Embed Size (px)
Citation preview

Renewed focus on family planning in India
Division of Reproductive and Child Health INDIAN COUNCIL OF MEDICAL RESEARCH
NEW DELHI
CME 100th ICCR 20th April, 2012
Malabika Roy Scientist ‘F’ and Head

13.2% (NFHS 3) unmet need for contraception of which about 50% is for spacing methods
Introduction of any additional method in NFWP increases contraceptive use by 3.3% & would fulfill unmet need by 1.7%
Annually 78% conceptions are unplanned & 25% unwanted
8% maternal mortality related to abortion
Need for contraception

India in World Population India in World population
Source: Series – 1, India, Provisional Population Totals, Paper-1 of 2011 (http://www.censusindia.gov.in)

Population share of States- Census 2011
Source: Series – 1, India, Provisional Population Totals, Paper-1 of 2011 (http://www.censusindia.gov.in)
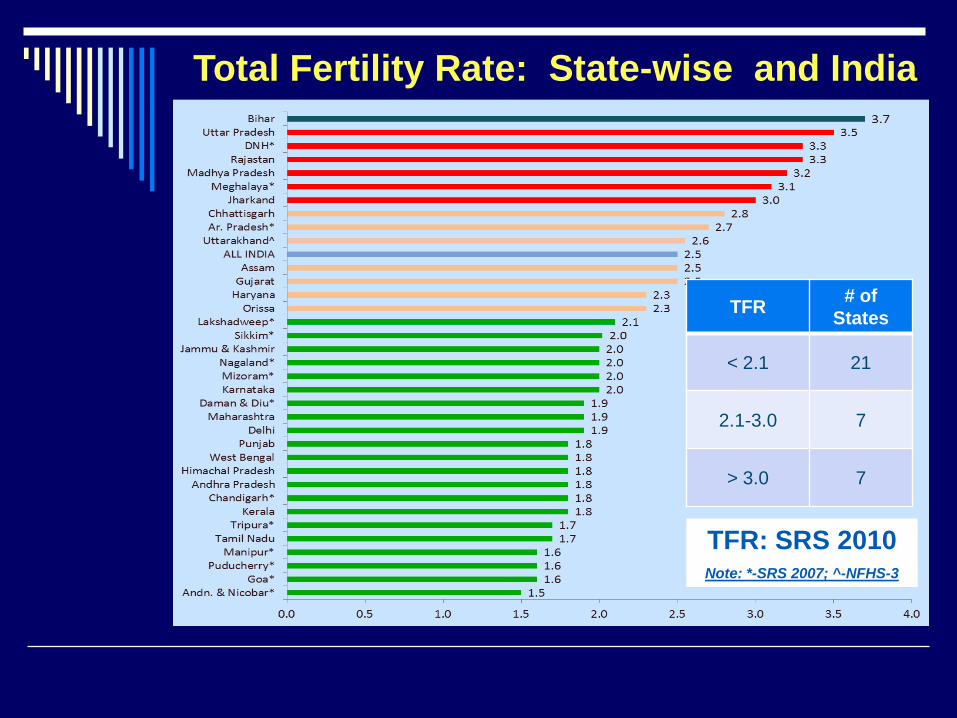
TFR: SRS 2010 Note: *-SRS 2007; ^-NFHS-3
TFR # of States
< 2.1 21
2.1-3.0 7
> 3.0 7
Total Fertility Rate: State-wise and India
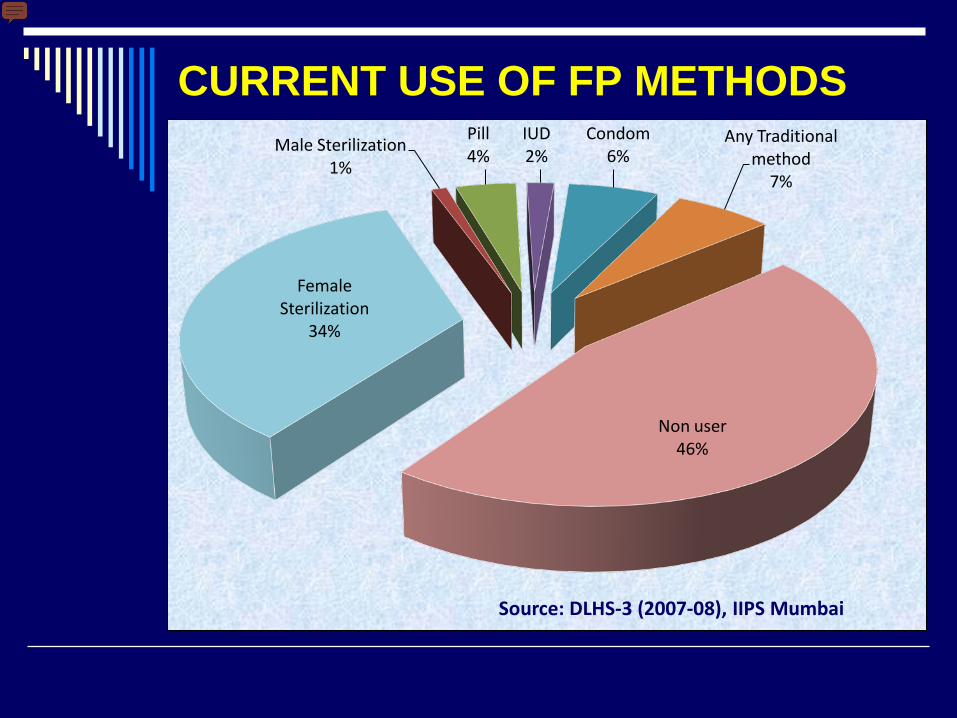
Female Sterilization
34%
Male Sterilization 1%
Pill 4%
IUD 2%
Condom 6%
Any Traditional method
7%
Non user 46%
CURRENT USE OF FP METHODS
Source: DLHS-3 (2007-08), IIPS Mumbai
Utilization and quality of family planning services in rural areas of India: A
community based cross sectional study- An ICMR task force study
Indian J Med Sc, 57 (7); 303-10: 2003
B.S.
OBJECTIVE To obtain information from rural women regarding their contraceptive knowledge, practices and utilization of services and assess quality of services provided.

