Embed Size (px)
DESCRIPTION
CV Risk Assessment for T2DM Therapies. Reliable Evaluation of Benefit-to-Risk in T2DM: Some Statistical Considerations July 1, 2008 Thomas R. Fleming, Ph.D. Professor, Dept of Biostatistics University of Washington - PowerPoint PPT Presentation
Citation preview

Reliable Evaluation of Benefit-to-Risk in T2DM:
Some Statistical Considerations
July 1, 2008
Thomas R. Fleming, Ph.D.Professor, Dept of Biostatistics
University of [email protected]
CV Risk Assessment for T2DM Therapies
Reliable Evaluation of Benefit-to-Risk
• Surrogate Endpoints
• Validation of Surrogates
• Evaluation of Safety
• Conclusions

Biomarkers (Surrogates) in Diabetes
Treatment effects on Biomarkers ~ HbA1c , C-Peptide
• Establish Biological Activity
• But not necessarily overall Clinical Efficacy ~ Retinopathy, Nephropathy, CVD, Stroke, MI ~ Major hypoglycemic events: Coma/Seizure
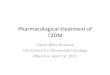
HbA1c End-Organ Glycemic Control Diabetic Complications
Intervention
Disease
End-Organ DiabeticComplications HbA1c
Glycemic Control
Disease
Intervention
Multiple Pathways of the Disease Process
What magnitude and what duration is needed?
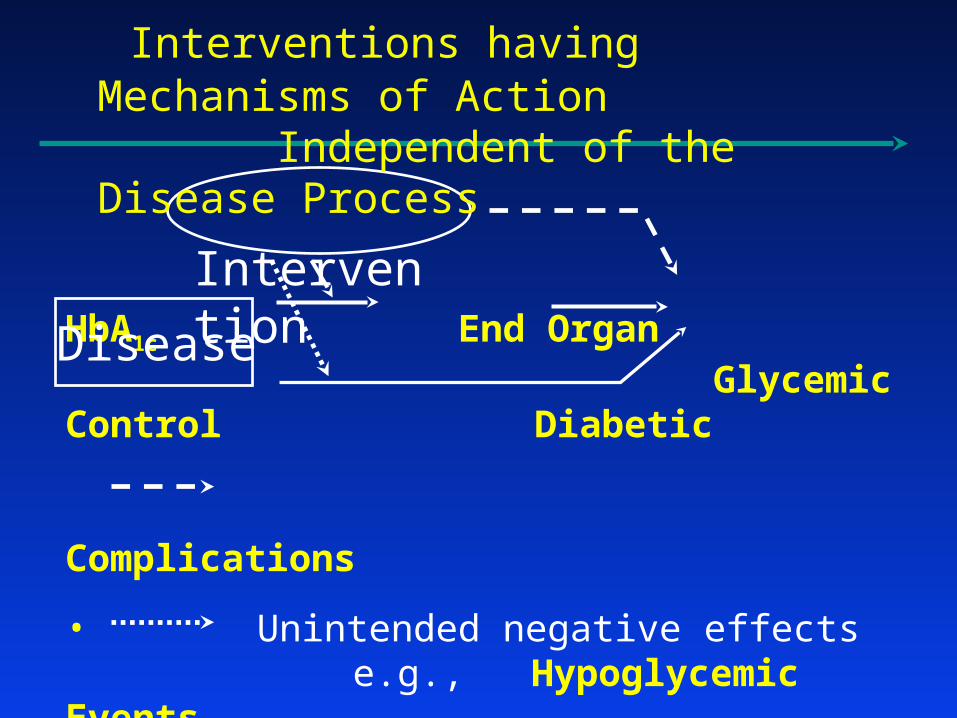
HbA1c End Organ Glycemic Control Diabetic Complications
• Unintended negative effectse.g., Hypoglycemic Events
• Alternative beneficial effects
Disease
Intervention
Interventions having Mechanisms of Action Independent of the Disease Process

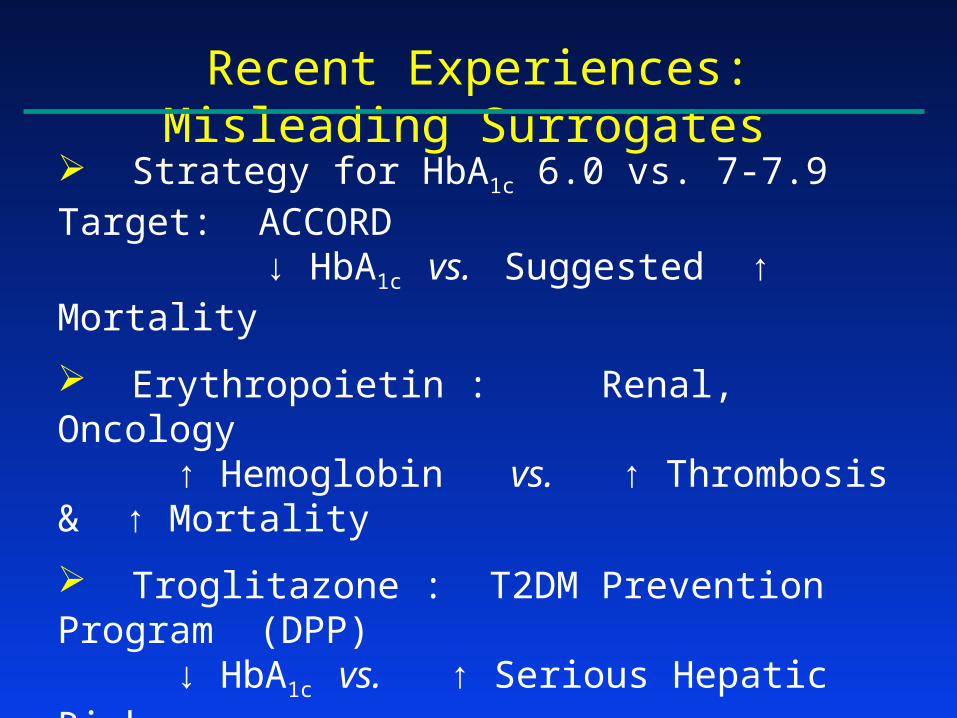
Recent Experiences: Misleading Surrogates
Strategy for HbA1c 6.0 vs. 7-7.9 Target: ACCORD ↓ HbA1c vs. Suggested ↑ Mortality
Erythropoietin : Renal, Oncology ↑ Hemoglobin vs. ↑ Thrombosis & ↑
Mortality
Troglitazone : T2DM Prevention Program (DPP) ↓ HbA1c vs. ↑ Serious Hepatic Risks
Torcetrapid / Atorvastatin in CHD: ILLUMINATE ↑ HDL ↓ LDL vs. ↑ Death & ↑ CHD
Death/MI/Stroke
Muraglitazar & Rosiglitazone : Type 2 Diabetes↓ HbA1c vs. Suggested ↑ Death / Stroke / MI or ↑
MI

