Embed Size (px)
Citation preview

Research ArticleRestoration of a Critical Mandibular Bone DefectUsing Human Alveolar Bone-Derived Stem Cells andPorous Nano-HACollagenPLA Scaffold
Xing Wang12 Helin Xing1 Guilan Zhang1 Xia Wu1
Xuan Zou1 Lin Feng1 Dongsheng Wang1 Meng Li1 Jing Zhao2
Jianwei Du3 Yan Lv1 Lingling E1 and Hongchen Liu1
1 Institute of Stomatology Chinese PLA General Hospital Beijing 100853 China2Hospital of Stomatology Shanxi Medical University Taiyuan 030001 China3Department of Orthopedics Chinese PLA General Hospital Beijing 100853 China
Correspondence should be addressed to Lingling E elingling2004sinacom and Hongchen Liu chinese621163com
Received 22 November 2015 Accepted 8 March 2016
Academic Editor Armand Keating
Copyright copy 2016 Xing Wang et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Periodontal bone defects occur in a wide variety of clinical situations Adult stem cell- and biomaterial-based bone tissueregeneration are a promising alternative to natural bone grafts Recent evidence has demonstrated that two populations of adultbone marrow mesenchymal stromal cells (BMSCs) can be distinguished based on their embryonic origins These BMSCs are notinterchangeable as bones preferentially heal using cells that share the same embryonic origin However the feasibility of tissueengineering using human craniofacial BMSCs was unclear The goal of this study was to explore human craniofacial BMSC-basedtherapy for the treatment of localized mandibular defects using a standardized minimally invasive procedureThe BMSCsrsquo identitywas confirmed Scanning electron microscopy a cell proliferation assay and supernatant detection indicated that the nHACPLAprovided a suitable environment for aBMSCs Real-time PCR and electrochemiluminescence immunoassays demonstrated thatosteogenicmarkers were upregulated by osteogenic preinductionMoreover in a rabbit critical-sizemandibular bone defect modeltotal bone formation in the nHACPLA + aBMSCs group was significantly higher than in the nHACPLA group but significantlylower than in the nHACPLA + preinduced aBMSCs These findings demonstrate that this engineered bone is a valid alternativefor the correction of mandibular bone defects
1 Introduction
Periodontal bone defects caused by periodontal diseasetrauma surgery or tumor resection are very common andthus consume a large amount of medical resources annuallyAutogenous bone (AB) grafting is the gold standard toreconstruct these defects but sources of donor tissue arelimited Allografts have not been extensively applied inclinical practice due to the associated risks of antigenicityand cross-infection [1] Synthetic materials have been studiedextensively as potential bone substitutes but due to a lackof inherent osteogenic cells and osteoinductivity limitedformation of new bone occurs after osteoconduction isachieved [2]
As one approach to overcome these problems bioma-terial- and autologous stem cell-based tissue engineering hasattractedmuch attention as a promising alternative to naturalbone grafts Among adult stem cells mesenchymal stromalcells (MSCs) are favorite candidate seed cells for bone tissueregeneration because of their multipotency immunomodu-latory properties and ability to release trophic factors [3 4]Although various adult tissue sources of MSCs such as bonemarrow fat muscle dermis and dental tissues have beendiscovered iliac bone marrow aspirates remain the principalsource for bone regeneration [5 6]
In preclinical and clinical studies iliac-derived bonemar-row mesenchymal stromal cells (BMSCs) have demonstratedpromise for restoring bone defects and healing nonunion
Hindawi Publishing CorporationStem Cells InternationalVolume 2016 Article ID 8741641 13 pageshttpdxdoiorg10115520168741641
2 Stem Cells International
fractures [7 8] However in clinical treatment fear of painand postoperative iliac complications has precluded theroutine therapeutic use of BMSCs particularly in dentalpatients who require alveolar bone augmentation This issuesuggests the need for the development of a more usable andminimally invasive procedure to isolate BMSCs [9 10]
