Urinary Tract Infection Keep in mind the possibility of UTI
should be considered in any febrile child (temp >39) Girls 10^5
colony forming units of single organism /ml) or the presence of
more than 1 organism Older child > 6Years will be presented by
Fever vomiting Abdominal pain Dysuria Urgency Frequency Enuresis
& Incontinence Most common causes gram ve colonic bacteria
(E.Coli 80%) Klebsiella Proteus (more in males ) Note: Pseudomonas
usually indicates structural anomaly as vesico-ureteric reflux
Further investigations for ( recurrent attack or prolonged fever
> 48 hours with good treatment )Abdomino-pelvic US Abdominal
X-ray Micturating cystourethrography to exclude vesico-ureteric
reflux Medication ( Outpatient Antibiotics choice for 7-10days
)1-TMP-SFX 20mg/kg/day PO q12h
2-1st generation cephalosporins 50mg/kg/day PO q6hCephalexin or
cephradine or cefadroxil3-2nd generation cephalosporins 50mg/kg/day
PO q8hcefaclor
3-fluroquinolone cipro 20-30mg/kg/day PO q12h >18 years
Parental therapy ( Inpatient Antibiotics
choice)1-Ampicillin100-200mg/kg/day q12h I.V + Gentamicin
3mg/kg/day q12h IM Or Amikin 15mg/kg/day q12h IM2-Ceftriaxone
50-100mg/kg/day q12-24h IV Analgesics as acetaminophen &
Ibuprofen Analgesics to provide relief from burning , spasticity
during voidingPhenazopyridine like urisept 100mg tab (3LE) 6-12y :
1 tablet q8h after meal >12y : 1-2 tablets q8h after meal
Alkalinizing agents to change the urine PH As Epimag sachets /
Xenomag sachets or Coliurinal eff. Orally twice dailyFor recurrent
attacks
Hematuria (Acute post streptococcal glomerulonephritis)DDxAsk
about Dysuria,frequency and abdominal pain ( UTI) History of trauma
Bruising (HSP) Nose bleeding (Coagulation disorders) Recent drugs
(Aspirin) Vigorous ExerciseOther DDx1-Hemolytic uremic syndrome
history of bloody diarrhea 2-7days before onset of renal failure
edema and petechiae pallor diagnosis made upon signs of ARF +
thrombocytopenia + Anaemia (stool culture E-coli)2-IgA
nephropathy3-Hypercalciuria4-SLE5-Urolithiasis6-Sickle cell
haemoglobinopathies7-Calculi8-Wilm`s tumor Acute post streptococcal
glomerulonephritisClinical presentation of Acute post Streptococcal
glomerulonephritis1-Acute nephritic syndromeOliguria and hematuria
usually improved by end of the 1st weekLow grade fever
,hedacheHistory of infection 2 weeks before onset of
symptomsHypertension present in >70% cases (125/80)Edema mild
acute puffy eye lids & Lower limb edema 2-Hypertensive heart
failure3-Hypertensive encephalopathyRenal biopsy is indicated only
with persistent low C3 >3months or persistent hematuria
>6monthsHome management in 95% of cases only hospitalization
with severe hypertension or severe oliguria Management Rest at
least 1st week (during oliguria) Diet salt & protein
restriction Fluids restrictions to 1L/day Control of hypertension
and edema (mild hypertension may persist for few weeks)1-Furesmide
is helpful in both and increase urine ouput (1mg/kg/day q12h) 12
2-If hypertension persists add CCBlockers as Hydralazine
(1mg/kg/day q12h) PO3-ACEIs effective but cause hyperkalemia
Penicillin (10 days oral course for eradication of any
streptococcal infection Furosemide : 1-Lasix 20,40mg ampule (2-4LE)
2-lasix 40mg tab (6LE) 3-Lafurex 20mg tab (4.5LE) 4-Lafurex 20mg
ampule (1.5LE) 5-Diusex 20mg ampule (1.5LE)
Nephrotic SyndromeIt`s combination of edema, heavy proteinuria,
hypoalbuminemia & hyperlipidemaWith NO hypertension or gross
hematuriaInvestigationsProtein in 24 hours urine >
40mg/m2/hrSerum albumin < 3gm%Serum cholesterol > 300mg%Note
: Renal function test C3 & A.S.O.T all are normalManagement :
exclude active infection or other contraindications before starting