Number of women covered in the survey
Eligible women - 1,17,465 Current user of Family Planning - 14,276 Non user of Family Planning Method - 17,082
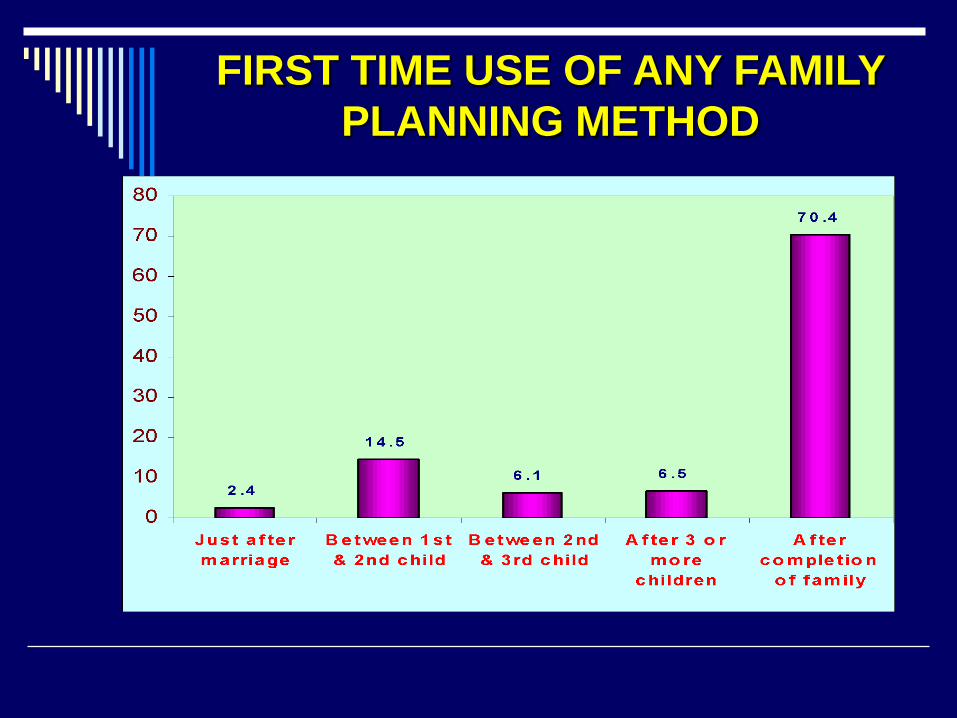
FIRST TIME USE OF ANY FAMILY PLANNING METHOD

Contraceptive use and desire for more children in rural districts of two States
in India - A cross sectional survey
Objective To study the association between met desire for children and contraceptive acceptance

