-fold foralcohol abuse (p < .001 ), and 1.44-fold for marijuanaabuse (p < .00 1). Higher cluster 2 scores showed a relative risk of 1.45 times for CO (p < .05).
689
KUPERMAN ET AL.
TABLE 4Relative Risks (Odds Ratios) of Children Having a DSM-JlI-R Diagnosis With the Specified Independent Variable
Family Cluster I Cluster 2Child Diagnoses Gender" Age"" Type" PAO' BPAN Score! Score-
ADHD 3.20'" 0.74 1.98 3.80" 1.78 1.04 1.17Oppositional defiant disorder 1.62 0.90 1.89 0.41 3.17" 1.07 1.00Conduct disorder 3.32" 2.24' 1.10 6.57''' 0.46 1.37'" 1.45'Separation anxiety disorder 0.41' 1.87 0.42 7.79'" 1.96 1.11 0.83Overanxious disorder 0.74 0.83 1.36 0.92 1.40 1.05 1.14Alcohol abuse 2.17' 0.42 0.43 1.14 1.55'" 0.99Marijuana abuse 2.46 0.66 0.30 3.35 1.44'" 0.64
Note: Generalized estimating equations modeling; PAO = parental alcoholism only; BPAA = both parental alcoholism andantisocial personality disorder: ADHD = attention-deficit hyperactivity disorder.
.t An odds ratio> I indicates that the disorder was more common in males./,An odds ratio> 1 indicates that the disorder was more common in children older than 12 years.. All children with alcohol abuse and marijuana abuse were older than 12 years.d An odds ratio> I indicates that the disorder was more common in children from Collaborative Study on the Genetics of
Alcoholism families., An odds ratio> 1 indicates that the disorder was more common in children from the listed parent type group than in chil-
dren from the "neither alcohol nor antisocial personality disorder" parent type group.IAn odds ratio> 1 indicates that the disorder was more common in children with higher cluster 1 scores.g An odds ratio> I indicates that the disorder was more common in children with higher cluster 2 scores.'p < .05;" P < .01; .. , P < .001.
To determine whether cluster scores were directlyrelated to each other or to either PT group, 2 additionalGEE analyses were performed. These compared a clusterscore, either 1 or 2, with placement in the PAO group,placement in the BPAA group, and the remainingcluster score. PT group placement did not affect the relative risk of cluster 1 scores, though higher cluster 2
scores were related to a lA-fold increase in the relativerisk for higher cluster 1 scores (p < .002). PAO groupmembership and BPAA group membership increasedthe relative risk for higher cluster 2 scores 1.9 and 1.7times, respectively (p < .004 for both). Higher cluster 1scores increased the relative risk for higher cluster 2scores 1.1 times (p < .002).
DISCUSSION
An indirect measure of the validity of the procedurefor determining child psychiatric diagnoses in this studycan be based on the similar age and gender relationshipsof the examined psychiatric disorders compared with otherchild psychiatry epidemiological studies: ADHD childrenin this study were more likely to be male (Szarrnari, 1992);children with a diagnosis of ODD were more likely tobe younger boys whereas CD occurred in older maleswith more disruptive families (Bauermeister et al., 1994);and a diagnosis of SAD occurred more often in younger
690
girls who came from lower SES homes, while OAD wasmore common in older girls (Bell-Dolan and Brazeal,1993). Unfortunately, age and gender data for the specificdiagnoses of alcohol or marijuana abuse were not available. However, comparisons of children in this study withthose in studies offrequent users of these substances, a prerequisite for children who go on to develop a substanceabuse diagnosis, were similar. Substance users were morelikely to be adolescent males (johnston et al., 1995) andto have parents who were rejecting of their children(Farrell et al., 1995).
The finding of increased psychopathology in the offspring of alcohol-dependent parents is not unique to
this study (Hill and Hruska, 1992; Hill and Muka, 1996;Reich et al., 1993), but the relationship of specific diagnoses to parents with only alcoholism and parents withboth alcoholism and ASPD is. Specifically, children fromfamilies with only parent alcoholism had a significantrelative risk for the diagnoses ofADHD, CD, particularlyin boys, and OAD in girls. Surprisingly, BPAA childrenhad a significant relative risk for only the single diagnosis of ODD though there was a suggestion for the diagnosis of marijuana abuse. A high cluster 1 score did notseem to be related to parental diagnoses of alcoholism orASPD but did seem to be related to a diagnosis of CD.Unfortunately, the study did not allow direct determination of whether disturbed parenting style was more
I. AM ACAIl. CHILIl AIlOLESc:. PSYCHIATRY, .~H:('. JLJNE 1999

likely to lead to a diagnosis of CD or whether a diagnosis of CD was more likely to lead to disturbed parenting.
