Embed Size (px)
Citation preview
RENAL CELL CARCINOMAAnother “most fascinating” cancer entity.
Dr Christoph OingThe Christie NHS Foundation TrustManchester, UK
CONFLICT OF INTEREST DISCLOSURE Dr Christoph Oing
Personal financial interests• Honoraria speaker activity: Medac (2018), IPSEN (2017)Institutional financial interests• NoneNon-financial interests / Leadership role medical societies non-remunerated• Chairman “Junge DGHO” of the German Society of Hematology and Oncology
(DGHO)• ESMO YOC memberOther• Travel and conference attendance: IPSEN (2017)
PATHOPHYSIOLOGY
RISK CLASSIFICATION
TREATMENT
RENAL CELL CARCINOMAAgenda

Macroscopic hematuria
Lower back pain
Palpable lumbar mass
Anemia
Fatigue
Incidentally, asymptomatic (ultrasound, MR)
KIDNEY TUMOURSClinical presentation
Classic triad 10-15% of ptsX
RCC suspected: Abominopelvic CT (contrast-enhanced) or MRI Chest X-ray Bone scan (if clinically indicated)
Who needs a biopsy? If surgery anyways No
But you need a biopsy... To assess indeterminate (small) renal masses To select most suitable therapy strategy (“Treat or not to treat”)
KIDNEY TUMOURSDiagnostic work-up
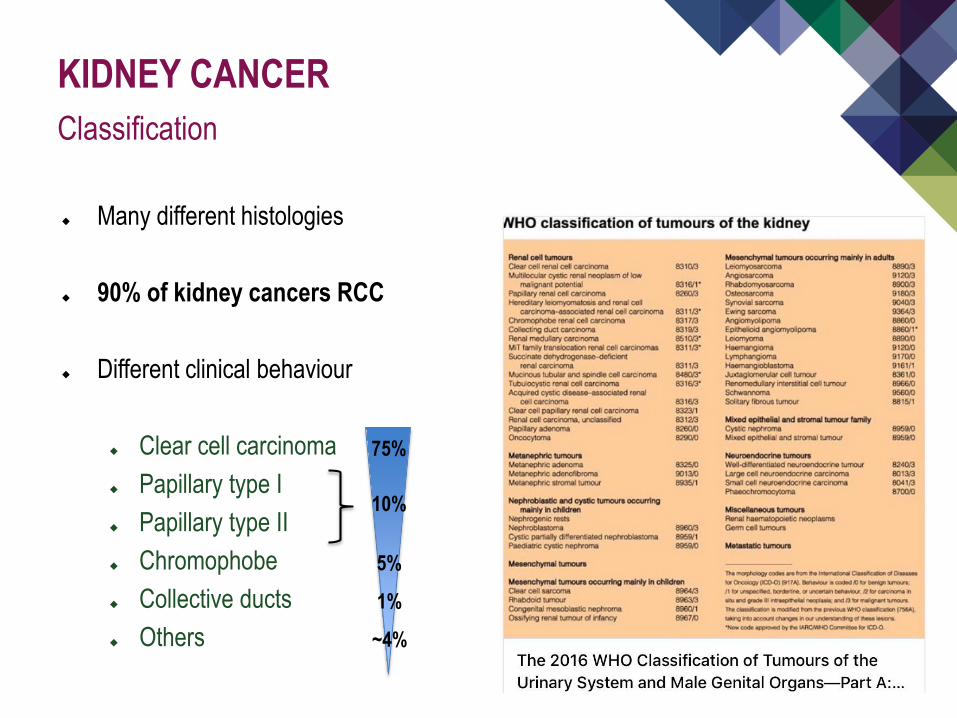
Many different histologies
90% of kidney cancers RCC
Different clinical behaviour
Clear cell carcinoma Papillary type I Papillary type II Chromophobe Collective ducts Others
KIDNEY CANCERClassification
75%
10%
5%
1%
~4%
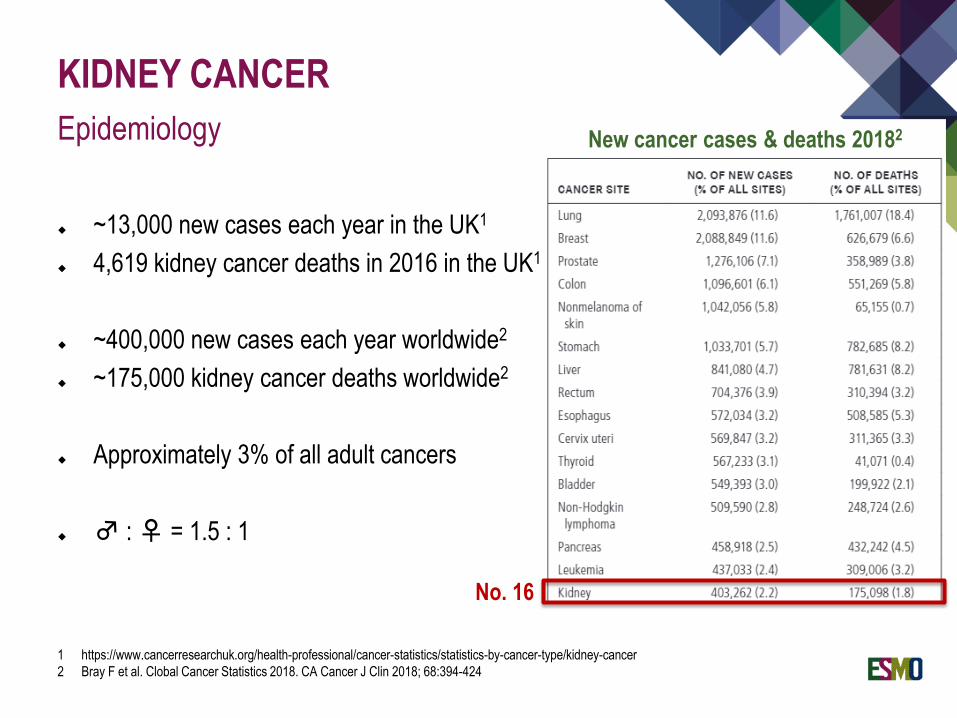
~13,000 new cases each year in the UK1
4,619 kidney cancer deaths in 2016 in the UK1
~400,000 new cases each year worldwide2
~175,000 kidney cancer deaths worldwide2
Approximately 3% of all adult cancers
♂ : ♀ = 1.5 : 1
KIDNEY CANCEREpidemiology