Steroids therapy induction of remission ( daily therapy )Prednisone
(2mg/kg/day, maximum 60mg) for 6 weeks maximum single daily dose or
split into 2 dosesEither Steroid responsive : urine become free of
Albumin Steroid resistant : no response after 1 month so renal
biopsy indicated maintenance of remission ( alternate day therapy )
for steroid responsivePrednisone (1.5mg/kg/day, maximum 40mg)
single daily dose on alternate days for 2-6 months better 6 months
to decrease relapse by about 33% relapses (recurrence of edema)
treated as the initial attack but alternate day therapy is
continued for longer period (6-12 months)1-Hostacortin 5mg tab
(4LE) 2-Hostacortin-H 5mg tab (4LE) 3-Prednisolone tab (1LE)
4-Predilon tab (2LE) 5-Deltacortil 5mg tab (1.5 LE) 6-Urbason
4mg-8mg tab (10LE) 7-Solupred 5mg-20mg tab (23-40LE)
Frequently relapsing and steroid dependant disease2 or more
replases within 6 months 2 or more relapses during tapering4 or
more relapses within 12 months or within 14 days of stopping
steroidsBoth are steroids sensitiveCyclophosphamide e.g: Endoxan
50mg tab (38LE) Alkyloxan tab (62LE)It decrease rate of relapse
compared to treatment of prednisolone Dose (2mg/kg/day) single dose
for 12 weeks . alternate day therapy with prednisone is continued
during the course of cyclophosphamide therapyCyclophosphamide is
discontinued if WBCs count falls below 5000/cmmNote:Diuretics
(furosemide) may be of benefit in childrens with edema however
hypovolaemic shock occurs with aggressive treatmentAntihypertensive
therapy may be used but not with Acute Renal FailureHome monitor
for daily weight gain urine protein level steroid
doseEnuresisRepeated involuntary voiding in childrens > 4years
(expected age of bladder control)It`s either 1ry (chiled never
attained bladder control) or 2ry (chiled attained bladder control
for at least 6 months)It`s either Nocturnal (at night) in majority
of cases with good prognosis or Diurnal (day & night) with bad
prognosis Note: Urinalysis (the most important screening test in a
child with enuresis) exclude U.T.IIn 2ry enuresis (5% of cases)
you`ll search for a cause and manage1-Diabetes Mellitus (do Random
blood sugar) 2- Diabetes Insipidus (look for urine specific
gravity) 3-genitourinary anomaly ( do U/S) 4-decrease level of ADH
(measure it) 5-known patient with Sickle cell anaemia 6-chronic
constipation press on urinary bladderManagement of 1ry enuresis:
before age of 5 years no drug treatment only 1-simple measures 3
Reassurance bladder control usually between 1-5 years Avoid
excessive fluid intake 2 hours before bedtime No punishment Let
child urinate before sleep Reward the baby for the dry nights
Proper training such as holding urine as much as possible
2-Alarm therapy should be considered for every patient. It is
reported to improve bedwetting by increasing nocturnal bladder
capacity or by enhanced arousal; it does not reduce nocturnal urine
output.cure rate up to 80% but relapse rate between 10-40% it gives
good results after 2 weeks but it may be used upto 3 months or 1
month after being dry. If failed it should be used again once the
child is older and more motivated
3-Drug therapy : it`s only indicated for children above 5 years
with 1ry nocturnal enuresis1-imipramine it`s tricyclic
antidepressant increase release of Anti Diuretic Hormone (theory)
success rate about 60% but relapse >90%1-Tofranil 25mg
tab(2.5LE) 2-tofranil 10mg tab(1.5LE) 3-imipramine 25mg tab(4.5LE)
4- toframine 25mg tab(4.5LE)Dose: start with 1 tablet daily 1 hour
before sleep for 2 weeks if no response give 2 tablets (50mg) for
another 2 weeks if no response stop the drug . if there`s response