Recent evidence has suggested that at least two popula-tions of adult skeletal progenitor cells can be distinguishedbased on their embryonic origins Craniofacial bone arisesfrom neural crest cells and ossifies via intramembranousossification whereas the appendicular skeleton arises frommesenchymal condensations of the mesoderm which thenundergoes perichondral ossification [11 12] Bridging cranio-facial defects with grafts obtained from a craniofacial donorsite is usually more successful than doing so with graftsfrom appendicular sites indicating that skeletal site-specificdifferences affect graft integration [13 14] Furthermorea selective recruitment mechanism through which adultskeletal defects heal involving recruitment of progenitor cellsof the same origin has been demonstrated indicating thatBMSCs from the craniofacial and appendicular skeletonsare not interchangeable [15] The presence of two distinctpopulations of BMSCs in the adult might have clinical impli-cations because if bones preferentially heal using cells thatshare the same embryonic origin then reparative strategiesmay have to take this variable into account to be maximallyeffective However before the present investigation the fea-sibility and effectiveness of tissue engineering using humancraniofacial BMSCs to restore mandibular bone defects wereunclear
The goal of this study was to explore human cranio-facial BMSC-based tissue engineering for the treatment oflocalized mandibular defects using a standardized mini-mally invasive procedure For this purpose human alveolarBMSCs (aBMSCs) were isolated painlessly during conven-tional dental implant surgery and the characteristics ofthe aBMSCs were analyzed in 2-dimensional cultures andon a porous nanohydroxyapatitecollagenpoly(L-lactide)(nHACPLA) scaffold The osteogenic capability biocom-patibility and biological safety of the constructs were alsoevaluated both in vitro and in vivo
2 Materials and Methods
21 Isolation and Culture of aBMSCs Human alveolar bonemarrow specimens were obtained from 52 patients duringdental implant surgery following Chinese PLA General Hos-pital Review Board approval In particular after informedconsent was obtained we administered local anesthesia andremoved the gingival flap and bone cortex at the implantsites using a flapless surgical procedure Next we graduallydrilled into the cancellous bone at 50 rpm without irrigationuntil the desired diameter and length for the implant wereobtained Bone marrow scraped from the bone core thatwas harvested from the pilot drill was immediately placedin sterile tubes containing minimum essential alpha medium(120572MEM Gibco Carlsbad CA USA) (Figure 1) Beforedental implant placement a 225-gauge needle connected toa heparinized syringe was inserted into the drill holes to
obtain themarrow aspirate [16] Both the collected debris andthe aspirate were immediately transported to the laboratoryfor aBMSC isolation The samples in 120572MEM medium werethen centrifuged at 500 g for 5 minutes The supernatantwas removed and the cell pellets were transferred to 25 cm2culture flasks and resuspended in 5mL of basic mediumconsisting of 120572MEM supplemented with 15 fetal bovineserum (FBS Gibco) The culture flasks were then incubatedundisturbed without medium changes for 5 days in a 37∘Chumidified tissue culture incubator at 5 CO
2 Once the
cell density reached approximately 80 confluence the cellswere detached using trypsinethylenediaminetetraacetic acid(EDTA Sigma St Louis MO USA) treatment and werepassaged or used for subsequent analysis Not all specimenscould be included in every experiment because of the surgicalschedule and the number of cells needed for each assayIn each experiment cells obtained from different subjectswere stored for analysis at the same time to avoid technicaldifferences between assays
