Embed Size (px)
Citation preview
Request for Proposal Intensive In-Home Services
RFP #2013-302
Overview
Alliance Behavioral Healthcare is soliciting proposals from network providers to deliver Intensive In-
Home services for children and adolescents through the age of 20 with mental illness and/or substance
abuse diagnoses in Cumberland, Durham, Johnston and Wake counties. In order to be considered for a
contract through this RFP process respondents must be able to demonstrate that they offer or will offer
a continuum of care, including outpatient therapy and medication management, within the Alliance
county(ies) where Intensive In-Home (IIH) is to be provided.
The objective of the RFP is to select quality organizations that:
• Demonstrate evidence-based approaches to address the diversity and cultures of the population
served.
• Identify the preferences of individuals and families in the design of services and supports
through development and utilization of person-centered planning.
• Facilitate the development and utilization of natural supports.
• Facilitate the use of services that foster resiliency, support stable housing, and address the
development and maintenance of healthy social networks and skills, employment, and school
performance.
If awarded a contract, selected network providers may consider expansion of this service into additional
sites within the Alliance catchment area. Providers who wish to expand must identify this plan in their
proposal.
Respondents to this RFP must meet the following minimum requirements:
Be current network providers in good standing with Alliance Behavioral Healthcare, other
LME/MCOS, all applicable federal and state oversight agencies and the organization’s
accrediting body.
Currently providing Intensive In-Home Services from a credentialed site in the Alliance
catchment area.
IIH Request for Proposal RFP #2013-302
2
Submit a complete and timely RFP response that includes all required elements and a well-
designed and detailed implementation plan (including transition timeline) that clearly articulates
tasks, time frames, and expected results.
Have at least one year of experience successfully providing evidence-based Intensive In-Home
Services from a credentialed site in the Alliance catchment area, with a preference for providers
with at least two years’ experience.
Respondents who meet the above minimum criteria will proceed to a desk review of the written
proposal.
Note: Providers who are contracted to deliver services from credentialed sites outside of the four
county area and who are currently serving Alliance enrollees should not respond to the RFPs. Alliance
will enter into out-of-network agreements if necessary to ensure that Alliance enrollees who reside
outside of the catchment area have access to these services.
During the evaluation, preference may be given to bidders that meet the following criteria:
Demonstrated capacity to implement the requirements specified in the Scope of Work in this
RFP.
Have a solvent and financially viable organization with a history of financial stability that has
sufficient financial and administrative resources to implement and operate the services specified
in this RFP.
Have a history of serving a monthly average of at least six per team in Intensive In-Home
Services, based on claims since 2/1/2013. Although team size is not a determining factor,
organizations must demonstrate experience, financial viability, and the ability to provide the
service in accordance with the service definition and the criteria in this RFP.
History of submitting timely and complete requests for prior authorization that contain all
administrative and clinical requirements (i.e. does not have an excessive number of
administrative denials).
Demonstrated ability to timely and successfully submit clean claims using the Alpha provider
portal or 837s.
Have a well-developed quality management program that monitors and improves access, quality
and efficiency of care.
Have human resources and management support necessary to effectively recruit and retain
clinical and administrative qualified professional staff.
IMPORTANT NOTE: All currently contracted Alliance network providers of Intensive In-
Home Services who are interested in providing Medicaid-funded IIH services in the
Alliance catchment area after December 31, 2013 must respond to this RFP in order to
be considered for renewal of their 2013 Medicaid-funded contract with Alliance for this
IIH Request for Proposal RFP #2013-302
3
service. Providers with state-funded (IPRS) contracts for this service must have a
Medicaid-funded contract with Alliance for the service in order for the state-funded
(IPRS) contract to be renewed in 2014. Providers that do not plan to respond to the RFP
must submit at a minimum a 90 day plan for transition of their Medicaid consumers to
other providers of care. This transition plan should be submitted as soon as possible,
but no later than the due date for responses to this RFP (November 1, 2013).
Submission Requirements
Indicate the respondent organization name and Request for Proposal (RFP) number on the front of each
proposal envelope or package. All proposals must be received by Alliance on or before 5:00 p.m.
Eastern Standard Time on November 1, 2013. Late proposals will not be accepted. Proposals should be
mailed or hand delivered directly to:
Alliance Behavioral Healthcare 4600 Emperor Boulevard, Suite 200 Durham, NC 27703 Attention: Carlyle Johnson, Ph.D
Alliance will not be held responsible for the failure of any mail or delivery service to deliver a proposal
response prior to the stated proposal due date and time. It is solely the proposer’s responsibility to
ensure that all required and necessary information, documents and attachments are included prior to
submitting a response and to ensure that the response is received at the correct location and time. Late
responses, regardless of delivery means, will not be accepted. Alliance will not accept responses
delivered even one minute after 5:00 pm Eastern Standard Time on November 1, 2013. No fax or
emailed responses will be accepted or considered.
When responding to this RFP be sure to follow all instructions carefully. Submit proposal contents
according to the outline specified and submit documents according to the instructions. Failure to follow
these instructions will be considered a non-responsive proposal and may result in immediate elimination
from further consideration. Bidders are responsible for reviewing the Alliance Behavioral Healthcare
web page for additional information that is posted after the initial release of the RFP. Copies of all
postings will be emailed directly to anyone who registers with Alliance. To register, please send an email
to [email protected] with your name and contact information.
Questions concerning the specifications in this RFP will be received until 5:00 pm, Friday October 11,
2013. Please submit all questions in writing by e-mail to [email protected] A summary of all
questions and answers will be posted by Friday, October 18, 2013 on the Alliance Behavioral Healthcare
website at: http://www.alliancebhc.org/about-alliance/rfps-rfis-qas
IIH Request for Proposal RFP #2013-302
4
Eligible providers who do not intend to respond to the RFP are required to submit Appendix A “Intent
Not to Bid” as soon as possible, and no later than November 1, 2013. The “Intent Not to Bid” form
should be emailed to [email protected] using “Intent Not to Bid” in the subject line. The
form should be signed by an authorized signer of the organization.
