Embed Size (px)
Citation preview

The stuUniversi
PresenteMeeting
Accepte
ReprintWomenE-mail:
0039-60
� 2014
http://d
Relative value units and payer mixanalysis of facial trauma coverageat a level 1 trauma center: Is thecurrent model sustainable?Mohamed F. Osman, MD,a,b Reginald F. Baugh, MD,b Aaron D. Baugh, MD,b
Marlene C. Welch, MD, PhD,b Joseph J. Sferra, MD, FACS,c and Mallory Williams, MD, MPH,b
Boston, MA, and Toledo, OH
Purpose. We aimed to approximate the annual clinical work that is performed during facial traumacoverage and analyze the economic incentives for subspecialty surgeons providing the coverage.Methods. A retrospective, clinical productivity data analysis of 6 consecutive years of facial traumacoverage at an American College of Surgeons–verified Level I trauma center was performed by the use ofa trauma database and relative value unit (RVU) data. A payer mix analysis also was completed. SPSSV19 was used for analysis.Results. Between 2006 and 2011, 526 patients were treated for facial injuries. The annualnonoperative RVUs ranged from 371 to 539, whereas the annual operative RVUs range was 235–426.Trend analysis displayed that most of the annual RVUs were nonoperative until the year 2011, when theoperative RVUs surpassed the nonoperative. Payer mix analysis revealed that commercial insurancecoverage was the most common (range 21–54%, median 41%) followed by self-pay coverage (18–32%,median 29%). This finding was a consistent phenomenon except in the year 2009, when self-paycovered the majority of the RVUs (32%). Nasal bone fractures (24%) and mandibular fractures (16%)were the two most common diagnoses. Open reduction and internal fixation of mandibular fractures(17%), open reduction and internal fixation orbital bone fractures (15%), and complex facial repair(12%) constituted the most common operative procedures. Facial trauma consultations were obtained22% (16–24%) of covered days. The percent of days requiring emergency procedures was (0.5–1%).Conclusion. The infrequency of subspecialty consultations and operative interventions, and significantpayer mix differences between facial trauma patients relative to the current ambulatory surgerypopulation of the covering subspecialties poses economical challenges for both the hospitals and providersthat use the traditional coverage models. (Surgery 2014;156:995-1002.)
From the Brigham and Women’s Hospital, Harvard Medical School,a Boston, MA; University of ToledoCollege of Medicine,b and ProMedica Health System/The ProMedica Toledo Hospital,c Toledo, OH
AMERICAN COLLEGE OF SURGEONS (ACS)-verifiedtrauma centers improved clinical outcomes ininjured patients.1-3 At least one in each five patientscared for in ACS-verified trauma centers will havefacial trauma. An essential component of trauma
dy was supported by the Department of Surgery at thety of Toledo College of Medicine.
d at the Central Surgical Association 2014 Annualin Indianapolis, IN, March 8, 2014.
d for publication June 23, 2014.
requests: Mohamed F. Osman, MD, Brigham and’s Hospital, 75 Francis Street, Boston, MA [email protected].
60/$ - see front matter
Elsevier Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2014.06.046
care at Level I centers is subspecialty operativecoverage for facial trauma.4 Call coverage for facialtrauma usually is shared by several subspecialties,including oral andmaxillofacial surgeons, otolaryn-gologists, and plastic surgeons. In theUnited States,recent observed trends have identified a decrease inemergency department (ED) coverage for facialtrauma.5,6 The demanding and irregular hours,poor compensation/reimbursement by third-partypayers, competing clinical activities, and the lackof insurance coverage by a large percentage of thetrauma population are major deterrents for manysubspecialty surgeons to dedicate their time towardthis discipline.5,6 As physician reimbursementmodels continue to change and payment for sub-specialty call coverage remains highly variable,7 athorough analysis of both the work performed by
SURGERY 995

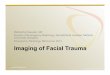
Fig 1. Operative versus nonoperative relative value units(RVUs).
