Embed Size (px)
Citation preview

Europ. J. clin. Invest . 6, 299 - 305 (1976)
Removal of Exogenous Plasma Triglycerides in Forearm Muscle and Subcutaneous Tissue of Hyper- and Normotriglyceridaemic Men S. Rossner, B. Eklund, L. Kaijser, A.G. Olsson and G. Walldius
King Gustaf V Research Institute, Departments Of Internal Medicine and Clinical Phy- siology, Karolinska Hospital, Stockholm, Sweden
Received: December 24, 1975, and in revised form: February 20, 1 9 7 6
Abstraci
Absolute arterio-venous removal and fractional removal of blood-borne exogenous trigly- ceride particles by skeletal and subcutaneous tissues were determined in eight normo- triglyceridaemic and six hypertriglyceridaemic men. Estimations were made by sinul- taneously sampling blood from catheters inserted into a brachial artery, and in the distal direction, into a superficial and deep vein, draining subcutaneous tissue and skeletal muscle respectively. During the infusion of the fat emulsion IntralipidR for 3 hours steady arterial concentrations of exogenous TG particles were found, indicating first order kinetics.
In all subjects absolute arterio-venous and fractional removal of triglycerides were about twice as high in skeletal muscle as in subcutaneous tissue. In skeletal muscle the fractional removal and absolute removal were significantly higher in normotriglycerid- aemic than in hypertriglyceridaemic subjects (p < 0.001). No decrease in removal with time was observed, which would have suggested saturation of removal sites. Mean frac- tional removal in skeletal muscle was significantly correlated with the k2 value deter- mined by an intravenous fat tolerance test before the infusion study (r = 0.61, p < 0 . 0 5 ) . In subcutaneous tissue fractional removal was also significantly higher in normotriglyceridaemic subjects (p < 0.05).
The results suggest that in both skeletal muscle and subcutaneous tissue the removal system is impaired in hypertriglyceridaemic subjects. This finding supports the concept that a decreased elimination capacity in these tissues may partly account for triglyceride elevation in hypertriglyceridaemic subjects.
Key words
Intravenous fat tolerance test, Hypertriglyceridaemia, Plasma triglycerides, Skeletal muscle, Subcutaneous tissue, Triglyceride removal
Introduction
Previous studies of the removal from blood of an infused fat emulsion, Intra- lipidR, have demonstrated that human heart (1) and skeletal muscle ( 2 ) are both capable of removing substantial amounts of such exogenous fat particles. During a continuous infusion of a fat emulsion for four hours fractional re- moval by the heart muscle was found to be 5.5 percent. Assuming a normal cor- onary blood flow, about 1 4 % of infused Intralipid fat would have been taken up by the heart. If the average fractional
removal by muscle tissue in the whole body was similar to that of the forearm it has been calculated that skeletal muscle would remove almost 50% of an infused fat emulsion ( 3 ) . No signifi- cant further removal of triglyceride (TG) particles could be demonstrated during dynamic forearm work.
Almost half of an infused amount of Intralipid seems to be initially re- moved by skeletal muscle and an impaired removal of Intralipid, as shown by the intravenous f a t tolerance test ( I V F T T ) is found in subjects with hypertrigyl- ceridaemia (HTG). Therefore it is of

3 00 S . Rijssner e t al.: Trig lycer ide Removal i n Hypertrigylceridaem.ia
interest to determine if the skeletal muscle removal of exogenous TG in HTG subjects differs from that in normo- triglyceridaemic (NTG) subjects. Adipose tissue is another important removal site for circulating TG ( 2 , 6 ) and by sampling from a superficial as well as a deep forearm vein, the removal of TG by sub- cutaneous tissue can also be studied.
The object of the present study was ( 1 ) to determine if exogenous TG is re- moved by both skeletal muscle and sub- cutaneous tissues of the forearm during longer infusion periods and ( 2 ) to study whether the impaired fractional removal of Intralipid in HTG, as determined by the intravenous fat tolerance test, could be due to a decreased ability of skeletal muscle and/or subcutaneous tis- sues to remove exogenous fat particles from the circulation.