A pre-proposal conference for prospective bidders will be held on Monday, October 7, 2013 from
10:00am until noon. This meeting will be held at Alliance Behavioral Healthcare’s corporate office at
4600 Emperor Blvd., Durham NC 27703 in rooms 104 and 105. Directions to this location are available
at: http://www.alliancebhc.org/contact-us.
The purpose of this conference is to discuss the RFP and provide an opportunity to receive and answer
any questions from prospective applicants. Questions asked at the pre-proposal conference will be
included in the summary of questions and answers noted above. It is strongly recommended that
interested parties attend this conference. Please confirm your interest in attending this meeting by
sending an e-mail message to [email protected].
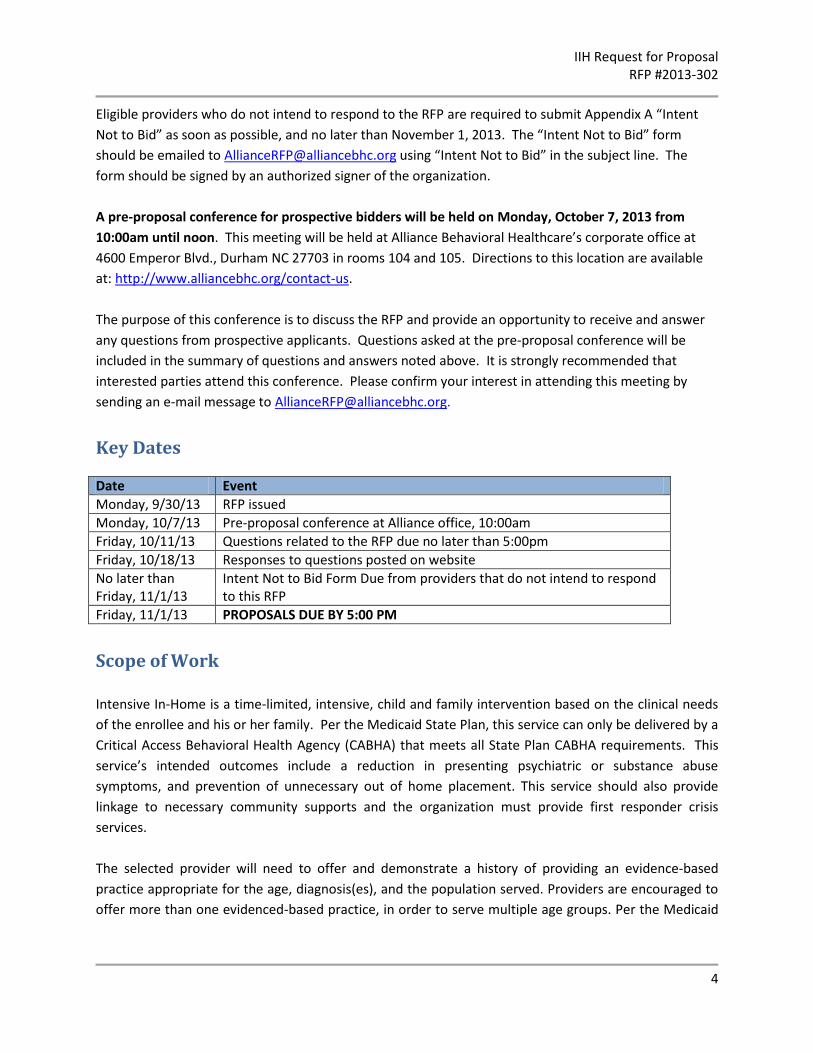
Key Dates
Date Event
Monday, 9/30/13 RFP issued
Monday, 10/7/13 Pre-proposal conference at Alliance office, 10:00am
Friday, 10/11/13 Questions related to the RFP due no later than 5:00pm
Friday, 10/18/13 Responses to questions posted on website
No later than Friday, 11/1/13
Intent Not to Bid Form Due from providers that do not intend to respond to this RFP
Friday, 11/1/13 PROPOSALS DUE BY 5:00 PM
Scope of Work
Intensive In-Home is a time-limited, intensive, child and family intervention based on the clinical needs
of the enrollee and his or her family. Per the Medicaid State Plan, this service can only be delivered by a
Critical Access Behavioral Health Agency (CABHA) that meets all State Plan CABHA requirements. This
service’s intended outcomes include a reduction in presenting psychiatric or substance abuse
symptoms, and prevention of unnecessary out of home placement. This service should also provide
linkage to necessary community supports and the organization must provide first responder crisis
services.
The selected provider will need to offer and demonstrate a history of providing an evidence-based
practice appropriate for the age, diagnosis(es), and the population served. Providers are encouraged to
offer more than one evidenced-based practice, in order to serve multiple age groups. Per the Medicaid
IIH Request for Proposal RFP #2013-302
5
service definition, respondents must demonstrate that the organization and its staff use and are trained
in one of the following evidenced-based models:
Cognitive Behavior Therapy as appropriate for the cognitive status and age of the consumer
Trauma-Focused Therapy ( e.g. Seeking Safety, Trauma-Focused CBT, Real Life Heroes)
Family Therapy (e.g. Brief Strategic Family therapy, Multidimensional Family Therapy, Family
Behavior Therapy, Child Parent Psychotherapy, or Family Centered Treatment).
PCIT, Seven Challenges, or other evidence-based practices endorsed by SAMHSA.