SurgeryOctober 2014
996 Osman et al
these subspecialty surgeons and the economics ofthe call coverage (both for the hospital and the sur-geon) is required to determine the long-term feasi-bility of providing this call coverage using thetraditional subspecialty models. Furthermore, aweak economic incentive model for maxillofacialsubspecialty coverage threatens both trauma centerviability and expansion. Specifically within the cur-rent ACS Committee on Trauma definition of LevelI trauma care, trauma center structure, operations,and capability are threatened. Therefore, in thisstudy, we performed a relative value unit (RVU)analysis of facial trauma coverage at an ACS-verified Level I trauma center. Our goals were toevaluate the annual in-hospital clinical work thatis performed during facial trauma coverage andquantify the economic incentives for subspecialtysurgeons providing the coverage.
METHODS
A retrospective RVU analysis of 6 consecutiveyears of maxillofacial trauma coverage at theUniversity of Toledo Medical Center (UTMC), anACS-verified, Level I trauma center, was performedby the use of a trauma database and calculatedRVUs. The trauma database includes all traumapatients admitted to UTMC and is quality assuredfor accuracy with daily admission logs from thehospital ED and all inpatient services. All maxillo-facial trauma subspecialty coverage services’ pa-tients are admitted to the trauma service, andadmissions for outpatient surgery are listed ondaily inpatient admission logs that are screened bythe trauma program manager.
During the period of January 1, 2006, toDecember 31, 2011, a total of 526 patients withfacial injuries were entered into the UTMC traumadatabase. The following patient data were collected:mechanism of injury, type of injury (location andconcomitant injuries), length of stay, InternationalClassification of Diseases, Tenth Revision, codes,operative procedure and their Current ProceduralTerminology codes, and payer source. Traumacare process data also were extracted, includingsubspecialty coverage of specific injuries, numberof consultation days, type of consultation (routinevs emergent), time of consultation performance,and days with operative procedure.
Using the January 2013 Revision file, we usedthe resource-based relative value scale (RBRVS) totranslate each scheduled Current Procedural Ter-minology code into RVUs.8 A descriptive analysisof the data was performed. SPSS V19 (SPSS Insti-tute, Chicago, IL) was used for analysis. Becauseof the lack of recent published data on the
numbers and incidences of facial trauma casesamong ACS-verified trauma centers, these valueswere extracted from the National Trauma DataBank for the years 2008–2013.
RESULTS
The total number of facial trauma patients was526, with a hospital-based incidence rate of 7%.The maxillofacial trauma coverage in our institu-tion was provided by maxillofacial surgeons 50%,plastic surgeons 25%, and otolaryngologists 25%.
From 2006 to 2011, the total RVUs were 4564,ranging annually between 579 and 874 with anaverage of 760 RVUs per year (2 RVUs/day). Theannual operative RVUs range was 235–426 with anaverage of 309. The annual nonoperative RVUsranged from 371 to 539 with an average of 452(Fig 1). Trend analysis displayed that most of theannual RVUs were nonoperative until the year2011, when the operative RVUs (426) surpassedthe nonoperative counterpart (370), Table I.
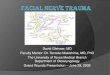
Payers’ data analysis revealed that the commer-cial insurance coverage (range 21–54%, median41%) was the most common, followed by self-paycoverage (18–32%, median 29%; Fig 2). Thisfinding was a consistent phenomenon except inthe year 2009 when self-pay covered the majorityof the RVUs. Medicare coverage was (7–27%, me-dian 17%), whereas Medicaid coverage was (8–19%, median 17%), Table I and Table II.
Open reduction and internal fixation ofmandibular fractures (17%), open reduction andinternal fixation orbital bone fractures (15%), andcomplex facial repair (12%) constituted the mostcommon operative procedures for maxillofacialtrauma patients. Nasal bone fractures (24%),mandibular fractures (16%), and facial lacerations(14%) represented the most common diagnoses inour patient population (Table III).

Table I. RVUs and payer mix
Year Total RVUs Nonoperative RVUs Operative RVUs
Insurance status of patients, %
Commercial Medicare Medicaid Self-pay
2006 874.03 539.20 334.83 54 7 8 312007 817.59 512.24 305.35 51.42 8.57 8.57 31.442008 731.04 431.36 299.68 40.45 13.48 19.10 26.972009 765.42 512.24 253.18 21.87 27.08 18.75 32.292010 579.11 343.74 235.37 38.71 27.42 16.13 17.742011 796.69 370.70 425.99 41.66 21.43 17.86 19.05
RVU, relative value unit.
