Embed Size (px)
Citation preview

Version 01 1
REPORT of the Regulatory/HTA/Payer EAP
01|06|2021
Dalia Dawoud, Isabelle TONGIO, Peter Dailey, Pall Jonsson, Colm LEONARD
Session 2

Version 01 2
This project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking
under grant agreement No 820755. This Joint Undertaking receives support from the
European Union’s Horizon 2020 research and innovation programme and EFPIA and
bioMérieux SA, Janssen Pharmaceutica NV, Accelerate Diagnostics S.L., Abbott, Bio-Rad
Laboratories, BD Switzerland Sàrl, and The Wellcome Trust Limited.

Version 01 3

Version 01 4
Table of contents 1. Summary .......................................................................................................................................... 5
2. Background ...................................................................................................................................... 5
2.1. The Expert Advisory Panel (EAP) ............................................................................................................ 5
2.2. Membership ............................................................................................................................................ 5
2.3. Conduct of meetings ............................................................................................................................... 6
3. Panel Session ................................................................................................................................... 7
3.1. Second EAP session (11 March 2021, webinar virtual meeting ) ........................................................... 7
3.1.1. Attendees ............................................................................................................................................. 7
3.1.2. Requests .............................................................................................................................................. 7
3.2. Detailed EAP discussion and feedback ................................................................................................... 7
3.2.1. VALUE Dx progress............................................................................................................................... 7
3.2.2. COVID 19 and its impacts on diagnostics, AMR and healthcare ......................................................... 8
3.2.3. Epidemiologic and cost data required for the economic evaluation alongside the clinical trials ...... 9
3.2.4. Designing a lifetime health-economic model for respiratory-tract infection diagnostics ................10
4. Appendix ........................................................................................................................................ 13
4.1. VALUE Dx Regulatory/HTA/payer Expert Advisory Panel Session 2: Meeting Minutes .......................13

Version 01 5
1. Summary This report summarises the proceedings of the second session of the Regulatory/HTA/Payer Expert
Advisory Panel (EAP), which aims to advise and support IMI VALUE-Dx in a range of activities to ensure
that the activities and outputs of the project will not only be of the highest scientific quality but will also
have meaningful applicability in the regulatory, HTA and payer contexts. The EAP has been established
under Work Package 5 (WP5) by partner organisations leading and contributing to Task 5.1.
The meeting took place on 11 March 2021 where input on general topics as well as on health economics
focused topics related to WP5 work was provided. This included feedback on the impact of COVID 19 on
the awareness of diagnostics and their value to society.
The next EAP will be held, if required by the consortium, approximately 6 months after this second
meeting.
2. Background
2.1. The Expert Advisory Panel (EAP)
A Regulatory and Health Technology Assessment (HTA) Expert Advisory Panel (EAP) has been established
to ensure the relevance and usability of VALUE Dx activities and outputs to regulators and HTA agencies
throughout the project. The core role will be to inform and advise the activities in work package 5 ensuring
that all relevant perspectives, expertise and concerns are considered. The EAP has the following aims for
the duration of the project:
• Engage actively in discussions, provide feedback and input into topics brought forth by the work
packages, including providing advice on research activities and outputs.
• Ensure that the VALUE Dx outputs are not merely of high scientific quality but will have meaningful
applicability in the regulatory, HTA, and payer contexts.
The EAP consists of individual experts from different European countries with regulatory, HTA (Health
economic), payer or clinical expertise. Some of the experts also have experience in antimicrobial
resistance (AMR) and diagnostics. At the start of the project, it was planned that there would be 5-7
meetings in total over the 4-year period: 3-4 virtual and 2-3 face-to-face meetings.
The Regulatory /HTA/Payer Expert Advisory Panel acts in an advisory capacity within the context of
VALUE-Dx on research, outputs and deliverables. It has no formal legal responsibilities or fiduciary duties
to VALUE-Dx or its partner organisations.
2.2. Membership
The EAP currently has 13 standing members (see below) who are asked to participate in meetings and
input in other tasks such reviewing of documentation and completing surveys using their expertise. NICE