End Stage Renal Disease
Standard Dose Epogen Hematocrit 30%
High Dose Epogen Hematocrit 42%R
Goal: Normalize Hematocrit Values
reduce Death and MI

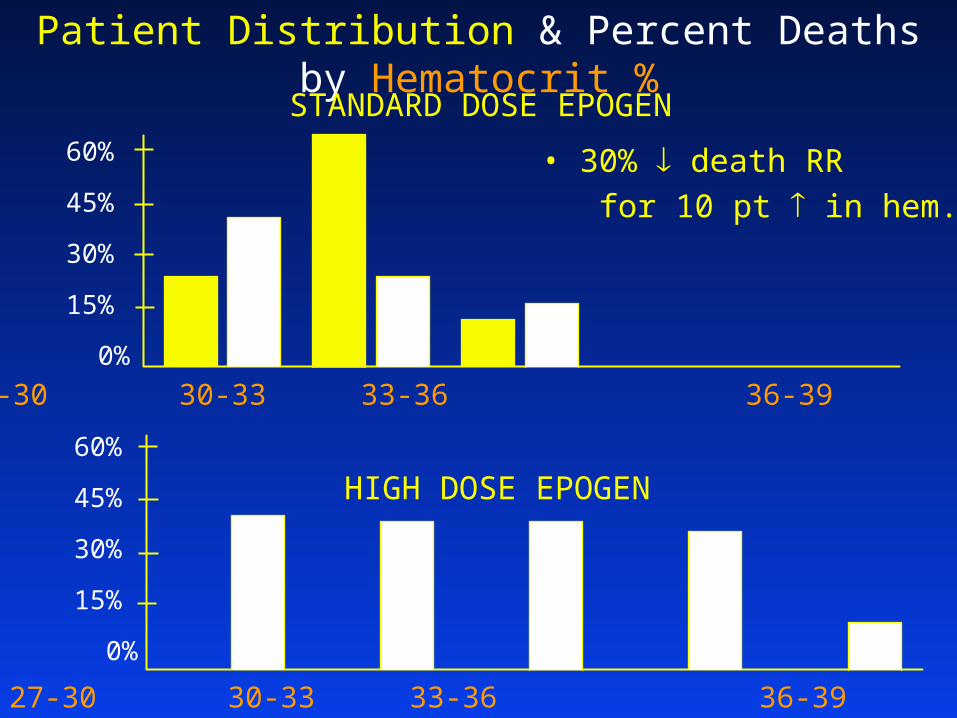
Patient Distribution & Percent Deaths by Hematocrit %
27-30 30-33 33-36 36-39 39-42
STANDARD DOSE EPOGEN
60%
45%
30%
15%
0%

Patient Distribution & Percent Deaths by Hematocrit %
27-30 30-33 33-36 36-39 39-42
STANDARD DOSE EPOGEN
HIGH DOSE EPOGEN
• 30% death RR
for 10 pt in hem.
60%
45%
30%
15%
0%
60%
45%
30%
15%
0%
27-30 30-33 33-36 36-39 39-42
Patient Distribution & Percent Deaths by Hematocrit %
27-30 30-33 33-36 36-39 39-42
STANDARD DOSE EPOGEN
HIGH DOSE EPOGEN
• 30% death RR
for 10 pt in hem.
60%
45%
30%
15%
0%
60%
45%
30%
15%
0%
27-30 30-33 33-36 36-39 39-42

Patient Distribution & Percent Deaths by Hematocrit %
27-30 30-33 33-36 36-39 39-42
STANDARD DOSE EPOGEN
HIGH DOSE EPOGEN
• 30% death RR
for 10 pt in hem.
• in hematocrit
60%
45%
30%
15%
0%
60%
45%
30%
15%
0%
27-30 30-33 33-36 36-39 39-42

