Embed Size (px)
DESCRIPTION
Relationships that Heal. William R. Miller, Ph.D. The University of New Mexico The Eileen Pencer Memorial Lecture. What’s Missing in EBTs?. Have you noticed: that in multisite clinical trials (like CTN) of treatments that are already evidence-based - PowerPoint PPT Presentation
Citation preview
William R. Miller, Ph.D.
The University of New Mexico
The Eileen Pencer Memorial Lecture
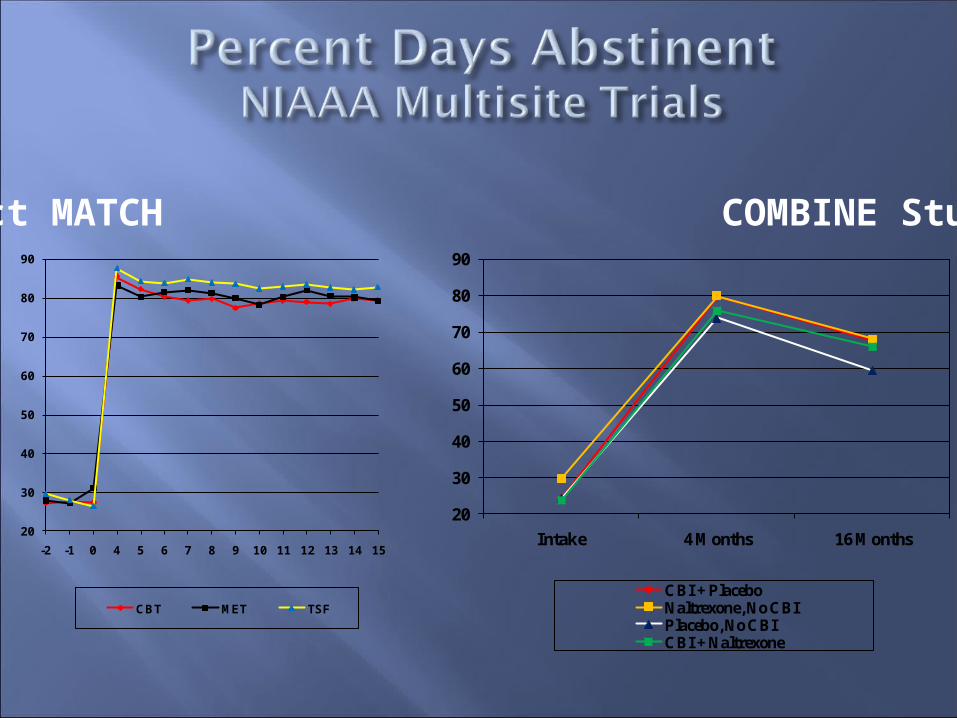
Have you noticed:that in multisite clinical trials (like CTN)of treatments that are already evidence-basedeven under highly controlled, supervised,
manual guided delivery conditionsthe expected main effects are often quite small?and that efficacy often varies by therapist and by
site? This even happens with
pharmacotherapies In practice, EBTs are not homogeneous
entities
20
30
40
50
60
70
80
90
Intake 4 Months 16 Months
CBI + PlaceboNaltrexone, No CBIPlacebo, No CBICBI + Naltrexone
20
30
40
50
60
70
80
90
-2 -1 0 4 5 6 7 8 9 10 11 12 13 14 15
CBT MET TSF
Project MATCH COMBINE Study
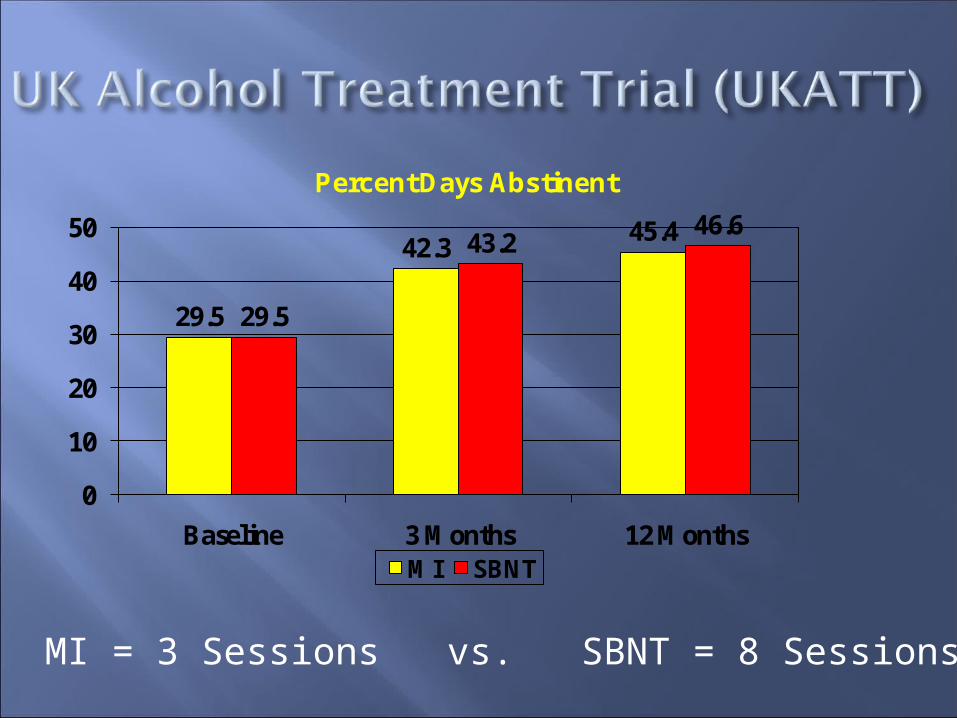
29.5
42.345.4
29.5
43.246.6
0
10
20
30
40
50
Baseline 3 Months 12 MonthsMI SBNT
Percent Days Abstinent
MI = 3 Sessions vs. SBNT = 8 Sessions
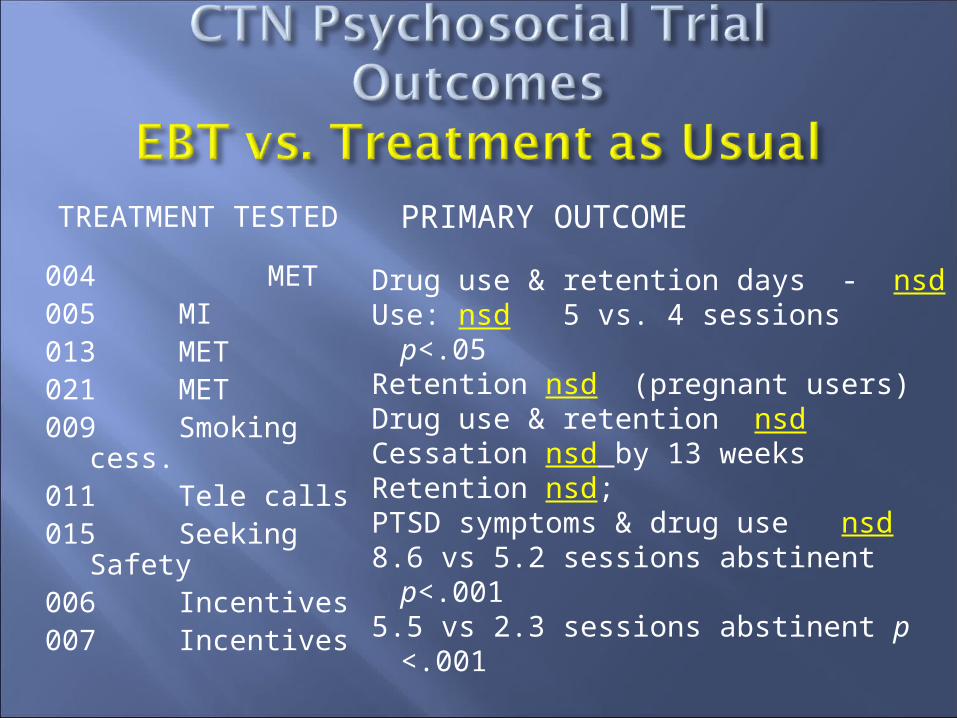