The provider must demonstrate the use of one of the above-listed evidence-based model(s) for at least
the last year. Preference will be shown to those agencies who have been using an evidence-based
model(s) for two or more years. Provider must be able to identify expected outcomes of their model(s)
and be able to show the outcomes that they have achieved through use of the model(s). Provider must
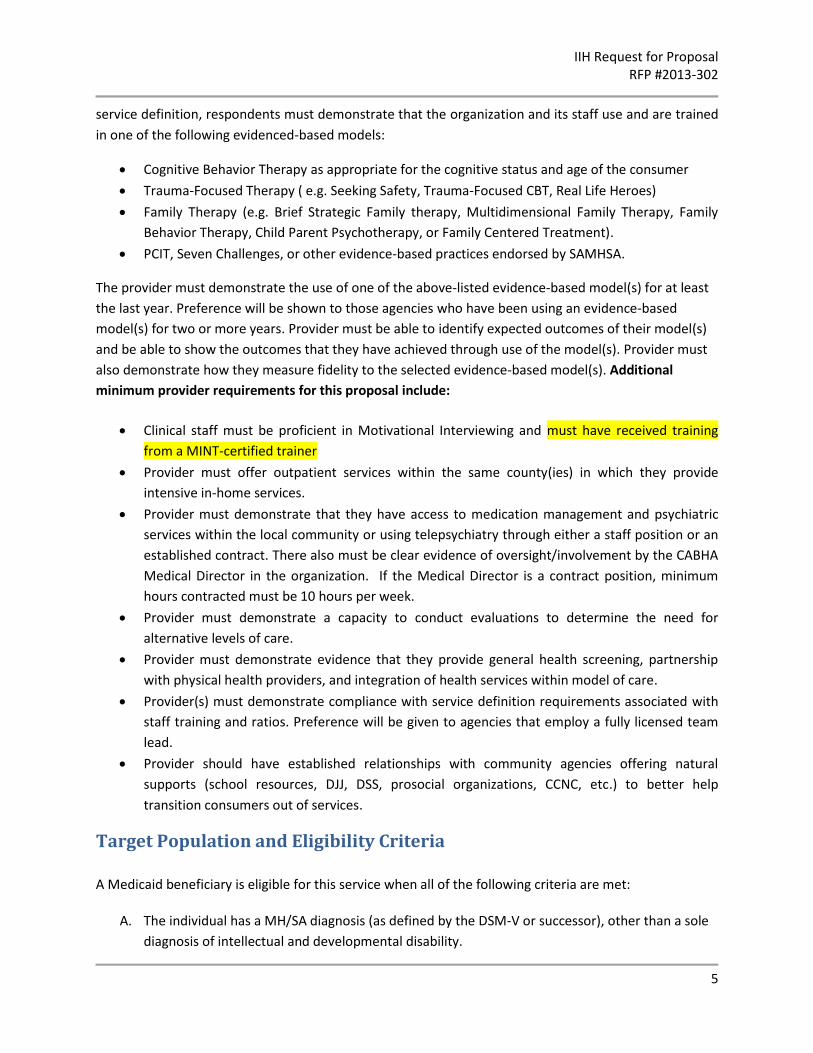
also demonstrate how they measure fidelity to the selected evidence-based model(s). Additional
minimum provider requirements for this proposal include:
Clinical staff must be proficient in Motivational Interviewing and must have received training
from a MINT-certified trainer
Provider must offer outpatient services within the same county(ies) in which they provide
intensive in-home services.
Provider must demonstrate that they have access to medication management and psychiatric
services within the local community or using telepsychiatry through either a staff position or an
established contract. There also must be clear evidence of oversight/involvement by the CABHA
Medical Director in the organization. If the Medical Director is a contract position, minimum
hours contracted must be 10 hours per week.
Provider must demonstrate a capacity to conduct evaluations to determine the need for
alternative levels of care.
Provider must demonstrate evidence that they provide general health screening, partnership
with physical health providers, and integration of health services within model of care.
Provider(s) must demonstrate compliance with service definition requirements associated with
staff training and ratios. Preference will be given to agencies that employ a fully licensed team
lead.
Provider should have established relationships with community agencies offering natural
supports (school resources, DJJ, DSS, prosocial organizations, CCNC, etc.) to better help
transition consumers out of services.
Target Population and Eligibility Criteria
A Medicaid beneficiary is eligible for this service when all of the following criteria are met:
A. The individual has a MH/SA diagnosis (as defined by the DSM-V or successor), other than a sole
diagnosis of intellectual and developmental disability.
IIH Request for Proposal RFP #2013-302
6
B. Based on the current comprehensive clinical assessment, this service was indicated and
outpatient treatment services were considered or previously attempted, but were found to be
inappropriate or not effective.
C. The beneficiary has current or past history of symptoms or behaviors indicating the need for a
crisis intervention as evidenced by suicidal or homicidal ideation, physical aggression toward
others, self-injurious behavior, serious risk-taking behavior (running away, sexual aggression,
sexually reactive, or substance use).
D. The beneficiary’s symptoms and behaviors are unmanageable at home, school, or in other
community settings due to the deterioration of the beneficiary’s mental health or substance
abuse condition, requiring intensive, coordinated clinical interventions.
E. The beneficiary is at imminent risk of out-of-home placement based on the beneficiary’s current
mental health or substance abuse clinical symptomotology, or is currently in an out-of-home
placement and a return home is imminent.
F. There is no evidence to support that alternative interventions would be equally or more
effective, based on North Carolina community practice standards (Best Practice Guidelines of
the American Academy of Child and Adolescent Psychiatry, American Psychiatric Association,
American Society of Addiction Medicine).