Patient Distribution & Percent Deaths by Hematocrit %
27-30 30-33 33-36 36-39 39-42
STANDARD DOSE EPOGEN
HIGH DOSE EPOGEN
• 30% death RR
for 10 pt in hem.
• in hematocrit
• 30% in death RR
60%
45%
30%
15%
0%
60%
45%
30%
15%
0%
27-30 30-33 33-36 36-39 39-42
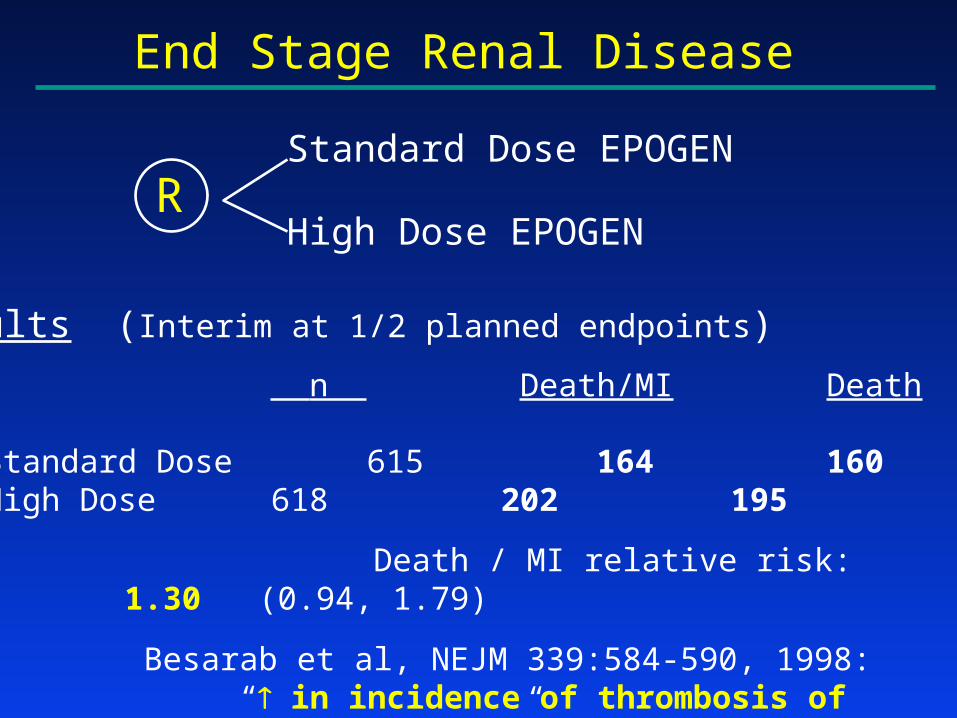
End Stage Renal Disease
Standard Dose EPOGEN
High Dose EPOGEN
Results (Interim at 1/2 planned endpoints)
n Death/MI Death
Standard Dose 615 164 160High Dose 618 202 195
Death / MI relative risk: 1.30 (0.94, 1.79)
Besarab et al, NEJM 339:584-590, 1998: “ in incidence of thrombosis of vascular access sites”
R
Recent Experiences: Misleading Surrogates
Strategy for HbA1c 6.0 vs. 7-7.9 Target: ACCORD ↓ HbA1c vs. Suggested ↑ Mortality
Erythropoietin : Renal, Oncology ↑ Hemoglobin vs. ↑ Thrombosis & ↑ Mortality
Troglitazone : T2DM Prevention Program (DPP) ↓ HbA1c vs. ↑ Serious Hepatic Risks
Torcetrapid / Atorvastatin in CHD: ILLUMINATE ↑ HDL ↓ LDL vs. ↑ Death & ↑ CHD
Death/MI/Stroke
Muraglitazar & Rosiglitazone : Type 2 Diabetes↓ HbA1c vs. Suggested ↑ Death / Stroke / MI or ↑
MI
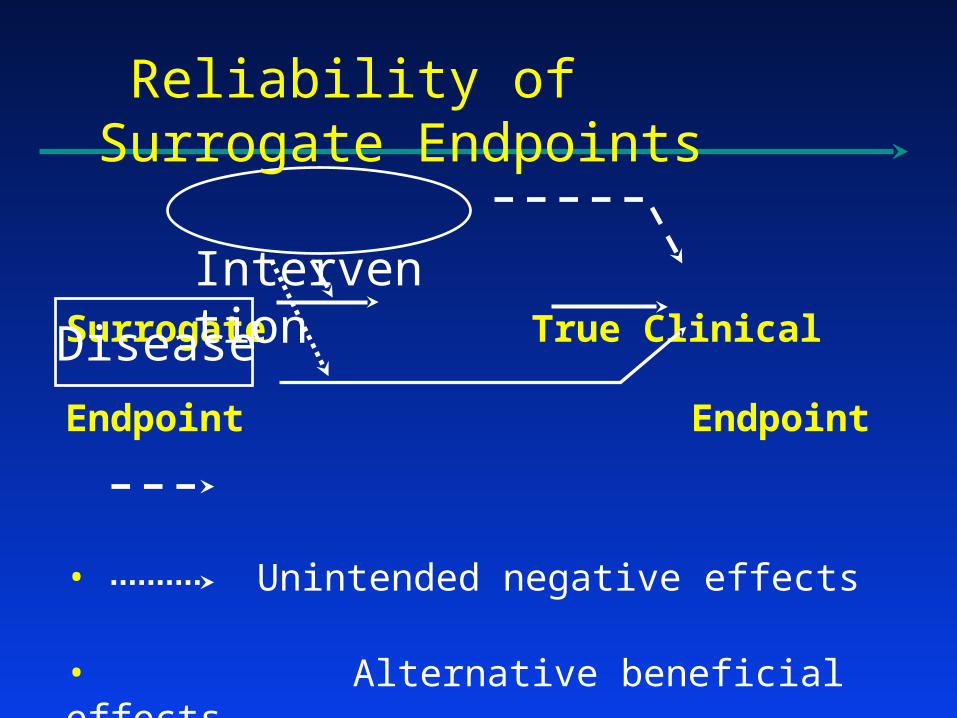
Surrogate True Clinical Endpoint Endpoint
• Unintended negative effects
• Alternative beneficial effects
Disease
Intervention
Reliability of Surrogate Endpoints
Reliable Evaluation of Benefit-to-Risk
• Surrogate Endpoints
• Validation of Surrogates
• Evaluation of Safety
• Conclusions
Validation of Surrogate Endpoints
Property of a Valid Surrogate
Effect of the Intervention on the Clinical Endpoint
is reliably predicted by the
Effect of the Intervention on the Surrogate Endpoint