Version 01 6
and the working group for Task 5.1. coordinates all EAP activities. There is some flexibility in the
membership of the EAP with the opportunity to include additional people depending on the needs of the
project.
Expert Advisory Panel members
Name Organisation Stakeholder group/perspective
Colm Leonard (Chair) NICE/NHS Clinical/HTA specialist
Dalia Dawoud (Co-Chair)
NICE HTA /Health Economics
Jordi Carratala
Bellvitge Hospital Clinical specialist
Alec Morton University of Strathclyde Health Economics/HTA
Abigail Colson University of Strathclyde Health Economics/HTA
Marcin Czech Institute of Mother and Child in Warsaw
Health Economics &former Vice-Minister for Health
Rossana Tarricone Bocconi University Health Economics /HTA/healthcare research
Lorenzo Mantovani University of Milano-Bicocca Health economics/health researcher
Wim Goettsch Utrecht University and Zorginstituut Nederland
HTA/HE
Joke Derksen Zorginstituut Nederland HTA
Sun Robin French Ministry of Health Payer
Piet Vancraeynest RIZIV – INAMI
HTA/Payer
Falk Ehmann European Medicines Agency (EMA)- chair of Innovation task force
Regulatory
2.3. Conduct of meetings
Advice is provided on concepts and issues specifically relating to VALUE-Dx. Any feedback/advice that is
provided by members of the EAP is non-binding and will not be recognised as formal Scientific Advice, or
as reflecting the official view or position of the organisations that employ the members of the EAP. All
attending members will maintain confidentiality with meetings run under the principle of Chatham house
rules, according to which information disclosed during a meeting may be reported by those present, but
the source of that information may not be explicitly or implicitly identified. The Panel meetings are open
to the VALUE-Dx Members who can act as observers.
Topics and queries for advice were canvassed by Task 5.1 WG by emailing WP leads and WP 5 task leads
with dates of sessions and request for advice by the EAP. A proforma template was used to give brief
Version 01 7
detail around specific queries to enable theming and ensure correct expertise is available within each
session. The VALUE-Dx Partner requesting advice for selected questions was asked to attend the session
and provide an outline and background on the issue for advice/consideration by the EAP.
3. Panel Session
3.1. Second EAP session (11 March 2021, webinar virtual meeting )
The second panel session of the EAP was held virtually on 11 March 2021, lasting 2 hours. The full panel
session minutes can be found in Annex I. The meeting provided an update on the progress achieved so far
within VALUE Dx. WP5 delivered short presentations on their specific aims, with a focus around clinical
and economic value frameworks including health economics and assessment policy for WP5. The full
presentation is available below.
EAP Session 2 Slides
3.1.1. Attendees
EAP members: Colm Leonard (Chair), Dalia Dawoud (Co-Chair), Alec Morton, Abigail Colson, Marcin Czech,
Lorenzo Mantovani, Sun Robin, Falk Ehmann (n=6)
Value Dx Consortium presenters: Colm Leonard, Jean-Louis Tissier, Herman Goossens, Simon van der Pol, Fernando Antonanzas Session facilitators/attendees with enhanced access: Dalia Dawoud, Maarten Postma, Thea van Asselt, Peter Dailey, Isabelle Tongio, Till Bachmann
3.1.2. Requests
Requests for input were received from WP5 (3 topics: 1 strategic, 2 operational). These were prioritised
by Task 5.1 working group based on time of deliverable, structured content and flow of session. Presenters
provided slides with the aim, context and question for discussion.
3.2. Detailed EAP discussion and feedback
3.2.1. VALUE Dx progress
Herman Goossens (HG) gave a presentation to the Panel about Value Dx progress so far, including
reflecting on the continued impact of COVID-19 on the progress of the project. HG briefly described the
impact of the pandemic on the planned clinical trials which will be conducted within VALUE Dx and the
planned start dates of each of the two trials. HG also provided an update on the progress of the point
prevalence audit surveys (PPAS).