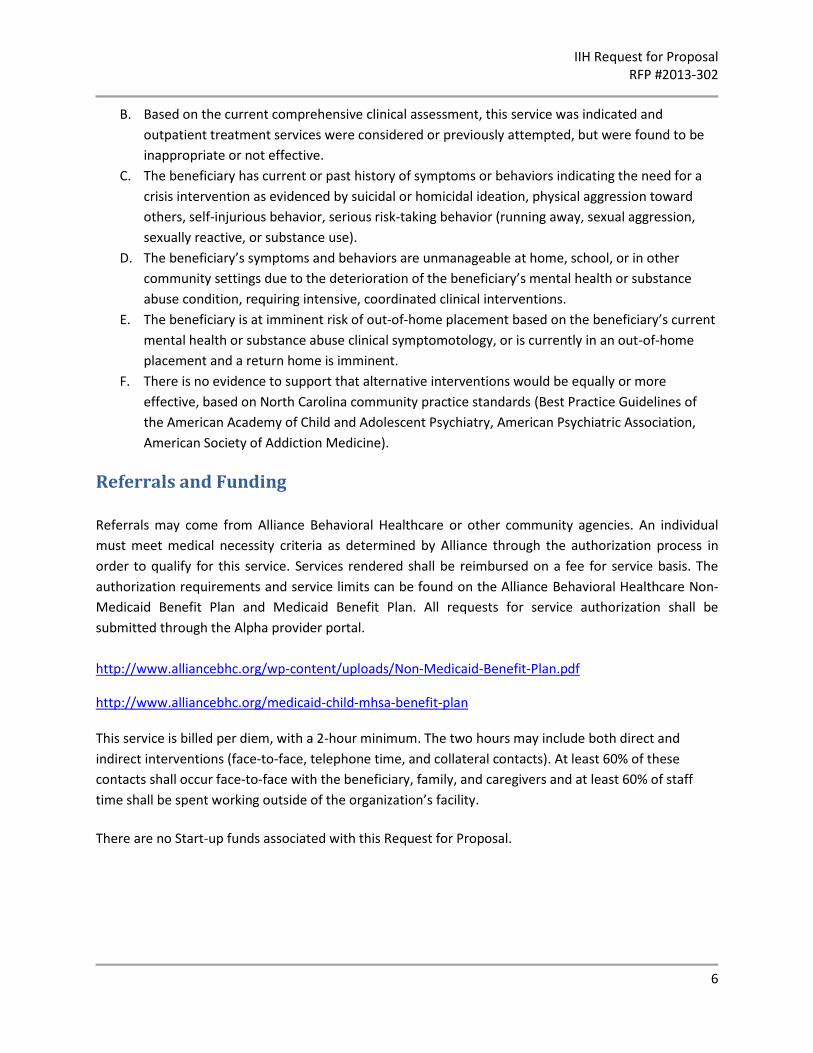
Referrals and Funding
Referrals may come from Alliance Behavioral Healthcare or other community agencies. An individual
must meet medical necessity criteria as determined by Alliance through the authorization process in
order to qualify for this service. Services rendered shall be reimbursed on a fee for service basis. The
authorization requirements and service limits can be found on the Alliance Behavioral Healthcare Non-
Medicaid Benefit Plan and Medicaid Benefit Plan. All requests for service authorization shall be
submitted through the Alpha provider portal.
http://www.alliancebhc.org/wp-content/uploads/Non-Medicaid-Benefit-Plan.pdf
http://www.alliancebhc.org/medicaid-child-mhsa-benefit-plan This service is billed per diem, with a 2-hour minimum. The two hours may include both direct and
indirect interventions (face-to-face, telephone time, and collateral contacts). At least 60% of these
contacts shall occur face-to-face with the beneficiary, family, and caregivers and at least 60% of staff
time shall be spent working outside of the organization’s facility.
There are no Start-up funds associated with this Request for Proposal.
IIH Request for Proposal RFP #2013-302
7
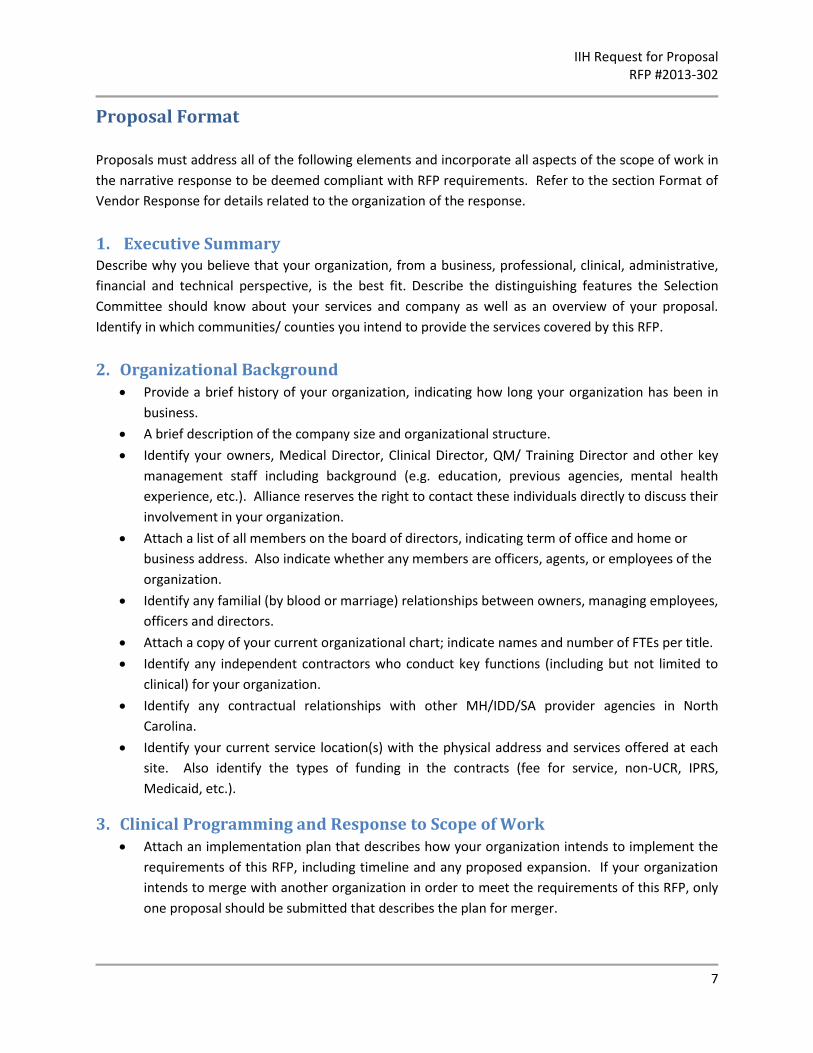
Proposal Format
Proposals must address all of the following elements and incorporate all aspects of the scope of work in
the narrative response to be deemed compliant with RFP requirements. Refer to the section Format of
Vendor Response for details related to the organization of the response.