Unexpectedly, there were 2 "relationships" in this studythat were nonsignificant: the relationship between aparental diagnosis of alcoholism and a childhood diagnosis of alcohol abuse, and between a parental diagnosisof ASPD and a childhood diagnosis of CD. The lack ofa significant relationship for both of these may be due to
the relatively young age of the children in this study.Overall, the average age of 12.1 ± 3.3 years for the children in the study who had an alcoholic parentts) was significantly younger than the averageage of 14.2 ± 3.0 yearsfor the children whose parents did not have this diagnosis (T= 6.31, df= 223.3,p < .0001). Both of these ageswere well below the late-adolescent to early-adulthoodyears more commonly associated with the onset of alcohol abuse or dependence (Goodwin, 1985);(Schuckit,1982). Additional support for this hypothesis was thefinding that the diagnosis of alcohol abuse was givenonly to older children in this study; the average age ofthe 29 children with this diagnosis was 16.6 ± 1.0 years.Therefore, it is possible that as the children with alcoholic parents grow older they will themselves developincreasing problems with alcoholism. Similarly, the average age of the 79 children with an ASPD parentis) was12.2 ± 3.2 years, which was somewhat young for a diagnosis of CD. Combining the number of children withODD (the possible child precursor of adolescent CD)with the number of children with CD produced a rate of27.8% of the children with an ASPD parentfs) (BPAAchildren) versus 14.4% in NPAA and 20.7% in PAOchildren. These rates were in the direction that suggesteda relationship to parental ASPD.
A strength of this study is that it has improved uponsome of the methodological difficulties found in earlystudies. Families were not selected on the basis of directparental involvement in alcohol treatment programs oron the basis of children being followed in psychiatryclinics; the study is therefore more representative ofalcohol-dependent parents and families in the generalpopulation. Appropriate statistical methods were used to
allow the inclusion of multiple siblings from a givenfamily so that appropriate inferences could be made onthe contribution of familial data, in addition to that ofparental diagnoses of alcoholism and ASPD, to childpsychopathology. Finally, the sample size was larger thanin previous studies and increased the statistical power ofthe analyses.
J. AM. ACAD. CHIl.D ADOl.ESC. PSYCHIATRY, .\8:6, JUNE 1999
PSYCHOPATHOLOGY IN CHILDREN OF ALCOHOLICS
However, limitations exist for this study. First, althoughthere were minimal site differences in the rates of 2 diagnoses, recruitment site differences in rates of psychopathology have been reported in other multisite studies suchas the Epidemiologic Catchment Area and the DepressionCollaborative studies (Coryell et al., 1981; Weissmanet al., 1988). The minimal differences in rates in the current study were felt to be due to chance and not to procedural differences because of standardized instruments andinterviewer training. Second, all comorbid parental diagnoses were not considered. This was an intentional decision because differentiation of children based on multiplecombinations of parental diagnosis would greatly decreasethe number of children in each PT group, thus reducingstatistical power. Third, the study design did not allowexamination of actual genetic transmission of specificDSM-III-R diagnoses among the COAs. Therefore, findings can be interpreted as only familial in nature, neitherpurely genetic nor environmental. Finally, although anattempt was made to account for the factors of DPS andfamily SES, the literature in this area is still incompleteand the effect of additional individual items or clusters ofsymptoms is unknown.
Clinical Implications
Children from familieswith an alcohol-dependent parent (or parents) were at increased risk for several psychiatric diagnoses includingADHD, CD, and OAD. BPAAchildren were at increased risk for the single diagnosis ofODD, though it is likely they were at increased risk forthe spectrum of child/adolescent equivalents of ASPD,i.e., ODD in children and CD in adolescents.The risk foralcohol abuse was not greater in the offspring of these parents, although this likely was the result of the relativelyyoung age of the examined offspring. Familial and SEScharacteristics had an additive effect to parental diagnoseson the risk of some childhood diagnoses but overall contributed less to this risk than did parental diagnoses.
The observed increased risk for the offspring of alcoholdependent and ASPD parents developing a child psychiatric disorder was familial in nature and included the potential of genetic predisposition as well as the possibility ofother environmental interactions that were not measuredby this study. This finding may lead to the hypothesis thatthe etiology of the child psychiatric diagnoses discussedabove may be different from that of those occurring inchildren whose parents do not have alcohol dependence orASPD or in parents who have the same psychiatricdiagno-
691

KUP E RM A N ET A I..
sis as their offspring (e.g., a parent has a diagnosis ofADHD and his or her child has the same diagnosis).