1 https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/kidney-cancer2 Bray F et al. Clobal Cancer Statistics 2018. CA Cancer J Clin 2018; 68:394-424
New cancer cases & deaths 20182
No. 16
Smoking (x4)
Obesity Chemical exposure
VHL disease (2-3%, clear cell RCC)
MET germline mutations (80% papillary type I RCC)
Familial (hereditary leiomyomatosis, etc.)
KIDNEY CANCERRisk factors & primary prevention
@nhssmokefree
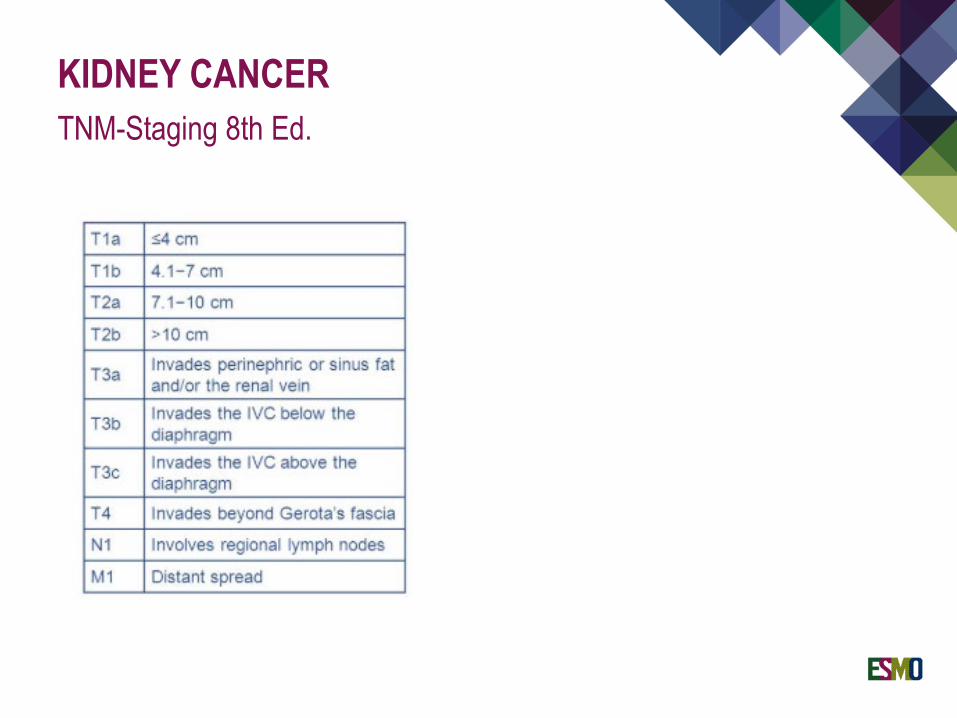
KIDNEY CANCERTNM-Staging 8th Ed.
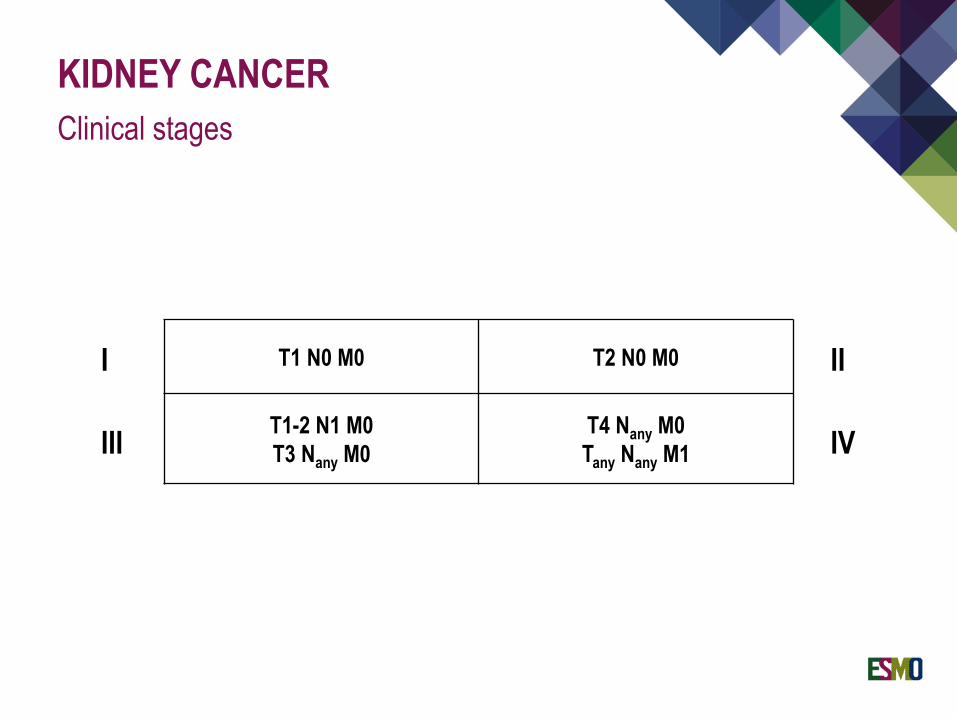
KIDNEY CANCERClinical stages
T1 N0 M0 T2 N0 M0
T1-2 N1 M0T3 Nany M0
T4 Nany M0Tany Nany M1
I II
III IV
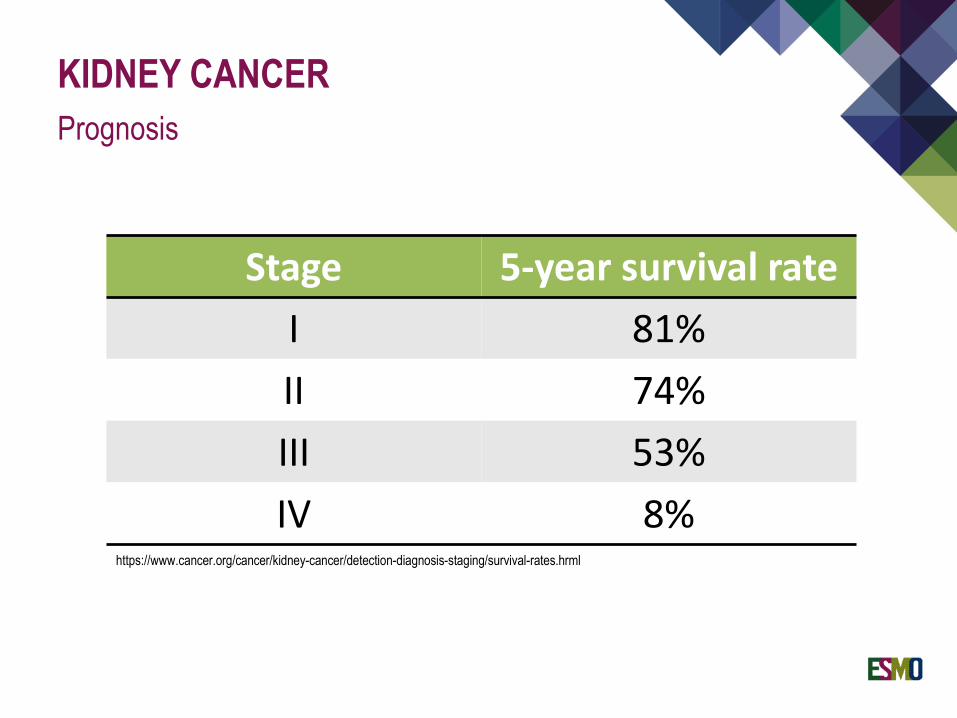
KIDNEY CANCERPrognosis
Stage 5-year survival rateI 81%II 74%III 53%IV 8%
https://www.cancer.org/cancer/kidney-cancer/detection-diagnosis-staging/survival-rates.hrml