Fig 2. Payers’ trend analysis.
SurgeryVolume 156, Number 4
Osman et al 997
Subspecialty coverage for facial trauma wasavailable 24 hours a day, 7 days a week. Consulta-tions were needed on an average of 22% (16–24%)of covered days. The number of days with emer-gency procedures was 2–4 days/year (0.5–1%),Table IV.
DISCUSSION
The creation of trauma centers and traumaprograms has been shown to have positive impacton outcomes in themanagement of severely injuredpatients.1-3 The clinical capability ofmanaging com-plex facial injuries is essential for Level 1 traumaverification by the ACS4; however, maintaining aLevel I trauma center is a resource-intense institu-tional effort that requires the commitment of sub-specialty surgeons. Trauma care is associated withlow reimbursement by federal agencies, placing aneconomic burden on major trauma centers in theUnited States.9-13 So far in themedical literature, an-alyses of financial data have been limited to studiesthat compared economic outcomes of differenttreatment strategies for mandible and isolated mid-face fractures14-19; however, there is no systematiceconomic analysis that describes the underlyingeconomic incentives for specific subspecialties to
invest the needed commitment. Current subspe-cialty coveragemodels provide a stipendormandatecall coverage as a part of staff privileges. This callcoverage mandate may informally expire withseniority in larger trauma centers and is assumedby younger subspecialty surgeons. There arenopub-lished data that analyze the cost of providing subspe-cialty call coverage to the hospital or to the surgeon.Both changes to physician reimbursement and leanmanagement policies have made these types of dataessential. Assuming that subspecialty coverage willcontinue under the current models may understatethe challenges facing trauma centers in the future.
Our institution has been an ACS-verified, Level 1trauma center all through the 6 years of study timeand facial trauma is covered by maxillofacial sur-geons, plastic surgeons, and otolaryngologists. AtUTMC, most of the coverage was provided bymaxillofacial surgeons (50%), and the rest wasequally shared by otolaryngologists and plasticsurgeons. Recent national survey of 57 Level Itrauma centers indicates that plastic surgeons areresponsible for 40% of the subspecialty callcoverage for facial trauma followed by maxillofacialsurgeons (36%), and otolaryngologists (23%).20
Each of these specialties’ participation in traumacare is usually secondary to robust consultativeand outpatient practices. Hence, the managementof trauma patients usually is not the primary focusor motivation of these subspecialties, particularlythe call coverage, which can interfere with both elec-tive surgery and clinic schedules. Recent survey dataof 1,300 otolaryngologists, 85% of respondentsparticipated in trauma call coverage revealed thatonly 36% of those surveyed would increase their vol-ume of maxillofacial trauma if reimbursementimproved.21 A sense of duty was the number onereason for respondents participating in traumacall coverage.21 Although admirable, this is certainlynot an economic strategy or incentive model.
The incidence of facial injuries occurring inconjunction with major trauma was shown in

Table II. Payer mix analysis
Year
Nonoperative RVUs, N, % Operative RVUs, N, %
Commercial Medicare Medicaid Self-Pay Commercial Medicare Medicaid Self-Pay
2006 283 (53%) 34 (6%) 34 (6%) 189 (35%) 205 (61%) 47 (14%) 44 (13%) 39 (12%)2007 270 (53%) 74 (14%) 47 (9%) 121 (24%) 140 (46%) 12 (4%) 17 (5%) 137 (45%)2008 196 (45%) 54 (13%) 81 (18%) 101 (23%) 133 (45%) 44 (15%) 40 (13%) 83 (28%)2009 182 (36%) 101 (20%) 94 (18%) 135 (26%) 156 (62%) 38 (15%) 26 (10%) 34 (13%)2010 162 (47%) 74 (22%) 47 (14%) 61 (18%) 94 (40%) 15 (6%) 33 (14%) 95 (40%)2011 148 (40%) 94 (25%) 61 (16%) 67 (18%) 217 (51%) 95 (22%) 88 (21%) 26 (6%)
RVU, Relative value unit.