T he study raises several treatm ent issues: Will the successful treatment of parental alcoho lism lower the risk(or recurrent risk) of a psychiatri c disorder in the offspring? Will the successful treatment of a child with apsychiatr ic disorder who has a parenrts) with alcoholismlower that child's risk of develop ing alcoholism as he/sheapproaches the typ ical age of risk? Is the successful treatment of a child with a psychiatric disorder who has parent s with alcoholism similar to the treatment of a childwith a psychiatric disorder whose parents do not havealcoholism?The ongoing COGA study has the potentialto provide the opportunity to periodically reexamine thechild ren over time and, in a naturalistic way, to determine the outcome of several of these questions.
Collaboratioe Study 0 11 thr Generics ofAicoho lism: H. Begleiter. SVNY.Principal tn restigm or. 7: Reich, W,ubillg toll University. Co-PrincipalIIll'migator. The 6 sitrs an d Principal bll't'stigaton and Co- ln oestigators are
Indiana Uniuersit y (j. Num hugrr. [r., T.-K. Li. PM. Co11nrally ,H. Edmhrrg); Uniuersiry of louia (R. Crou'r, S. Kuperman); University ofCitliJom itl Stili Dirgo and Th « Scripps Rrsearch Institute (M . Sch ucla t.
r: Bloom ); Uniurrsiry 0/ Connrcticut ( V, Hrssrlbrock): SVNY HSCH(H. Brglrita. H. Porjesz): and Wasbillgloll University ill St. Louis ( T. Rricb.C.R. Clol/illgt'r,j. Rice). This national collaborative sw dy is supported by theNational Institutr 0 11 Alcohol Ab use and Alcoholism (N 1AAA) by U.S.Public Health Seruic« grtl1JtS N 1AAA U IOAA 0840 1. UIOAA08402. andV IOAA 08403.
REFERENCES
Bauermeister jJ, Canine C, Bird H (1')') 4) , Epide m iology of disruptive beh avio t d isorders. In: Disruptiue Disorders. Cteenhill LL, ed. Philadelphia:Sau nders, PI' 177-1')4
Bell-Dolan D, Brazeal TJ (1') ')3). Separation anxie ty disorder, overan xiousdiso rder, and schoo l refusal. In : Anxietv Disorders, Leonard H L. cd .Phi ladelp hi a: Saunders. 1'1' 'i(,j - 'i78 .
Bird H R. Could MS . Sraghczz» B ( 1') ')2). Aggrega ting d ata from mult iplein fo rm anrs ill child psychiat ry epidemiological research . ] Am Acad ChildAdolrsc Psychiatry 3 1:78-85
Bucholz KK. 'C,dor~t R. Cloninger C R er al. (1')') 4 ). A new. semi-structuredpsychiatric in terview for usc in gen et ic linkage stud ies: a repon on thereliabi lity of rhc SSAC;A.] Stud Alcohol 55 : 14')-1 58
C on nolly CM. Casswell S, Stewart J. Silva PA. O ' Brien M K ( 1') ')3). T heetTen nf parents alco ho l problems on chil d ren's beh aviour as reported byparel1ls and by teac hers . Addiction 88 : U83-1390
C oryell W. Wi no kur C. Andreasen N C (198 1). Ellec t of case de fini t ion onalle ctive di sorde r rates. Am] Psvchiatrv U8 :1106 - 1109
Earls 1'. Reich W. Jung KG , C lon i,;g<'r Cll. ( 1')88). Psychopatho logy in child ren of alcoh ol ic an d antisocial parent s. Alcohol Cli» £\1' R" 12:48 1- 487
692
Farrell M P, Barnes GM, Baner jee S ( I')')S). Family cohesion as a buffe r againstthe effec ts of pro blem- d rinki ng fathers on psych ological dist ress. deviantbehavior. and heavy d rinki ng in ado lescent s.J Health SocBehau36:377-385
Feigh ner J p, Robins E, G UI.e SB. Woodruff RA. W ino kur G . Mu nos R (1972 ).D iagnostic criteria fo r use in psychi atri c research . Arch Gen Psychiatry26 :S7-63
Fergusson D M , Lynskey MT, Horwood l.J (1994 ). C hi ld hoo d exposu re toalco hol and ado lescent d rink ing patterns. Addiction 89 :1007-10 16