22 Flow Cytometric Analysis aBMSCs at passage 3 weretrypsinized washed and resuspended in phosphate-bufferedsaline (PBS Gibco) at a concentration of 1 times 105 cellsmLThe cells were subsequently immunolabeled with mousemonoclonal anti-human antibodies specific for the followingCD14 CD34 CD44 CD90 CD106 and HLA-DR (AbcamCambridge MA USA) Mouse isotype antibodies served ascontrolsThe cells were thenwashed again with PBS and fixedin 2 paraformaldehyde after which the immunolabeledcells were detected by flow cytometry (BD Biosciences NJUSA)
23 Immunofluorescence aBMSCs at passage 3 weredetached using solution of versene (EDTAPBS) and weresubcultured on 12-chamber slides for 24 hours The sampleswere then fixed in 2 paraformaldehyde for 15 minutesfollowed by incubation with anti-STRO-1 antibody (1 200RampD Systems Inc Minneapolis MN USA) for 3 hoursThe cells were subsequently incubated with anti-mouseIgG TRITC (1 50 Santa Cruz Biotechnology Inc USA)for 1 hour and stained with 410158406-diamidino-2-phenylindole(DAPI 2120583gmL Sigma)
24 Multilineage Differentiation aBMSCs at passage 3 werecultured on six-well culture plates at a density of 2 times 105cellscm2 in induction medium For osteogenic differentia-tion the osteogenic induction medium consisted of 120572MEM15 FBS 10 nM dexamethasone 100mM glycerophosphateand 50120583gmL ascorbic acid [17] The medium was renewedtwo times each week At day 21 the cells were stained withAlizarin red
For adipogenic differentiation the induction mediumconsisted of 200120583M indomethacin 1 120583M dexamethasone05mM 3-isobutyl-1-methylxanthine and 100 nM insulinThemediumwas renewed two times each week At day 21 thecells were fixed and stained with fresh Oil red O solution Asa control the same batch of aBMSCs was cultured in 120572MEMcontaining 15 FBS and stained at day 21
Stem Cells International 3
(a) (b) (c)
(d) (e) (f)
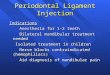
Figure 1 Clinical techniques for harvesting alveolar bone marrow (a) The cancellous bone was drilled at 50 rpm until achieving the desireddiameter and length for the implant site (b) Before dental implant placement bonemarrowwas harvested using a flapless minimally invasivesurgical procedure (c d) Bone marrow scraped from the pilot drill was immediately placed in sterile tubes and transported to the laboratory(e) Confirmation of the initial stability of the dental implant by cone-beam CT (f) Photomicrograph of aBMSCs 7ndash10 days following initialplating revealing a fibroblastic spindle shaped morphology similar to that of stem cells from other cell sources Magnification times400
25 Biometric Preparation and Seeding of nHACPLA Scaf-folds The features of the nHACPLA porous scaffold (All-gens Beijing China) were similar to that of natural bone aporosity of 70ndash90 and a pore size of 300ndash400plusmn150 120583m [18]aBMSCs at passage 3 were seeded into nHACPLA materialsthat had been cut into 10 times 5 times 3mm blocks The nHACPLA+ aBMSCs constructs were then incubated in basic mediumin a 24-well plate for 24 hours at 37∘C After the aBMSCs hadadhered to the nHACPLA the constructs were cultured inbasic medium or osteogenic induction medium for in vitrocharacterization and in vivo implantation
26 MTS Assay 3-(45-Dimethylthiazol-2-yl)-5-(3-carbox-ymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium innersalt (MTS Promega) was used as an indicator of cellviability In preparation aBMSCs at passage 3 were seededonto nHACPLA discs in 96-well culture plates at density of15 times 104 cellscm2 After culture for 24 hours the cells wereserum starved overnight in 120572MEM with 1 FBS and thencultured in basic medium (nHACPLA + aBMSCs group)or osteogenic induction medium (nHACPLA + preinducedaBMSCs group) for another 7 days On days 1 3 5 and7 during this period 20120583L of MTS was added and thesamples were incubated for 2 hours at 37∘C Subsequently
the absorbance of each well was measured at 490 nm usingan ELx800 UV reader (Bio-Tek Instruments Winooski VTUSA)