Table III. Frequent diagnosis and procedures
YearThree most frequent
ICD codesThree most frequent
CPT codes
2006 Nasal bone FrxFacial LacMandibular Frx
ORIF mandibleORIF orbital boneComplex repair facial Lac
2007 Nasal bone FrxFacial LacMandibular Frx
ORIF mandibleORIF orbital boneComplex repair facial Lac
2008 Nasal bone FrxOrbital bone FrxMandibular Frx
ORIF mandibleORIF orbital boneComplex repair facial Lac
2009 Orbital bone FrxFacial LacMandibular Frx
ORIF mandibleORIF orbital boneComplex repair facial Lac
2010 Nasal bone FrxZygomatic bone FrxMandibular Frx
ORIF mandibleORIF orbital boneComplex repair facial Lac
2011 Nasal bone FrxOrbital bone FrxMandibular Frx
ORIF mandibleORIF orbital boneComplex repair facial Lac
CPT, Current Procedural Terminology; Frx, fracture; ICD, InternationalClassification of Diseases; Lac, laceration; ORIF, open reduction and inter-nal fixation.
Table IV. Work intensity
YearConsultations/day
of coverageDays with noconsultations
Days with emergentoperation
2006 84 (23%) 281 (77%) 2 (0.5%)2007 87 (24%) 278 (76%) 4 (1.1%)2008 82 (22%) 284 (78%) 2 (0.5%)2009 85 (23%) 280 (77%) 2 (0.5%)2010 58 (16%) 305 (84%) 4 (1.1%)2011 78 (21%) 288 (79%) 4 (1.1%)
Table V. Incidence of facial trauma from NTDBannual reports
Year No. facial trauma cases Percent
2008 127,751 25.222009 155,848 24.822010 178,352 14.062011 170,821 23.632012 182,671 23.622013 201,013 24.12
NTDB, National Trauma Data Bank.
SurgeryOctober 2014
998 Osman et al
several surveys that ranged from 34% of 87,174trauma patients in a North American Database onTrauma to 15% of 1,088 trauma patients in Liver-pool, and 25% of 802 trauma patients in Lon-don.22-24 Extracted from the National Trauma DataBank from 2008 to 2013, the incidence of facialtrauma has ranged between 14 and 25%, with anaverage of 22.6% (Table V). The rate of facialinjury within our trauma population was 7%,which is substantially less than the rates previouslyreported in the literature. This finding should notimpact the overall annual RVU data presentedhere because the actual facial trauma volume pre-sented is comparable to similar ACS-verified cen-ters reported in National Trauma Data Bank.Moreover, the numbers presented here are abso-lute RVUs and no denominator effect included.It would be an oversimplification to suggest the
RVU data presented in this study are attributableto the fact that there are 3 ACS-verified, Level Itrauma centers in Toledo. In fact, an informal re-view of operative volume in facial trauma at thetwo other centers revealed similar numbers.
Most previous epidemiologic studies have foundthat the most common site of facial injury to be themandible.25-27 A 5-year review of facial fracturesfrom Canada by Hogg et al28 noted an excess ofmandibular fractures over zygomatic and maxillaryfractures with a ratio of 6:2:1; however, a nation-wide administrative data based study by Allareddyet al29 have shown that 50% of visits to the EDwith facial fractures were associated with fracturesof the nasal bone. The facial injuries pattern inour trauma population was consistent over the6 years, with nasal bone fractures (24%) andmandibular fractures (16%) the two most com-mon diagnoses. The cause of this contrast in

Fig 3. Payers trends for nonoperative relative value units(RVUs).
Fig 4. Payers trends for operative relative value units(RVUs).
SurgeryVolume 156, Number 4
Osman et al 999
incidence is unclear, but one explanation could berelated to the inclusion criteria. Although previousstudies have included facial fracture patients afteradmission to a hospital, our study and EDpopulation-based studies included all patientswho presented to EDs with facial trauma. More-over, nasal fractures only need to be correctedwhen there is a functional or esthetic defect, andit may be that many of the nasal fractures present-ing to an ED may not require inpatienthospitalization.