Clinical behaviour
Prognosis
Treatment decision making
„Renal Cell Carcinoma“ ≠ ccRCC
Subtyping can be tricky (i.e. eosinophilic RCC, RCC NOS, familial cases)
KIDNEY TUMOURSSubtyping is critical
#BCritical
Most frequent histology (60-75%)
~90% driven by mutations or hypermethylation of the VHL gene on 3p26 (sporadic ccRCC)
Pseudohypoxia via lost HIF1a degradation
Constitutively active VEGF signalling
RENAL CELL CARINOMAClear cell carcinoma

CLEAR CELL RCCResult of angiogenesis
Strongly hypervascular tumors

RISK CLASSIFICATION
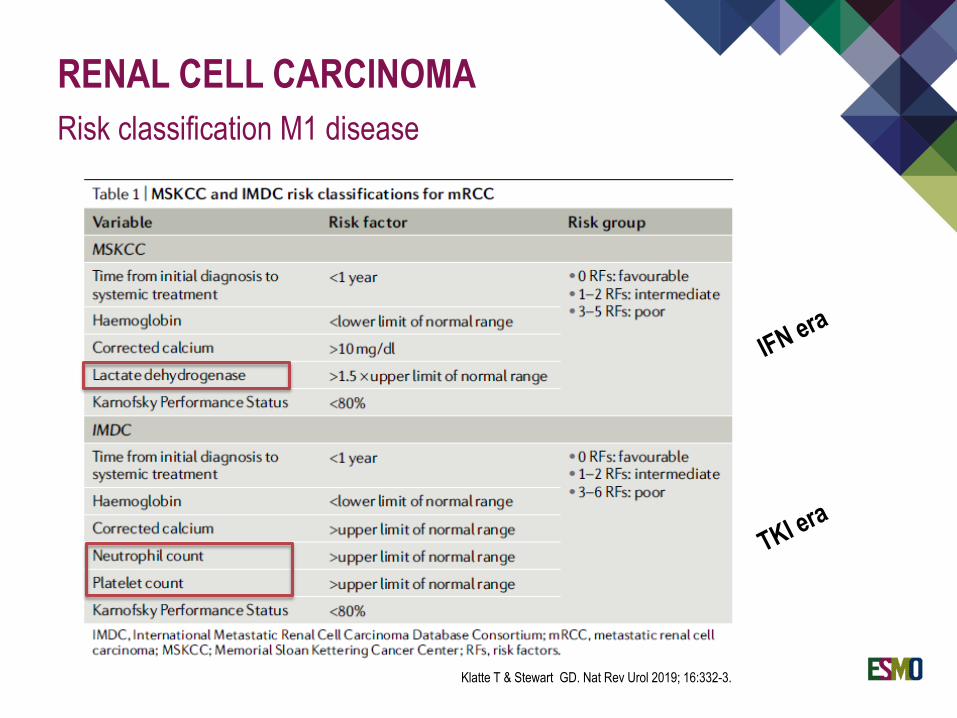
RENAL CELL CARCINOMARisk classification M1 disease
Klatte T & Stewart GD. Nat Rev Urol 2019; 16:332-3.
RENAL CELL CARCINOMA
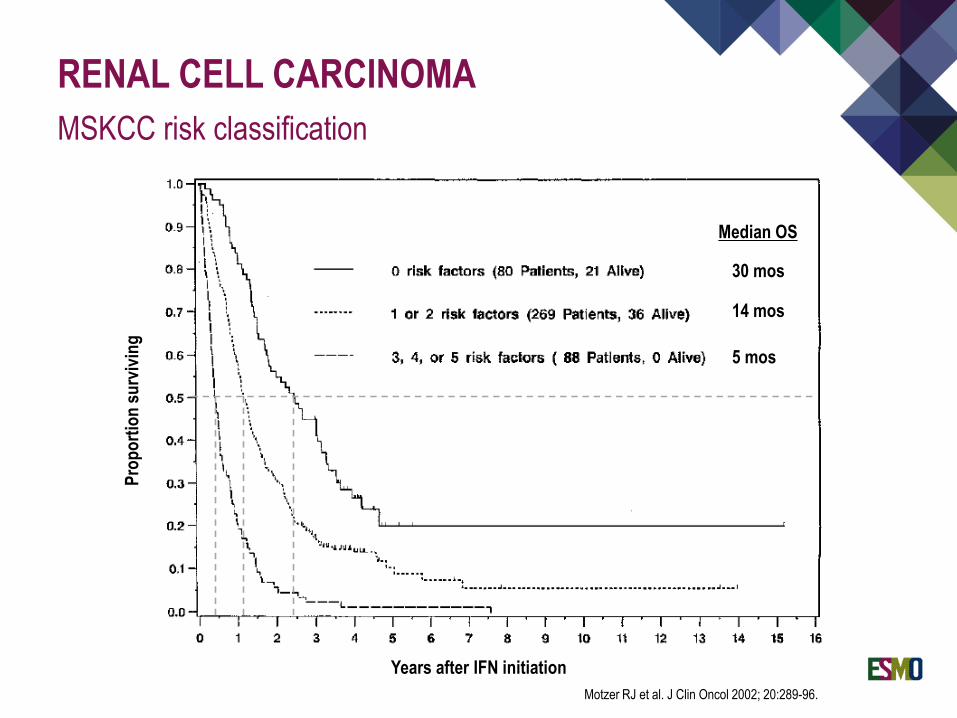
Motzer RJ et al. J Clin Oncol 2002; 20:289-96.
MSKCC risk classification
5 mos
30 mos
14 mos
Median OS
Prop
ortio
n su
rvivi
ng
Years after IFN initiation

