Embed Size (px)
Citation preview

Research ArticleAssessment of Airway Bronchodilation by Spirometry Comparedto Airway Obstruction in Young Children with Asthma
Daphna Vilozni,1,2 Fahed Hakim,1,3 Galit Livnat,1 Miryam Ofek,2
Ronen Bar-Yoseph,1 and Lea Bentur1,3
1Pediatric Pulmonary Institute, Ruth Rappaport Children’s Hospital, Rambam Health Care Campus, 31096 Haifa, Israel2The Edmond and Lily Safra Children’s Hospital, Sheba Medical Center, Sackler Medical School, 52621 Tel Aviv, Israel3The Bruce Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, 31096 Haifa, Israel
Correspondence should be addressed to Daphna Vilozni; avi [email protected]
Received 29 July 2015; Revised 19 April 2016; Accepted 8 May 2016
Academic Editor: Christophe Leroyer
Copyright © 2016 Daphna Vilozni et al.This is an open access article distributed under the Creative CommonsAttribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A reversibility test by an increase of greater than 12% in FEV1 can support a diagnosis of asthma and alter a patient’s treatmentplan but may not be applicable to the young ages. We retrospectively gathered spirometric data from 85/271 asthmatic childrenhaving mild obstruction (FEV1 > 80% predicted), age 2.6–6.9 years. Spirometry was performed before and 20min after inhalationof 200mcg Albuterol. We defined a deviation below −1.64 𝑧 scores from control as obstruction and an increased above 1.64 scoresfrom control as a positive response to bronchodilators. Sensitivity of the index was considered significant if it captured >68% ofthe participants. The sensitivity of detecting airway obstruction in these children by FEV1 was 15.3% and 62.4% by FEF25–75. Apositive response toAlbuterol was an increase of 9.2% for FEV1 (12% for adults) and 18.5% for FEF25–75.The sensitivity for detectinga response to Albuterol in mild asthma was 64.7% by FEV1 and 91.8% by FEF25–75. Young children having normal spirometry candemonstrate airway reversibility.The response of spirometry parameters to bronchodilatorsmay bemore sensitive than obstructiondetection and may help to support the diagnosis of asthma and adjust treatment plan.
1. Introduction
Asthma is a chronic inflammatory disorder of the airwaysassociated with a variable, widespread, airflow obstructionthat is often reversible, either spontaneously or with treat-ment [1]. A decrease of >20% predicted in FEV1 is consideredmild airway obstruction, yet many people with mild asthmamay present normal FEV1 values [2]. “Reversibility” is gen-erally applied to rapid improvements of 12% in forced expi-ratory volume [2, 3] at the first second of expiration (FEV1)measured within minutes after inhalation of a rapid-actingbronchodilator. A reversibility test can support a diagnosis ofasthma and can alter a patient’s treatment plan and, therefore,it is of clinical importance.
Wheezing, cough, and/or breathlessness are major causesof morbidity in young children regardless of current treat-ment [4, 5]. Despite recent advances in spirometric measure-ment techniques, spirometry is rarely used in clinical practicefor defining obstruction/reversibility of airways in young
children [6, 7].When spirometry is used, the interpretation ofobstruction and a positive response have been based on thatobserved in adults.Theuse of FEV1may be questionable sincenot all young children will exhale more than one second [6–9]. When exhalation continues beyond one second, the FEV1value is close to that of the forced expiratory vital capacity(FVC) [6]. FEV0.5 and FEV0.75 have been proposed as surro-gates for FEV1 [8, 9]. We reason that there may be differencesbetween the ability to diagnose airway obstruction and dilata-tion. The aim of this study was to define airway reversibilitycompared to airway obstruction detection in young children.
2. Subjects and Methods
2.1. Study Design: Retrospective. The study design includedclinical and spirometry data from children referred to MeyerChildren’s Hospital during 2011–2014 (data included childrenfrom our previous study [9]).
Hindawi Publishing CorporationCanadian Respiratory JournalVolume 2016, Article ID 5394876, 6 pageshttp://dx.doi.org/10.1155/2016/5394876

2 Canadian Respiratory Journal
2.1.1. Inclusion Criteria. Inclusion criteria consisted of datafrom children who performed spirometry before and 20minafter Albuterol inhalation.
Asthmatic Children’s Data. Data included children presentingsymptoms highly suggestive of asthma according to GINAguidelines [1] and/or frequent episodes of wheezing, activity-induced cough/wheeze, nocturnal cough without viral infec-tions, and absence of seasonal variation. All children hadpositive challenge tests (either methacholine or exercise).