TREATMENT TESTED
004 MET005 MI013 MET 021 MET009 Smoking cess.011 Tele calls015 Seeking Safety006 Incentives007 Incentives
PRIMARY OUTCOME
Drug use & retention days - nsdUse: nsd 5 vs. 4 sessions p<.05Retention nsd (pregnant users)Drug use & retention nsdCessation nsd by 13 weeksRetention nsd; PTSD symptoms & drug use nsd8.6 vs 5.2 sessions abstinent
p<.0015.5 vs 2.3 sessions abstinent p
<.001
The specific effect size for manual-guided EBT is typically small
Even small effects may be clinically meaningful
With large multisite samples, statistical significance can be found for small effects, but do clinicians care?
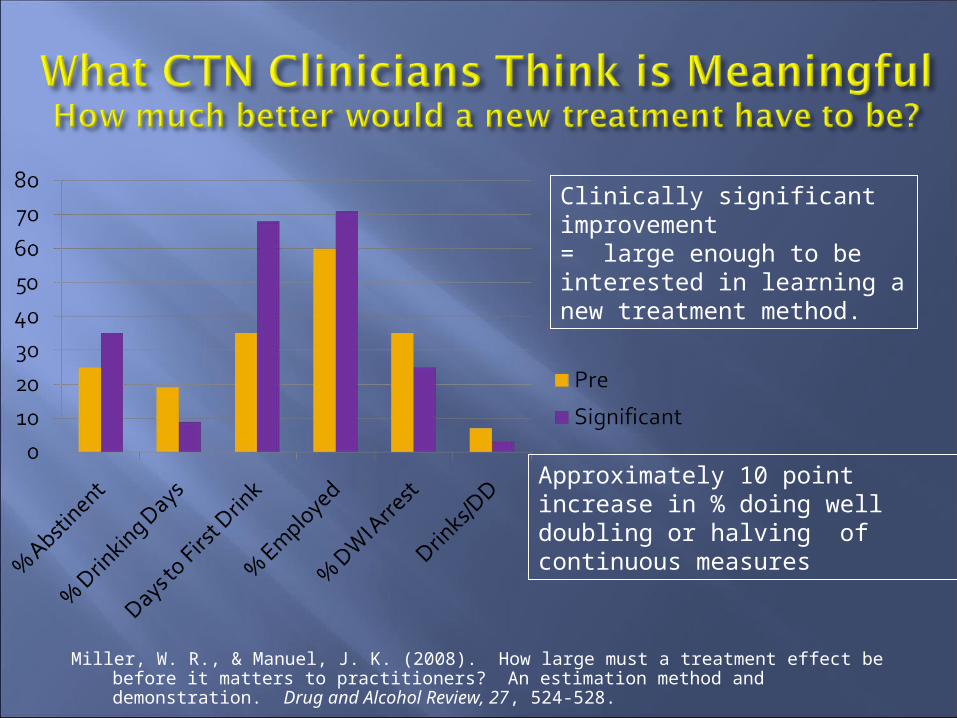
Miller, W. R., & Manuel, J. K. (2008). How large must a treatment effect be before it matters to practitioners? An estimation method and demonstration. Drug and Alcohol Review, 27, 524-528.
Clinically significant improvement= large enough to be interested in learning a new treatment method.
Approximately 10 pointincrease in % doing well ordoubling or halving ofcontinuous measures

Learning More from Clinical Trials
In practice, there is.In practice, there is.
In practice, evidence-based treatments are not homogeneous entities

Where are the bigger effects?