RENAL CELL CARCINOMA
Heng et al. Lancet Oncology 2013
IMDC risk classification
7.8 mos 22.5 mos 43.2 mos
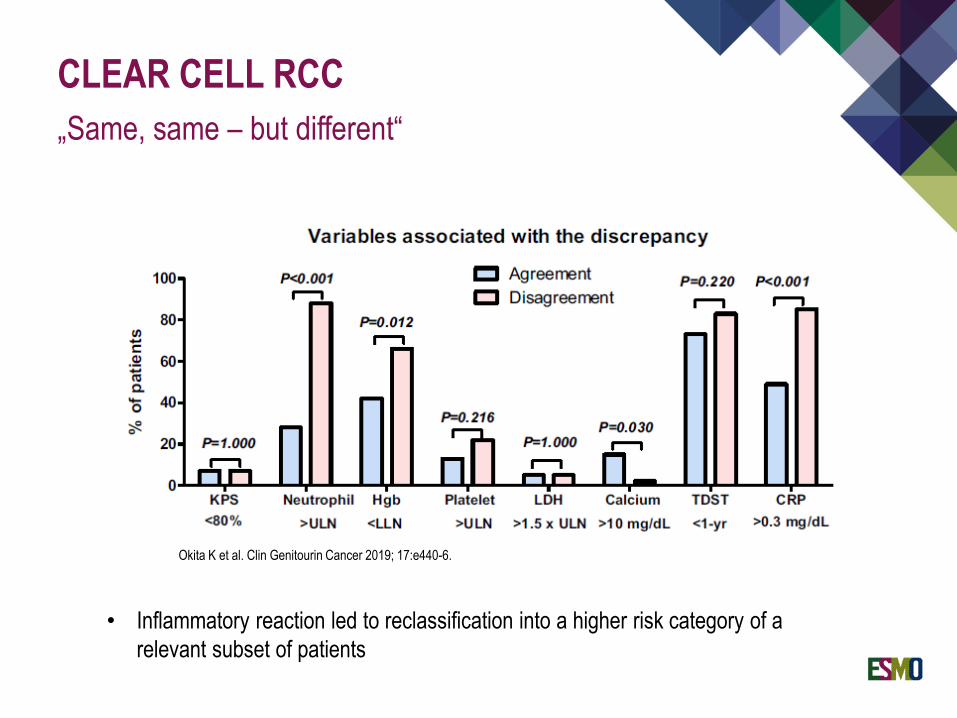
CLEAR CELL RCC„Same, same – but different“
Okita K et al. Clin Genitourin Cancer 2019; 17:e440-6.
• Inflammatory reaction led to reclassification into a higher risk category of a relevant subset of patients
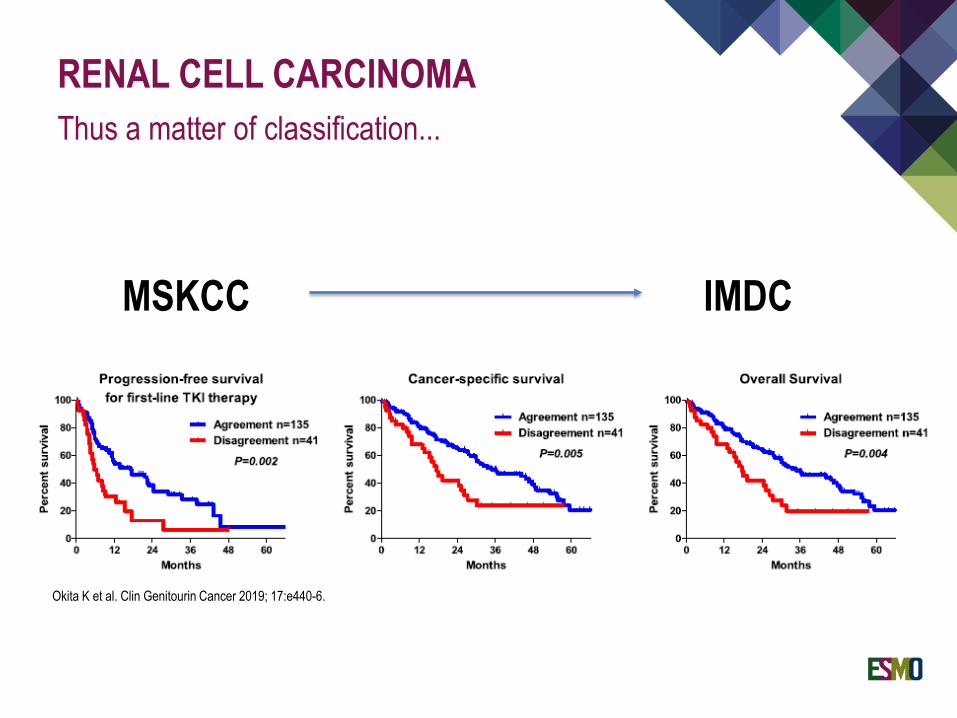
RENAL CELL CARCINOMAThus a matter of classification...
Okita K et al. Clin Genitourin Cancer 2019; 17:e440-6.
MSKCC IMDC
Commonly spreads to lymph nodes, lung, and bone
Prognostic role for site of metastasis Atypic
Pancreatic M1 special entitiy? Thyroid M1 special entitiy?
Oligometastatic (incl. Bone, Lung, Liver) Better outcomes Metastasectomy!? Different disease?
Bone M1 or liver M1 poor prognosis
RENAL CELL CARCINOMAClinical behaviour

TREATMENT
RENAL CELL CARCINOMAPrinciples of cancer treatment
TREATMENT „LOCALISED DISEASE“

RENAL CELL CARCINOMATreatment localised disease (stage I / II)
Capitanio U & Montorsi F. Renal Cancer. Lancet 2016; 387:894-906.

