Embed Size (px)
DESCRIPTION
Religious care in a multi-cultural world – lost or leading?. We’re here and we’re not going away! Jim McManus UHB Chaplaincy Study Day January 2010. Rainbow or Vegetable Puree?. Homogenised. Government Policy. Chasing the rainbow or the Holy Grail? This has implications for NHS Trusts - PowerPoint PPT Presentation
Citation preview
Religious care in a multi-cultural world – lost or leading?
We’re here and we’re not going away!
Jim McManus
UHB Chaplaincy Study Day January 2010
Rainbow or Vegetable Puree?
Homogenised
Government Policy Chasing the rainbow or the Holy Grail?
This has implications for NHS Trusts This has implications for social care There are implications for Chaplaincy
Although everyone knew where the Chaplaincy was....

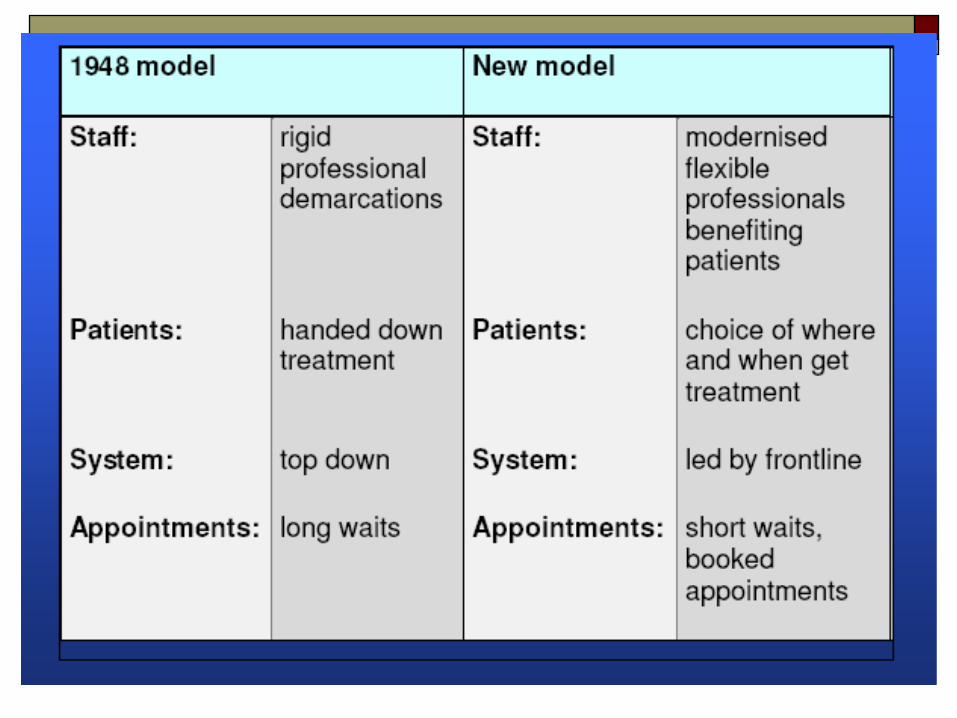
Change in healthcare systems
Current Health Policy Directions Current Health Policy
The drive towards personalisation The drive towards instrumentalisation The drive towards professionalisation The Evidence based agenda
Chaplaincy going the wrong way? Personalisation or vegetable puree? One size DOES NOT fit all “Units” of spiritual care
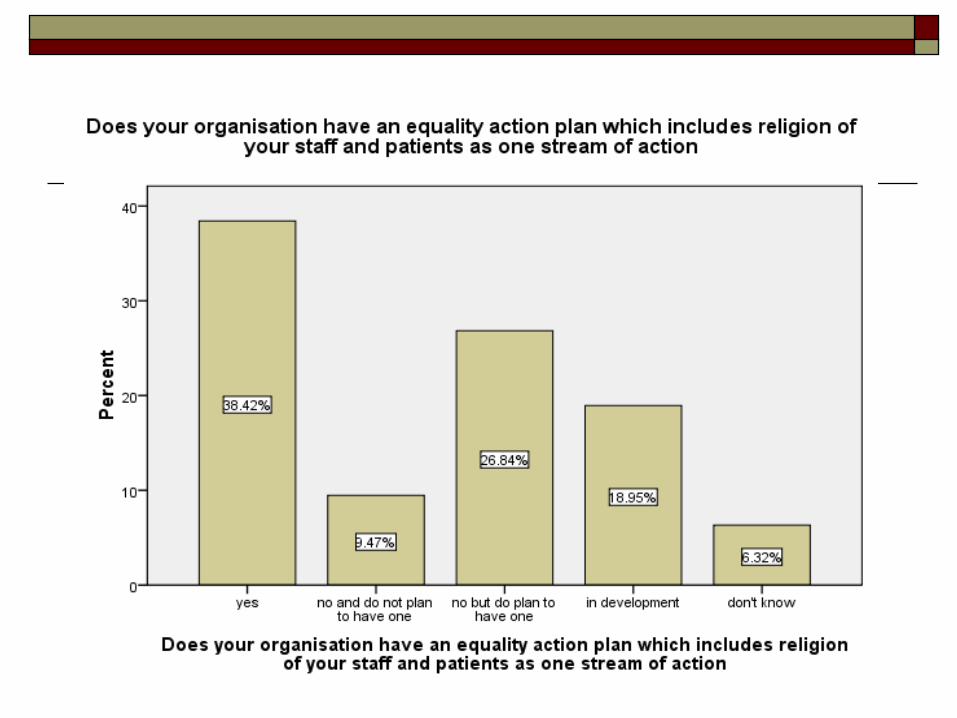
Diversity Policy Duties of NHS Trusts Confusion The homogenisation agenda for Diversity is
doomed! Hooks for Chaplaincy
Personalisation Covenant Rights – Safeguarding Single Equality Scheme Making Religious Diversity work for your trust