Garmezy N , Mas ten AS (199 4) . C hro nic adve rsities . In: Child and AdolescentPsychiatry: ModernApproaclm. Rut ter M. Taylo r E. He rsov L. eds. London :Blackwell Scientific Publicat ions. PI' 191-208
(;oodwi n D W (1985), Alcoho lism and genet ics: the sins of the fathers . ArchGm Psychiatry 42 :17 1-174
Goodwi n DW, Schulsinger F, Hermansen l., G uzc SB. W inoku r G (1975 ).Alco ho lism and th e hype rac t ive chil d sy nd ro m e. J Nail Menr Dis160:349-353
H ill SY, C lo ninger CR, Ayre FR (1977). Ind ependent familial tran sm issionof alcoholism and opiate abuse. Alcohol Clin F..xp Res 1:335-342
Hi ll SY. Hruska DR (1992 ). C hild hood psychopathology in famil ies withrnulr igenerarional alc o h o lism. JA m Acad Child Adolrsc Psychiatry31: 1024 - 1030
Hi ll SY. Muka D (1996). C hild hood psychopathology in ch ildre n fro m families of alco holic fema le probands. J Am Acad Child Adolrsc PsychiatryJ5:725-7.B
joh nsron LD , O 'Ma lley PM . Bachman J G (199S) . National Sltrl't'JResult: onDrug UseFromMonitoring thr filfllrt'SlUdy. 1975-1992. Vol I: SecondarySchool St udents. Rockvi lle. MD: Narional Inst irute on Drug Abuse
Mcri kangas KR. Weissman MM. Prusoff BA. Pauls DL . Leckm an J F (1985).Depressives with secon dar y alco holism: psychiat ric disord ers in offspring .l Slltd Alcohol At»: 199-204
Patterso n G R, Debaryshe BD . Ram sey E (1')89 ). A developmental pe rspec tive on antisocia l behavior. Am PsychoI 44:.U9-335
Patterson G R. Srourharner-Loeber M (1984). T he co rrela tio n of family ma nagemc nt practi ces and delinquency. Child Deu 55 :1299-1307
Reich W, Earls F. Frankel O. Shay ka JJ (1993), Psychopathology in childr enof alco ho lie.s.] Am AcadChild Adolesc Psychiatry 32:')95-1002
Reich W. Her jan ic B, Weiner Z . Gandhy pR (198 2) . De velopment of a structured psychiat ric interview for child ren: agree ment on d iagnosis co mparing child and parent in terviews. J Ab norm Child P~ychollO :3 2 5-.B6
Roosa M W. Sandler IN. Beals J. Sho rt J L (1988). Risk sta tus o f adolescentchi ldren of problem-dr inkin g parents . Am ] Commu nity Psycho/ 16:225-23')
Schuckit MA (1982 ). A study of you ng men wi th alcohol ic close relat ives.Am] Psychiatry 139:79 1- 794
Shaffer D. Fisher P. Dulcan MK et al. ( 1')96) . The NIMH Diagnosti c int erview Schedule lor Children Version 2.3 (D1SC- 2 .3): description. acceptability. prevalence rates. and perfor man ce in the MECA study.] Am AcadChild Adolesc Psychiatry 35:865-877
Srcinhauscn He, G obel D . Nestler V (1984). Psychopathology in the offspring of alcoholic pa rents.] Am Acad Child Psychiatry 23:465- 471
Stewart MA , DeBl ois CS . Cum m ings C (1980) . Psych iatr ic di sord er in thepa rents o f hyperactive boys and those wi th co nd uct di sord er. ] ChildPSY"ho! Psychi,ury 2 1:283- 292
Szatrnari I' (1992). The epi demiology of attention d eficit hyper act ivity d isor der. In: Attrntion-Deficit Hyperaa iuity Disorder; Weis G . cd . Ph iladel ph ia:Saunders . 1'1' .~6 1-384
Tub man JG ( 1993), A pilot study of school-age chi ld ren of m en wi th m odcrate to severe alcoho l depend ence: materna l distress and child out co mes .J Child Psycho! Psychiatry 34:729- 741
Weissma n MM, Leaf P] , T ischler G L et al, (1988 ). Affective d isord ers in fiveUni ted Sta tes co m m u nit ies. Psycho! Med /8:141-1 53
West M O . Pri nz RJ (1987 ), Parent al alcoholis m and ch ild hood psych opat ho logy, Psycho! Bull 102:20 4 -218
J , AM. ACAD. CHIl.D ALJ O l. ESC . PSYCH IAT RY, .18:6, JUN E 199 9