Z = 0 : target 7-7.9; Z = 1 : target 6.0S(t) : HbA1c at time t
is the CVD / MI / Stroke rate
(t | Z) = 0(t) e
In ACCORD, to detect e = 0.85 with 89% power when preserving 0.025 false pos error rate,
the trial requires L = 1540 events.In turn, this requires approximately 10,000 patients, followed for approximately 5-6 years.
i.e., 1(t) = 0(t) e

Prentice’s Sufficient Conditionsto Validate a Surrogate Endpoint
1. The surrogate endpointmust be correlated with
the clinical outcome
2. The surrogate endpointmust fully capture
the net effect of treatmenton the clinical outcome

Z = 0 : target 7-7.9; Z = 1 : target 6.0S(t) : HbA1c at time t
is the CVD / MI / Stroke rate
(t | Z) = 0(t) e
(t | Z, S(t) ) = 0(t) eZ + S(t)
Proportion of net treatment effectexplained by the surrogate endpoint:
p = 1 -

Meta-analysesare required to explore
the validityof surrogate endpoints
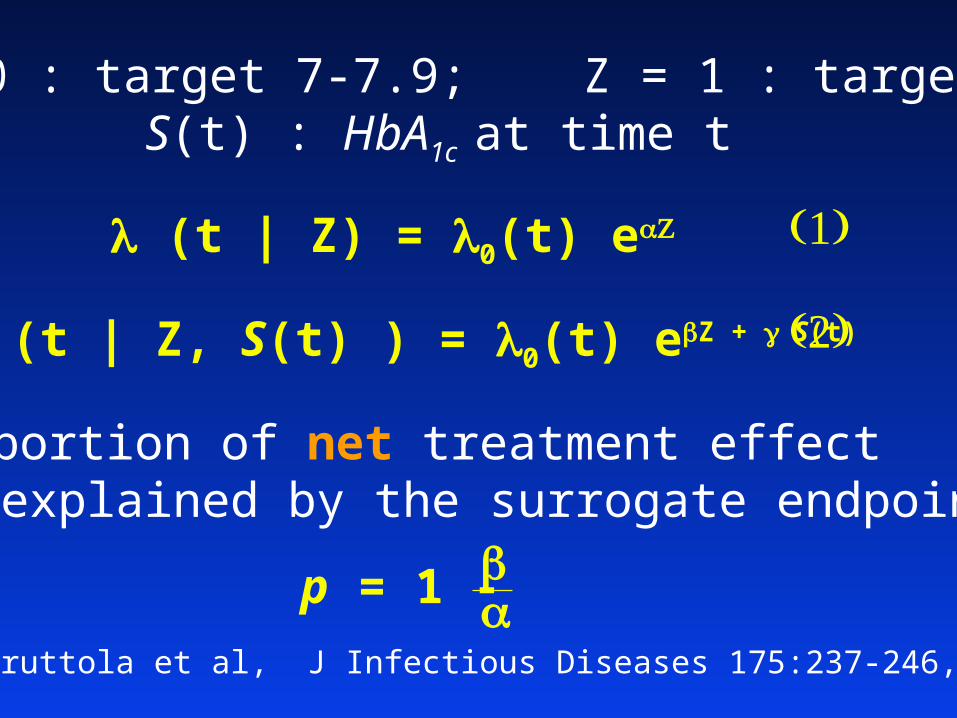
Z = 0 : target 7-7.9; Z = 1 : target 6.0S(t) : HbA1c at time t
(t | Z) = 0(t) e
(t | Z, S(t) ) = 0(t) eZ + S(t)
Proportion of net treatment effectexplained by the surrogate endpoint:
DeGruttola et al, J Infectious Diseases 175:237-246, 1997
p = 1 -

HbA1c Major Clinical Glycemic Control Events
• Unintended negative effectse.g., Hypoglycemic Events
• Alternative beneficial effects
Disease
Intervention
Validation of Surrogate Endpoints

Z = 0 : target 7-7.9; Z = 1 : target 6.0S(t) : Hypoglycemic Event at time t
(t | Z) = 0(t) e
(t | Z, S(t) ) = 0(t) eZ + S(t)
Proportion of net treatment effectexplained by the surrogate endpoint:
DeGruttola et al, J Infectious Diseases 175:237-246, 1997
p = 1 -

Validation of Surrogate Endpoints
Statistical Meta-analyses of clinical trials data
Clinical Comprehensive understanding of the
~ Causal pathways of the disease process ~ Intervention’s intended and unintended
mechanisms of action