Version 01 8
He also reported that the clinical algorithm (CA) has been developed and validated in WP1, using the large
databases of the patient-level information. Data from the point prevalence survey were all included in the
clinical algorithm, divided by viral and bacterial pathogens. The next steps for this work will focus on
working with WP5 to integrate the cost evaluation assessment into the CA development. Publication of
this CA will be dependent on validation with real-life data, however, little else is seen but COVID-19 at the
moment.
HG also reported that integrated business and sustainability model for VALUE-Dx now completed and
consists of three, closely interconnected parts: sustainable model of clinical networks, business plan for
creating and maintaining a biobank of clinical specimens, strains and DNA and business plan for creating
and maintaining an integrated database. This will be presented and discussed during VALUE-Dx Annual &
General Assembly meeting (30-31 August, Bologna). It will fit under the umbrella of a new organisation
that will be based in the Netherlands and will be launched in summer as the European Clinical Research
Alliance on Infectious Diseases (ECRAID)
3.2.2. COVID 19 and its impacts on diagnostics, AMR and healthcare
COVID-19 has highlighted the importance of Diagnostics through the PCR and antigen tests. In a few
months timeframe, most people have heard about Diagnostics when previously the role and impact of
diagnostics was poorly understood. In addition, rapid procedures have been put in place by policy
makers/healthcare organisations to speed their availability in the market. The EAP were asked to
consider the situation after COVID-19 and make suggestions regarding the possible ways to maintain
this high level of contribution of diagnostics towards populations, public and government bodies and
how it can be translated in a better recognition of the value.
Feedback themes
Country-to-country variation The EAP highlighted that the situation will vary on a country-by-country basis. In the UK, where progress
has been made in controlling the spread of infection and the opening up of schools with the aid of
widespread use of lateral flow testing (LFT), the interest in and awareness of the benefits for diagnostic
tests may well be maintained beyond the pandemic. Alec Morton (AM) also explained that universities
in the UK are considering the widespread use of these tests also to facilitate return to face-to-face
teaching while protecting their employees and students. The experience from the US also showed that
testing can make a difference and help protect students in university communities.
Sun Robin (SR) reflected that the situation in France means that the use of diagnostic tests is continuing
to expand with the move from PCR testing to salivary tests and the move towards the approval of other
diagnostic tests. So, population awareness is also increasing, and this is likely to drive public interest and
influence future attitudes towards adoption of widespread testing. However, Marcin Czech (MC)
reported that situation in Poland was not as favourable as in the UK and France, with increasing number
of cases PCR and antigen testing is still the basis of management practices and no move yet to use LFT.
Fast adoption of new diagnostic technologies The EAP emphasises that the increased awareness as well as simplification of the market access process
may result in faster adoption of new diagnostic technologies in the future. The pandemic has

Version 01 9
accelerated attempts to standardise the laboratory procedures and approval processes in Poland,
according to MC. AM also explained that some organisations will fund the use of rapid diagnostics to
protect themselves against liability. This applies to universities as explained above but it also potentially
spills over to non-COVID testing.
Need for educating the public CL has commented that the pandemic has provided an opportunity to educate the public about diagnostics tests, with basic concepts like sensitivity and specificity being explained in simple terms as is currently being done in the UK by some academic professors in mainstream media and on different social media channels to simplify these concepts and explain to the public.
3.2.3. Epidemiologic and cost data required for the economic evaluation alongside the clinical trials
Fernando Antonanzas (FA) presented 3 operational questions to the EAP relating to the economic
evaluation being undertaken alongside the clinical trials (task 5.3) The question focused on the data
sources required for adapting the model to different countries’ contexts. The first question asked whether
the EAP members’ jurisdiction require cost effectiveness information to make funding decisions, in which
case there would be interest in getting the results of the modelling specific to their jurisdiction. The second
question asked if the EAP members know the key sources of unit costs for health care interventions in
their jurisdictions, particularly the costs of tests. The final question asked the EAP whether they would be
able to facilitate the collection of these unit costs for the items needed in the short-term economic
evaluation of WP5 (Tasks 5.3 and 5.4).
FA gave examples of the unit costs required for the models and these included:
• Costs of diagnostic methods (per test costs, Investment costs (e.g. devices)
• (Additional) testing costs/complimentary explorations
• Emergency room costs
• Visit costs
• PCR costs,
• Microbiology tests in central laboratory costs
• Antiviral treatments costs of each prescribed treatment
• Antibiotic costs of each prescribed treatment
• Symptomatic medication costs (either prescribed or over-the-countrer)
• Time spent by doctors/nurses/pharmacists
• Antibiotic/medicine costs
• Hospitalization costs
• Societal costs (sick leave/productivity losses, informal care, patient travel time)
Additionally, epidemiological data are needed particularly data on the proportion of patients attending
with the conditions relevant to the trial (i.e. with lower respiratory tract infection where cough is the
predominant symptom (<28 days) OR upper respiratory tract infection where symptoms of an acute sore
throat (<14 days) or difficulty swallowing are the dominant symptoms; AND for whom the responsible
clinician is considering or has decided to prescribe an antimicrobial) with respect to the total number of