continue the drug for 3 months then tapering it by giving the same
dose (25mg or 50mg) once every other day for 3 weeks then once
every third night for 3 weeks 2 . 3 3 3 3
2-Desmopressin it`s synthetic vasopressin analogue salt
retention urine concentrate decrease urine volume it`s mainly used
in ttt of Diabetes Insipidus but effective in enuresis it has 50%
success but relapse >94% Dose: start with minirin melt 60mcg
(30tabs) (155LE) for 2 weeks if no response may increase dose upto
minirin melt 120mcg (30tabs) (300LE) for another 2 weeks in case of
response use the drug for 2 months then gradual tapering for 4
weeks it`s very expensive drug3-Anticholinergic drus the only
benefit of these drugs it makes the bladder hold more urine but it
doesn`t decrease bed time dose of oxybutynin 5mg PO daily and
increased gradually up to 20mg/day at sleep time 1-uripan 5mg/5ml
(7.5LE) 2-Detrusan 5mg/5ml (6.5LE) 3-Detronin 5mg/5ml (6.5LE)Some
doctors use : bellacid tab (2LE) it contains belladonna 10mg &
phenobarbitone 20mg for nocturnal enuresis 1/2 to 1 tablet before
bed time but it`s used for spastic colon
Surgical conditions in pediatricsYou should know about it ? you
will see it ? you`ll refere it Testicular Disorders undescended
testisThe diagnosis of undescended testes is usually made by the
parents or first examining physician. The important point is the
absolute necessity of distinguishing between retractile testes and
the true undescended testes. Testes that can be drawn to the
scrotum, even if they retract again, are retractile testes and not
undescended, the squatting position may aid in helping descend the
testes for exam. Retractile testis needs no further surgical
management.Time of operation ? Tell the parents that pediatrics
surgeon wait until the baby reach 6 months there`s a good chance
for testicular descent without surgery if this not occurred surgery
must be done. Testicular swellingAny case of testicular swelling
should do Testicular Ultrasonography why ? because in children it`s
very difficult to differentiate Hydrocele from Inguinal hernia
clinically. don`t rely on testicular size , transillumination or
the size of swelling over time . moreover there may be both hernia
and hydrocele together specially in preterm babies Why you do U/S ?
because hernia may be incarcerated and this is surgical emergency
associated with acute pain, swelling(hard-red-painful), pulling up
legs and vomiting Hydrocele
A hydrocele is a collection of fluid in the space surrounding
the testicle between the layers of the tunica vaginalis. Hydroceles
can be scrotal, of the cord, abdominal, or a combination of the
above. A hydrocele of the cord is the fluid-filled remnant of the
processus vaginalis separated from the tunica vaginalis. A
communicating hydrocele is one that communicates with the
peritoneal cavity by way of a narrow opening into a hernial sac.
Hydroceles are common in infants. Some are associated with an
inguinal hernia. They are often bilateral, and like hernias, are
more common on the right than the left. Most hydroceles will
resolve spontaneously by 1-2 years of age. After this time,
elective repair can be performed at any time Inguinal hernia is the
most common surgical problem of childhood. The infant or child with
an inguinal hernia generally presents with a bulge at the internal
or external ring or within the scrotum. no pain is associated with
a simple inguinal hernia in an infant. The parents may perceive the
bulge as being painful when, in truth, it causes no discomfort to
the patient. The bulge commonly occurs after crying or straining
and often resolves during the night while the baby is sleeping.