Effects on HbA1c vs. Effects on CVD / Stroke / MI
Hypothetical Illustration
Validation across multiple Clinical Outcomes
T2DM (For an array of interventions)
• Effects on HbA1c predicting effects on:
Microvascular composite outcomes Macrovascular composite outcomes Other composites of clinical efficacy measures
Anti-Hypertensives (>500,000 patients from rand trials)FDA Cardio-Renal Advisory Committee: June 15, 2005
• Effects on Blood Pressure predicting effects on each of the following, considered individually:
Stroke, MI, CVD, Overall Mortality, Heart Failure
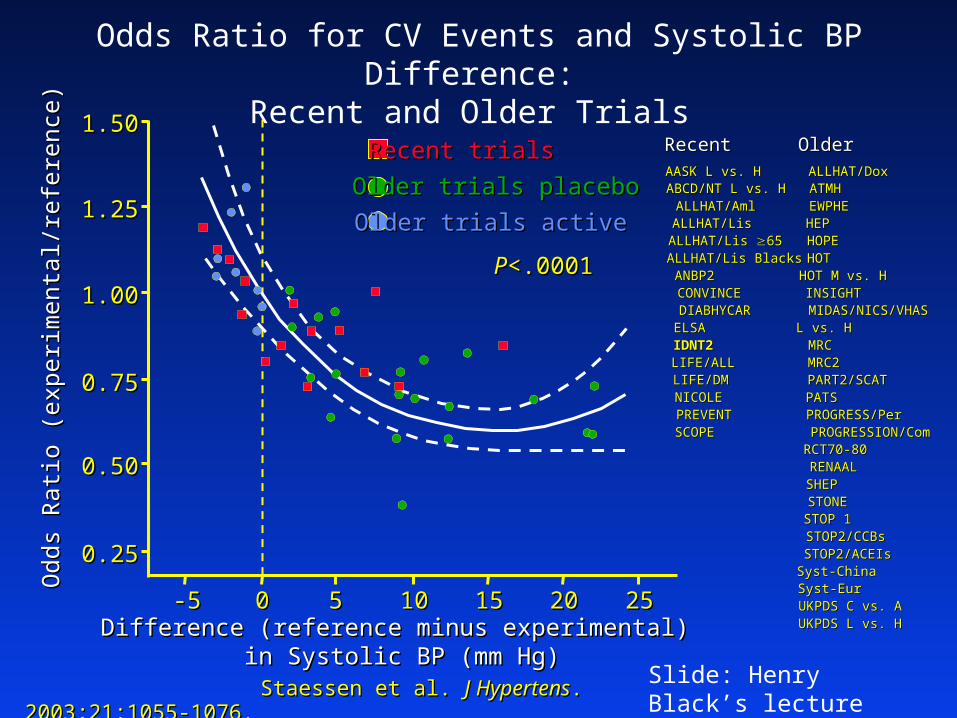
Odds Ratio for CV Events and Systolic BP Difference: Recent and Older Trials
Staessen et al. Staessen et al. J HypertensJ Hypertens. 2003;21:1055-1076.. 2003;21:1055-1076.
Odd
s R
atio
(ex
peri
men
tal/
refe
renc
e)O
dds
Rat
io (
expe
rim
enta
l/re
fere
nce)
1.501.50
1.251.25
1.001.00
0.750.75
0.500.50
0.250.25
-5-5 00 55 1010 1515 2020 2525
PP<.0001<.0001
Difference (reference minus experimental) Difference (reference minus experimental) in Systolic BP (mm Hg)in Systolic BP (mm Hg)
Recent trialsRecent trials
Older trials placeboOlder trials placebo
STONESTONE
UKPDS L vs. HUKPDS L vs. H
PROGRESSION/ComPROGRESSION/Com
STOP 1STOP 1
RCT70-80RCT70-80
EWPHEEWPHEHEPHEP
MRC2MRC2
SHEPSHEP
Syst-EurSyst-Eur
PART2/SCATPART2/SCAT
HOPEHOPE
STOP2/ACEIsSTOP2/ACEIs
ALLHAT/DoxALLHAT/Dox
UKPDS C vs. AUKPDS C vs. A
MIDAS/NICS/VHASMIDAS/NICS/VHAS
STOP2/CCBsSTOP2/CCBs
HOT M vs. HHOT M vs. HINSIGHTINSIGHT
HOTHOT
PROGRESS/PerPROGRESS/PerPATSPATS