RENAL CARCINOMARadical nephrectomy
Only if organ-sparing approach not feasible (i.e. ≥ cT3) LND controversial in cN+ adds staging information, no survival benefit Also for cytoreductive nephrectomy in Stage IV patients
No RCT phase III data supporting use of adjuvant systemic treatment
Conflicting trial results for TKI S-TRAC SUNITINIB vs. PLACEBO OS immature ASSURE PAZOPANIB vs. PLACEBO No OS benefit PROTECT SUNITINIB vs. PLACEBO No OS benefit Toxicity↑ / QoL↓ vs. uncertain clinical benefit
Adjuvant sunitinib available for high risk patients in the US pT3 tumors │ N1 disease
IO to come?! (NIVO or DURVA±TREME vs. PLACEBO)
CLEAR CELL RCCAdjuvant therapy

TREATMENT „ADVANCED DISEASE“

SURGERY

CLEAR CELL RCCCytoreductive nephrectomy
Sunitinib aloneNephrectomy plus Sunitinib
Role of CN in TKI era questionable Still recommended for good risk patients Certainly no option for poor risk patients / high metastatic burden
Flanigan RC et al. New Engl J Med 2001; 345:1655-9. Méjean A et al. New Engl J Med 2018; 379:417-27.

RADIOTHERAPY

Low response rates to conventional RT (i.e. 2 Gy / fraction)
BUT High responses to high-dose-per-rate schedules
Stereotactic Ablative Radiotherapy (SABR) (i.e. 26 Gy / 1 fraction or40 Gy / 5 fractions)
Causes break down of blood supply
Sufficient local control and low toxicity Rarely used for primary RCC Regularly used for metastases (e.g. brain, bone)
CLEAR CELL RCCExternal Beam Radiotherapy

IMMUNOTHERAPY„OLD FASHIONED“
RCC are strongly immunogenic tumors
Historical treatment (and still in some US centers...) High dose IL-2 High dose Interferon α2
Provides durable responses in 10% of patients
Extremely toxic (IL-2) Massive capillary leakage, SIRS, organ failure due to cytokine
storm
RENAL CELL CARCINOMAImmunotherapy
ANTIANGIOGENICTHERAPY
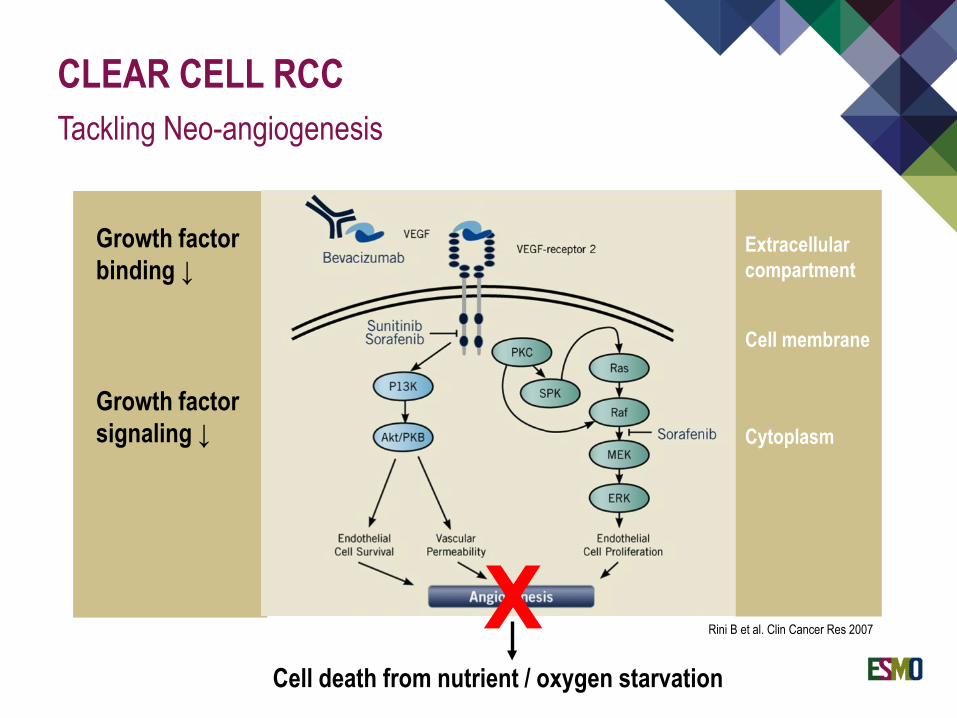
CLEAR CELL RCCTackling Neo-angiogenesis
Rini B et al. Clin Cancer Res 2007XCell death from nutrient / oxygen starvation
Growth factorbinding ↓
Growth factorsignaling ↓
Extracellularcompartment
Cell membrane
Cytoplasm
Anti-VEGF tyrosine kinase inhibitors Block intracellular activation of VEGF pathway
Orally available
Good penetration of blood-brain barrier
CLEAR CELL RCCAvailable drugs: TKI
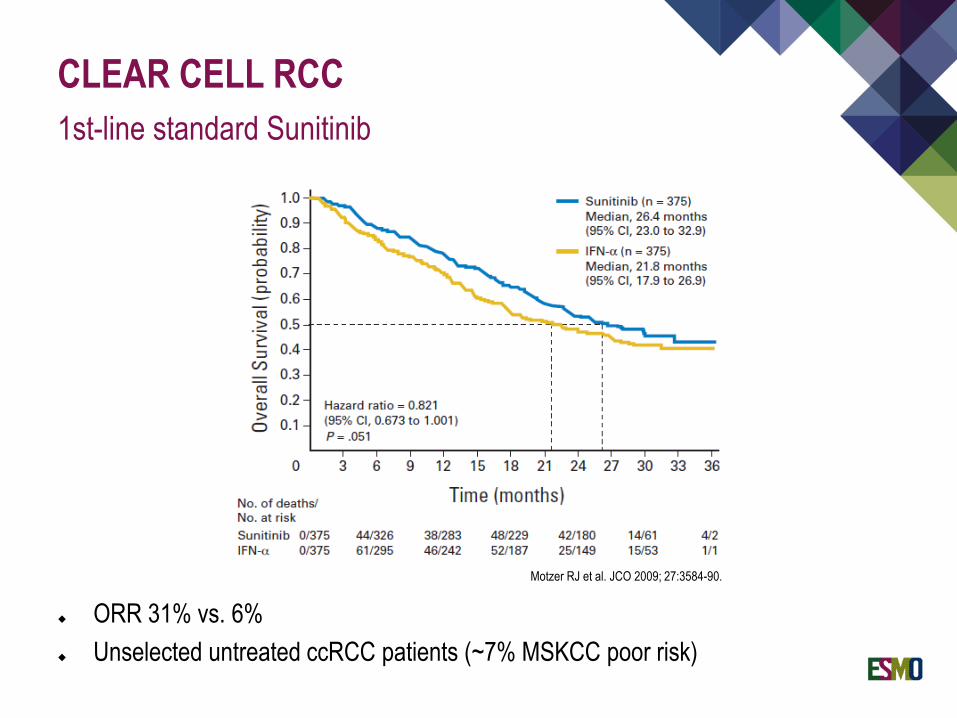
CLEAR CELL RCC1st-line standard Sunitinib
ORR 31% vs. 6% Unselected untreated ccRCC patients (~7% MSKCC poor risk)
Motzer RJ et al. JCO 2009; 27:3584-90.