Making Chaplaincy an Intervention What kind of intervention? Will you lose in a battle with psychologists? Where’s the evidence? Why would you want to be a “talking”
intervention?
Question Is the only reason Chaplaincy teams are still
provided because Chief Executives haven’t worked out psychologists would be cheaper, provide better evidence and more easily assessable outcomes?
AND/OR Is the only reason Chaplaincy teams are still
there is because Trusts are frightened of religion? (CBCEW Survey, 2008)
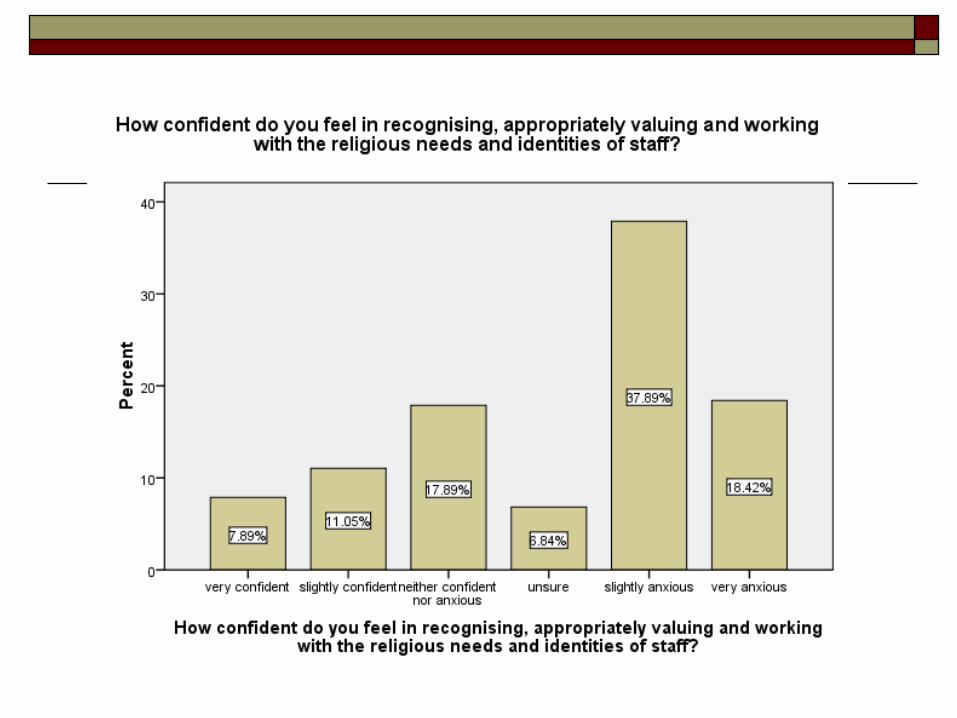
Why? 57%) felt anxious in trying to recognise and work with the
religious needs of staff. This became a focus for the telephone interviews The most common responses from telephone interviews were
a) staff working on diversity did not feel knowledgeable about or comfortable with faith (35 of 50),
b) staff did not want to cause offence (43 of 50) and staff were often unaware of the make up of faiths in their area (38 of 50.)
19 respondents specifically said there was some hostility to dealing with religion from colleagues whereas
23 stated that the issue was repeatedly deprioritised because “it’s in the too difficult box.”
20 said lack of government guidance was salient
Professionalising or Competence-ising? Registers Faith Community
connections lost? A body of professional
practice which is distinct from..well what exactly?
Licensing spirituality which is so vague as to be indefinable
Refugees from faith communities? (Chris Swift)
Key Competencies Boundaries and Limits Reflexivity and Power Personalisation Leadership models Use psychology, don’t try
to be psychologists or counsellors…