Since the Health Care Financing Administra-tion introduced the RBRVS in 1992, it has becomethe prevailing model to describe, quantify, andreimburse physician services. Medicare, Medicaid,and many private insurance companies use theRBRVS to determine payment for physician ser-vices, and many practices and institutions useRVUs to track physician productivity and evaluatejob performance.8 Our facial trauma RVU dataanalysis revealed that the majority of the RVUswere from nonoperative clinical work, a findingthat reflects on the relatively lower rate of proce-dures needed in caring for this subset of traumavictims (Figs 3 and 4). Over the study 6 yearsperiod the total RVUs were 4,564, ranging annuallybetween 579 and 874 with an average of 760 RVUsper year. This equals to 2 RVUs/day, an absolute
number that highlights the lesser financial yieldand hence economic drive.
Our analysis shows that facial trauma subspe-cialty consultations were obtained in only 22%(16–24%) of covered days. Moreover the emer-gency procedures needed only in 0.5–1% of thetime. These findings materialize significant chal-lenges to both the hospitals ability to justifyproviding financial support for subspecialty callcoverage and the surgeons’ ability to both remainhighly skilled at providing operative trauma ser-vices and rationalize the allocation of their time. Aconcern with maintenance of skill levels is revealedin a survey of ear-nose-throat surgeons who specif-ically stated ongoing clinical education in traumaas heavily needed.21
A recent analysis based on the NationwideEmergency Department Sample of the HealthcareCost showed that 26.4% of those who presented toan ED with facial fracture were uninsured and only37.5% of those who presented with facial fractureshad private health insurance.29 Our payers mixanalysis revealed that commercial insurancecoverage was the most common (range 21–54%,median 41%), followed by self-pay coverage. Thisis not typical of most ACS-verified trauma centers,which consistently had average of 21% commercialcoverage over the last 6 years. However, even with afacial fracture population with a superior payermix to most other trauma centers, the payer mixis substantially inferior to the ambulatory practicesof the covering subspecialists.
A close look at the trend analysis reveals thatthere is more year-to-year variability in the contri-bution of the commercial and self-pay groupscompared with the relatively stable contributionin the Medicare and Medicaid groups. Comparingthese data with the outpatient private practices ofthe subspecialty surgeons makes the relatively highcommercial insurance coverage in this cohort oftrauma patients still appear less desirable from theperspective of the subspecialty surgeon. Our sub-specialty surgeons’ private practice payer sourcesare 82% commercial and 15% Medicare. There-fore, operative or nonoperative time spent intrauma coverage is inefficient for these surgeons.
This study is a retrospective descriptive analysisfrom a single Level 1 trauma center. To ourknowledge, this is the first report on RVU andpayer mix analysis of subspecialty facial traumacoverage. The observations in this study challengethe sustainability of the current coverage modelsand could potentially undermine the quality offacial trauma care in trauma centers unless a morecomprehensive and effective solutions to on-call

SurgeryOctober 2014
1000 Osman et al
coverage are entertained. This study highlights thecritical situation of the economic incentives andsustainability of subspecialty trauma coverage.
The infrequency of subspecialty consultationsand operative interventions needed in thecoverage of facial trauma challenges the long-term feasibility of providing this coverage usingthe traditional subspecialty models. Further studiesare needed to assess the reproducibility of this dataand to further characterize the facial trauma workload in different regions of the country. Thisresearch is essential to understanding the sustain-ability of current level I trauma care in the contextof health care reform and payment innovation.
REFERENCES
1. Sampalis JS, Lavoie A, Bookas S, et al. Trauma center desig-nation: Initial impact on trauma-related mortality. J Trauma1995;39:232-9.
2. Baker CC, Degutis LC, DeSantis J, et al. Impact of a traumaservice on trauma care in a university hospital. Am J Surg1985;149:453-8.
3. Demetriades D, Berne TV, Belzberg H, et al. The impact ofa dedicated trauma program on outcome in severelyinjured patients. Arch Surg 1995;130:216-20.