Sunitinib (SutentTM) 50mg caps OD, 4w on 2w off Side effects: fatigue, hand-foot syndrome, stomatitis
Pazopanib (VotrientTM) 800mg OD Side effects: diarrhoea, hair discoloration
Axitinib (InlytaTM) 5mg BID Side effects: diarrhoea, dysphonia, fatigue
Tivozanib (FotivdaTM) 1,340µg OD, 3w on 1w off Side effects: dysphonia, diarrhoea, fatigue
CLASS EFFECTS: HYPERTENSION, HYPOTHYROIDISM
CLEAR CELL RCCTKI – First line
IMMUNOTHERAPY„MODERN WARFARE“

Anti-CTLA-4 monoclonal antibodies (Ipilimumab) First generation High incidence of auto-immune toxicity Moderate efficacy
Anti-PD-1 and anti-PD-L1 monoclonal antibodies (Nivolumab, Pembrolizumab, Avelumab, Atezolizumab) Second generation Less toxic More efficient
Combination therapy Higher response rate but also toxicity
CLEAR CELL RCCImmune checkpoint inhibitors 2019
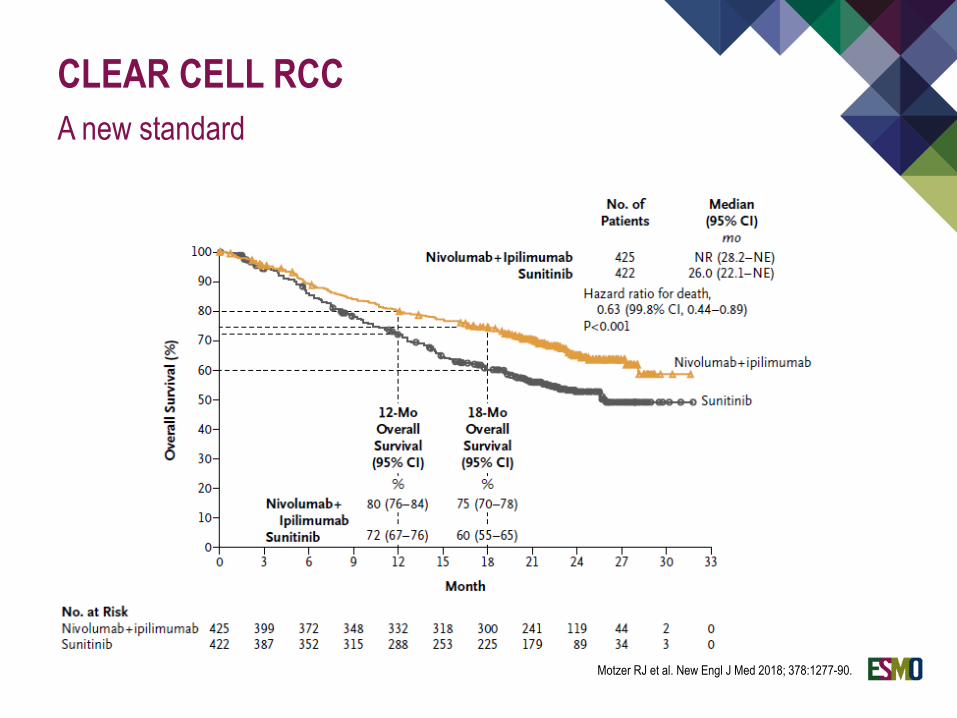
CLEAR CELL RCCA new standard
Motzer RJ et al. New Engl J Med 2018; 378:1277-90.
15-20% responders to PD-1i are long term responders iRECIST important When to stop treatment? When to consider a cure of stage IV RCC?
No measure for proper response prediction Also PD-L1 negative tumours respond
Combinations with promising results PD-1i + CTLA-4i PD-L1i + TKI PD-L1i + VEGFi
CLEAR CELL RCCEvolution of concepts