TTAABBLLEE :: NNUUMMBBEERR OOFF WWOOMMEENN CCOOVVEERREEDD FFOORR VVAARRIIOOUUSS CCOOMMPPOONNEENNTT
State District Eligible women Uttar Pradesh
Barabanki Allahabad Kanpur Meerut Ghaziabad TOTAL
5276 3935 4036 4283 4814
22,344
Tamil Nadu
Chengai MGR N.Chengelpet Cuddalore Madurai Vellore Cheyyar HUD TOTAL
4139 5741 4805 5022 5368 4995
30,070
Total 52,414

Current age, Age at marriage and age of 1st conception

Per cent women expressing desire for one male and one female child by age

55.8
73.779.7
8.618.5
31.1
0
20
40
60
80
100
15-24 years 25-34 years 35-45 years
Perc
enta
ge
Age
Uttar Pradesh Tamil Nadu
Per cent women expressing desire for 3 or more child by age

COMPARATIVE DATA ON LIVING CHILDREN, DESIRED CHILDREN AND CONTRACEPTIVE USE
IN TWO STATES IN INDIA
Summary: Promote small family norm and make people aware of the benefits of FP

Community based survey on induced abortion and adoption of contraception
in 28 districts of India (AN ICMR TASK FORCE STUDY)
Indian J Med Sc, 56 (11); 478-84: 2004
Objective: To assess women's perceptions, knowledge, practices and utilization of
services for induced abortion.

REASONS FOR INDUCED ABORTION

PRECENTAGE OF WOMEN ACCEPTING POST-ABORTAL CONTRACEPTIVE
Contraceptive use mentioned (% ) Total acceptors………………………...48.9 IUD …..……………………21.9 OCP …..……………………15.3 Tubectomy (minilap)…….28.5 Tubectomy (laproscopy)..20.6 Others………………………13.7

REASON FOR NOT ACCEPTING POST-ABORTAL CONTRACEPTIVE
NON ACCEPTORS (%) (Multiple response) 51.1
Do not want 12.7 Husband objection 32.3
Private doctor do not offer 6.9 Family planning method also fail 3.7 Husband has vasectomy 1.3 Husband use condom 8.4 NR 20.7

1.9
1.6
2.1
0.8
0.5
0.9
0 1 2 3 4
Total
Urban
Rural
Wanted TFR Unwanted TFR
WANTED AND ACTUAL FERTILITY RATES
NFHS-3, India, 2005-06
If unwanted fertility is averted
TFR will reach replacement level.

RISING INSTITUTIONAL DELIVERY
7.39
31.58
73.29
90.37
100.78 106.97 108.70
0
20
40
60
80
100
120
2005-06 2006-07 2007-08 2008-09 2009-10 2010-11 2011-12
In la
khs
JSY BENEFICIERIES: 2005-06 to 2011-12
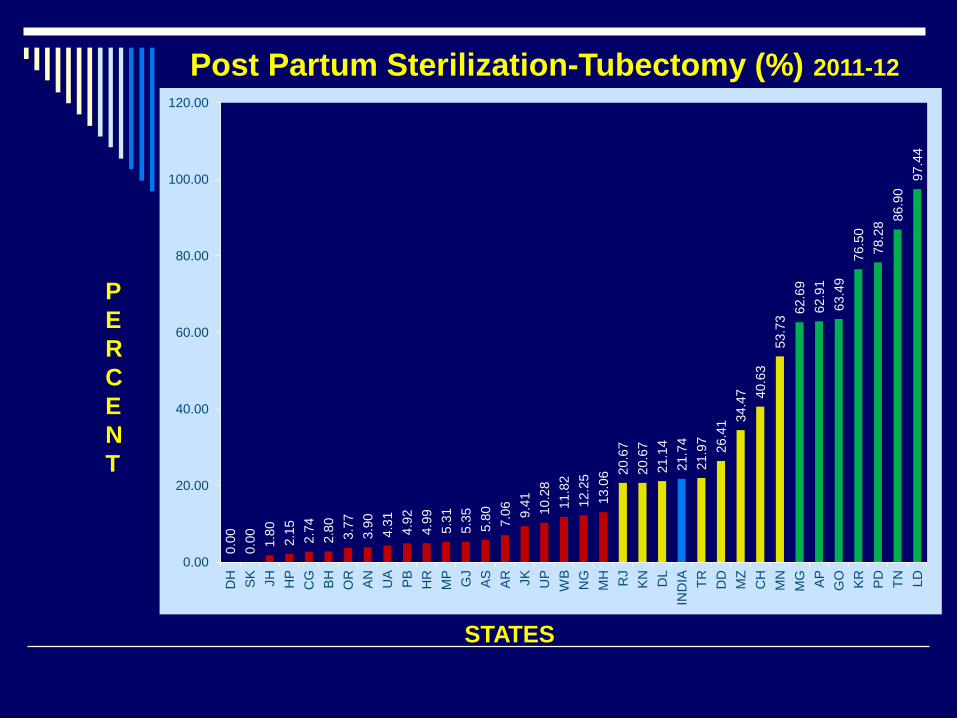
Post Partum Sterilization-Tubectomy (%) 2011-12
STATES
P E R C E N Tnt
0.00
0.
00
1.80
2.
15
2.74
2.
80
3.77
3.
90
4.31
4.
92
4.99
5.
31
5.35
5.
80
7.06
9.
41
10.2
8 11
.82
12.2
5 13
.06 20
.67
20.6
7 21
.14
21.7
4 21
.97 26.4
1 34.4
7 40.6
3 53
.73 62
.69
62.9
1 63
.49
76.5
0 78
.28 86
.90
97.4
4
0.00
20.00
40.00
60.00
80.00
100.00
120.00
DH
SK
JH
H
P C
G
BH
OR
AN
U
A PB
H
R
MP GJ
AS
AR
JK
UP
WB
NG
M
H
RJ
KN
DL
IND
IA
TR
DD
M
Z C
H
MN
M
G
AP
GO
KR
PD
TN
LD