1. Executive Summary Describe why you believe that your organization, from a business, professional, clinical, administrative,
financial and technical perspective, is the best fit. Describe the distinguishing features the Selection
Committee should know about your services and company as well as an overview of your proposal.
Identify in which communities/ counties you intend to provide the services covered by this RFP.
2. Organizational Background Provide a brief history of your organization, indicating how long your organization has been in
business.
A brief description of the company size and organizational structure.
Identify your owners, Medical Director, Clinical Director, QM/ Training Director and other key
management staff including background (e.g. education, previous agencies, mental health
experience, etc.). Alliance reserves the right to contact these individuals directly to discuss their
involvement in your organization.
Attach a list of all members on the board of directors, indicating term of office and home or
business address. Also indicate whether any members are officers, agents, or employees of the
organization.
Identify any familial (by blood or marriage) relationships between owners, managing employees,
officers and directors.
Attach a copy of your current organizational chart; indicate names and number of FTEs per title.
Identify any independent contractors who conduct key functions (including but not limited to
clinical) for your organization.
Identify any contractual relationships with other MH/IDD/SA provider agencies in North
Carolina.
Identify your current service location(s) with the physical address and services offered at each
site. Also identify the types of funding in the contracts (fee for service, non-UCR, IPRS,
Medicaid, etc.).
3. Clinical Programming and Response to Scope of Work Attach an implementation plan that describes how your organization intends to implement the
requirements of this RFP, including timeline and any proposed expansion. If your organization
intends to merge with another organization in order to meet the requirements of this RFP, only
one proposal should be submitted that describes the plan for merger.
IIH Request for Proposal RFP #2013-302
8
Describe the payor mix of clients currently served (Medicaid, IPRS, County, Medicare, Private
Insurance, Other, etc.)
Summarize demographic and clinical profiles of individuals currently served and numbers
served.
Describe your experience in providing Intensive In-Home.
Describe your service philosophy and models of service delivery for individuals with Mental
Illness and/or Substance Abuse diagnoses.
Describe how you will address each of the required elements listed in the Scope of Work, including but not limited to what evidence-based model(s) your organization utilizes for this service.
Describe how your organization implements its selected evidence based model(s) for this
service.
Provide evidence that staff have been trained in evidence-based model(s) and best practices to
be offered as part of the proposed service array (e.g., training documentation, certification, CV’s
and/or resume) and your plan to provide ongoing training for the staff. For cognitive-behavioral
evidence-based practices, provide evidence that training is targeted to child and adolescent
populations.
Provide information about your current processes for measuring fidelity to your organization’s
selected evidence-based practice model(s).
Identify how your organization renders services that are culturally and gender responsive.
Identify all other LME/MCOs with which your organization holds contracts or Memoranda of
Agreement and the services covered by these agreements.
Provide information about your strategies for recruitment, retention and support of qualified
staffing.
Describe your organization’s ability to recruit, hire, train and supervise staff who may be needed
to ensure accessibililty of the services if awarded this RFP. Preference will be given to
organizations that offer a standard benefit package to their employees.
Describe your staff training and clinical supervision plan.
Provide a job description for each clinical position as it relates to the services in this RFP.
Describe your capacity to ensure accessibility and transfer consumers effectively from providers
who are not selected for this RFP and provide a detailed plan for transition of consumers to your
organization, including anticipated capacity, service locations, staffing and timelines for
increasing capacity.
Describe how your organization monitors and improves access, quality and efficiency of care.
Provide customer satisfaction ratings for the past two years.
Provide information about your organization’s procedures for promoting and ensuring
consumer rights, including but not limited to privacy and security of protected health
information.
Describe your organization’s procedures for responding to complaints from consumers.
Describe your organization’s discharge and transition planning process.
IIH Request for Proposal RFP #2013-302
9
Describe your organization’s Crisis Plan process and response.
Describe how consumer input is included in your program evaluation process.
Describe how you evaluate consumer outcomes and how you determine whether your
consumers are benefitting from your services.
Attach a sample of consumer outcome data for the most recent two years that is relevant to the
services that your organization provides, including but not limited to the outcomes achieved
through use of your identified evidence-based practice model(s).
4. Legal and Compliance Information
Note that for this section “Sanction” is defined as an overpayment, recoupment, payment
withhold, payment suspension, prepayment review, moratorium, probation, Gold Star
performance decrease, referral suspension, referral freeze, referral limitation, revocation,
suspension of admissions, imposition of penalties or damages, contract termination (in whole or
part), exclusion, debarment, suspension, or any other synonymous or similar action.
Identify whether your organization or any owner, director, managing employee, billing
professional, or other employee has been excluded from participation in a federal healthcare
program.
Identify whether the organization or any owner, director, managing employee, or billing
professional have ever been sanctioned in any state or federally-funded healthcare program. If
yes, fully explain the details, including date, the state where the incident occurred, the
organization taking the action, the type of sanction, whether the sanction was appealed or
litigated, and current status, including any corrective actions.