IO
TKI
IO
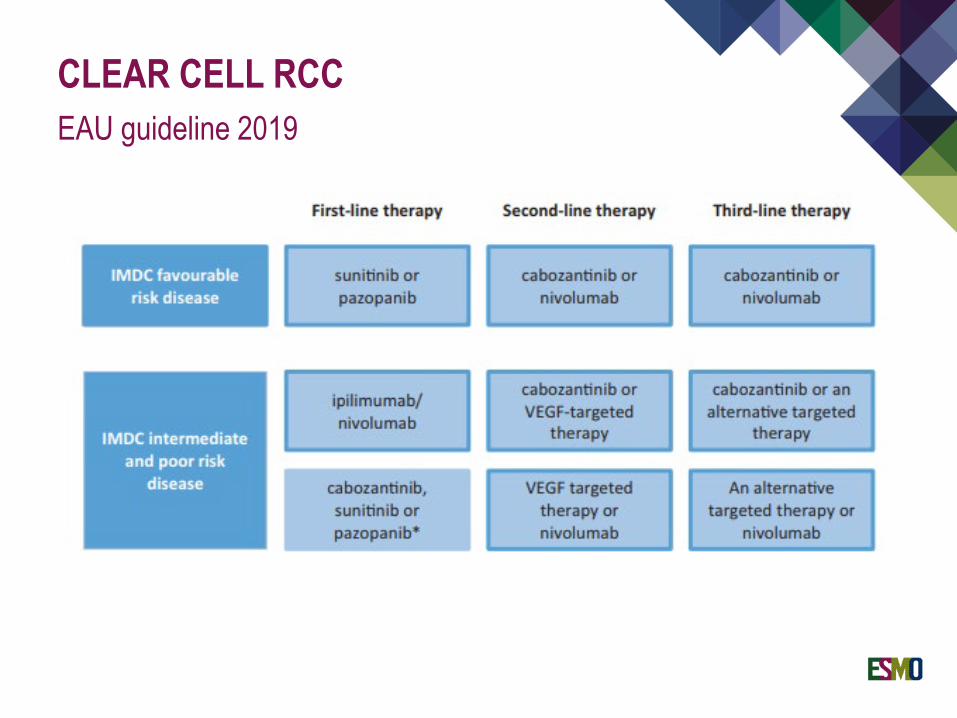
CLEAR CELL RCCEAU guideline 2019
NON-CLEAR CELL RCCLimited evidence, limited options
Papillary type I RCC MET-driven Consider Cabozantinib
Papillary type II RCC Consider anti-VEGFR TKI
Chromophobe RCC Consider Temsirolimus (mTORi)
Collective duct / medullary RCC Chemotherapy according to urothelial cancers
Kidney tumours comprise a bunge of different entities
Consider carefully if you need a biopsy
Challenge your pathologist
Clear Cell Renal Cell Carcinoma most common RCC subtype
ccRCC related to VHL inactivation and Pseudohypoxia
Angiogenesis very important for ccRCC growth
LN, lungs and bones common sites for metastatic spread
TAKE HOME MESSAGE IRCC characteristics
TAKE HOME MESSAGE IIRCC treatment
Conventional chemo- and radiotherapy ineffective
Organ-sparing surgery whenever possible in localised disease
ccRCC‘s Achilles‘ heel: Angiogenesis and Immunogenicity
No role for adjuvant systemic TKI
Total resection for oligometastatic disease if feasible
Cytoreductive nephrectomy no more in poor risk mRCC patients
TKI still standard of care for good risk metastatic ccRCC
TKI and PD-1i ± key to success in intermediate / poor risk ccRCC

EMUC 2019… if you haven‘t been to Vienna!