Healthy Children’s Data. Healthy children’s data included datafrom children having no recurrent respiratory symptoms ortreatment suggestive of asthma, no family history of asthma,and no hospitalization due to respiratory syncytial virusbronchiolitis, with normal baseline spirometry and nega-tive methacholine, who underwent bronchodilator response.Most were evaluated and followed up for habitual cough.
2.1.2. Exclusion Criteria. For asthmatic children, theyincluded chronic respiratory illness other than asthma.
The local ethics committee of Rambam Health CareCampus (Institutional Review Board 0304-11-RambamMC)approved the study.
2.2. Methods. Routinely, we instructed children’s parents towithdraw Albuterol at least 12 hours before spirometry tests[1].
Spirometry Tests. Children performed spirometry in thestanding position without a nose clip with a commercialspirometer (KoKo-PDS Dosimeter, nSpire Healthcare Inc.,Longmont CO, USA) that includes incentives. Tests wereperformed according to the official ATS/ERS statement onpulmonary function testing in preschool children [6]. Theseguidelines include the recommended reproducibility andacceptability to rule out abnormal or unacceptable curves.After satisfactory baseline measurements, children receiveda bronchodilator (2 puffs of 100mcg Albuterol) administeredvia a volumetric spacer. Children repeated the spirometrytests 15–20min after bronchodilator inhalation.
2.2.1. Data Analysis. We visually inspected each spirometrycurve for technical errors and only technically correctedcurves were included for analysis. The single best baselinecurve values and the best postbronchodilator (BDR) curvevalues were further analyzed. For predicted values of FVC,FEV1, and FEF25–75, we used the spirometry reference equa-tions from Global Lung Function Initiative [10]. For otherindices, we used the predicted values of our former study [11].When FEV1/FVC > 0.98 was present and the curves wereacceptable, we used FEV0.5 as representative of FEV1.
Obstruction Categories. We further subgrouped the asthmaticchildren according to FEV1% predicted values as follows:Mild obstruction included children showing FEV1 ≥ 80%predicted, moderate obstruction included children showingFEV1 of 60–79% predicted, and severe obstruction included
children showing FEV1 < 59% predicted. Sensitivity cap-turing >68% of the participants (values within 1 standarddeviation of the mean) was considered clinically significant.We assessed the sensitivity of spirometric indices to detectairway obstruction or dilatation within the three subgroupsof asthma severity (see below) and in relation to the healthypopulation.
Response to BD. We defined a meaningful response tobronchodilators by the various spirometry parameters by anelevation of 1.64 𝑧 scores from the response of our healthycontrol providing normal distribution.
In capturing either bronchoconstriction or dilatation, asensitivity >68% (values within 1 standard deviation of themean) was considered significant.
Statistics. Spirometry data was tested for normal distribution.We used paired 𝑡-tests to compare the differences betweenbaseline lung function and predicted values or differencesbetween prebronchodilator inhalation and postinhalationchanges of each subject. Significant differences between thesubgroups (healthy, mild, moderate, and severe) were testedby ANOVA. Diagnostic test evaluation was used for sensi-tivity for each parameter. We used Pearson correlation teststo determine associations between baseline and response tobronchodilators.We report the findings as mean (±SD) whennormally distributed or as median and 95% confidence limitif nonnormally distributed. Statistical significance was set at𝑃 < 0.05.
3. Results
We inspected spirometry data from 360 (female, 𝑛 = 157)children. The age composition was as follows: <4.0 years 𝑛 =90 (17 <3.0 y), between 4 and 5 years 𝑛 = 109, between 5 and6 years 𝑛 = 102, and between 6 and 7 years 𝑛 = 59. The meanage was 4.8 ± 1.1 years; the mean height for all children was108 ± 9 cm and weight 19 ± 4 kg.
Table 1 presents the anthropometric data (top table) andbaseline spirometry data (bottom table) for healthy and asth-matic children according to subgroups. The table shows thatthere was no significant difference in the anthropometric databetween the groups.
Healthy children’s spirometry values (bottom table) didnot differ from predicted values for that age group. Healthychildren’s FEV1/FVC ratio decreased from 0.96 ± 0.01 at ageof 3.0–3.9 years to 0.90±0.01 at age of 6.0–6.9 years, similar toreference values. The differences between the two measure-ments were less than 5% for FVC, FEV0.5, FEV1, and peakflow and less than 9% for FEF50 and FEF25–75; otherwise thecurves were not accepted for analysis. FEV1 was unachievablein 46 of the 360 children where FEV0.5 was taken as asubstitute.