Identify and describe any governmental or regulatory action currently pending against your
organization with any state or federal oversight agency or accrediting body (e.g. DMA,
DMH/DD/SAS, DHSR, NC Department of Labor, IRS, U.S. or N.C. Department of Justice, NC
Department of Revenue, CARF, COA), regardless of the status of any appeal of such action.
Describe the organization’s corrective actions to address these issues.
Identify any legal actions in which your organization is a party, including all federal, state and
administrative actions.
Identify whether any owner, director or managing employee has ever had his or her professional
license or certification revoked, suspended, voluntarily surrendered in lieu of disciplinary action,
subject to a licensing or certification board order or otherwise restricted.
Identify whether the organization has ever been subject to the terms of a settlement
agreement, corporate compliance agreement or corporate integrity agreement in relation to
any State or Federally-funded healthcare program.
Identify whether the organization has any outstanding debt or overpayment in relation to any
State or Federally-funded healthcare program (including but not limited to DMA and other
LME/MCOs).
Identify whether the organization or its owners, directors or managing employees, are now, or
have ever been, under civil or criminal fraud investigation by the North Carolina Office of
Attorney General Medicaid Investigations Division, any other State Medicaid Fraud
IIH Request for Proposal RFP #2013-302
10
Investigations Unit, the U.S. Department of Justice or the U.S. HHS Office of Inspector General,
and the outcome of any such investigation.
Identify whether the organization currently or in the last six months has been under a Plan of
Correction with Alliance, DMH/DD/SAS, DHSR or any other LME/MCO. If yes, include a copy of
the POC and any resolution if applicable.
Identify whether the organization has ever voluntarily withdrawn or had its MOA or
endorsement for any MH/SA service withdrawn or terminated by any LME, area authority or
county program. If so, identify the LME and date and describe the circumstances.
Identify whether the organization has ever reported any Health Insurance Portability and
Accountability Act (HIPAA) violations to the U.S. Office of Civil Rights and describe your
organization’s procedures for ensuring the privacy and security of protected health information.
Identify whether there has been a change in ownership or control of the organization within the
last two years. If yes, provide a detailed description of the change of ownership and indicate
whether any of the new owners are related to any of the former owners, and whether any
former owners transferred their ownership interest to any new owners in anticipation of or
following the assessment of a civil monetary penalty or overpayment.
Indicate whether the organization anticipates any change of ownership or control within the
next twelve months. If yes, describe any pending agreements to acquire other organizations,
merge or sell your organization.
Provide details of any site location or office closures that resulted in the termination of services
within the last two years.
Identify whether your organization has ever been evicted from any office location or otherwise
defaulted on a lease.
Describe your organization’s procedures for the storage and maintenance of medical records
and other required documentation.
Attach a copy of your corporate compliance plan, and describe how your organization ensures
compliance with federal and state laws, rules, regulations, policies, manuals and other guidance
concerning publicly-funded MH/IDD/SA services.
5. Financial Information Submit one electronic copy of your most recent audit report, audited financial statements and
management letter.
If audits or post-payment reviews have been performed on your organization during the past
year, provide information about the name of the auditor, dates of audit, findings and corrective
actions or paybacks required, if any.
Indicate if your organization is current on all tax filings and payments, including all payroll tax
returns and annual tax returns. Any outstanding tax liabilities or tax liens may be grounds for
exclusion from further consideration at the discretion of Alliance.
Indicate if your organization is compliant with all financial reporting requirements from all
funding sources.
Indicate if your organization is considering filing for bankruptcy in the next twelve (12) months.

IIH Request for Proposal RFP #2013-302
11
6. Technological Capability Provider must have the ability to create and test electronic 5010 compliant 837 Professional and
Institutional claims and send via secure FTP to Alliance Behavioral Healthcare, the ability to send and
receive encrypted electronic communications for transfer of PHI, have secure access to the internet to
utilize the Alliance Behavioral Healthcare web based provider portal (AlphaMCS), and have a computer
system utilizing one of the following internet browsers: : IE9 (Windows 7) , IE10 (Windows 7 or 8),
Firefox with Silverlight plugin or Chrome with Microsoft Silverlight plug-in.
7. References Submit contact information for three (3) references, to include, name, title, email address, phone and
description of relationship. The results of the reference check will be used in final selection of vendors
and Alliance reserves the right to ask for additional references. Failure to provide this information will
result in the proposal being considered incomplete.
Format of Vendor Response
The following section identifies the specific criteria that a provider must meet and address in its
proposal. The Selection Committee will review all documentation to determine if evidence to satisfy the
criteria is included. Elaborate proposals in the form of brochures or other presentations beyond that
necessary to present a complete and effective proposal are not desired. All submittals are to be printed
double sided and use Times New Roman, 12 point font with standard 1-inch margins. Written materials
should be submitted in 3-ring binders with clearly labeled provider information on the front. Sections
should be in separate, labeled tabs.
Content of the Proposal
The proposal must be assembled in the following order:
1. Attestation Letter to include the point of contact and signed by an owner or authorized official
certifying the truthfulness, completeness and accuracy of the proposal and the intent of the
organization to provide the services as delineated in the proposal.
2. Table of Contents.
3. Executive Summary.
4. Organizational Background.
5. Clinical Programming and Response to Scope of Work.
6. Legal and Compliance Information.
7. Financial Information.
8. Technological Capability.
9. References.
10. Attachments
1. Additional documentation that supports the proposal response and that the bidder
desires the Selection Committee to consider.