RENAALRENAAL
L vs. HL vs. HMRCMRC
ATMHATMH
Syst-ChinaSyst-China
OlderOlderRecentRecentAASK L vs. HAASK L vs. HABCD/NT L vs. HABCD/NT L vs. H
ALLHAT/Lis BlacksALLHAT/Lis BlacksALLHAT/Lis ALLHAT/Lis 6565ALLHAT/LisALLHAT/LisALLHAT/AmlALLHAT/Aml
CONVINCECONVINCEDIABHYCARDIABHYCAR
ANBP2ANBP2
LIFE/ALLLIFE/ALL
ELSAELSA
LIFE/DMLIFE/DMNICOLENICOLEPREVENTPREVENT
IDNT2IDNT2
SCOPESCOPE
Older trials activeOlder trials active
Slide: Henry Black’s lecture
Reliable Evaluation of Benefit-to-Risk
• Surrogate Endpoints
• Validation of Surrogates
• Evaluation of Safety
• Conclusions
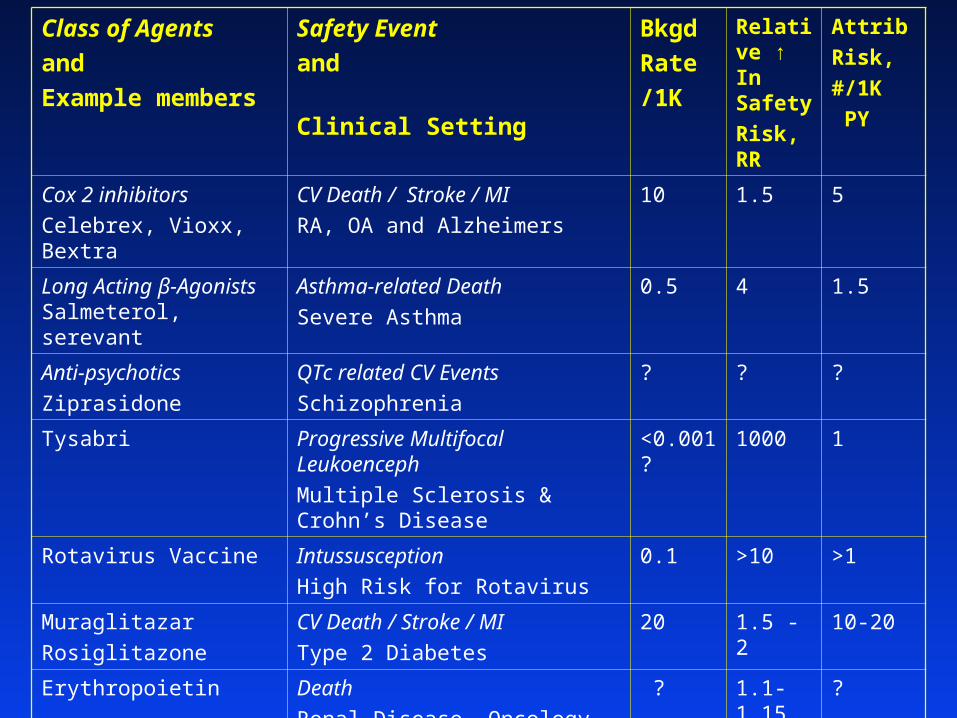
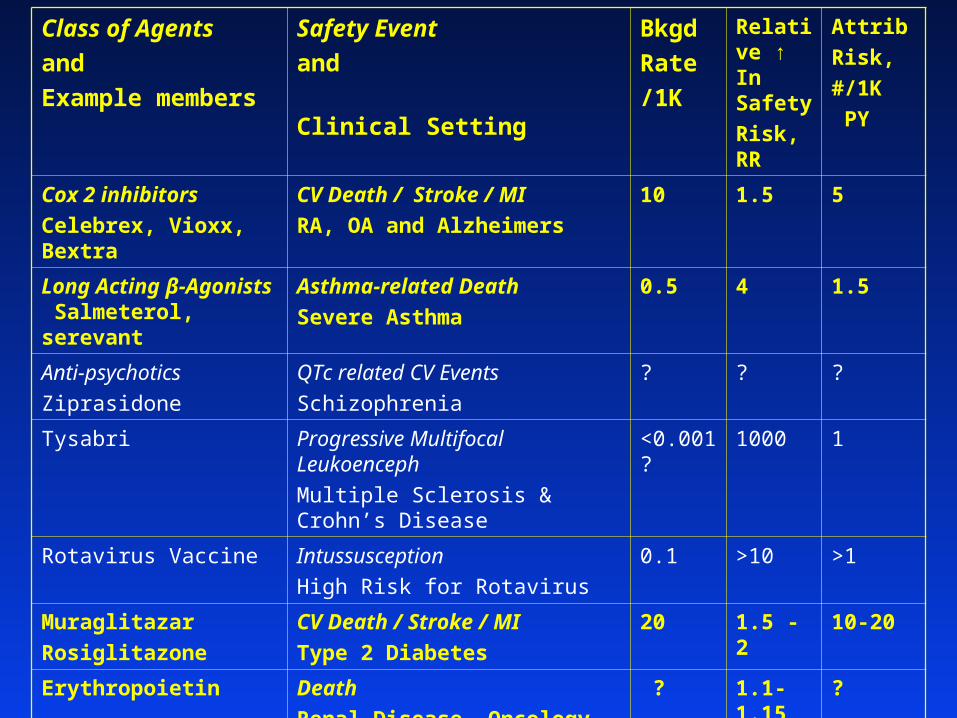
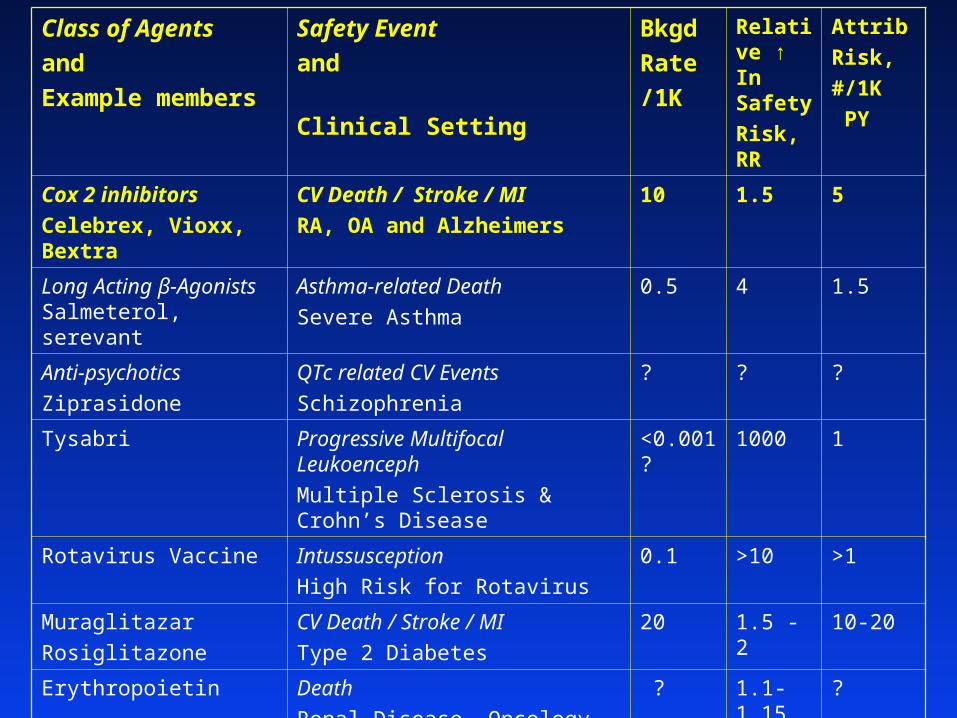
Class of Agents
and
Example members
Safety Event
and
Clinical Setting
Bkgd
Rate
/1K
Relative ↑ In Safety
Risk, RR
Attrib
Risk,
#/1K
PY
Cox 2 inhibitors
Celebrex, Vioxx, Bextra
CV Death / Stroke / MI
RA, OA and Alzheimers
10 1.5 5
Long Acting β-Agonists Salmeterol, serevant
Asthma-related Death
Severe Asthma
0.5 4 1.5
Anti-psychotics
Ziprasidone
QTc related CV Events
Schizophrenia
? ? ?
Tysabri Progressive Multifocal Leukoenceph
Multiple Sclerosis & Crohn’s Disease
<0.001? 1000 1
Rotavirus Vaccine Intussusception
High Risk for Rotavirus
0.1 >10 >1
Muraglitazar
Rosiglitazone
CV Death / Stroke / MI
Type 2 Diabetes
20 1.5 - 2 10-20
Erythropoietin Death
Renal Disease, Oncology
? 1.1-1.15 ?
ADHD Psychostimulants
Adderall, Ritalin in Adults
ADHD Drugs in Pediatrics
CV Death / Stroke / MI
ADHD Adult Setting
ADHDPediatric Setting
10
0.12
2.5
2.5
15
0.2