We found that 85 children had normal to mild obstruc-tion severity, 142 had moderate obstruction, and 44 of theasthmatic group had severe obstruction. FVC decreased insimilar magnitude as FEV1 across the different severity’sgroups, while FEF25–75 decreased significantly more thanboth FEV1 and FVC (𝑃 < 0.01) with increasing obstruction

Canadian Respiratory Journal 3
Table 1: Anthropometric and baseline lung function (% GLI).
Healthy (𝑛 = 89) Asthma (𝑛 = 271)Mild (𝑛 = 85) Moderate (𝑛 = 142) Severe (𝑛 = 44)
M/F 54/36 50/35 74/68 24/20Age (y) 5.1 ± 1.1 4.8 ± 0.9 4.7 ± 1.1 4.7 ± 1.1Ht (cm) 110 ± 8 108 ± 8 109 ± 7 108 ± 9Wt (kg) 19.5 ± 3.5 19 ± 4 18 ± 4 19 ± 5
Baseline spirometry (% predicted)FVC 96 (94–98) 87 (86–91) 72 (72–74) 55 (52–58)FEV1 102 (100–104) 88 (97–91) 71 (70–72) 55 (51–54)FEV0.5 98 (98–103) 87 (87–91) 68 (68–71) 57 (53–56)PEF 92 (90–94) 80 (77–83) 65 (63–68) 48 (49–55)FEF25–75 91 (90–98) 77 (73–81) 65 (63–70) 48 (43–52)FEF50 96 (94–101) 71 (67–76) 56 (54–60) 39 (38–44)Values are presented as median and 95% confidence limit.
Table 2: Sensitivity (% population) of spirometric indices for detecting airway obstruction or dilatation.
Obstruction Response to BDMild (𝑛 = 85) Moderate (𝑛 = 142) Severe (𝑛 = 44) Mild Moderate Severe
FVC 14.1 40.1 75.0 42.3 64.1 77.3FEV1 15.3 50.0 90.9 64.7 78.2 86.4FEV0.5 21.1 56.1 93.1 63.1 70.6 86.4PEF 18.8 60.5 94.4 89.5 95.1 95.5FEF25–75 62.4 76.1 97.7 91.8 94.4 93.2FEF50 67.1 80.0 95.5 87.5 81.2 87.5
severity. FEV1/FVC ratio declined with severity of obstruc-tion from 0.92 ± 0.05 in mild obstruction to 0.87 ± 0.07 inmoderate obstruction to 0.83± 0.06 in the severe obstructiongroup (𝑃 = 0.004).
Table 2 presents the sensitivity of the various spirometryindices to detect either airway obstruction or bronchodilata-tion according to the subgroups. The sensitivity of detectingairway obstruction in relation to our healthy for the entireasthmatic group was 37.62% for FVC, 45.8 for FEV1, and75.7% for FEF25–75. The table shows that FEV1 is insensitiveto mild and moderate obstruction, while FEF25–75 maycapture 62.4% even in mild obstruction and become moresensitive at moderate and severe obstruction.
Response to Bronchodilators. The response (% baseline) ofhealthy controls to bronchodilators was normally distributedand was as follows (mean ± SD): FVC = 0.44 ± 4.33%;FEV1 = 0.53 ± 4.35; FEV0.5 = 0.55 ± 4.3; PEF = 1.09 ± 5.82;FEF25–75 = 3.55 ± 4.71; and FEF50 = 2.60 ± 7.4. A positiveresponse to Albuterol (>1.64 𝑧-score from control response)was equal to an increase of 9.7% for FVC, 9.2% for FEV1, and18.5% for FEF25–75. The 9.2% for FEV1 was lower than therecommended 12% for adults.
Table 2 presents the sensitivity of the various spirometryindices to detect bronchodilatation.The sensitivity for detect-ing bronchodilation was higher than that of the detection ofbronchoconstriction.
100
80
60
40
20
0Sens
itivi
ty in
child
ren
with
mild
FVC FEV1 FEV0.5 PEF FEF25–75 FEF50Spirometry index
ObstructionDilatation
obstr
uctio
n (%
gro
up)
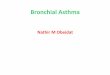
Figure 1: Detection of obstruction and response to BDR by thevarious spirometry indices, in children with mild obstruction.
Figure 1 presents the detection of obstruction andresponse to BDR by the various spirometry indices in chil-dren with mild obstruction. The figure shows that the sen-sitivity of mid-flow to BDR is the highest.