Subjects and Procedures
Eight healthy men with normal serum lipids and six healthy men with HTG were studied. All subjects were selected from a health control centre where lipid values were screened ( 7 ) . The eight NTG men were between the ages of 43 and 56 years. At the time of the study their serum TG concentration ranged from 0 . 5 2 to 1 . 3 0 mmol/l. The six HTG subjects (age 3 9 to 48 years) had been found to have elevated serum TG concentrations on several screening tests. At the time of the study the serum TG concentrations ranged from 2.44 to 5.31 mmol/l. The mean body weight was for NTG men 79 5 3 kg (SEMI and for HTG men 7 4 2 3 kg (N.S.). The corresponding Broca indexes [weight (kg) / height (cm) - 1001 were 1 . 0 5 ? 0 . 0 2 and 0.99 c 0.02 (N.S.). No subject gave a history of metabolic disease, had symptoms suggestive of metabolic dis- order or recent illness or was on any medication expected to affect lipid metabolism.
In all subjects an intravenous fat tolerance test was undertaken. NTG sub- jects had k2 values ranging from 3 .7 to 5.8 %/min., mean 2 SEM was 4 .7 5 0.3 %/ min. In HTG subjects k2 varied from 1 . 2 to 5 .4 %/min., the mean value being 3.3 2 0.5 %/min. The difference between NTG and HTG k2 values was significant ( p < 0.05).
HTG and NTG subjects TG removal was studied in forearm tissues at similar arterial concentrations in all subjects. Since HTG subjects have been shown to exhibit impaired removal of fat partic- les from plasma ( 3 ) , the Intralipid in- fusion rates were selected with regard
To facilitate the comparison between
to the serum TG concentrations and IVFTT k2 values. Thus the infusion rates were varied between 0 . 6 5 and 1.15 ml/min.
The design of the study has previously been described in detail ( 2 ) . The sub- jects were studied in the supine position after an overnight fast. Teflon cath- eters were inserted into a brachial artery, and, in the distal direction into one deep (dv) and one superficial (sv) antebrachial vein. The dv catheter was introduced until the tip could no longer be palpated, usually 5 - 8 cm. The distance it had been introduced was checked again when the catheters were withdrawn after the study. During blood sampling the hand circulation was oc- cluded by a wrist cuff. Under these con- ditions the deep vein almost exclusively drains the forearm muscles ( 8 ) . The su- perficial vein mainly samples blood from the skin and subcutaneous tissues of the forearm and the hand ( 8 ) . A 10 % Intralipid emulsion was infused into another catheter which had been advanced from an antebrachial vein to the axil- lary vein. After a bolus dose of 4 0 ml it was infused at a constant rate. The catheters were kept patent by saline, and heparin was not used. Blood for nephelometric determinations of arterio- venous (a-v) differences of exogenous TG was drawn after 20, 30, 60, 120 and 1 8 0 minutes of infusion simultaneously from the artery, the deep and the super- ficial veins. Before the start of the Intralipid infusion 5 - 8 uC 1251-label- led-albumin was given intravenously (iv) in order to detect any possible concen- tration changes of plasma water.
Methods
Fasting arterial serum TG and cholest- erol concentrations were determined by Technicon Auto-Analyzer methods (9 , 10) . Blanks for nephelometry were sampled from the.artery, the deep and the super- ficial vein. Blood was drawn simultan- eously from these catheters into dry syringes, and transferred into plastic tubes containing lyophilized heparin and placed into ice water. Samples for nephelometry were centrifuged twice at 600 g/min. From each sample 5 0 ul of plasma was diluted 1 :lo0 in ten repli- cates. The light scattering index of each sample was determined by a Thorp micronephelometer ( 1 1 ) . The samples were read in a random order. The blank value was subtracted from the light scattering index, and then the light scattering index was converted to umol exogenous TG/1 by means of a standard curve and an assumed molecular weight of 878 for Intralipid TG.

s. Rossner et a l . : Triglyceride Removal in Hypertriglyceridaemia 3 0 1
Four to eight 0 . 5 ml plasma samples from the same tube as used for nephel- ometry were taken for countin and sub- sequent determination of the q25~-label- led-albumin concentration in plasma.
Results
Unless otherwise stated values in the text are given as mean t SEM.
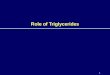
In 5 out of 8 NTG subjects and 4 out of 6 HTG subjects the infusion rate of Intralipid was 0.91 ml/min. In 3 out of 8 NTG subjects with the lowest fasting serum TG concentration 1.05 - 1 .15 ml Intralipid/min. was given and in the two HTG subjects with the highest fasting TG concentration 0.65 ml Intra- lipid/min. was infused. Fairly steady Intralipid concentrations were obtained in most NTG and HTG subjects (Fig. 1). In two HTG subjects (no 1 1 and 12) an increase in concentration of exogenous TG particles was observed with time. However, in both these subjects the arterial concentration tended to reach a plateau level. In one NTG subject the exogenous TG concentration decreased continuously after 60 minutes. The mean arterial concentration during the in- fusion period was 712 c 47 pmol/l in the NTG subjects and 1151 t 89 p r n o l / l in the HTG subjects (p < 0.001).
did not differ systematically between artery and veins. However, in 6 out of 7 8 paired arterial and venous samples a statistically significant concentration difference in either direction was ob- served. Correction for these differences were made but they did not significantly affect the mean arterio-venous concen- tration differences of exogenous TG.