27 Scanning Electron Microscopy (SEM) aBMSCs were cul-tured on nHACPLA scaffolds in basic medium or osteogenicinduction medium at 1 times 105 cellscm2 for 7 days afterwhich the samples were washed with PBS and fixed in25 glutaraldehyde The samples were then coated withseveral nanometer-thick layers of gold The adhesion andmorphology of the aBMSCs on the surface of the nHACPLAcomposite were observed using a variable-pressure scanningelectron microscope (S-3400N Hitachi Japan) with beamenergies of 6ndash25 kV
28 Osteogenic Gene aBMSCs on nHACPLA scaffolds werecultured in osteogenic induction medium or basic mediumfor 7 days Total RNA was subsequently extracted usingTRIzol (Invitrogen Grand Island NY USA) and first-strandcomplementaryDNA (cDNA)was synthesized using a cDNAsynthesis kit (Promega Madison WI USA) Quantitativereal-time PCR was then performed using human osteocalcin(OCN) Runx2 Osterix and 120573-actin primers and FastSYBR Green MasterMix in a StepOnePlus Real-Time
4 Stem Cells International
PCR System (Applied Biosystems Carlsbad CA USA) Thefollowing primer sets were used Runx2 GenBank Accessionnumber 860 F51015840-CGGAATGCCTCTGCTGTTATGAA-31015840R51015840-AGGATTTGTGAAGACGGTTATGG-31015840 Osterixnumber 121340 F51015840-CTCCTCCTGCGACTGCCCTAAT-31015840 R51015840-AGGTG CGAAGCCTTG CCATACA-31015840 OCNnumber 632 F51015840-GGAGGGCAGCGAGGTAGTGAAG-31015840 R51015840-GATGTGGTCA GCCAACTCGTCA-31015840 actinnumber 60 F51015840-TGCCCATCTA CGAGGGGTATG-31015840 R51015840-TCCTTAAT GTCACGCACGATTTC-31015840 The expressionsof the genes were normalized to the internal control b-actinmRNA levels Data were analyzed using the comparison Ct(2minusΔΔCt)methodThe specificity of single-target amplificationby each primer pair was confirmed bymelting curve analysis
29 Alkaline Phosphatase (ALP) OCN Calcium and Phos-phonium Content Assays aBMSCs on nHACPLA scaffoldswere cultured for 21 days in basic medium or osteogenicinduction medium at 15 times 104cm2 cells per graft Thesupernatants were collected at 3 time points days 7 14 and21 The ALP activity in the medium was assayed using RocheDiagnostics ALP kits on the cobas e602 platform (RocheDiagnosticsMannheimGermany) and calcium content andphosphonium content were assayed using Roche DiagnosticsCaP kits OCN activity was assayed using N-MID osteocal-cin kits based on electrochemiluminescence immunoassaytechniques All data were measured and analyzed on thecobas 8000 platform (Roche Diagnostics)
210 Genetic Stability Assay Reverse transcription PCR wasperformed to examine the gene expression of tumor suppres-sors and protooncogenes For this purpose RNAwas isolatedfrom aBMSCs cultured on flasks at passages 1 and 2 and fromaBMSCs cultured on nHACPLA scaffolds in basic mediumor osteogenic induction medium at passage 3 The primersequences were as follows p53 F51015840-CCTCACCATCAT-CACA CTGG-31015840 R51015840-TTATGGCGGGAGGTAGACTG-31015840c-myc F51015840-CTCCTGGCAAAAGGTCAG AG-31015840 R51015840-GGC-CTTTTCATTGTTTTCCA-31015840 ARF F51015840-TGGGTCCCA-GTCTGCA GTTA-31015840 R51015840-CTGCCCATCATCATGACCT-31015840 GAPDH F51015840-ACAGTCAGCC GCATCTTCTT-31015840 R51015840-ACGACCAAAT CCGTTGACTC-31015840
At the end of culture aBMSCs from three different patientsamples at passage 4 were subjected to karyotyping analysisThese aBMSCs were cultured on nHACPLA scaffolds inosteogenic induction medium followed by treatment with60 ngmL colcemid (Sigma) and harvesting with 025trypsinEDTA The cells were then collected by centrifu-gation and karyotyping analysis was performed using G-banding techniques in a clinical laboratory at the ChinesePLA General Hospital
211 Bone Regeneration in the Mandibular Defect Model Thebone-forming capacity of 20 different aBMSCs populationswas evaluated qualitatively in a New Zealand white rabbitsegmental critical-size mandibular defect model [18 19] Forthis purpose 30 female rabbits were housed in the laboratoryanimal center at the Chinese PLA General Hospital The