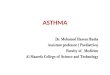
Figure 2 shows the correlation between FEF25–75 values(% predicted) and the response to BDR (% baseline) inchildren with mild asthma. A significant change in FEF25–75 values in our study was >18.5% from baseline values. It

4 Canadian Respiratory Journal
92.5
55.5
18.5
0.0
40 60 80 100 120 140
Baseline FEF25–75 (% predicted)
FEF2
5–75
resp
onse
to B
DR
(% ch
ange
from
bas
eline
) r2= −0.5513; P = 0.0001
Figure 2: Correlation between airway obstruction severitiesassessed by FEF25–75 and the response of this index to BDR.
can be seen that the lower the FEF25–75% predicted values,the greater the response to BDR despite the normal FEV1(𝑟2 = −0.5513, 𝑃 = 0.0001).
4. Discussion
In this study, we focused on the common spirometry indicesto determine the degree of the response to BDR comparedto the detection of airway obstruction in young childrenwith asthma of various severities. Our main findings showthat rate of detection of response to BDR was higher for allspirometry indices than the rate of detection of bronchialobstruction. The response of FEV0.5, FEF25–75, or FEF50to bronchodilators captured >68% of the participants, evenin children with mild asthma. Conversely, the sensitivity ofdetection of airway obstruction in mild asthmatics by com-mon parameters (FVC, FEV1, FEV0.5, and PEF) was weakand only mid-flows parameters (FEF25–75/FEF50) captured>68% of this group. Indeed, the response of mid-flow indicescorrelated with severity of obstruction. These findings mayimply that mid-flows are more sensitive in the detection ofobstruction and bronchodilation in young asthmatic chil-dren.
The definition of airway obstruction and a response toBDR in any studied group depends on defining the responsein a healthy group of similar age and gender. Our controlgroup consisted of well-defined, healthy subjects in whichasthmawas excluded andnot a randompopulation.Given thehigh rate of asthma in the young population, preselecting thecontrol group was more likely to avoid inadvertent inclusionof asthmatic subjects. Our study represents the largest controlgroup evaluated for bronchodilator response in this age groupby spirometry. The response of the control group was similarto that published in the literature for various age ranges.Goldstein et al. [12] used the raised flow/volume technique tomeasure infants aged 0.1–2.9 years and found a response (%frombaseline) of 2.2 in FEV0.5 and 3.7 in FEF25–75.Galant etal. tested a population aged 4–17 years and found a change of2.2% in FEV1 [13]. Dundas et al. [14] assessed healthy childrenaged 5–10 years in theDutchCNSLD study group and found aresponse of 3.8% in FEV1; they also tested an adult population(aged 20–80 years) and found amean change of 1.0% in FEV1.
The large number included in this study enabled segrega-tion into a spectrum of disease activity. We related the defi-nition of airway obstruction severity to our established refer-ence values [11]. We found that FEV0.5 and FEV1 were simi-larly low sensitivity indices for detection of mild and moder-ate airway obstruction. Mid-flows captured more than two-thirds of children with mild obstruction.The use of mid-flowparameters was formerly suggested despite their large stan-dard deviations. Rao et al. [15] studied 437 asthmatic childrenwith normal % predicted FEV1 and found that % predictedFEF25–75 positively correlated with methacholine challengetest results. FEF25–75 also correlated with morning andevening peak expiratory flow [16, 17].
Our study used spirometry to demonstrate airwayreversibility in young children. The ability to measure aresponse to BDR was previously shown by nonspirometrictechniques, including force oscillation, specific resistancemeasured in the plethysmograph [18, 19], and the Rinttechnique [20]. It is not surprising, therefore, that spirometrycould also identify response to BDR in our tested children.In our children, the positive response to Albuterol shownby FEV1 was an elevation of 9.2% and this magnitude ofresponse is lower than recommended for the adult definitionof reversibility. Our study suggests that spirometry indices aremore sensitive for detecting BDR response than detecting air-way obstruction in mild asthma. In response to BDR, FEV0.5had a sensitivity of similar magnitude to mid-flows. Interest-ingly, we also found that the change in PEF was similar tothat of FEV0.5 in response to BDR. However, FEV0.5 is notmounted onmost commercial spirometers and, therefore, wecannot recommend its use.