1251-labelled-albumin concentrations
A-v Differences of Exogenous TG
There was no systematic arterio-venous difference in nephelometric background before the infusion of Intralipid. In NTG subjects a statistically significant removal of Intralipid was found in 38 out of 3 9 paired a-dv samples (Table 1 ) . The mean a-dv concentration difference was 48 +- 2 pmol/l, which corresponds to a fractional removal of 7 . 7 t 0.7 % of the arterial concentration. The frac- tional.remova1 increased with time and was significantly higher at 180 min. than at 20 min. ( p < 0.05) . Since at the same time a slight but insignificant decrease in Intralipid TG concentration occurred, there was no significant change in a-dv concentration difference with time.
Significant positive a-dv venous concentration differences of fat partic- les were found in 16 out of 25 paired samples in HTG subjects (Table 1 ) . A significant release was not found in any case. The mean a-dv difference was 36 2 4 umol/l which corresponds to a fractional removal of 3.4 f 0.7 % of the arterial concentration.
difference (p < 0.05) and the mean frac- tional removal (p < 0.001) were lower in HTG than in NTG subjects.
ences were found in 20 out of 30 paired samples from NTG subjects. In 9 out of 30 samples no significant removal could
Both the absolute a-dv concentration
Significant a-sv concentration differ-
..
i I + - > > I I I I
120 180 rnin 2 0 & 6 0
Fig. 1. Arterial concentrations of exogenous plasma TG during constant infusion with Intra- lipidR in hyper- and normotriglyceridaemic men
%
* O l
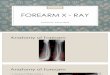
x x = NTG .o .P * x X * = HTG
r = 0.61 - 0 * I . p < 0.05
I
5 10 K 2 %/min
Fig. 2. Relationship between mean fractional extraction of exogenous TG in skeletal muscle and IVFTT k2 value
I

Table 1. Individual values for arterial concentrations (a) and concentration differences of exogenous
subjects 20 min. 30 min. number
a a-dv % of a a a-dv % of a
normotriglyceridaemia 1
2
3
4
5
6
7
8
X i. SEX -
68028
48223
123425
75727
92057
59526
101426
42026
763298
282 13"'
1227 ** 41f9***
5821 3***
3428 *** 3627 *** 59ir9 *** 5727 ***
*** 4126
hypertriglyceridaemia 9 133829 13t13nS
10 157629 89212***
11 133227 36210**
12 96326 72214 *** 13 51523 1724***
14 827i.3 1624 *** r( ? SEM 10922160 41513***
4.1
2.5
3.3
7.7
3.7
6.1
5.8
13.6
5.9+1.3***
6562 13
426?5
126225
733210
95124
5 502 7
101524
368C6
7455110
46218*
2527***
34211
87+16***
2927 *** 5 42 1 O***
52+11***
42k9 *** 4627 ***
**
1 .o 1403511 27212*
5.6 159657 14929***
2.7 1353210 27212 * 7.5 973214 - 3.3 525t3 1124 *** 1.9 65426 329
3.721 .O*** 1084f178 43ir27ns
ns
7 .O
5.9
2.7
11.9
3 .O
9.8
5.1
11.4
7.121.3***
1.9
9.3
2.1 - 2.1
0.5
3.221.6 ns
Table 2. Individual values for arterial concentrations (a) and concentration differences of exogenous Mean t SEM are given in umol/l. Statistical symbols as in Table 1
- subjects 20 rnin. 30 min. number
% of a a a-sv % of a a a-sv -
norm0 tr igly cer idaemi a 1
2
3 123425 40210***
4 75727 25f9**
- - - -
5 92027 527ns
6 595C6 -428"'
7 101426 70+8 *** 8 42026 -2928 ***
ns x 2 SEM - 18214
hypertriglyceridaemia ns 9 133829 -4+10
10 157629 77kll***
1 1 133227 31?12*
12 96326 56222 *** 13 - - ? 2 SEM - 40217nS
- - 3.2
3.3
0.5
-0.7
6.9
-6.9
1.121.9 ns
, -0.2 4.9***
2.3
5.8 -
ns 3.2k1.4
- -
126225
733210
951k4
55w7
1015f4
36856 -
1403211
159627
1353f10
973214 - -
- -
1721 2"'
3 42 10 *** 3225 *** 4129 *** 54212***
ns -11t9
28f9 *
21k1 zns ns 52 9
82 1 2ns
1 1225ns -
1 If3 *
- -
1.3
4.6
3.4
7.5
5.3
-3 .O
3.2f1.5*
1.5
0.0
0.6
0.1 -
ns 0.6f0.3
-
= p < 0.01, *** = p < 0.01. The statistical evaluation is based ns = no significance, * = p < 0 . 0 5 , **

plasma TG,determined by nephelometry, between a r t e r y and deep v e i n (a -dv) . Mean t SEM a r e g iven i n pmol/l
60 rnin. 120 rnin. 180 rnin.