4. Committee on Trauma, American College of Surgeons: Re-sources for Optimal Care of the Injured Patient. 1999. Avail-able from http://www.facs.org/trauma/publications.html.
5. Hausamen J. The scientific development of maxillofacialsurgery in the 20th century and an outlook to the future.J Craniomaxillofac Surg 2001;29:2-21.
6. Vanlandingham B, Marone B. On-call specialist coverage inUS emergency departments: ACEP survey of emergencydepartment directors. American College of Emergency Phy-sicians 2004. Available from www.acep.org. Accessed January4, 2014.
7. Buntin MB, Escarce J, Goldman D, et al. Determinants ofIncreases in Medicare Expenditures for Physicians’ Services.Rockville (MD): Agency for Healthcare Research and Qual-ity (US); 2003 Oct. (Technical Reviews, No. 7.) Appendix A,Payment for Physicians’ Services Under the Resource BasedRelative Value Scale. Available from http://www.ncbi.nlm.nih.gov/books/NBK43875/.
8. 2013 National Physician Fee Schedule Relative Value File.Washington, DC: Centers for Medicare and Medicaid,Department of Health and Human Services; 2013. Availablefrom http://www.cms.gov.
9. Bach BR Jr, Wyman ET Jr. Financial charges of hospitalizedmotorcyclists at the Massachusetts General Hospital.J Trauma 1986;26:343-7.
10. Shapiro MJ, Keegan M, Copeland J. The misconception oftrauma reimbursement. Arch Surg 1989;124:1237-40.
11. Bolhofner B, Carmen BA, Donohue SD, Harlen K. Motor-cycle accident injury severity, blood alcohol levels, insur-ance status, and hospital costs: a 4-year study in St.Petersburg, Florida. J Orthop Trauma 1994;8:228-32.
12. Henry MC, Thode HC Jr, Shrestha C, Noack P. Inadequatehospital reimbursement for victims of motor vehiclecrashes due to health reform legislation. Ann Emerg Med2000;35:277-82.
13. Lanzarotti S, Cook CS, Porter JM, et al. The cost of trauma.Am Surg 2003;69:766-70.
14. Abubaker AO, Lynam GT. Changes in charges and costsassociated with hospitalization of patients with mandibularfractures between 1991 and 1993. J Oral Maxillofac Surg1998;56:161-7; discussion 167-8.
15. Azevedo AB, Trent RB, Ellis A. Population-based analysis of10,766 hospitalizations for mandibular fractures in Califor-nia, 1991 to 1993. J Trauma 1998;45:1084-7.
16. Dodson TB, Pfeffle RC. Cost-effectiveness analysis of openreduction/nonrigid fixation and open reduction/rigid fixa-tion to treat mandibular fractures. Oral Surg Oral Med OralPathol Oral Radiol Endod 1995;80:5-11.
17. David LR, Bisseck M, Defranzo A, et al. Cost-based analysisof the treatment of mandibular fractures in a tertiary carecenter. J Trauma 2003;55:514-7.
18. Sanger C, Argenta LC, David LR. Cost-effective managementof isolated facial fractures. J Craniofac Surg 2004;15:636-41.
19. Erdmann D, Price K, Reed S, Follmar KE, et al. A financialanalysis of operative facial fracture management. Plast Re-constr Surg 2008;121:1323-7.
20. Bagheri SC, Dimassi M, Shahriari A, Khan HA, Jo C, SteedMB. Facial trauma coverage among level-1 trauma centersof the United States. J Oral Maxillofac Surg 2008;66:963-7.
21. McCusker SB, Schmalbach CE. The otolaryngologist’s costin treating facial trauma: American Academy of Otolaryn-gology–Head and Neck Surgery survey. Otolaryngol HeadNeck Surg 2012;146:366-71.
22. Sastry SM, Sastry CM, Paul BK, Bain L, Champion HR. Lead-ing causes of facial trauma in the major trauma outcomestudy. Plast Reconstr Surg 1995;95:196-7.
23. Cannell H, Dyer PV, Paterson A. Maxillofacial injuries in themultiply injured. Eur J Emerg Med 1996;3:43-7.
24. Down KE, Boot DA, Gorman DF. Maxillofacial and associ-ated injuries in severely traumatized patients: implicationsof a regional survey. Int J Oral Maxillofac Surg 1995;24:409-12.