So
0
10
20
30
40
50
60
70
80
90
100
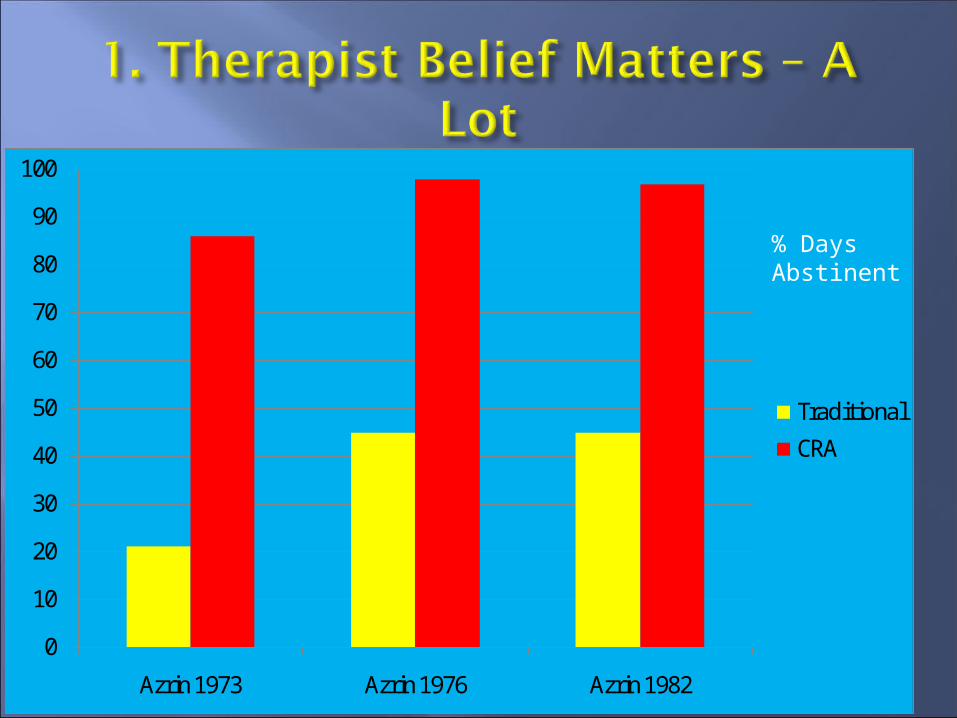
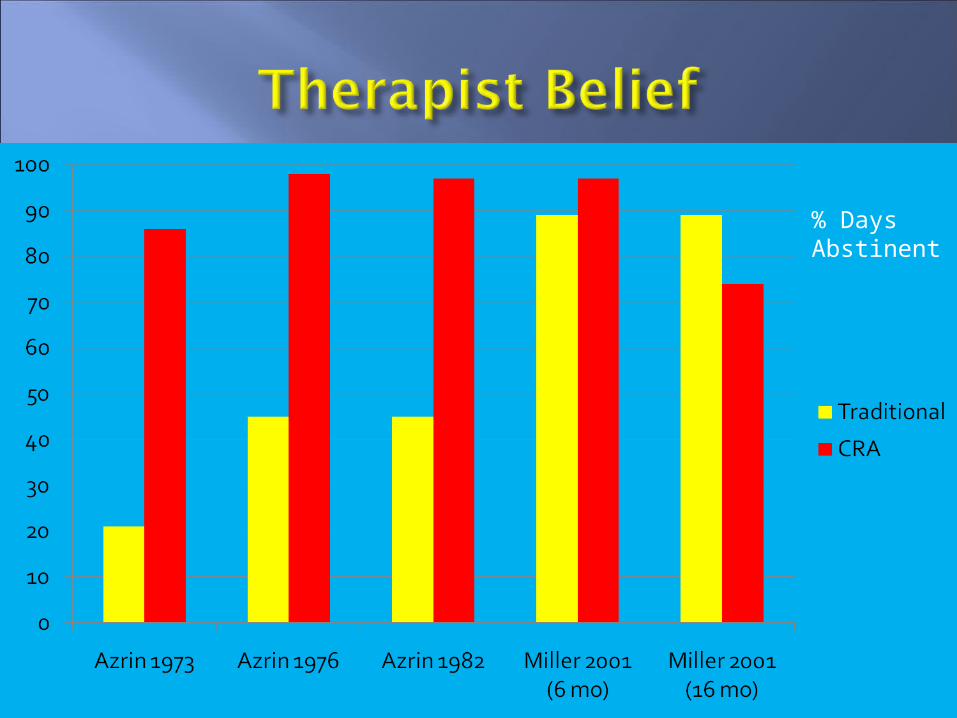
Azrin 1973 Azrin 1976 Azrin 1982
Traditional
CRA
% DaysAbstinent
% DaysAbstinent
Psychologists tested patients in three different treatment programs
They identified patients with particularly high alcoholism recovery potential (HARP)
HARP vs. non-HARP patients did not differ from each other on prior treatment history or severity of alcoholism
More motivated for counseling More punctual in meeting
appointments Showing greater self-control Neater and more attractive in
appearance More cooperative Trying harder to stay sober Showing better recovery
Higher rates of abstinence Longer spans of abstinence Fewer slips More employment
“HARPs” had been selected at random.

Counselor expectations matter a lot.
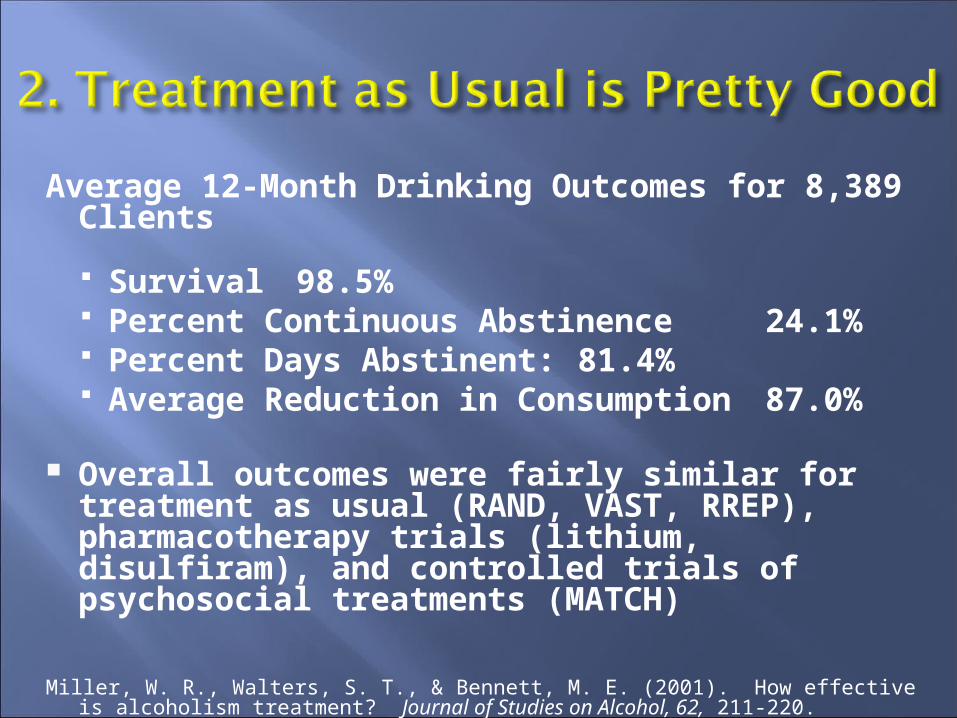
Average 12-Month Drinking Outcomes for 8,389 Clients
Survival 98.5% Percent Continuous Abstinence
24.1% Percent Days Abstinent: 81.4% Average Reduction in Consumption 87.0%
Overall outcomes were fairly similar for treatment as usual (RAND, VAST, RREP), pharmacotherapy trials (lithium, disulfiram), and controlled trials of psychosocial treatments (MATCH)
Miller, W. R., Walters, S. T., & Bennett, M. E. (2001). How effective is alcoholism treatment? Journal of Studies on Alcohol, 62, 211-220.