Version 01 10
patients seen by physicians. This information will give an idea in relation to where the new diagnostic
could be used in medical practice.
Feedback
It was highlighted that some countries have national lists of unit costs (e.g. the Netherlands) while others
do not have such data and this will make it difficult to adapt the model to their jurisdictions. Marcin Czech
(MC) explained that for Poland, the data is available on the national level from National Health Fund
(payer) and the majority of the required unit costs will be available. The epidemiological data would be
more challenging as these are not electronically available within Poland.
AM explained that the UK has these unit costs available on national level. Also, countries that have DRG-
based system for payment should have these data available but how difficult it is to access them will differ.
He also explained cross-country comparisons have their own complexities and it is not straightforward.
FA explained that the main aim is to adapt the model to each country’s jurisdiction rather than
undertaking cross-country comparisons.
3.2.4. Designing a lifetime health-economic model for respiratory-tract infection diagnostics
Simon van der Pol (SvdP) presented 5 operational questions with subpoints in relation to Task 5.4 that is
focused on developing a lifetime economic model to assess the cost effectiveness of rapid diagnostics and
relates to the following aim:
Aim: Develop new health economic models to determine the long-term clinical, public health and economic
impact of diagnostics in terms of AMR prevention with the support of HTAs reflecting the integral value of
diagnostics.
The questions related to the following main topics:
• The demographic model
o What would the panel consider relevant demographic parameters related to community-
acquired respiratory tract infections, besides those already included?
o Consultation data for the emergency room setting is difficult to obtain, does the panel have
ideas on getting data for this setting?
• The consultation model
o Would the panel consider the model structure to be appropriate?
o Assumption: transmission and consultation rates do not change based on the introduction
of point-of-care diagnostics
• The AMR forecasting model
o Does the EAP find it appropriate to forecast AMR based on statistical forecasting methods,
rather than mechanistic dynamic transmission?
o Assumptions:
▪ Number of infections does not change, only the percentage of resistant infections.
▪ Elasticity of 1 between antibiotic consumption and AMR.
o What is the relevance of the following outcomes? :
▪ AMR rates
▪ Clinical effects of future AMR rates
▪ Future AMR-related costs.

Version 01 11
o This will be subject to considerable uncertainty, does the panel have ideas on how to
handle this?
• Outcomes
o What would the panel consider to be other relevant aspects of value we should cover in
this study?
Feedback
The EAP members provided input to each of these questions in turn.
• Demographic model
MC explained that in Poland it will be difficult to provide this data. CL reported that in the UK there is
emergency care data and targets available from the Hospital Episode Statistics (HES). AM commented that
it would be tricky to have this data on the European level and the ECDC would be the first port of call to
get this data. CL also suggested the European Society of Emergency Medicine as a potential source on the
European level.
CL stressed the importance of including smoking status in the model as it affects outcomes for patients.
Vaccination status is another potential characteristic that can be affect outcomes and care provided.
• Consultation model
AM commented that the approach chosen for modelling is an appropriate one, as microsimulation will
allow incorporation of patient characteristics. The assumptions of no change in consultation rates and
transmission were discussed in more detail and the potential of these to be affected due to behaviour
change, and the potential for re-consultation rates to change was also flagged. CL commented that this
assumption may not always hold and can go in either direction, as patients might be encouraged to go to
their GP to get the point of care test. It was also suggested that if the model is flexible to accommodate
assessing the value of using these point of care tests earlier in the disease pathway (e.g. at community
pharmacies), it would be helpful.
• AMR forecasting model
The EAP enquired whether the link between the antibiotic utilisation and AMR levels is based on an
assumption and SvdP explained that it is. Abigail Colson (AC) explained that the team at Strathclyde has
been working in this area using statistical modelling and also expert elicitation. She also explained that
the assumption relating to elasticity will be very much dependent on what else is happening, for example
new clinical guideline recommendations, so there will be a lot of variability around that. AM also
explained that reducing antibiotic consumption on its own is an important aim that governments are now,
and specifically the UK government, are all interested in, so would be an important element of value to
demonstrate. CL explained that it will be important to take into account the effect of the pandemic itself
on the prescribing of antibiotics as there is some evidence of reduced prescribing in certain settings, and
overprescribing of antibiotics in patients admitted to hospital with COVID-19 pneumonia.
• Outcomes
AM reported that an Office of Health Economics (OHE) working paper that discussed the additional value
elements to be considered in the assessment of AMR-related technologies is available and would be a