Salient FACTs
If the current unmet need for family planning in India
could be fulfilled over the next 5 years, we can:
Avert 35,000 maternal deaths
Avert 12 lacs infant deaths
Save more than Rs.4450 crores
Saving of Rs.6500 crores if safe abortion services
are coupled with increased family planning services.
SOURCE: GoldieSJ, Sweet S, Carvalho N, Natchu UCM, Hu D (2010) Alternative Strategies to reduce maternal mortality in India: A cost-effective analysis, PLoS Med 7(4): e1000264. Doi:10.1371/journal.pmed.1000264

KEY POINTS in the census Positives Steepest fall in growth rate since independence:
17.64% decadal growth during 2001-2011 as compared to 21.54% during 1991-2001.
Annual growth rate declined sharply from 1.97% to 1.64%. Marked decline in fertility
3.08% decline in proportion of 0-6 child population Least population added compared to the previous decade:
18.15 crores added compared to 18.23 crores in previous decade
Concerns UP and Bihar together share 25.1% (one fourth)
of country’s population 8 EAG states have 45.87% of India’s population.
KEY Challenges
Acceptance of IUCDs have not improved significantly
Shortage of trained service providers. Lack of regular family planning services (fixed day)
at sub-district level. Increase in institutional deliveries through JSY is
not tapped fully for post-partum family planning. Services of private providers not brought into the
fold optimally. Lack of managerially skilled personnel for effective
monitoring of the programme. At Many areas in the country community is not
aware of benefits of the Family Planning (weak IEC).

THRUST areas – 12TH FIVE YEAR PLAN (2012-2017):
Strengthening Family Planning (FP) service delivery, especially post -partum FP in facilities with high case load
Promotion of spacing methods as a major initiative Introduction of newer contraceptives- to address
unmet need Community based distribution of contraceptives
through Accredited Social Health Activists (ASHAs) Involving private/NGO /CBO facilities to improve
the provider base for FP services Vigorous advocacy for family planning at all levels
specially at the highest political level

STRATEGIES –to address thrust areas
High focus approach ( 6 Northern states & 264 HFDs)
Operationalising ‘delivery points’ first , expand to other facilities.
Strengthening HR structures from national to the district level: Programme management structure
Counsellors at high delivery load facilities
Delivery of contraceptives to the door step by ASHA.
Roll out of ML 375 IUCD as a short term spacing method,
Ensuring vigorous advocacy Development of BCC tools (including IEC materials) for spacing between children
Development of IEC materials for IUCD
Enlisting more number of private providers/ NGOs /CBOs for provision of services (social franchising/ accreditation)
Initiatives in FP services Repositioning Family Planning for improvement in
maternal and child health along with population stabilisation. Popularising spacing methods (IUD 380-A) with
emphasis on training of providers for skilled insertion through ANM Establishment of QACs at state and district levels for
ensuring quality of family planning services Promoting Post Partum Family Planning
services Introducing revised compensation scheme for
FP services Introducing National Family Planning
Insurance Scheme Advocating population stabilisation through debate
in parliament and other national council meetings on population Research in newer contraceptive technologies to
expand the contraceptive choices.

Acknowledgements
SK Sikdar, Deputy Commissioner (FP), Ministry of Health and Family Welfare, Government of India
BS Dhillon, Scientist ‘E’ , RCH, ICMR Roopa Hariprasad, Scientist ‘C’, RCH, ICMR

Indian Council of Medical Research
Thank You