IIH Request for Proposal RFP #2013-302
12
Proposals should be numbered consecutively beginning with the Statement of Intent. Provide one
original and one (1) copy of the proposal in separate binders plus one electronic version of the response
on a CD. Note that paper copies of your organization’s most recent audit report, audited financial
statements and management letter are not required and should only be submitted on the CD. The CD
should include Adobe pdf format versions of all documents, readable by MS Office computers, and file
names and content must comply with the directions listed below:
Content of each scanned document should correspond to the sections noted above. For
example, the CD should include separate documents for each numbered section noted above,
and separate scans for each reference and attachment.
Files should be labeled using the format YOURAGENCYNAME_SECTION#. For example, the
scanned document for the Financial section would be “YourAgencyName_7.”
Review and Evaluation of Proposals
Alliance Behavioral Healthcare will review all proposals submitted by the deadline specified in the RFP
for format and completeness. If the applicant meets the minimum requirements of the RFP (including
format), Alliance Behavioral Healthcare will continue to evaluate the proposal. At its sole discretion,
Alliance Behavioral Healthcare may request clarification of information throughout the proposal
evaluation process. Prospective bidders should be prepared for an oral presentation and/or interview
by the Selection Committee. The Selection Committee will include medical and/or clinical staff, Alliance
staff across departments and counties, CFAC or consumer representative(s), and members of the
Alliance Board and community stakeholders from all four counties, depending on availability. The
award of contract(s) is subject to approval by the Alliance Behavioral Healthcare Board of Directors.
Evaluation Criteria The Selection Committee will first evaluate the bidder’s compliance with minimum RFP requirements.
Respondents who do not meet minimum RFP requirements (including formatting) will be eliminated
from further consideration. The Selection Committee will next evaluate and score the written proposal,
including adherence to evidence-based practice model(s), and business, professional, clinical,
administrative, financial and technical strengths, capabilities, and experience including corporate
background, past and current projects, financial soundness, and performance history. Respondents who
receive a score of at least 70 out of 100 on the written proposal and meet a minimum score for each
category will be invited to interview. The Selection Committee will use a group rating tool to score
interview performance. A zero finding or low score in any single category for the written proposal and
interview may eliminate the respondent from further consideration.
IIH Request for Proposal RFP #2013-302
13
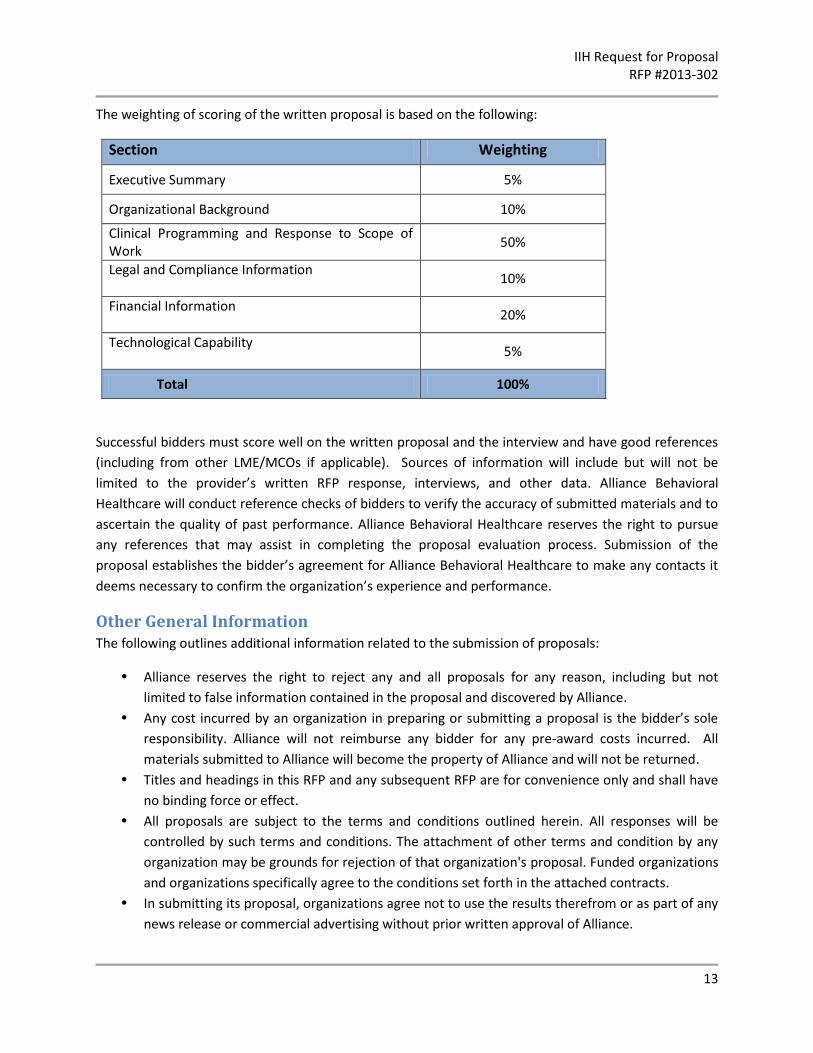
The weighting of scoring of the written proposal is based on the following:
Section Weighting
Executive Summary 5%
Organizational Background 10%
Clinical Programming and Response to Scope of Work
50%
Legal and Compliance Information
10%
Financial Information
20%
Technological Capability
5%
Total 100%
Successful bidders must score well on the written proposal and the interview and have good references
(including from other LME/MCOs if applicable). Sources of information will include but will not be
limited to the provider’s written RFP response, interviews, and other data. Alliance Behavioral
Healthcare will conduct reference checks of bidders to verify the accuracy of submitted materials and to
ascertain the quality of past performance. Alliance Behavioral Healthcare reserves the right to pursue
any references that may assist in completing the proposal evaluation process. Submission of the
proposal establishes the bidder’s agreement for Alliance Behavioral Healthcare to make any contacts it
deems necessary to confirm the organization’s experience and performance.