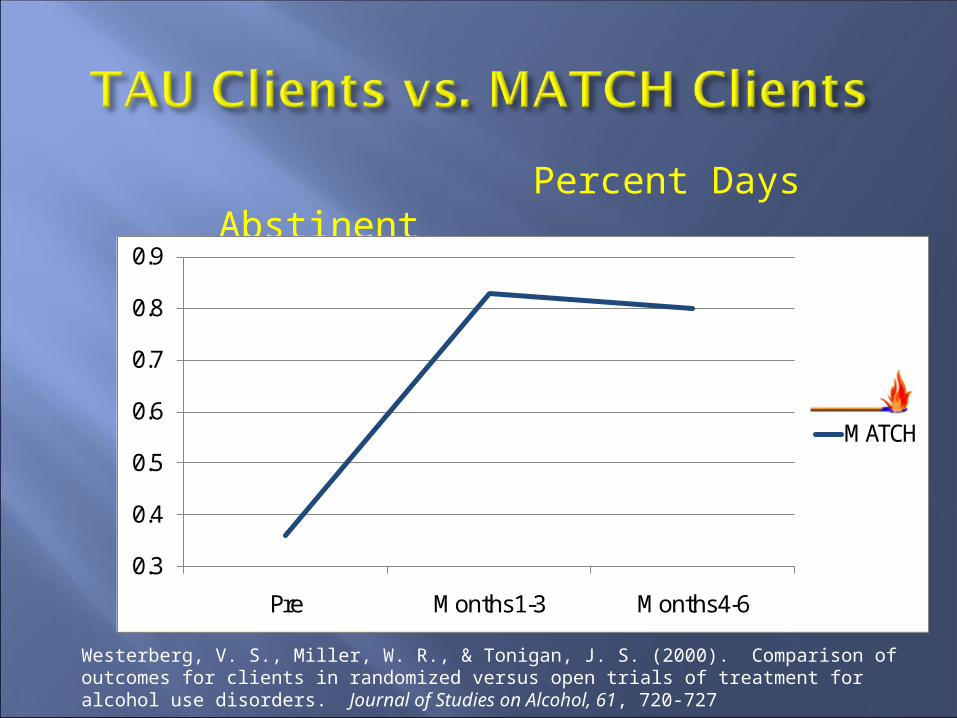
Percent Days Abstinent
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Pre Months 1-3 Months 4-6
MATCH
Westerberg, V. S., Miller, W. R., & Tonigan, J. S. (2000). Comparison of outcomes for clients in randomized versus open trials of treatment for alcohol use disorders. Journal of Studies on Alcohol, 61, 720-727
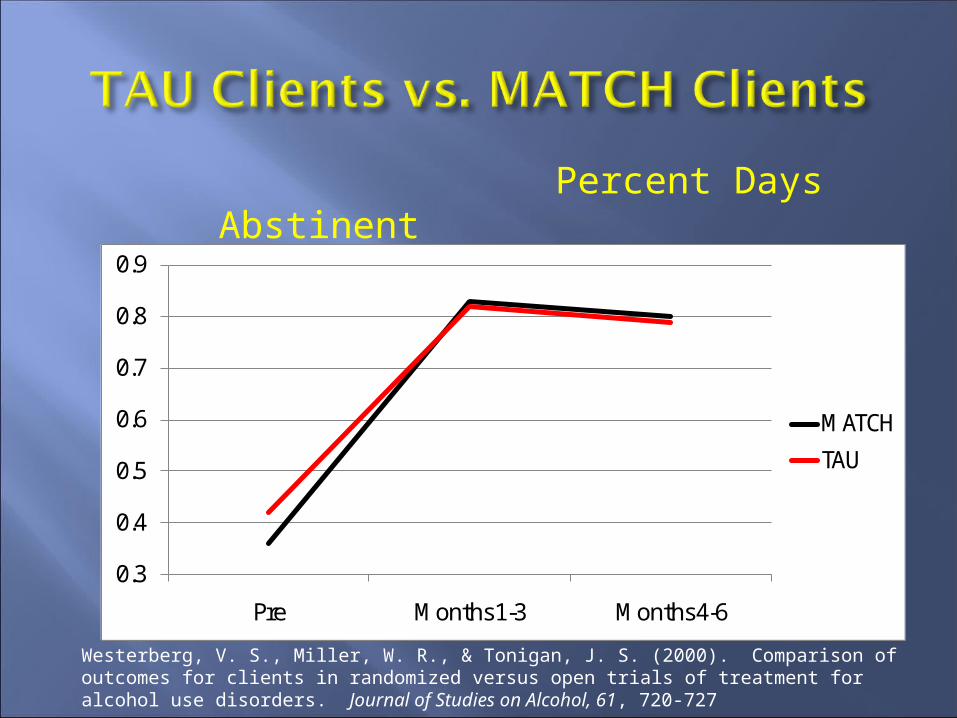
Percent Days Abstinent
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Pre Months 1-3 Months 4-6
MATCH
TAU
Westerberg, V. S., Miller, W. R., & Tonigan, J. S. (2000). Comparison of outcomes for clients in randomized versus open trials of treatment for alcohol use disorders. Journal of Studies on Alcohol, 61, 720-727
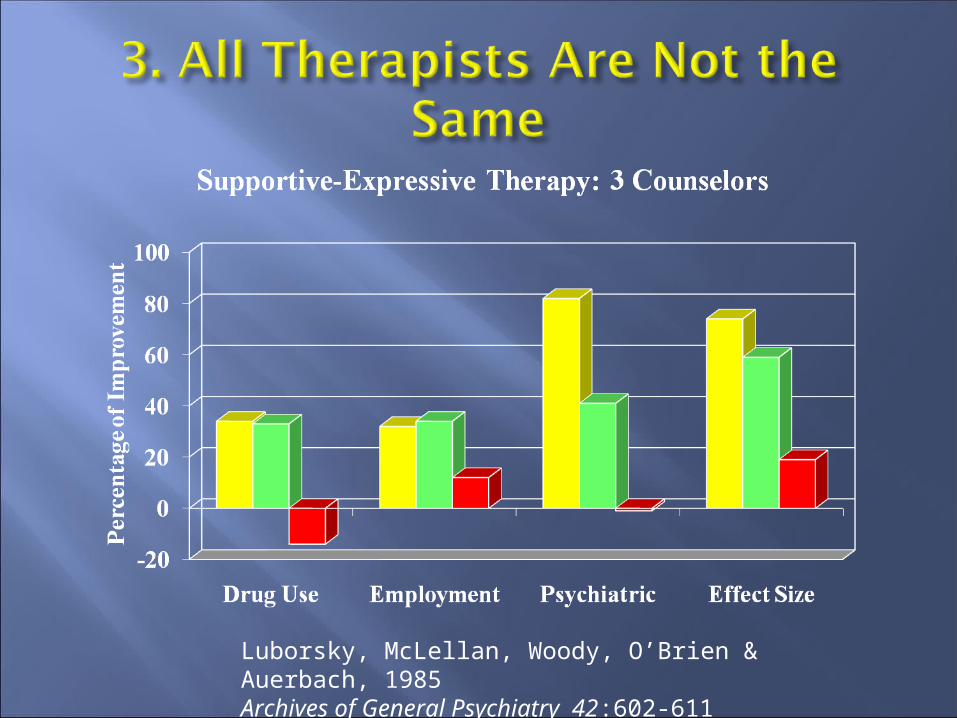
Luborsky, McLellan, Woody, O’Brien & Auerbach, 1985 Archives of General Psychiatry 42:602-611
Two drug treatment counselors resigned
Their 62 cases were assigned randomly to the four remaining counselors
There were dramatic differences in client outcomes.