The sensitivity of an elevation of 18.2% in FEF25–75 wasabove 91.8%, even in children with mild asthma severity.This positive response correlated with the airway obstructionseverity of the entire group.Our findings for higher sensitivityof mid-flow indices are in agreement with previous publica-tions in children [13, 21]. It must be stressed that findings ofhigh sensitivity of mid-flows were unrelated to the changesin FVC, which may result in either elevation or declinein functional residual capacity. We wish to emphasize thatspirometry in the preschool age differs from that of the olderpopulation, not only in the approach to the child, criteriafor acceptability, and repeatability, but also in the shape ofthe flow-volume of the basic curve. We should also take intoconsideration the sensitivity of each of the parameters indetecting airway obstruction and bronchodilation.
Study Limitations. Ideally, the study would have had aprospective, double-blind design, with at least one repetitionon separate days. One could claim that the preschool age is2–5 years, while we included data from children of up to6.9 years of age. However, none of the children in this studyhad entered first grade in school; therefore, they representedpreschool ages in our country.
5. Conclusion
Our study shows that the sensitivity of spirometric parame-ters to detect BDR response is significantly higher than the

Canadian Respiratory Journal 5
sensitivity to detect obstruction. Lower than recommendedmagnitude of improvement in FEV1 may be applied in thisage group. Peak flow and mid-flows may be considered assensitive markers for bronchoconstriction and bronchodila-tion in young children. Bronchodilator response should beassessed in this age group, even when baseline spirometry iswithin the normal range.
Abbreviations
BDR: BronchodilatorsFEF25–75: Forced expiratory flow between 25% and
75% of vital capacityFEF50: Forced expiratory flow at 50% vital
capacityFEV1: Forced expiratory volume in 1st secondFEV0.5: Forced expiratory volume in 0.5 secondsFVC: Forced vital capacityPEF: Peak expiratory flow.
Competing Interests
None of the authors have any financial competing interestsor received reimbursements, fees, funding, or salary from anorganization thatmay in anyway gain or lose financially fromthe publication of this paper, either now or in the future in thelast five years. None of the authors holds any stocks or sharesin an organization thatmay in anyway gain or lose financiallyfrom the publication of this paper, now or in the future. Noneof these authors is currently applying for any patents relatingto the content of the paper and received reimbursements,fees, funding, or salary from an organization that holdsor has applied for patents relating to the content of thepaper. None of these authors has any nonfinancial competinginterests (political, personal, religious, ideological, academic,intellectual, commercial, or any other) to declare in relationto this paper.
Authors’ Contributions
Dr. Daphna Vilozni and Professor Lea Bentur made substan-tial contributions to the conception and design, acquisitionof data, analysis and interpretation of data, drafting the paperor revising it critically for important intellectual content,and the final approval of the version to be published. Dr.Fahed Hakim, Dr. Miryam Ofek, Dr. Ronen Bar-Yoseph, andDr. Galit Livnat all made substantial contributions to theacquisition of data, analysis and interpretation of data, andthe final approval of the version to be published.
Acknowledgments
This study was supported by the J. Baum Foundation of theIsrael Lung Association, Israel.
References
[1] E. D. Bateman, S. S. Hurd, P. J. Barnes et al., Global Strategyfor Asthma Management and Prevention, Global Initiative forAsthma (GINA), 2012.
[2] National Asthma Education and Prevention Program, “ExpertPanel Report 3 (EPR-3): guidelines for the diagnosis andmanagement of asthma-summary report 2007,” The Journal ofAllergy And Clinical Immunology, vol. 120, no. 5, pp. S94–S138,2007.
[3] R. Pellegrino, G. Viegi, V. Brusasco et al., “Interpretative strate-gies for lung function tests,” European Respiratory Journal, vol.26, no. 5, pp. 948–968, 2005.
[4] P. L. P. Brand, E. Baraldi, H. Bisgaard et al., “Definition, assess-ment and treatment of wheezing disorders in preschool chil-dren: an evidence-based approach,” European Respiratory Jour-nal, vol. 32, no. 4, pp. 1096–1110, 2008.
[5] W. J. Morgan, D. A. Stern, D. L. Sherrill et al., “Outcomeof asthma and wheezing in the first 6 years of life follow-up through adolescence,” American Journal of Respiratory andCritical Care Medicine, vol. 172, no. 10, pp. 1253–1258, 2005.
[6] N. Beydon, S. D. Davis, E. Lombardi et al., “An official AmericanThoracic Society/European Respiratory Society statement: pul-monary function testing in preschool children,” American Jour-nal of Respiratory and Critical CareMedicine, vol. 175, no. 12, pp.1304–1345, 2007.