rabbits had weights of 250ndash300 kg All surgical proceduresand care followed Chinese PLA General Hospital ReviewBoard approval The rabbits were first intravenously anes-thetized with 2 pentobarbital sodium (30mgkg) The hairon the right of the rabbit mandible was then depilated Underaseptic conditions a 10mm incision was made along theupper edge of the rabbit mandible and the right buccal wasexposed A segmental defect (10 times 5 times 3mm) was prepared inthe alveolar bone of all rabbits using a surgical oscillating sawand sterile saline irrigation nHACPLA blocks withwithout5 times 106 aBMSCs were implanted in the segmental defectand the rabbits were assigned to five groups mandibulardefects were treated with nHACPLA nHACPLA + aBM-SCs or nHACPLA + preinduced aBMSCs (preinduced inosteogenic induction medium for 7 days) or with AB fromthe iliac bone as a positive control or untreated defect as anegative control
After eight weeks the samples were surgically removedand fixed Goldnerrsquos trichrome staining was used to examinebone regeneration at the defects All samples were analyzedby morphometric analysis using the Leica-Q Win 32 imageanalysis system Five sequential sections per implant wereselected and the type of tissue (mature bone-like or osteoid-like) was identified by an independent observer The extentof newly formed bone was indicated by the percentage of thenewly formed bone areas within a section An average valuewas then calculated for each implant and data were averagedacross all implants within each group
212 Assessment of Bone Regeneration byMicro-CT Thebonevolume and trabecular microarchitecture were monitoredusing a Quantum FX micro-CT Imaging System (CaliperUSA) at 70 kV and 114mA A total of 512 binary images wereobtained with a wide field of view (FOV) with scanning at36mm and a 45 120583m voxel size resolution The thresholdswere set at 1300 which was adequate to separate bone andnHAC using discrimination analysis The calculated bonevolume density (bone volumetotal volume) in this area ispresented as the percentage regeneration of the defect
213 Statistical Analysis All data are presented as the meanplusmn standard deviation Statistical analyses of the results wereperformed using SPSS 160 software Studentrsquos 119905-test was usedto study significant differences in the MTS PCR SEM ALPOCN and calcium and phosphonium content results One-way ANOVA and an unpaired 119905-test were used to studysignificant differences in the bone volume density and thepercentage of bone formation area between study groupsThesignificance threshold was set at 119901 lt 005
3 Results
31 Isolation and Characterization of aBMSCs We collectedalveolar bone marrow samples from 52 patients undergoingdental implant surgery Every dental implant was initiallystable (final torque gt 35Ncm) and no complications afterbone marrow collection were reported Postoperative 1- to 3-month cone-beam CT results revealed closely aligned dentalimplants and bone (Figure 1(e))
Stem Cells International 5
(a) (b) (c)
0
0
102
103
104
105 0
0
102
103
104
105
0
0
102
103
104
1050
0
102
103
104
105
0
0
102
103
104
105 0
0
102
103
104
105
CD44962
CD34217
CD90955
CD140866
CD106973
HLA-DR158
(d)
Figure 2 Characterization of human aBMSCs (a) The aBMSCs expressed STRO-1 a mesenchymal stromal cell marker Positive stainingof the cells with Alizarin red (b) or Oil red O (c) demonstrated the osteogenic and adipogenic differentiation potential of the aBMSCsMagnification times400 (d) The aBMSCs were positive for MSC markers including CD44 CD90 and CD106 and negative for hematopoieticand endothelial markers including CD14 CD34 and HLA-DR
The aBMSCs in 37 samples adhered to the culture surfaceand proliferated in vitroThe isolated aBMSCs formed single-cell-derived colonies and most of the cells retained theirfibroblastic spindle shape (Figure 1(f)) The aBMSCs wereexpanded in culture followed by characterization of cellsurfacemarkers by flow cytometry and immunofluorescenceImmunofluorescence analysis demonstrated that the cells
were STRO-1 positive (Figure 2(a)) To evaluate the invitro differentiation potential of the aBMSCs the cells wereinduced to differentiate along osteogenic and adipogeniclineages under specific culture conditions as revealed byAlizarin red (Figure 2(b)) and Oil red O (Figure 2(c))staining Flow cytometry revealed that the cultured cellswere homogenously positive for CD44 CD90 and CD106