Do chaplains feel left out?

Chaplains as Pastors The five functions of pastoral care
Healing Guiding Nurturing Reconciling Discipline
The sixth function - personalisation
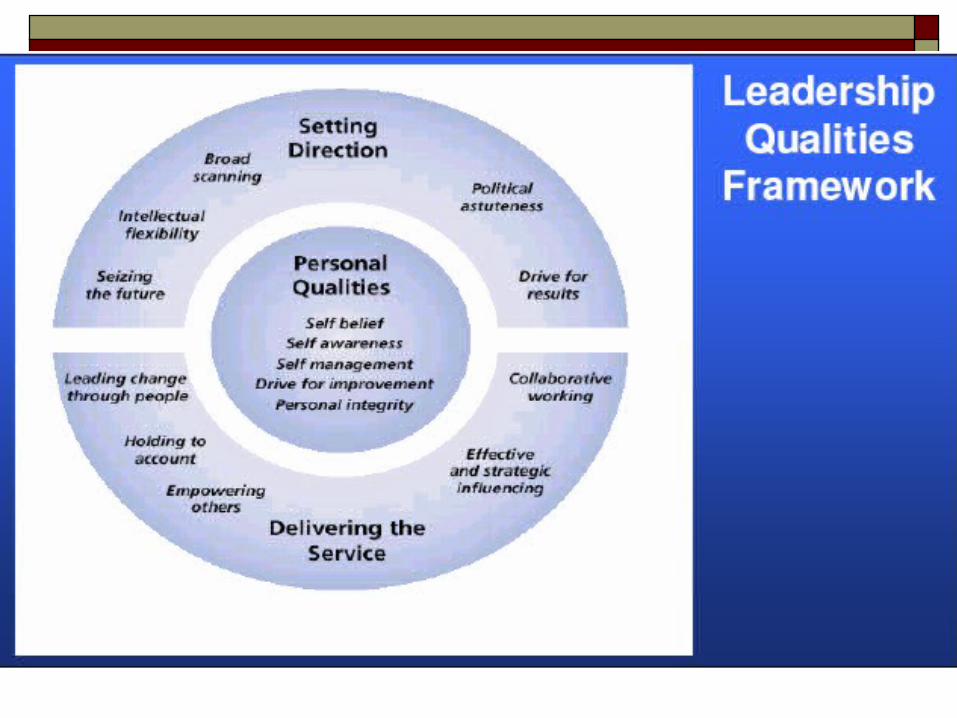
Chaplains/ as Invitational Leaders
Invitational Leadership: Improving the atmosphere and message sent out by
the organisation Focus on reducing negative messages
sent out through the everyday actions of the business both externally and, crucially, internally
Review internal processes to reduce these Build relationships and sense of belonging and
identity with the organisation – that gets communicated to customers, etc.
Evidence
Some initial thoughts…
Some thoughts on research It isn’t that evidence doesn’t exist, it’s that we
don’t train people to find, appraise and use it It isn’t that quantitative designs are not
organic, it’s that using numbers and discourse together tells us more about the world
The state of the evidence base is a function of the state of UK and Irish social science....
Evidence
Evidence for faith communities impact (Health/Care Specific) Mark J. DeHaven, Irby B. Hunter, Laura Wilder, James W. Walton, and Jarett Berry,
(2004) American Journal of Public Health. June; 94(6): 1030–1036. Health Programs in Faith-Based Organizations: Are They Effective?
Helen Rose Ebaugh , Paula F. Pipes , Janet Saltzman Chafetz & Martha Daniels (2003) Where's the Religion? Distinguishing Faith-Based from Secular Social Service Agencies. Journal for the Scientific Study of Religion. Volume 42 Issue 3, Pages 411 – 426
A Social Policy Role for Faith-Based Organisations? Lessons from the UK Jewish Voluntary Sector
HARRIS, HALFPENNY, and ROCHESTER (2003) A Social Policy Role for Faith-Based Organisations? Lessons from the UK Jewish Voluntary Sector . Journal of Social Policy , 32 : 93-112
Flannelly,; Weaver,; Tannenbaum, (2005) What Do We Know about the Effectiveness of Faith-based Health Programs? Special Section Southern Medical Journal. 98(12):1243-1244, December 2005.
More Evidence
http://www.manhattan-institute.org/html/crrucs-obj_hope.htm