[7] M. Rosenfeld, J. Allen, B.H.G.M.Arets et al., “An official Amer-ican Thoracic Society workshop report: optimal lung functiontests for monitoring cystic fibrosis, bronchopulmonary dyspla-sia, and recurrent wheezing in children less than 6 years of age.American Thoracic Society Assembly on Pediatrics WorkingGroup on Infant and Preschool Lung Function Testing,” Annalsof the American Thoracic Society, vol. 10, no. 2, pp. S1–S11,2013.
[8] L. M. Borrego, J. Stocks, I. Almeida et al., “Bronchodilatorresponsiveness using spirometry in healthy and asthmaticpreschool children,” Archives of Disease in Childhood, vol. 98,no. 2, pp. 112–117, 2013.
[9] D. Vilozni, F. Hakim, G. Livnat, and L. Bentur, “Forced expira-tory decay in asthmatic preschool children—is it adult type?”Respiratory Medicine, vol. 107, no. 7, pp. 975–980, 2013.
[10] P. H. Quanjer, S. Stanojevic, T. J. Cole et al., “Multi-ethnicreference values for spirometry for the 3-95-yr age range: theglobal lung function 2012 equations,” European RespiratoryJournal, vol. 40, no. 6, pp. 1324–1343, 2012.
[11] D. Vilozni, A. Barak, O. Efrati et al., “The role of computergames in measuring spirometry in healthy and “asthmatic”preschool children,” Chest, vol. 128, no. 3, pp. 1146–1155, 2005.
[12] A. B. Goldstein, R. G. Castile, S. D. Davis et al., “Bronchodilatorresponsiveness in normal infants and young children,” Ameri-can Journal of Respiratory and Critical Care Medicine, vol. 164,no. 3, pp. 447–454, 2001.
[13] S. P. Galant, T. Morphew, S. Amaro, and O. Liao, “Value of thebronchodilator response in assessing controller naıve asthmaticchildren,”The Journal of Pediatrics, vol. 151, no. 5, pp. 457–462.e1,2007.
[14] I. Dundas, E. Y. Chan, P. D. Bridge, and S. A. McKenzie, “Diag-nostic accuracy of bronchodilator responsiveness in wheezychildren,”Thorax, vol. 60, no. 1, pp. 13–16, 2005.
[15] D. R. Rao, J. M. Gaffin, S. N. Baxi, W. J. Sheehan, E. B. Hoffman,and W. Phipatanakul, “The utility of forced expiratory flowbetween 25% and 75% of vital capacity in predicting childhoodasthmamorbidity and severity,” Journal of Asthma, vol. 49, no. 6,pp. 586–592, 2012.
[16] M. R. Simon, V. M. Chinchilli, B. R. Phillips et al., “Forcedexpiratory flow between 25% and 75% of vital capacity and

6 Canadian Respiratory Journal
FEV1/forced vital capacity ratio in relation to clinical and phys-
iological parameters in asthmatic children with normal FEV1
values,” Journal of Allergy and Clinical Immunology, vol. 126,no. 3, pp. 527–534.e8, 2010.
[17] E. Bar-Yishay, I. Amirav, and S. Goldberg, “Comparison ofmaximal midexpiratory flow rate and forced expiratory flow at50% of vital capacity in children,” Chest, vol. 123, no. 3, pp. 731–735, 2003.
[18] K. G. Nielsen and H. Bisgaard, “Discriminative capacity ofbronchodilator response measured with three different lungfunction techniques in asthmatic and healthy children aged 2to 5 years,” American Journal of Respiratory and Critical CareMedicine, vol. 164, no. 4, pp. 554–559, 2001.
[19] E. Oostveen, S. Dom, K. Desager, M. Hagendorens, W. DeBacker, and J. Weyler, “Lung function and bronchodilatorresponse in 4-year-old children with different wheezing pheno-types,” European Respiratory Journal, vol. 35, no. 4, pp. 865–872,2010.
[20] N. Beydon, C. M’Buila, C. Peiffer, A. Bernard, I. Zaccaria, andA. Denjean, “Can bronchodilator response predict bronchialresponse to methacholine in preschool coughers?” PediatricPulmonology, vol. 43, no. 8, pp. 815–821, 2008.
[21] J. Black, A. D. G. Baxter-Jones, J. Gordon, A. L. Findlay, and P. J.Helms, “Assessment of airway function in young children withasthma: comparison of spirometry, interrupter technique, andtidal flow by inductance plethsmography,” Pediatric Pulmono-logy, vol. 37, no. 6, pp. 548–553, 2004.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com