Primary Goal
Identifying effective interventions that are safe An important objective: Obtaining a Timely & Reliable Assessment
of Benefit-to-Risk
… Detecting long & short term risks… … Detecting rare & frequent risks…
Enabling one to rule outunacceptable increases in safety risks

Approaches to Pre- and Post-MarketingEvaluation of Safety
I Passive Surveillance Systems
II Active Surveillance Systems
III Large Randomized Clinical Trials
Surveillance for new safety signals
Exploration of existing signals

“Post Marketing” Passive Surveillance Systems
AERS: A single system for collection & analysis of reports on all serious AEs
(based on voluntary submission of MedWatch forms for AEs that caregivers believe might be drug related)
… for Safety Rare events: < 1/1000
“signal detection” … hypothesis generation requires
Large RR, or Temporal relationship

Passive Surveillance Systems
+ Timely information
+ Uniformity of reporting procedure
– Not randomized; no comparator group
– Lack of denominator
– Voluntary submission underreporting

“Post Marketing” Active Surveillance Systems
Large Prospective Cohorts & Large Linked Databases
Linking Automated Databases from HMOs 500,000 patients (e.g., Northern California Kaiser)
… for Safety• Rare events: < 1/1000

Active Surveillance Systems
+ Information on a defined population
+ Complete numerators & denominators
+ Fast & inexpensive
– Not randomized– Confounder information often unavailable– Outcome specificity
… is stated event truly an event?– Outcome sensitivity

Class of Agents
and
Example members
Safety Event
and
Clinical Setting
Bkgd
Rate
/1K
Relative ↑ In Safety
Risk, RR
Attrib
Risk,
#/1K
PY
Cox 2 inhibitors
Celebrex, Vioxx, Bextra
CV Death / Stroke / MI
RA, OA and Alzheimers
10 1.5 5
Long Acting β-Agonists Salmeterol, serevant
Asthma-related Death
Severe Asthma
0.5 4 1.5
Anti-psychotics
Ziprasidone
QTc related CV Events
Schizophrenia
? ? ?
Tysabri Progressive Multifocal Leukoenceph
Multiple Sclerosis & Crohn’s Dis.
<0.001? 1000 1
Rotavirus Vaccine Intussusception
High Risk for Rotavirus
0.1 >10 >1
Muraglitazar
Rosiglitazone
CV Death / Stroke / MI
Type 2 Diabetes
20 1.5 - 2 10-20
Erythropoietin Death
Renal Disease, Oncology
? 1.1-1.15 ?
ADHD Psychostimulants
Adderall, Ritalin in Adults
ADHD Drugs in Pediatrics
CV Death / Stroke / MI
ADHD Adult Setting
ADHD Pediatric Setting
10
0.12
2.5
2.5
15
0.2
Class of Agents
and
Example members
Safety Event
and
Clinical Setting
Bkgd
Rate
/1K
Relative ↑ In Safety
Risk, RR
Attrib
Risk,
#/1K
PY
Cox 2 inhibitors
Celebrex, Vioxx, Bextra
CV Death / Stroke / MI
RA, OA and Alzheimers
10 1.5 5
Long Acting β-Agonists Salmeterol, serevant
Asthma-related Death
Severe Asthma
0.5 4 1.5
Anti-psychotics
Ziprasidone
QTc related CV Events
Schizophrenia
? ? ?
Tysabri Progressive Multifocal Leukoenceph
Multiple Sclerosis & Crohn’s Disease
<0.001? 1000 1
Rotavirus Vaccine Intussusception
High Risk for Rotavirus
0.1 >10 >1
Muraglitazar
Rosiglitazone
CV Death / Stroke / MI
Type 2 Diabetes
20 1.5 - 2 10-20
Erythropoietin Death
Renal Disease, Oncology
? 1.1-1.15 ?
ADHD Psychostimulants
Adderall, Ritalin (Adults)
ADHD Drugs in Pediatrics
CV Death / Stroke / MI
ADHD Adult Setting
ADHD Pediatric Setting
10
0.12
2.5
2.5
15
0.2

Safety Assessments: Advantages provided by Randomized Prospective Cohorts
• Randomization removes systematically occurring imbalances in baseline characteristics
~ Pts/caregivers don’t start/stop treatments “at random” ~ Known & recorded covariates are the “tip of iceburg”
• Need to conduct an ITT evaluation Need ability to define a time 0 cohort
~ Assess risk over specified time interval, even if intervention is stopped earlier in time
~ Risk cannot be assumed to be independent of duration of exposure

