Embed Size (px)
Citation preview
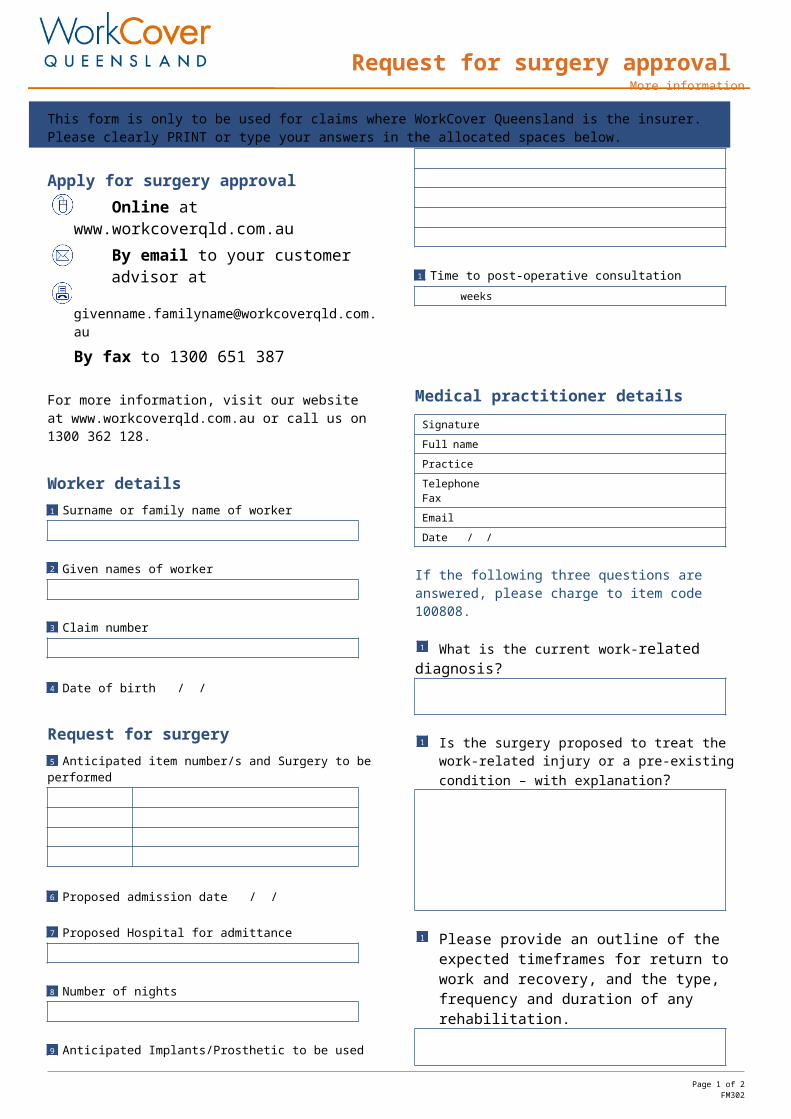
Request for surgery approval More information
This form is only to be used for claims where WorkCover Queensland is the insurer. Please clearly PRINT or type your answers in the allocated spaces below.
Apply for surgery approvalOnline at www.workcoverqld.com.auBy email to your customer advisor at
By fax to 1300 651 387
For more information, visit our website at www.workcoverqld.com.au or call us on 1300 362 128.
Worker detailsSurname or family name of worker
Given names of worker
Claim number
Date of birth / /
Request for surgeryAnticipated item number/s and Surgery to be performed
Proposed admission date / /
Proposed Hospital for admittance
Number of nights
Anticipated Implants/Prosthetic to be used
Time to post-operative consultation weeks
Medical practitioner detailsSignature
Full name Practice Telephone Fax
Date / /
If the following three questions are answered, please charge to item code 100808.
What is the current work-related diagnosis?
Is the surgery proposed to treat the work-related injury or a pre-existing condition – with explanation?
Please provide an outline of the expected timeframes for return to work and recovery, and the type, frequency and duration of any rehabilitation.
Please noteSurgical fees must be based on the Medical Items—Schedule of Fees.
No fee is payable for submitting this request, unless questions 11 – 13 are answered in full.
For more information about how we approve surgery requests, visit our website at www.workcoverqld.com.au.
Full name
Date / / I agree
Page 1 of 1FM302
1
2
3
5
6
8
10
4
9
7
11
12
13









![Salmon Creek Plastic Surgery DOR 16-08 · 10th Avenue in Vancouver [98685]. The procedures proposed include those typically associated with cosmetic and reconstructive plastic surgery](https://img.pdfslide.net/doc/110x75/5f66b94a16ef4f7c05268589/salmon-creek-plastic-surgery-dor-16-08-10th-avenue-in-vancouver-98685-the-procedures.jpg)



