a a-dv % of a a a-dv % of a a a-dv % of a
670?6
41823
1300213
665+6
99823
42724
106324
35424
7362123
- 165323
1573f9
1120216
47427
7 1627
11072231
3827*
36t4 *** 46219 * 3428 *** 3327 *** 7326 *** 7322 *** 57514 *** 4926 ***
- 79210***
46212 *** -
ns -828
3328 *** 382 1 8"'
5.7 63926
8.6 33153
3.5 102227
5.1 60626
3.3 103122
17.9 39553
6 .9 112224
16.1 345+2
8 .4~2 .0*** 687r i16
- 134555
4.8 160826
2.9 1867-+10
- 1343217
-2 36924
4.6 71129
2.621.6 12072230 ns
3129**
1624 *** -
64210 *** 9425 *** 1426 *
11823 *** 1926 *** 51216***
4 . 9
4 .8
- 10.6
9.1
3.5
10 .5
5.5
7.0+1.3***
69027
3a5+3
688510
595+9
934+9
35226
103522
33626
627293
n s 62 6 0.4 167925
88210*** 5.5 150927 n s
1898210
- - 1506221
1214 0.1
-556"' -1.4 44523
15+1lnS 2 . 1 55228
21217 ns 1.321.2 ns 1265t250
7328 *** 4054 *** 4021 1 *** 70214***
81210***
47+8***
4222 *** 47_+9***
5SC6***
ns -729
962 1 2*** n s 7214
- 5924 *** 41Cll***
38215 ns
10.6
10.4
5.8
11.8
8.7
13.4
4.1
14.0
9.9+1.2***
-0 .4
6 .4
0 . 4
- 13.3
7.4 ns 5 .4 t2 .5
plasma TG, de te rmined by nephelometry, between a r t e r y and s u p e r f i c i a l v e i n ( a - sv l .
60 min. 120 min. 180 min
% of a a a-sv % of a a a-sv a a-sv % of a
- -
1300213
66526
99823
42724
106354
354?4
-
- 165323
157329
1120216
- -
- -
59216***
92Bns
13+4*
5525 *** 49+3 *** 29214*
3629 *
- -3.29 ***
n s 3 5 t l 2 ***
-10226 -
-8225ns
- -
4.5
1.4
1 .3
15 .5
4.6
8.2
5 -922.2 *
- -3 .O ***
2 . 2
-0.1 -
ns -0.221.5
- -
102227
60626
103122
395c3
11 2224
34522
-
134525
160826
18672 10
1343217
- -
- n s
n s 829
157
2624***
3427***
8725 *** 16+7*
292 13"'
- 0.8
0 .2
2 .5
8 .6
7 .8
4 .6
4.121.4*
n s -429 -0.4
4829*** 3 .O
30t15* 1 . 6
0 ns 0224
- - ns 19+ 12"' 1.120.8
- -
688210 50211 *** 595t9 1329
ns
93429 37+4**
1035t2 2122 *** 352k6 4426***
ns 33626 -1 329
- 25210*
n s 1679+5 -127
1502+7 55217 ** 1898t10 -92 16
1506221 10230
n s
ns
- - n s . - 14214
- - 7.3
2 . 2
4.0
12.5
2 .o -2.9
4.222.1 n s
0.0
3.7**
-0.5
0.1
- n s
0.8c-1 .o
on t h e t es t of d i f f e r e n c e between means.