McLellan et al., 1988 Journal of Nervous and Mental Disease, 176, 423-430.
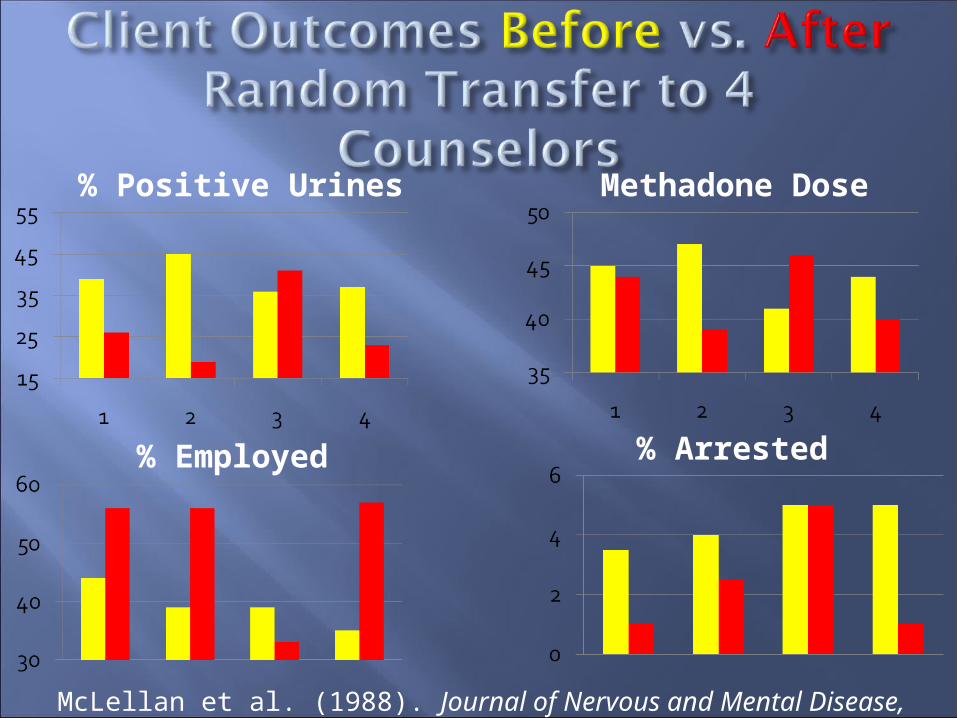
% Positive Urines Methadone Dose
% Employed % Arrested
McLellan et al. (1988). Journal of Nervous and Mental Disease, 176, 423-430.
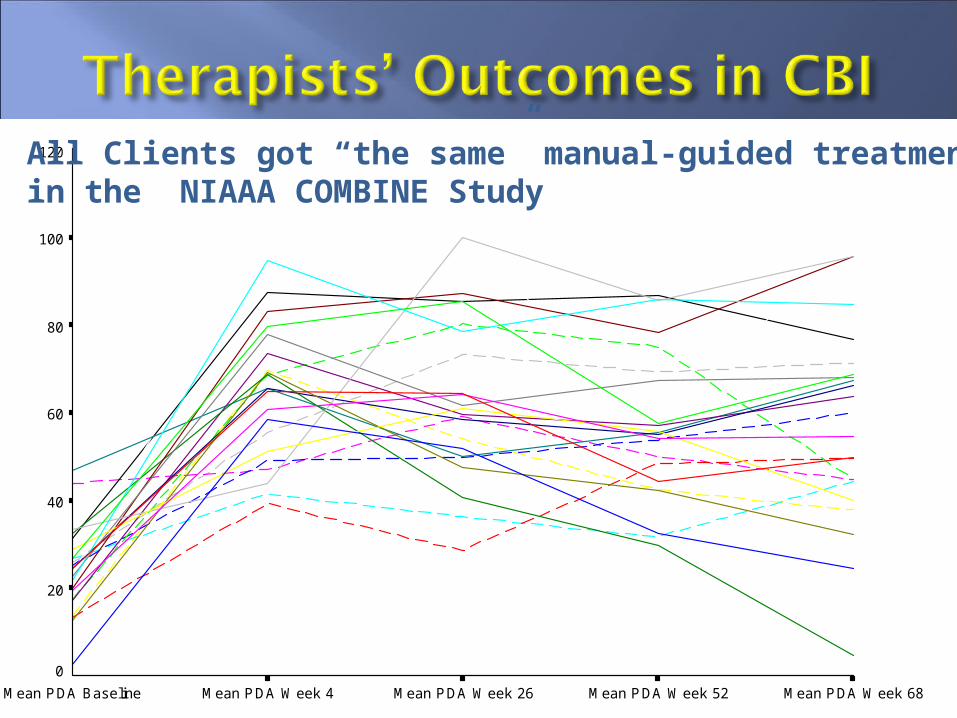
Mean PDA Week 68Mean PDA Week 52Mean PDA Week 26Mean PDA Week 4Mean PDA Baseline
120
100
80
60
40
20
0
All Clients got “the same” manual-guided treatmentin the NIAAA COMBINE Study
Much emphasis is given to “common factors” as an alternative to EBTs
So-called “common factors” may or may not be all that common in practice
If they do exert a large effect, they should not be hard to observe
“Nonspecific” just means that they have not yet been adequately specified and tested
So why not both . . and?