Version 01 12
valuable source to consult to identify the additional value elements to consider. Environmental impact
was another outcome suggested.
Version 01 13
4. Appendix
4.1. VALUE Dx Regulatory/HTA/payer Expert Advisory Panel Session 2: Meeting Minutes
March 11th- 2-4 pm (GMT)
In attendance
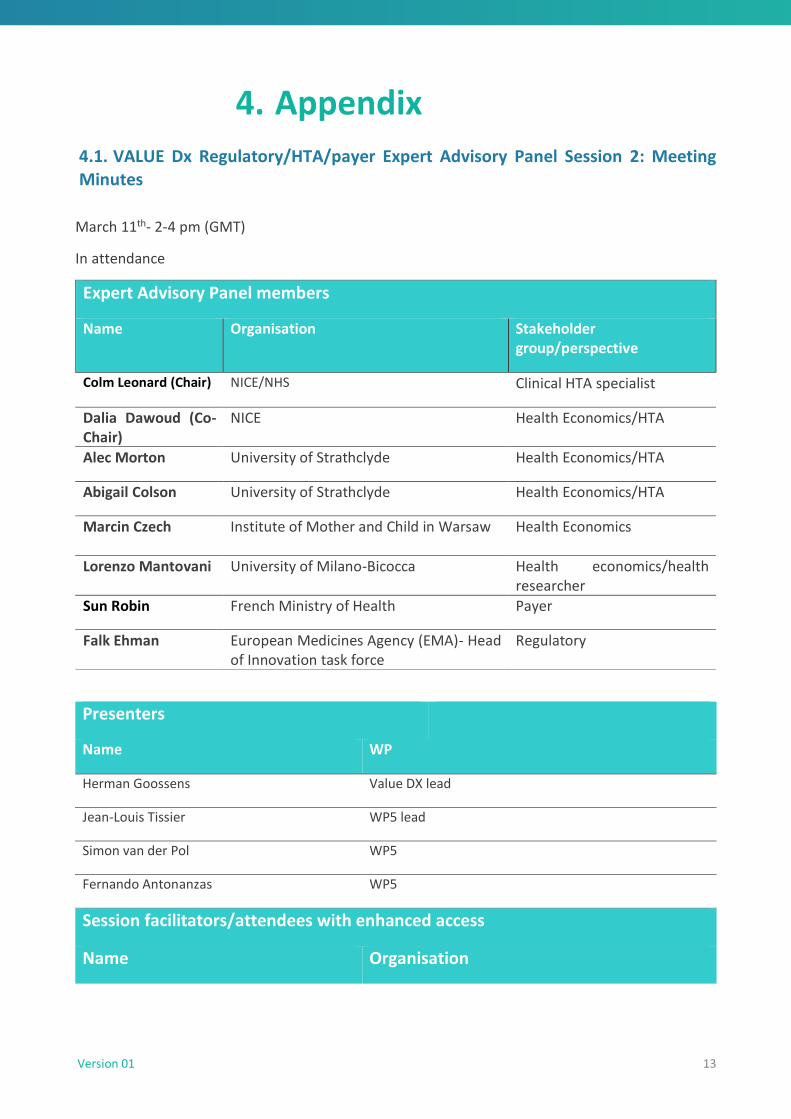
Expert Advisory Panel members
Name Organisation Stakeholder group/perspective
Colm Leonard (Chair) NICE/NHS Clinical HTA specialist
Dalia Dawoud (Co-Chair)
NICE Health Economics/HTA
Alec Morton University of Strathclyde Health Economics/HTA
Abigail Colson University of Strathclyde Health Economics/HTA
Marcin Czech Institute of Mother and Child in Warsaw
Health Economics
Lorenzo Mantovani University of Milano-Bicocca Health economics/health researcher
Sun Robin French Ministry of Health Payer
Falk Ehman European Medicines Agency (EMA)- Head of Innovation task force
Regulatory
Presenters
Name WP
Herman Goossens Value DX lead
Jean-Louis Tissier WP5 lead
Simon van der Pol WP5
Fernando Antonanzas WP5
Session facilitators/attendees with enhanced access
Name Organisation