Evidence 5
http://aspe.hhs.gov/fbci/comp08/report.pdf - US govt report on “Innovations in Effective Compassion”
Centre for Research on Religion and Urban Civil Society http://www.sas.upenn.edu/prrucs/research.html
Children
Book chapter by JohnsonIn Authoritative Communities – The Scientific case for nurturing the whole ChildEdited by Kathleen K Kline (2007). New York: Springer
Kairos or Crisis? Chaplaincy can go in two directions
Continue professionalising and homogenising Continue its existing tradition of personalising
and start demonstrating its value and contribution as a rainbow, not as a vegetable puree?
Where to now then? Health Policy – cyclical hooks for Christian
witness and presence Secularism and Response Public Theology or Professionalisation?
(Foucault just won’t die, will he?) A theology of pastoral presence in health? Some challenges
Hallmarks of Chaplaincy in a multi-cultural world Invitational Corporate and personal
Corporate – supports the Trust respect diversity and safeguard patient and staff rights
Personal – provides a core of care and recognises limits and boundaries as part of personalisation – this WILL challenge a one size fits all approach
Journeying Competent in appropriate use of various disciplines A locus for all faith groups to work together Dialoguing with other diversity strands Educating and empowering staff to address spiritual need Healing, Guiding, Nurturing, Reconciling and Disciplining

Value of Chaplaincy to NHS Trusts in a multi-cultural world The Gestalt argument
More than interventions Quality of patient experience Quality of staff experience Helps provide and retain compassion and values in health care Does things and is available in a way other “helping professions” cannot be Staff development and practice – addressing spiritual need Clinical Governance – supporting practice around these areas
Invitational Leadership for Staff and Patients A source of expertise on genuine diversity of faith work and provision Personalisation, not homogenisation Corporate and personal
Corporate – supports the Trust respect diversity and safeguard patient and staff rights Personal – provides a core of care and recognises limits and boundaries as part of
personalisation – this WILL challenge a one size fits all approach Competent in appropriate use of various disciplines Dialoguing with other diversity strands

synthesis of the Gospel Proposal: The Good Samaritan
Grounded in reality: looks at the wounded
Sharing: he moves and gives of himself
Heal: pouring oil and wine
Gives of his own resources: collocates the wounded in his horse
Goes to competent people : the master
Spends his money: two denari.
Without limits, generosity, if something lacks...
Tests the results: when I come back...
Lk 10,25-37Lk 10,25-37