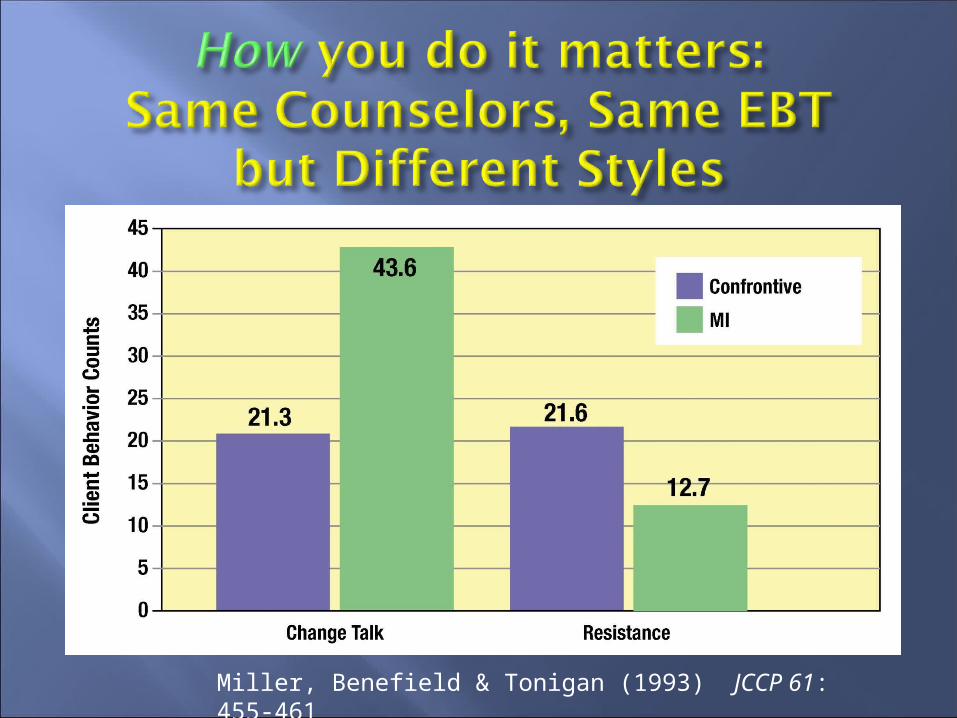
Miller, Benefield & Tonigan (1993) JCCP 61: 455-461
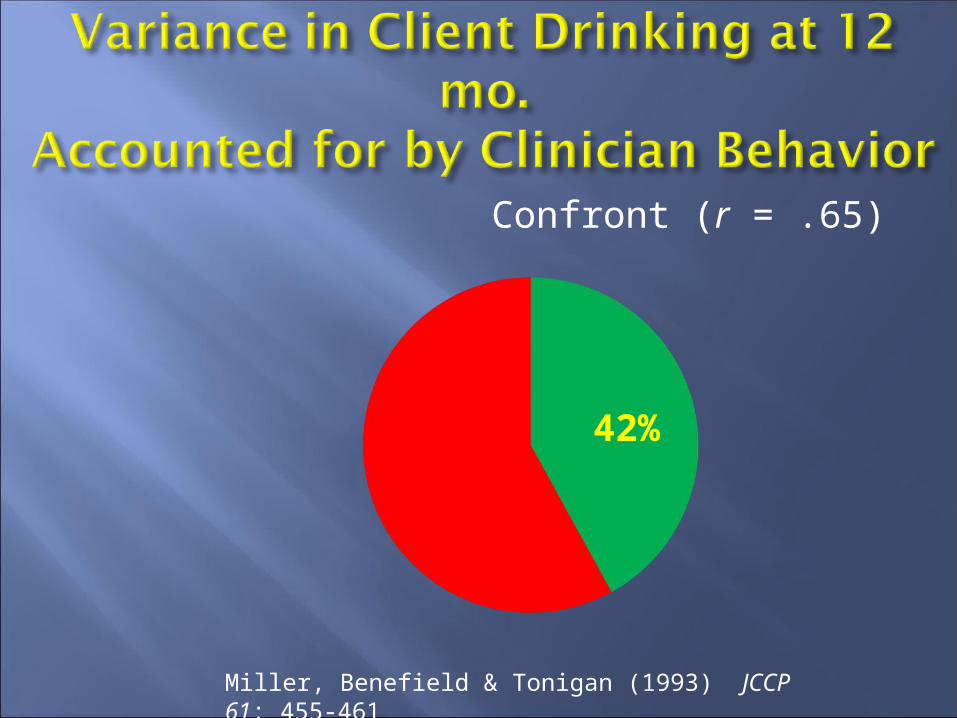
Confront (r = .65)
Miller, Benefield & Tonigan (1993) JCCP 61: 455-461
42%
Accurate empathy is a well-specified, learnable, reliably measurable therapist skill – the ability to understand and reflect clients’ meaning
Originally defined and studied by Carl Rogers
It is not identification with your client
Were delivering the same manual-guided behavior therapy (self-control training)
Were trained both in behavior therapy and accurate empathy
Had sessions independently observed and rated by three supervisors, including the Truax & Carkhuff scale for accurate empathy
Were then rank-ordered (1-9) for empathic skill while delivering behavior therapy
And when we examined 6-month client outcomes . . . .
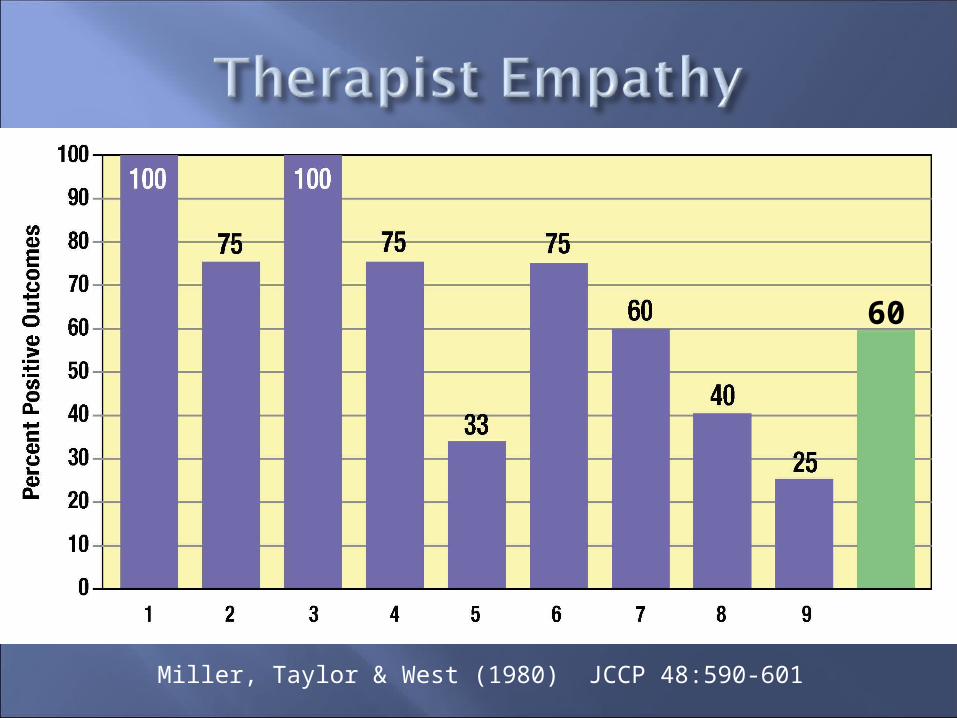
Miller, Taylor & West (1980) JCCP 48:590-601
60
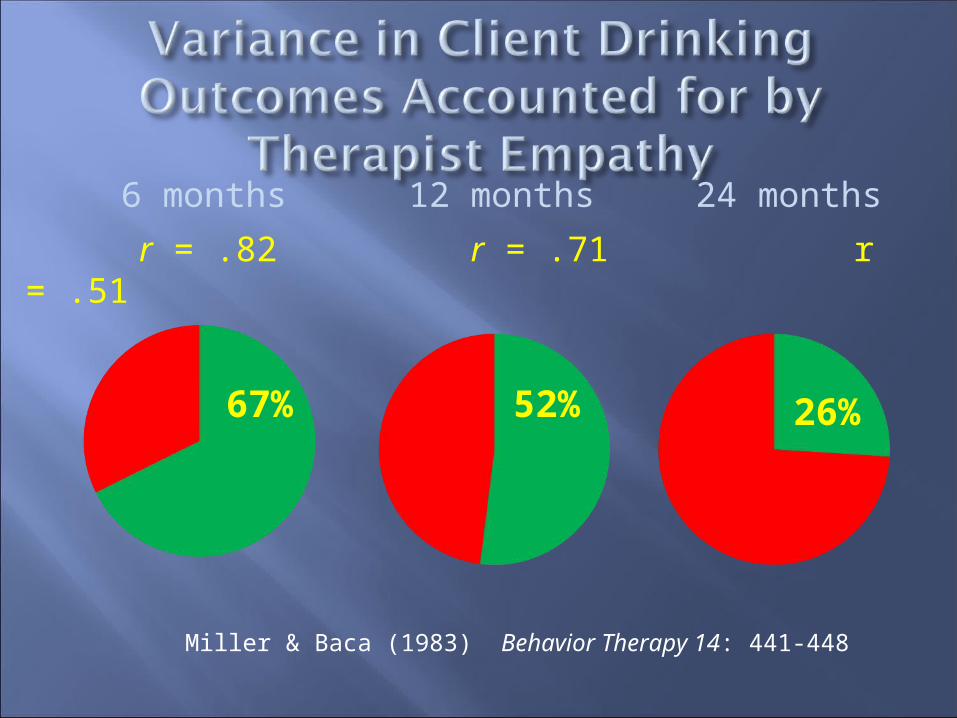
6 months 12 months 24 months
r = .82 r = .71 r = .51
Miller & Baca (1983) Behavior Therapy 14: 441-448
67% 52% 26%
Patients in treatment for alcoholism were randomly assigned to counselors with:
LOW levels of empathy and related skillsMEDIUM levels of empathy and related
skillsor HIGH levels of empathy and related skills
What percentage of patients relapsed?