25. Imahara SD, Hooper RA, Wang J, et al. Patterns and out-comes of pediatric facial fractures in the United States: Asurvey of the national Trauma DataBank. J Am Coll Surg2008;207:710-6.
26. Al-Khateeb T, Abdullah FM. Craniomaxillofacial injuries inthe United Arab Emirates: A retrospective study. J Oral Max-illofac Surg 2007;65:1094-101.
27. Bakardjiev A, Pechalova P. Maxillofacial fractures in South-ern Bulgaria---A retrospective study of 1706 cases.J Craniomaxillofac Surg 2007;35:147-50.
28. Hogg NJ, Stewart TC, Armstrong JE, Girotti MJ. Epidemi-ology of maxillofacial injuries at trauma hospitals in On-tario, Canada between 1992 and 1997. J Trauma 2000;49:425-32.
29. Allareddy V, Allareddy V, Nalliah RP. Epidemiology of facialfracture injuries. J Oral Maxillofac Surg 2011;69:2613-8.
DISCUSSION
Dr Steven Steinberg (Columbus, OH): Dr Os-man and his team have performed a retrospectivestudy looking at facial trauma care and, in partic-ular, the ability to support a facial trauma team, attheir Level 1 trauma center. They found that theclinical volume was low, about one consult every 5days. Well less than one half of the consults resultedin an operation. RVU productivity per year was low,about 800 total RVUs per year, which is far too littleto support even one physician full-time equivalent.

SurgeryVolume 156, Number 4
Osman et al 1001
Payer mix was not terribly abysmal for a trauma cen-ter, with 20–25% of patients being self-pay. Theirimplied conclusion is that the ACS should backoff on their requirement that Level I trauma cen-ters need to be able to provide facial trauma care,as that has the possibility to drive some trauma cen-ters out of the business of trauma care.
But, as Lee Corso says during his football broad-casts, ‘‘Not so fast, my friend!’’ First, the authorshave given an incomplete picture of what their ear-nose-throat, oral and maxillofacial surgery, andplastic surgery colleagues do in their spare timewhen they are not operating on trauma patients.Does the rest of their practice allow them to makeends meet? We all have ‘‘loss leaders’’ in ourpractice, but we make up for it in other ways.
Second, is this an indictment of the finances offacial trauma and ACS standards for trauma cen-ters, or is this an indictment of the Toledo commu-nity and how it chooses to spend its resources?I have some knowledge of the trauma system inToledo, as I live in Ohio, and have some knowledgeof the status of the trauma system on the state level.Also, I will admit that I am from Toledo.
As of the 2010 census, the city of Toledo had apopulation of 287,000, and the metropolitan areacontained 651,000 people. It is the fourth mostpopulous city in Ohio, but it has three Level 1trauma centers, more thanCleveland, Columbus, orCincinnati. In addition, there is another Level 1trauma center 50 miles away in Ann Arbor, Michi-gan, twootherLevel 2 centers innorthwesternOhio,and five Level 3 trauma centers in northwesternOhio, one of which is within the city of Toledo.
I don’t know the volume of each of Toledo’sLevel 1 trauma centers, but my experience tells methat Toledo does not need three Level 1 traumacenters, especially if they don’t work well with eachother. Are there opportunities to share some re-sources, such as those surgeons who manage facialtrauma, between the trauma centers in Toledo, orcombine three trauma centers into two?
Dr Mohamed F. Osman: Thank you Dr Stein-berg for the comments and valuable insight.Answering the second question, in Toledo, yes,we have three Level 1 trauma centers, and wemight have overcapacity in Level 1 trauma centersfor the city. Toledo might have the highest Level 1trauma per population in the world after Boston,but we believe that this observation does notexplain the phenomenon that we are highlightinghere, because with two RVUs per day, even if wequadruple this clinical work, it doesn’t seem tobe feasible or sustainable for the coverage of Level1 trauma centers under the current model.