BENEDICT XVI:
Renewal and deepening of the pastoral proposal in Health Care
that take into account the growing mass of knowledge spread by the media, and the higher standard of education of those they target.
Formation of conscience deep and clear in order to ensure that every new scientific discovery will serve the integral good of the person, with constant respect for his or her dignity.
To have advisers trained and competent.
ContinuedUpdating the training
of pastors and educators to enable them to take on their own responsibilities in conformity with their faith, And at the same time in a respectful and loyal dialogue with non-believers,is the indispensable task of any up-to-date pastoral health care.
To guarantee a prompt response to the expectations by each individual of effective help.To study proper methodology
to bring help to persons, to the families and to the society. in order to ensure an incisive presence of the Church at the pastoral level
To combine loyalty and dialogue.theological deepening and the capacity of mediation
From the address of Benedict XVI to the Participants at the 20° International Conference Organized by the Pontifical Council for Health Pastoral Care on the Theme of the Human Genome, November 19, 2005.
Human Ecology...an unexplored concept? Centesimus Annus
In addition to the irrational destruction of the natural environment, we must also mention the more serious destruction of the human environment…too little effort is made to safeguard the moral conditions for an authentic ‘human ecology’…..in this context, mention should be made of the serious problems of modern urbanization, of the need for urban planning which is concerned with how people are to live, and of the attention which should be given to a “social ecology” of work (next slide discusses these principles and application in PH work)
A Manifesto for Keeping Faith
… while professional competence is a primary, fundamental requirement, it is not of itself sufficient. We are dealing with human beings, and human beings always need something more than technically proper care. They need humanity. They need heartfelt concern.
Those who work for the Church's charitable organizations must be distinguished by the fact that they do not merely meet the needs of the moment, but they dedicate themselves to others with heartfelt concern, enabling them to experience the richness of their humanity.
Consequently, in addition to their necessary professional training, these charity workers need a “formation of the heart”: they need to be led to that encounter with God in Christ which awakens their love and opens their spirits to others.
As a result, love of neighbour will no longer be for them a commandment imposed, so to speak, from without, but a consequence deriving from their faith, a faith which becomes active through love (cf. Gal 5:6).
Deus Caritas Est, 31
The Strategist’s Theorem, a manifesto for change.
DSQ – Dissatisfaction with the status quo
CD – Clear Direction
CNS – Clear next steps
INS – Immediate next steps
EC=DSQ + CD + CNS + INSEC=DSQ + CD + CNS + INS
Rainbow or Vegetable Puree?
Homogenised
Chasing the rainbow….
Chasing the Rainbow…some principles 1
1. Ensure you acknowledge and point to the workforce research evidence on religion to underpin your strategy
2. Ensure your Policy addresses religion in the workplace in a way which values it as well as protects you from discrimination claims
3. Run a “Doing business with Religion” Seminar or another seminar like it

Chasing the Rainbow…some principles 2
4. Make sure you consult faith communities in developing your Single Equality Scheme
5. Learn from what other NHS organisations have done successfully for the organisation and their workforce and apply the schemes (page 9ff)
6. Learn from what other NHS organisations have done successfully for their patients
7. Benchmark your agency against others

Contact MeJim McManus, BD(Hons), CPsychol,CSci, FFPH, AFBPsS, FSA Scot, MEPS
Joint Director of Public Health
Birmingham Health and Wellbeing Partnership
Suite 203, CIBA Building
146 Hagley Road
Birmingham B16 9NX
Tel 0121 465 2966