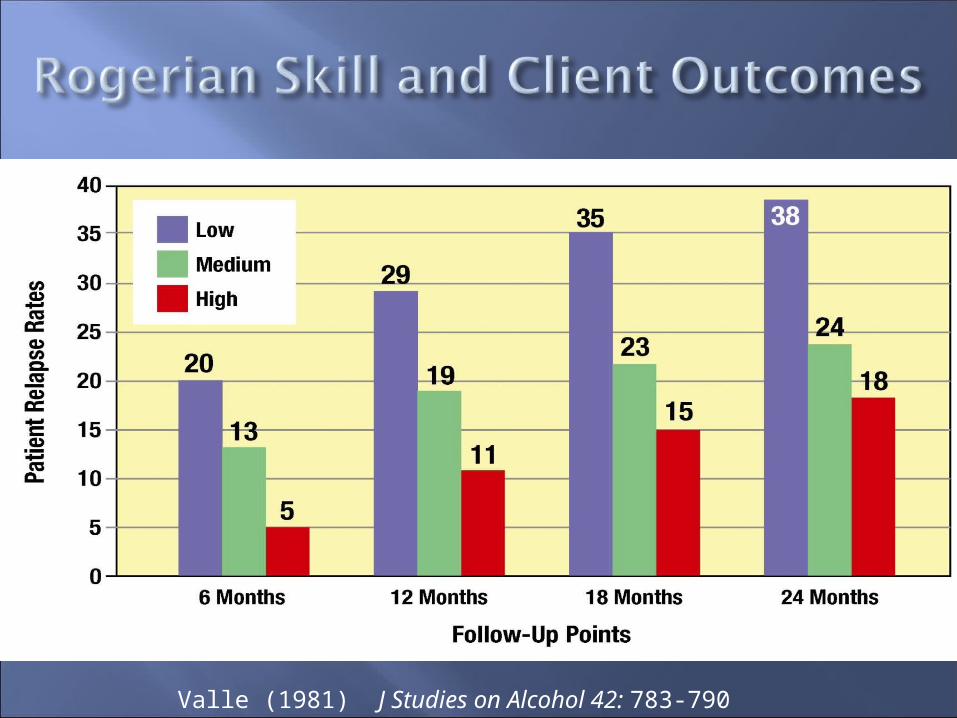
Valle (1981) J Studies on Alcohol 42: 783-790
Invalidated Resist Withdraw
Not respected Arguing DisengagedNot understood Discounting DislikingNot heard Defensive InattentiveAngry Oppositional PassiveAshamed Denying Avoid/leaveUncomfortable Delaying Not returnUnable to changeJustifying
Affirmed AcceptApproach
Understood Open Talk moreAccepted Undefensive LikingRespected Interested EngagedHeard Cooperative ActivatedComfortable/safe Listening Come backEmpoweredHopeful/Able to change
OpenCooperativeArguingEngagedActiveEmpoweredHopefulLiking
DefensiveOppositionalListeningDisengagedPassivePowerlessUnable to
changeDisliking
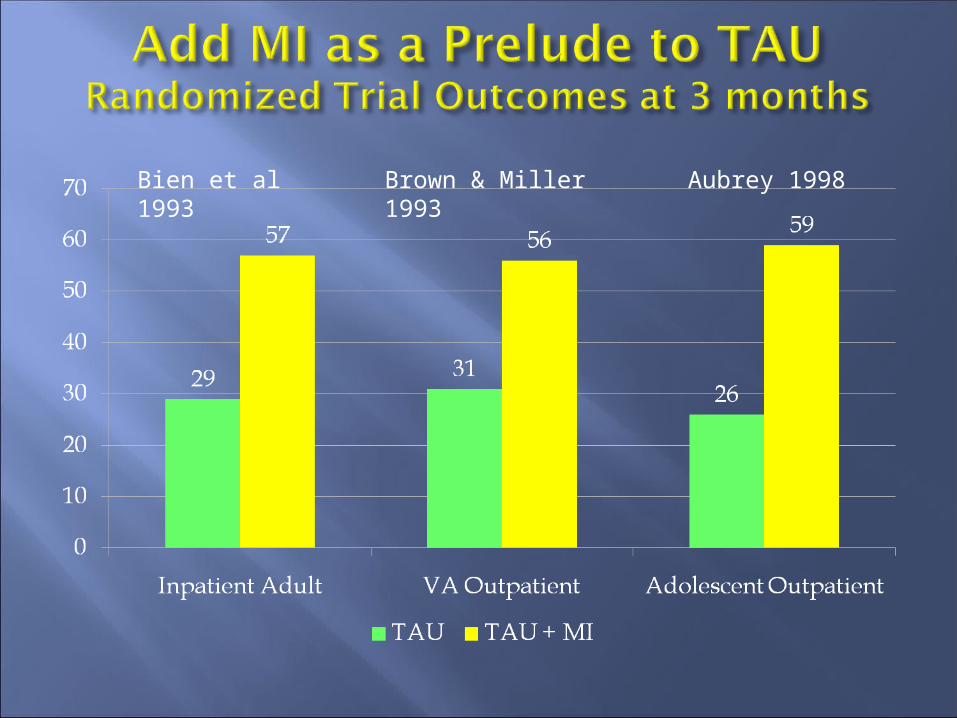
Bien et al 1993
Brown & Miller 1993
Aubrey 1998
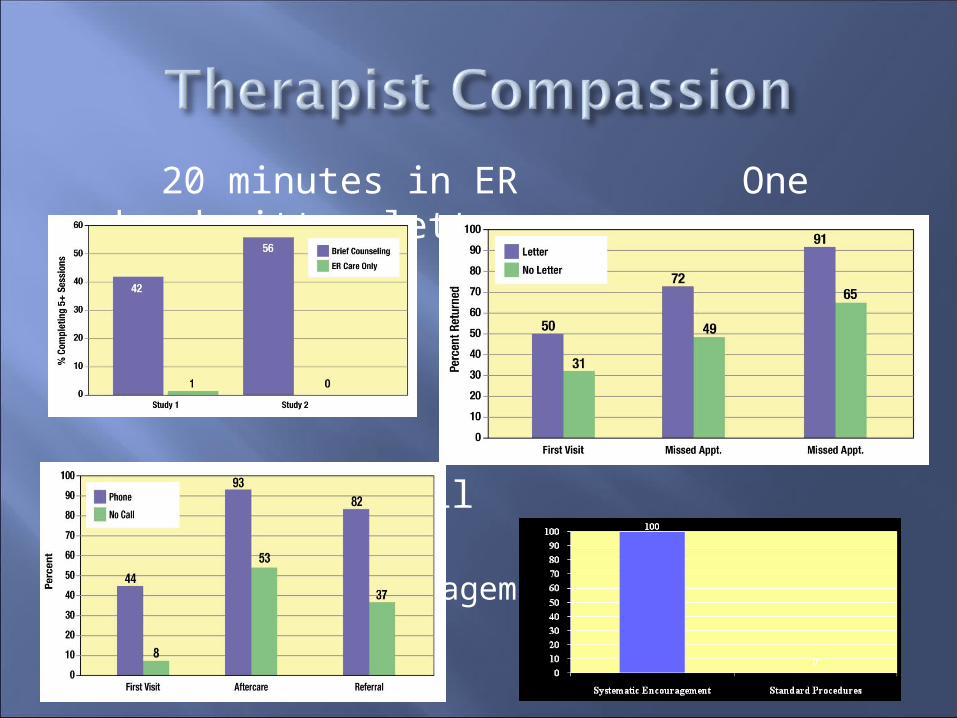
20 minutes in ER One handwritten letter
One telephone call Systematic
Encouragement
Hire Empathic Therapists!
It is an evidence-based practice to hire staff based on and to train staff in
the skill of accurate empathy
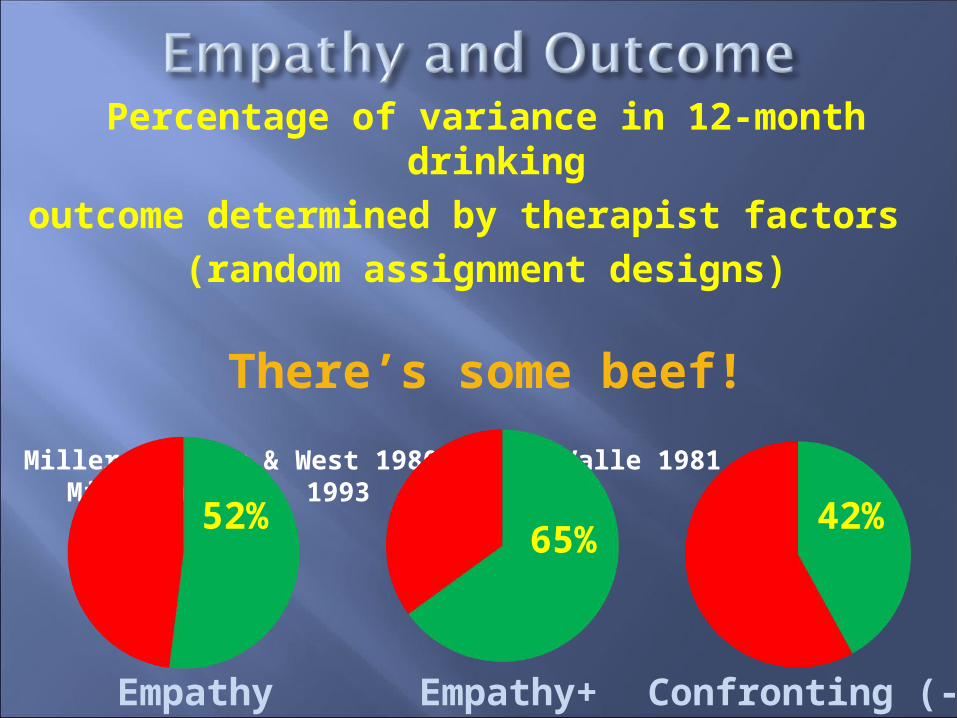
Percentage of variance in 12-month drinking
outcome determined by therapist factors (random assignment designs)
There’s some beef!
Miller, Taylor & West 1980 Valle 1981 Miller et al., 1993
52% 42%
Empathy Empathy+ Confronting (-)
65%
OR THE OR THE BOARDSBOARDS


and some of them are influenced by the therapist
Motivation for change Self-efficacy Hope/optimism Attendance/adherence
Involving a spouse in treatment significantly improves client substance use outcomes
And again it matters what you do
There are some specific treatment effects generally supported by clinical trials
They are often relatively small compared to Therapist effects Client effects and social context Overall impact of treatment And perhaps for these reasons they vary across
sites These larger “nonspecifics” (e.g.,
empathy) need to be specified, tested, and trained as EBTs

Treatment-as-usual is a high standard to beat
Re-training staff in EBTs can be challenging and expensive
Specific treatment effect size often shrinks with dissemination into clinical practice
Therapist belief/enthusiasm / style matters Testable question: Is it cost effective to re-
train staff in an EBT? In any event, it makes sense to train the
next generation of addiction professionals in EBTs from the very beginning!
What is it about the therapists who are delivering the treatment that affects outcome?
What is it about the treatment that really matters?
Understanding the underlying mechanisms of efficacy of treatments and therapists will help us to know: Whom to hire What is essential in training What to focus on in fidelity monitoring What can be changed in adaptations