3 94 S. RBssner et al.: Triglyceride Removal in Hypertriglyceridaemia
be demonstrated and in one pair a sig- nificant release was found. The mean a-sv concentration difference was 27 t 5 umol/l, 3.8 k 0.8 % of the arterial concentration. The a-sv difference was fairly constant during the infusion.
Sampling from the superficial vein was only possible in four HTG subjects. In 8 out of 19 paired samples a statis- tically significant extraction was found. In 1 out of 1 9 pairs a significant re- lease was found. The mean a-sv concen- tration difference in HTG subjects was significant, 1 6 c 7 pmol/l, 1.1 i 0.5 % of the arterial concentration. The ab- solute a-sv concentration differences did not differ significantly between HTG and NTG subjects, but the fractional ex- traction was lower in HTG subjects ( p < 0.05). The a-dv differences were greater than the a-sv differences in both HTG and NTG subjects (p < 0.001 and p < 0.05 respectively).
The mean fractional a-dv removal over the Intralipid infusion period €or each subject was significantly and positively correlated with the corresponding k2 values (r = 0.61, p < 0.05, Fig. 2 ) . A similar trend was observed for a a-sv differences versus k2 although it did not reach significance (p > 0 . 0 5 ) .
Discussion
The a-dv differences of exogenous TG in NTG subjects in the present study are in good agreement with our previous study using an Intralipid infusion time of 30 minutes. These new findings show that exogenous plasma TG are removed by skeletal muscle for three hours with no tendency towards a reduced absolute or fractional removal with time. This in- dicates that saturation of removal sites does not occur and consequently that the removal of fat particles is probably not merely due to absorption into the vessel walls. The fairly constant ar- terial concentrations of exogenous TG indicate that the removal process studied is constant and is a first order reac- tion over the whole period studied. Pre- viously we have shown that when dynamic forearm work for ten minutes was started 30 minutes after Intralipid infusion no further removal of exogenous TG could be observed. The results of the present study make it unlikely that these findings could be due to saturation occurring with time but suggest that the increase in flow without a simultaneous increase in TG uptake leads to a decrease in a-dv concentration difference. In fact previous studies suggest that muscular exercise does not increase TG uptake (12).
In HTG subjects the absolute a-dv concentration difference was signifi- cantly lower than in NTG subjects. Furthermore, a significant removal was demonstrated less frequently in HTG than in NTG subjects and the mean fractional removal was about half the value found in NTG. The difference between the groups are probably not due to a difference in plasma TG concentration since there is good evidence that the removal of TG from blood follows first order kinetics ( 1 3 ) . The findings thus support the con- cept that HTG subjects have an impaired ability to remove exogenous plasma TG in skeletal muscle. It may be argued that progressive de- lipidation of Intralipid particles during removal would diminish particle size. If so, light scattering in blood leaving the removing tissue would not be a valid measure of the concentration of exogenous TG. However, the use of nephelometry for the study of arterio- venous concentration differences of fat particles has previously been validated in several studies by comparison with chemical methods with very high precision (1 - 3). When replicate determinations of TG concentrations were made after extraction with Folch chloroform-methanol. extract, a very close correlation was found. Furthermore, electron-microscopy screening of Intralipid particle size in arteries and in the coronary sinus did not reveal any major differences (1). The results of these findings sug- gest.that nephelometry can be used to determine the concentration differences of fat particles. In these as well as in the present study no systematic ar- terio-venous concentration differences of 1251-labelled-albumin were found which could account for concentration differences of exogenous plasma TG.
The mechanisms responsible for TG removal by skeletal muscle are not known in detail. Lipoprotein lipase ac- tivity has been demonstrated in swine skeletal muscle (14). It has also been shown that a close arterial injection of heparin releases lipoprotein lipase activity in the deep forearm veins (151, i.e. from the forearm muscle vasculature. This lipase activity was not salt resis- tent which distinguishes it from lipase of hepatic origin (16).
The fractional removal of exogenous plasma TG in subcutaneous forearm tissue of NTG subjects was about half the value obtained in skeletal muscle. This re- lationship is in good agreement with the results we obtained in the short time infusion study (2). In NTG subjects no tendency towards saturation of the removal in subcutaneous tissue was ob-

305 S. RBssner et a l . : Triglyceri.de Removal in Hypertriglyceridaemia
served with time. In HTG subjects the number of paired samples does not war- rant any conclusion about removal satur- ation with time. However, there was a significant mean a-sv concentration difference when the figures from all paired samples were pooled.