6 Stem Cells International
(a) (b) (c)
(d) (e) (f)
20
15
10
05
00
OD
val
ue
1 3 5 7
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(g)
Rela
tive q
uant
ifica
tion
20
15
10
05
00OCN OSX RUNX2
lowast
lowast lowast
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(h)
Figure 3 Proliferation and osteogenic differentiation potential of aBMSCs on nHACPLA (a) SEM analysis showed that nHACPLA wassimilar to natural bone in terms of microstructure (b) After 3 days of culture the aBMSCs adhered to extended and connected with eachother and produced ECM on the nHACPLA surface The aBMSCs (cndashf) were spindle triangle or cube shaped with developed cytoplasmicextensions attached to the scaffold (g) The MTS results demonstrated that the aBMSCs were proliferative on days 1 3 5 and 7 after seedingonto nHACPLA (119899 = 6 mean plusmn SD) (h) Real-time PCR revealed that osteogenic induction for 7 days promoted aBMSC expression of OCNRunx2 and Osterix (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005 Magnification (ab) times100 SE (c) times500 SE (d) times150 k SE (e) times500 k SE (f) times100 k SE
and negative for hematopoietic and endothelial cell surfacemarkers including CD14 CD34 and HLA-DR (Figure 2(d))
32 Biocompatibility between aBMSCs and nHACPLA Theadherence and morphology of aBMSCs on nHACPLA wereobserved by SEM which revealed that the nHACPLAblocks without cells exhibited a hierarchical microstruc-ture (Figure 3(a)) After 3 days of culture the aBMSCsadhered to extended and connected with each other and
produced extracellular matrix (ECM) on the nHACPLAsurface (Figure 3(b)) The aBMSCs were spindle triangle orcube shaped with developed cytoplasmic extensions attachedto the scaffold (Figures 3(c)ndash3(f))
The proliferation of aBMSCs on nHACPLA was evalu-ated using theMTSmethod ondays 1 3 5 and 7 (Figure 3(g))Throughout the 7 days of culture the cell numbers increasedindicating that the nHACPLA had no negative effect onproliferation Compared with cells cultured in basic medium
Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

2 Stem Cells International
fractures [7 8] However in clinical treatment fear of painand postoperative iliac complications has precluded theroutine therapeutic use of BMSCs particularly in dentalpatients who require alveolar bone augmentation This issuesuggests the need for the development of a more usable andminimally invasive procedure to isolate BMSCs [9 10]
Recent evidence has suggested that at least two popula-tions of adult skeletal progenitor cells can be distinguishedbased on their embryonic origins Craniofacial bone arisesfrom neural crest cells and ossifies via intramembranousossification whereas the appendicular skeleton arises frommesenchymal condensations of the mesoderm which thenundergoes perichondral ossification [11 12] Bridging cranio-facial defects with grafts obtained from a craniofacial donorsite is usually more successful than doing so with graftsfrom appendicular sites indicating that skeletal site-specificdifferences affect graft integration [13 14] Furthermorea selective recruitment mechanism through which adultskeletal defects heal involving recruitment of progenitor cellsof the same origin has been demonstrated indicating thatBMSCs from the craniofacial and appendicular skeletonsare not interchangeable [15] The presence of two distinctpopulations of BMSCs in the adult might have clinical impli-cations because if bones preferentially heal using cells thatshare the same embryonic origin then reparative strategiesmay have to take this variable into account to be maximallyeffective However before the present investigation the fea-sibility and effectiveness of tissue engineering using humancraniofacial BMSCs to restore mandibular bone defects wereunclear
The goal of this study was to explore human cranio-facial BMSC-based tissue engineering for the treatment oflocalized mandibular defects using a standardized mini-mally invasive procedure For this purpose human alveolarBMSCs (aBMSCs) were isolated painlessly during conven-tional dental implant surgery and the characteristics ofthe aBMSCs were analyzed in 2-dimensional cultures andon a porous nanohydroxyapatitecollagenpoly(L-lactide)(nHACPLA) scaffold The osteogenic capability biocom-patibility and biological safety of the constructs were alsoevaluated both in vitro and in vivo