Safety Assessments: Advantages provided by (Randomized) Prospective Cohorts
• Sensitivity & Specificity ~ Systematic and reliable capture of all events ~ Timely adjudication, (esp. in open label settings)
• Retention ~ Maintaining follow-up for targeted durations
• Adherence ~ Achieving proper dose and duration of use
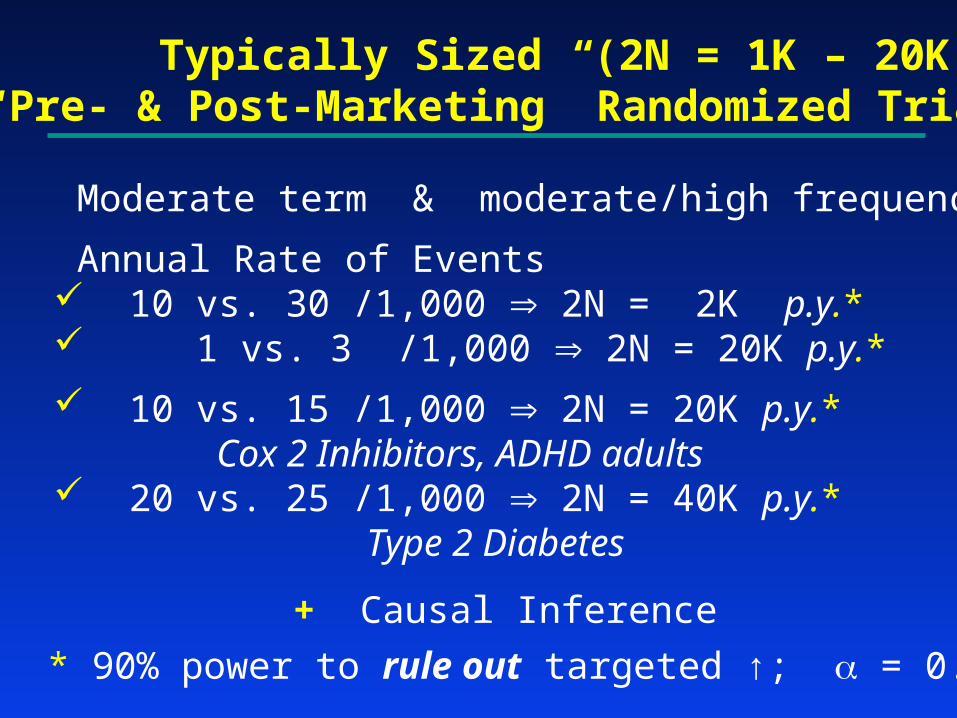
Typically Sized (2N = 1K – 20K) “Pre- & Post-Marketing” Randomized Trials
Moderate term & moderate/high frequency
Annual Rate of Events 10 vs. 30 /1,000 2N = 2K p.y.* 1 vs. 3 /1,000 2N = 20K p.y.*
10 vs. 15 /1,000 2N = 20K p.y.* Cox 2 Inhibitors, ADHD adults
20 vs. 25 /1,000 2N = 40K p.y.* Type 2 Diabetes
+ Causal Inference
* 90% power to rule out targeted ↑; = 0.025
Class of Agents
and
Example members
Safety Event
and
Clinical Setting
Bkgd
Rate
/1K
Relative ↑ In Safety
Risk, RR
Attrib
Risk,
#/1K
PY
Cox 2 inhibitors
Celebrex, Vioxx, Bextra
CV Death / Stroke / MI
RA, OA and Alzheimers
10 1.5 5
Long Acting β-Agonists Salmeterol, serevant
Asthma-related Death
Severe Asthma
0.5 4 1.5
Anti-psychotics
Ziprasidone
QTc related CV Events
Schizophrenia
? ? ?
Tysabri Progressive Multifocal Leukoenceph
Multiple Sclerosis & Crohn’s Disease
<0.001? 1000 1
Rotavirus Vaccine Intussusception
High Risk for Rotavirus
0.1 >10 >1
Muraglitazar
Rosiglitazone
CV Death / Stroke / MI
Type 2 Diabetes
20 1.5 - 2 10-20
Erythropoietin Death
Renal Disease, Oncology
? 1.1-1.15 ?
ADHD Psychostimulants
Adderall, Ritalin in Adults
ADHD Drugs in Pediatrics
CV Death / Stroke / MI
ADHD Adult Setting
ADHD Pediatric Setting
10
0.12
2.5
2.5
15
0.2

The PRECISION Trial:Ruling out Excess Rates of
CV Death / Stroke / MI
Pain Medications in Patients withOsteoarthritis & Rheumatoid Arthritis
With or at Hi Risk for CV Disease
CelecoxibIbuprofenNaproxen
R

Using the Proportional Hazards Model for the rate of “CV Death/Stroke/MI”
Naproxen : Celecoxib :
If one sets
with 1α=0.025 & power 0.90,
then L=508 events are required.
)(0 t ett )()( 01
1100 :: HH
PRECISION Trial
0:333.1ln: 10 HH

“CV Death / MI / Stroke” Events
0.84 1.00 1.12 1.19 1.333
Celecoxib better
Celecoxib compared with Naproxen
Naproxen better
Hazard Ratio (Celecoxib / Naproxen) Based on analysis at L=508 Events
A
B
C
D
CEL: superior
CEL: ruling out unacceptably inferior
CEL: neither ruling out to be unacceptably inferior, nor establishing as inferior
CEL: inferior

Performance Standards in Non-inferiority Safety Trials
Enrollment Rate need timely result
Target Population / Ineligibility Rate / Event Rate need to address settings where excess risk is most plausible need sufficiently high risk to achieve targeted number of events
Adherence must at least match adherence in prior trials with safety signal include frequency/timing of withdrawal from rand. treatment
Cross-ins minimize by: careful screening; educating caregivers & patients
…Very challenging in a post-marketing setting… Retention
critical to maintaining integrity of randomization
Reliable Evaluation of Benefit-to-Risk
• Surrogate Endpoints
• Validation of Surrogates
• Evaluation of Safety
• Conclusions

Consequences of Reliance on Surrogate Endpoints For Accelerated or Full Regulatory Approval
Less reliable evidence regarding Efficacy
Less reliable evidence regarding Safety
…The stronger the efficacy evidence , the greater the resilience regarding uncertainties about safety…
Recent Experiences:
• Tysabri : PML in Crohns Disease & Multiple Sclerosis
• Erythropoiesis Stimulating Agents : Chemo-Induced Amemia & Hemodialysis in
CHF
• Muraglitazar & Rosiglitazone : Type 2 Diabetes
Goals in Development of Interventions in Diabetes
• Achieving an efficient evaluation of experimental interventions… possibly with the use of biomarkers
• Achieving reliable as well as timely evaluation of both safety and efficacy
of new interventions
• Providing patients and care-givers not only a choice, but an informed choice