The other point is, with combining the traumacenters, wemight have a greater number of patientsbut the ratio will be the same, around 7%. If weshare the resources that will be hospital-centric, itmay well help the hospitals, but I don’t believe it’sgoing to help the coverage providers, because thetrauma population and practice will continue to bethe same with greater risk, greater liability, andirregular compensation. That will not be an attrac-tive solution from the provider standpoint; it mightbe from the hospital administrations standpoint.
The first question, about the providers and whatthey do, we performed informal discussion, and wetalked to the providers about the incentives andtheir opinion in different populations. We thinkthat, with the impending payment innovationwhich is going to put strains on their ambulatorypractices, it’s very hard to convince them tocontinue to be the loss leaders and to continueto take the risk and offer Level 1 traumas.
Recent national review showed that sense ofresponsibility is the main driver for those providersto cover trauma. It’s indeed admirable, but it’sdefinitely not an economically viable model tosustain the coverage of trauma.
Dr Charles Scoggins (Louisville, KY): I have twoquick questions. First, can you tell us what percent-age of your RVU data are procedure-based andwhat percent are Evaluation and managementbased? Because, as you know, a lot of trauma careinvolves the nonoperative management of pa-tients, and that generates evaluation and manage-ment charges. I wonder if you’ve captured those.Second, I think the point was raised, and is veryvalid, that you might be, on average, getting twoRVUs a day for taking care of facial trauma pa-tients, but I suspect that folks are doing other stuffwhen they are not rounding on trauma patientswho have a facial injury.
Dr Mohamed F. Osman: Around two thirds ofthe RVUs were from nonoperative clinical work,and one third from operative clinical work. The ra-tio has been consistent. The two RVUs per year is areflection of the total RVUs.
Regarding the subspecialty coverage, as youknow nontrauma activities for plastics and ENTsurgeons is definitely more lucrative and moreefficient and lower risk.
Dr Timothy Pritts (Cincinnati, OH): A couple ofquestions. First, what is the real opportunity cost toyour providers? That is, how often are they comingin at night? How often does this actually disrupttheir practices? If you are looking at one consultevery few days, it doesn’t seem like there’s a lotof disruption to their normal income stream and

SurgeryOctober 2014
1002 Osman et al
that taking trauma call really isn’t even a nuisancebut a rare opportunity to do something different.
Second, we’ve learned it at a trauma center farto your south. The key to all of this is reallyefficiency in billing and not leaving money onthe table. Along those lines, how often are folkscoming in at night, and how often are they billingfor the lacerations that are being repaired, or thelacerations being repaired by the emergency med-icine team, the trauma team, or residents that arecovering the services and therefore going unbilledand you’re potentially losing those RVUs toattending-level attribution?
Dr Mohamed F. Osman: Regarding the billing ofthe procedures being performed by the residentsand by the ED, we don’t have specific data on that.All of our data are extracted from the trauma data-base which did not include such details. I agree, itwouldbe interesting to know thosenumbers though.
The second question about the frequency ofthese consultations and the procedures, approxi-mately 24% of the time, there was consultation forfacial trauma. In only half to 1% of the time, thoseconsultations resulted in procedures. Our informaldiscussions with the providers, revealed a generalconsensus and feeling that is phenomenon was
very disruptive because of the irregularity factor.It’s hard for them to schedule a procedure at 7:00in the morning if there is a risk of staying up allnight dealing with a facial trauma patient in theoperating room. So, it is more disruptive to theirschedule and to their lifestyle, again with greaterrisk and lesser profit and lesser yield.
Dr Mallory Williams (Toledo, OH): Mallory Wil-liams, senior author on the paper. One quickcomment: at the end of the day, as the trauma di-rector there, the models and how we compensatethese people don’t work. And it doesn’t matterwhether you look into their lucrative practices foroffsetting costs or any other models. They couldspend and allocate their time concentrated in theirsubspecialty practices and make significantly moremoney.
What we are raising in this article---we are notchallenging, Steve, the criteria of the College thatthis coverage be provided. What we are simplysaying is that it has to be put into an economicmodel that everybody can understand, and that isboth workable for the hospital and for the pro-viders, because the providers will walk when theeconomic downward pressures are put on theirrevenue cycles from their subspecialty practice.