Version 01 14
Peter Dailey FIND
Isabelle Tongio BioMerieux
Maarten Postma UMCG
Thea van Asselt UMCG
Till Bachmann University of Edinburgh
Meeting Notes
1. Session outline and introductions Colm Leonard (CL- Chair)
Colm Leonard (CL) opened the meeting, welcoming the Expert Advisory Panel (EAP) members to the
second session and giving brief overview of how the panel would operate through the Zoom
environment. CL introduced the new members of the working group that oversees the operational
planning of the EAP meetings: Dalia Dawoud (DD) (NICE) and Peter Dailey (PD) (FIND). He then outlined
the agenda for the session.
2. Update on the progress of Value Dx Herman Goossens (HG)
Herman Goossens (HG) gave a presentation to the Panel about the progress achieved during the last 6
months since the first EAP session. He provided a quick recap of the objectives of ValueDx, the
organisations involved and the nature of the public and private organisation of the consortium, the WP
structures, their inter-dependencies and overall remits/scopes. HG then gave an update on the progress
of the project around the point prevalence audit surveys and their extension due to COVID-19. HG briefly
described plans for the clinical trials which will be conducted within VALUE Dx and flagged the delay in
their starting time due to the impact of the pandemic. He explained that for PRUDENCE trial, recruitment
start date has been postponed from January to September 2021, due to the pressures on primary care
with the continuing COVID-19 pandemic, the vaccine roll-out and lack of flu circulating. The team is also
currently reviewing how to incorporate a BD Veritor™ SARS-CoV-2 test into the diagnostic algorithm for
PRUDENCE with regard to possible varying COVID-19 situations across Europe later this year.
In relation to ADEQUATE trial, HG explained that a data collection process has been completed in close
communication with WP3 and WP5 to build a health-economic framework to assess and demonstrate the
value of diagnostics both for individual patients and for public health impact by reducing antibiotic use
and subsequent antibiotic resistance among patients. He also reported that the first patients are
expected to enrol as of March-April 2021.
3. WP5 objectives and strategic questions Jeal- Louis Tissier (JLT)
EAP
JLT presented a recap of the objectives for Work Package 5 (WP5) which includes clinical and economic
value frameworks including health economics and assessment policy. He then presented a strategic
question to the EAP which is related to the following WP5 aim:
Aim: To develop innovative frameworks to optimise assessment of the clinical and economic value of
diagnostics and facilitate sustainable funding systems over the entire lifetime of the diagnostic.

Version 01 15
Questions asked:
COVID-19 has highlighted the importance of Diagnostics through the PCR and antigen tests. In a few
months, most of people have heard about Diagnostics when previously the role and impact of
diagnostics was poorly understood. In addition, rapid procedures have been put in place by policy
makers/healthcare organisations to speed their availability in the market.
What do you think about the situation after COVID-19? What do you suggest to maintain this high
level of contribution of Diagnostics towards populations, public and government bodies. And how can
it be translated in a better recognition of the value?
The EAP discussed the question posed and provided their opinions. Points of discussion included:
• COVID pandemic continued to place testing and diagnostics in the spotlight. It has increased the
public awareness of the importance of testing to identify asymptomatic cases and reduce
transmission.
• This has been particularly observed due to the reliance on the use of the rapid lateral flow testing
to facilitate reopening society. For example, the reopening of schools in England has relied on
mass testing of students before return to classroom and mandating twice-weekly testing
thereafter as a condition to continued attendance.
4. WP5 - Operational questions Fernando Antonanzas
Fernando Antonanzas (FA) presented 3 questions to the EAP relating to Task 5.3 (Economic evaluation
alongside clinical trial). These related to the specific aim of Value DX to:
1. Aim: Develop health-economic models to determine the short-term economic impact of diagnostics in
terms of AMR prevention with the support of HTAs reflecting the integral value of diagnostics.
The questions were discussed by the EAP and responses provided. A number of suggestions for agencies,
organisations and groups were provided. It was agreed that contact via Email following the meeting
would be the best approach to providing this information to the team.
5. WP5 - Operational questions
Simon van der Pol
Simon van der Pol (SvdP) presented an overview of the epidemiological and economic models being
developed within the context of task 5.4. The following questions relating to the different aspects of the
model development process were posed to the panel members:
• Demographic model
• Consultation model
• Antibiotic resistance forecasting
• Outcomes
The panel members shared their experiences and provided input in relation to each of the
aforementioned questions, and sign-posted the team to other potential sources of information.
6. Close
Colm Leonard (CL)
Dalia Dawoud (DD)
CL thanked all Panellists and presenters for their participation in the second Panel session and DD invited
the panel members to provide their feedback on the running of these sessions and how it can be
improved.

Co
pyr
igh
t 20
19 V
ALU
E-D
x
www.imi.europa.eu
www.imi.europa.eu
www.value-dx.eu
www.value-dx.eu





