Inguinal hernias never go away without treatment. Furthermore, if
the sac is left open, a loop of bowel or other organ may become
trapped or incarcerated (strangulated) in the sac. Patients with an
incarcerated hernia generally present with a tender firm mass in
the inguinal canal or scrotum. The child may be fussy, unwilling to
feed, and inconsolably crying. The skin overlying the bulge may be
edematous, erythematous, and discolored.there`s sometimes vomiting
and the baby will stop stooling This is a surgical emergency
Congenital Orthopedic Disorders in pediatrics Clubfoot
(Congenital Talipes equivarus) It`s a congenital deformity of the
foot that occurs in about 1 in 1,000 births. The affected foot
tends to be smaller than normal, with the heel pointing downward
and the forefoot turning inward. The heel cord [achilles tendon] is
tight, causing the heel to be drawn up toward the leg. This
position is referred to as "equinus," and it is impossible to place
the foot flat on the ground. Since the condition starts in the
first trimester of pregnancy, the deformity is often quite rigid at
birth. The three classic signs of clubfeet are: Fixed plantar
flexion (equinus) of the ankle, characterized by the drawn up
position of the heel and inability to bring to foot to a
plantigrade (flat) standing position. This is caused by a tight
achilles tendon Adduction (varus), or turning in of the heel or
hindfoot Adduction (turning under) of the forefoot and midfoot
giving the foot a kidney-shaped appearance If left untreated, the
deformity will not go away. It will continue to get worse over time
so immediate refer to orthopaedic surgeon is required In-toeing
Gait in ChildrenAn in-toeing gait is very common in children, and
is a frequent complaint of many parents. In fact, an in-toeing gait
(pigeon-toed) is the most common rotational deformity seen in
pediatric orthopaedics. In the overwhelming majority of patients,
the in-toeing will correct with growth over time.What causes an
in-toeing gait in children? The three most common causes of
in-toeing in children are femoral anteversion (twisting of the
femur/thigh), internal/medial tibial torsion (twisted tibia/shin
bone), and metatarsus adductus (curved foot). Femoral
anteversion/torsionis the most frequent cause of in-toeing in
children between the ages of 3-10 years. Femoral anteversion is
therefore a condition in which the femoral neck leans forward with
respect to the rest of the femur. This causes the lower extremity
on the affected side to rotate internally (the knee and foot twists
towards the midline of the body). The normal child is born with
approximately 40 degrees of femoral anteversion. This will
gradually decrease to 10-15 degrees at adolescence and generally
improves with further growth. Femoral anteversion is more common in
females, and is usually most noticeable between the ages of 4-6
years. Parents will notice that when the child is standing with the
feet forward, the patellae (kneecaps) will point inwards.
Frequently, parents will also describe the child's gait as awkward
or clumsy. The in-toeing will often appear worse with running and
at the end of the day when fatigued. Femoral anteversion will
decrease naturally in 99% of cases. Internal tibial torsion It
causes an in-toeing gait from a twisting of the tibia (shin bone).
It is most often first noticed when a child is first starting to
walk, and is most common between the ages of 2-4 years. The inward
torsion is a variation of normal anatomy and is caused partially by
the child's position in the uterus. The toddler or young child
presents to the orthopaedic clinic with complaints of "bowing
legs." Examining a child with internal tibial torsion with the
patellae (kneecaps) straight, Tibial torsion almost always improves
without treatment, and usually before school age. Splints, special
shoes, and exercise programs do not help. Surgery to re-set the
bone may be done in a child who is at least 8 to10 years old and
has a severe twist that causes significant walking problems.Note:
Flat FootIn the child before age 3 years, the normal longitudinal
arch of the foot is present, but often masked by the fat pad in the
instep. Hence all young children before age 3 look flat-footed,
even though they are not. After age 3, the fat pad disappears, and
the arch becomes more evident.
Metatarsus Adductus /Varus/MTAMetatarsus adductus (MTA) or varus
is a condition that is commonly seen in newborns and young infants,
where the forefoot is twisted inwards relative to the hindfoot (or
heel). MTA is very common in the newborn, and is usually due to the
feet being "packed" in the womb in that position. The forefoot
adduction at this stage is very flexible, and with freedom of
movement, this postural condition of MTA often improves over the
next 6 to 12 weeks.In about 15% of cases, the adducted position of
the forefoot does not improve. MTA that is diagnosed at birth does
not require treatment. It is usually postural, and with growth, the
MTA resolves spontaneously over a period of 6 to 12 weeks. X-rays
are usually not necessarySevere cases of metatarsus adductus may
partially resemble a clubfoot deformity.