Other General Information The following outlines additional information related to the submission of proposals:
• Alliance reserves the right to reject any and all proposals for any reason, including but not
limited to false information contained in the proposal and discovered by Alliance.
• Any cost incurred by an organization in preparing or submitting a proposal is the bidder’s sole
responsibility. Alliance will not reimburse any bidder for any pre-award costs incurred. All
materials submitted to Alliance will become the property of Alliance and will not be returned.
• Titles and headings in this RFP and any subsequent RFP are for convenience only and shall have
no binding force or effect.
• All proposals are subject to the terms and conditions outlined herein. All responses will be
controlled by such terms and conditions. The attachment of other terms and condition by any
organization may be grounds for rejection of that organization's proposal. Funded organizations
and organizations specifically agree to the conditions set forth in the attached contracts.
• In submitting its proposal, organizations agree not to use the results therefrom or as part of any
news release or commercial advertising without prior written approval of Alliance.
IIH Request for Proposal RFP #2013-302
14
• All responses, inquiries, or correspondence relating to or in reference to the RFP, and all other
reports, charts, displays, schedules, exhibits, and other documentation submitted by the
organization or organization will become the property of Alliance when received.
• The signer of any proposal submitted in response to this RFP certifies that this proposal has not
been arrived at collusively or otherwise in violation of either Federal or North Carolina antitrust
laws.
• Organizations may propose to subcontract portions of work provided that their proposals clearly
indicate the scope of the work to be subcontracted, and to whom. All information required
about the prime grantee is also required for each proposed subcontractor.
• Trade secrets or similar proprietary data which the organization or organization does not wish
disclosed to other than personnel involved in the evaluation will be kept confidential to the
extent permitted by state law and rule if identified as follows: Each page shall be identified in
boldface at the top and bottom as "CONFIDENTIAL." Any section of the proposal that is to
remain confidential shall also be so marked in boldface on the title page of that section.
• Organizations chosen by the Selection Committee and approved by the Alliance Board of
Directors will be required to execute a standard contract that includes a Scope of Work outlining
the requirements of this RFP as well as federal certification(s) regarding Debarment, Suspension,
Ineligibility and Voluntary Exclusion - Lower Tier Covered Transactions, Drug Free Workplace
Requirements, Lobbying and Environmental Tobacco Smoke.
NOTE: In the event that sufficient numbers of respondents do not meet the requirements of this RFP,
Alliance reserves the right to utilize other procurement methods to ensure access and capacity.
IIH Request for Proposal RFP #2013-302
15
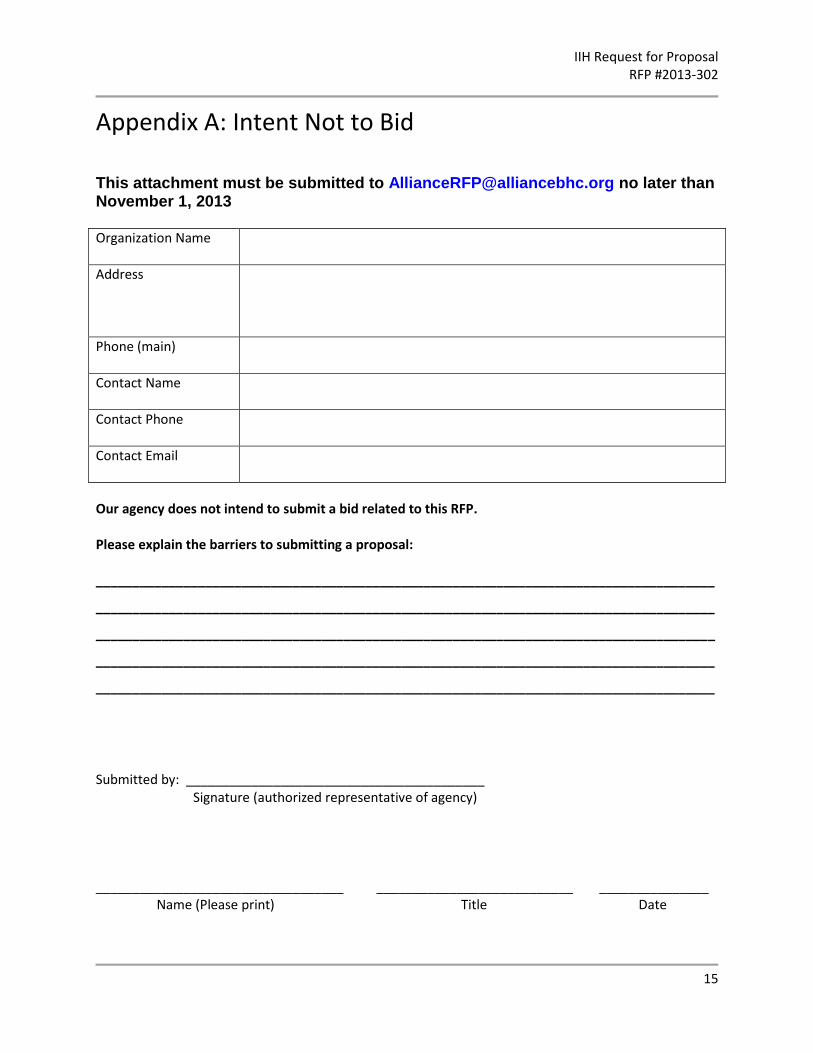
Appendix A: Intent Not to Bid
This attachment must be submitted to [email protected] no later than November 1, 2013
Organization Name
Address
Phone (main)
Contact Name
Contact Phone
Contact Email
Our agency does not intend to submit a bid related to this RFP. Please explain the barriers to submitting a proposal: _____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Submitted by: _________________________________________ Signature (authorized representative of agency)
__________________________________ ___________________________ _______________ Name (Please print) Title Date