If the TG removed in musle tissue had been taken up and completely utilized for oxidative metabolism, the fraction which it covers can be calculated as- suming normal a-dv 02 differences ( 2 ) . Thus TG would have covered 90 % of the oxidative metabolism in NTG subjects and 70 % in HTG subjects.
The present study has demonstrated that a substantial amount of i.v. ad- ministered fat particles can be removed by skeletal muscle.,The finding that the k2 value of the IVFTT was signifi- cantly correlated with the mean frac- tional a-dv removal rate suggests that removal in muscle tissue is of major importance for the elimination of exo- genous TG particles from plasma and that an impairment in muscle removal of TG particles might be of pathogenic im- portance in the development of hypertri- glyceridaemia.
A c k n o w l e d g e m e n t s . This work was supported by Tore Nilssons fund for Medical Research and by the Swedish Medical Research Council (194 - 2 0 4 ) .
References
1. Carlson, L.A., Kaijser, L., Rossner, S., Wahlqvist, M.L.: Myocardial metabolism of exogenous plasma triglycerides in resting man. Acta med. scand. 193, 233 - 245 (1973)
2. Kaijser, L., Rossner, S.: Removal of exo- genous triglycerides in human forearm muscle and subcutaneous tissue. Acta med. scand. 197, 289 - 294 (1975)
3. Rossner, S.: Studies on an Intravenous Fat Tolerance Test. Methodological, experimental and clinical experiences with IntralipidR. Acta med. scand. (Suppl. 564) , 3 - 24) (1974)
Application of a new intravenous fat toler- ance test in the study pf hypertriglycerid- aemia in man. J. Atheroscler. Res. 9, 159 - 169 (1969)
5. Carlson, L.A., Rdssner, S.: A methodological study on an intravenous fat tolerance test with the IntralipidR emulsion. Scand. J. clin. Lab. Invest. 29, 243 - 342 (1972)
4. Boberg, J., Carlson, L.A.., Hallberg, D.:
6. Robinson, D.S.: The function of plasma tri- glycerides in fatty acid transport. I n : Lipid Metabolism. M. Florkin and D.H. Stotz (eds.), p. 82. Amsterdam: Elsevier 1970
7. Olsson, A.G.: Studies in asymptomatic primary hyperlipidaemia. Clinical, biochemical and physiological investigations. Acta med. scand. (SUppl. 5811, 6 - 30 (1975)
8. Coles, D.R., Cooper, K.E., Mottram, R.F., Occleshaw, J.V.: The source of blood samples withdrawn from deep forearm veins via cathe- ters passed upstream from the median cubital vein. J. Physiol. (Lond.) 142, 323 - 328 (19581
measurement of triglycerides. In: Automation in Analytical Chemistry. Skeggs, L.T. (ed.), p- 341. New York: Medical Inc. 1965
10. Block, W.D., Jarrett, K.J., Leoine, B.: Use of a single color reagent to improve the automated determination of serum total chol- esterol. In: Automation in Analytical Chem- istry. Skeggs, L.T. (ed.), p. 345. New York: Medical Inc.
11. Stone, M.C., Thorp, J.M.: A new technique for the investigation of the low-density lipoproteins in health and disease. Clin. Chim. Acta 14, 812 - 830 (1966)
12. Wahlqvist, M.L., Rossner, S., Kaijser, L., Carlson, L.A.: Myocardial metabolism during infusions of glucose and a fat emulsion in healthy men. Studies at rest and during prolonged exercise. Acta Univ. Uppsala, 118 (1972)
from the blood stream. Acta physiol. scand. suppl. 254, 3 - 23 (1965)
14. Kinnunen, P., Ehnholm, C.: Studies on heparin releasable triglyceride lipase from swine skeletal muscle. Abstract 1974, Ninth Annual Meeting of the European Society for Clinical Investigation. Rotterdam 1975
15. Heaf, D.J., Kaijser, L., Eklund, B., CarlSon, L.A.: Heparin induced release of lipolytic activity from the human forearm. (In Prep- aration)
Fredrickson, D.S.: Comparison of the triqly- ceride lipase of liver, adipose tissue and postheparin plasma. J. Lipid Res. 13, 356 - 363 (1972)
9. Kessler, G., Lederer, H.: Fluorimetric
13. Hallberg, D.: Elimination of exogenous lipids
16. LaRosa, J.C., Levy, R.I., WindmfillerI H.G.,
Stephan Rdssner, M.D. King Gustav V Research Institute Karolinska Hospital Stockholm, Sweden