Bowed LegsBowed legs in a toddler is very common. When a child
with bowed legs stands with his or her feet together, there is a
distinct space between the lower legs and knees. This may be a
result of either one, or both, of the legs curving outward. Walking
often exaggerates this bowed appearance.Adolescents occasionally
have bowed legs. In many of these cases, the child is significantly
overweight.Cause Physiologic Genu VarumIn most children under 2
years old, bowing of the legs is simply a normal variation in leg
appearance. Doctors refer to this type of bowing as physiologic
genu varum.In children with physiologic genu varum, the bowing
begins to slowly improve at approximately 18 months of age and
continues as the child grows. By ages 3 to 4, the bowing has
corrected and the legs typically have a normal appearance. Blount's
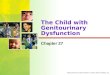
Disease
Left:Toddler with infantile Blount's disease involving the left
leg.Right:X-ray of the left knee shows the Blount's abnormality
along the top of the shinbone.Blount's disease is a condition that
can occur in toddlers, as well as in adolescents. It results from
an abnormality of the growth plate in the upper part of the
shinbone (tibia). Growth plates are located at the ends of a
child's long bones. They help determine the length and shape of the
adult bone.In a child under the age of 2 years, it may be
impossible to distinguish infantile Blount's disease from
physiologic genu varum. By the age of 3 years, however, the bowing
will worsen and an obvious problem can often be seen in an x-ray.
RicketsRickets is a bone disease in children that causes bowed legs
and other bone deformities. Children with rickets do not get enough
calcium, phosphorus, or Vitamin D all of which are important for
healthy growing bones.Nutritional rickets is unusual in developed
countries because many foods, including milk products, are
fortified with Vitamin D. Rickets can also be caused by a genetic
abnormality that does not allow Vitamin D to be absorbed correctly.
This form of rickets may be inherited (discussed
later).SymptomsBowed legs are most evident when a child stands and
walks. The most common symptom of bowed legs is an awkward walking
pattern.Toddlers with bowed legs usually have normal coordination,
and are not delayed in learning how to walk. The amount of bowing
can be significant, however, and can be quite alarming to parents
and family members.Turning in of the feet (intoeing) is also common
in toddlers and frequently occurs in combination with bowed
legs.Bowed legs do not typically cause any pain. During
adolescence, however, persistent bowing can lead to discomfort in
the hips, knees, and/or ankles because of the abnormal stress that
the curved legs have on these joints. In addition, parents are
often concerned that the child trips too frequently, particularly
if intoeing is also present.Doctor ExaminationYour doctor will
begin your child's evaluation with a thorough physical
examination.If your child is under age 2, in good health, and has
symmetrical bowing (the same amount of bowing in both legs), then
your doctor will most likely tell you that no further tests are
currently needed.However, if your doctor notes that one leg is more
severely bowed than the other, he or she may recommend an x-ray of
the lower legs. An x-ray of your child's legs in the standing
position can show Blount's disease or rickets.If your child is
older than 2 1/2 at the first doctor's visit and has symmetrical
bowing, your doctor will most likely recommend an x-ray. The
likelihood of your child having infantile Blount's disease or
rickets is greater at this age. If the x-ray shows signs of
rickets, your doctor will order blood tests to confirm the presence
of this disorder.TreatmentNatural Progession of Disease
Physiologic genu varum nearly always spontaneously corrects
itself as the child grows. This correction usually occurs by the
age of 3 to 4 years.An adolescent with Blount's disease.Untreated
infantile Blount's disease or untreated rickets results in
progressive worsening of the bowing in later childhood and
adolescence. Ultimately, these children have leg discomfort
(especially the knees) due to the abnormal stresses that occur on
the joints. Adolescents with Blount's disease are most likely to
experience pain with the bowing.
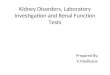
Congenital Torticollis
It`s shortening of the cervical muscles, most commonly the
sternocleidomastoid (SCM) muscle, and tilting of the head to the
opposite side. Management is conservative in most cases using early
physiotherapy exercises a mean duration of three months to achieve
full passive neck range of motion. Those children with failed
medical therapy should undergo surgical transection of the SCM
muscle. Consultation with orthopedic surgery is necessary
Thyroglossal Duct Cysts
Thyroglossal duct cyst (TDC) is the most common congenital
anterior midline neck mass usually (2/3 of cases) presenting before
the second decade of life. Symptoms appear at an average age of
four with the sudden appearance of a cystic mass at the angle of
neck level moving with tongue protrusion and swallowing. Management
is Sistrunk operation so immediate refer to general surgeon.