2 Materials and Methods
21 Isolation and Culture of aBMSCs Human alveolar bonemarrow specimens were obtained from 52 patients duringdental implant surgery following Chinese PLA General Hos-pital Review Board approval In particular after informedconsent was obtained we administered local anesthesia andremoved the gingival flap and bone cortex at the implantsites using a flapless surgical procedure Next we graduallydrilled into the cancellous bone at 50 rpm without irrigationuntil the desired diameter and length for the implant wereobtained Bone marrow scraped from the bone core thatwas harvested from the pilot drill was immediately placedin sterile tubes containing minimum essential alpha medium(120572MEM Gibco Carlsbad CA USA) (Figure 1) Beforedental implant placement a 225-gauge needle connected toa heparinized syringe was inserted into the drill holes to
obtain themarrow aspirate [16] Both the collected debris andthe aspirate were immediately transported to the laboratoryfor aBMSC isolation The samples in 120572MEM medium werethen centrifuged at 500 g for 5 minutes The supernatantwas removed and the cell pellets were transferred to 25 cm2culture flasks and resuspended in 5mL of basic mediumconsisting of 120572MEM supplemented with 15 fetal bovineserum (FBS Gibco) The culture flasks were then incubatedundisturbed without medium changes for 5 days in a 37∘Chumidified tissue culture incubator at 5 CO
2 Once the
cell density reached approximately 80 confluence the cellswere detached using trypsinethylenediaminetetraacetic acid(EDTA Sigma St Louis MO USA) treatment and werepassaged or used for subsequent analysis Not all specimenscould be included in every experiment because of the surgicalschedule and the number of cells needed for each assayIn each experiment cells obtained from different subjectswere stored for analysis at the same time to avoid technicaldifferences between assays
22 Flow Cytometric Analysis aBMSCs at passage 3 weretrypsinized washed and resuspended in phosphate-bufferedsaline (PBS Gibco) at a concentration of 1 times 105 cellsmLThe cells were subsequently immunolabeled with mousemonoclonal anti-human antibodies specific for the followingCD14 CD34 CD44 CD90 CD106 and HLA-DR (AbcamCambridge MA USA) Mouse isotype antibodies served ascontrolsThe cells were thenwashed again with PBS and fixedin 2 paraformaldehyde after which the immunolabeledcells were detected by flow cytometry (BD Biosciences NJUSA)
23 Immunofluorescence aBMSCs at passage 3 weredetached using solution of versene (EDTAPBS) and weresubcultured on 12-chamber slides for 24 hours The sampleswere then fixed in 2 paraformaldehyde for 15 minutesfollowed by incubation with anti-STRO-1 antibody (1 200RampD Systems Inc Minneapolis MN USA) for 3 hoursThe cells were subsequently incubated with anti-mouseIgG TRITC (1 50 Santa Cruz Biotechnology Inc USA)for 1 hour and stained with 410158406-diamidino-2-phenylindole(DAPI 2120583gmL Sigma)
24 Multilineage Differentiation aBMSCs at passage 3 werecultured on six-well culture plates at a density of 2 times 105cellscm2 in induction medium For osteogenic differentia-tion the osteogenic induction medium consisted of 120572MEM15 FBS 10 nM dexamethasone 100mM glycerophosphateand 50120583gmL ascorbic acid [17] The medium was renewedtwo times each week At day 21 the cells were stained withAlizarin red
For adipogenic differentiation the induction mediumconsisted of 200120583M indomethacin 1 120583M dexamethasone05mM 3-isobutyl-1-methylxanthine and 100 nM insulinThemediumwas renewed two times each week At day 21 thecells were fixed and stained with fresh Oil red O solution Asa control the same batch of aBMSCs was cultured in 120572MEMcontaining 15 FBS and stained at day 21
Stem Cells International 3
(a) (b) (c)
(d) (e) (f)
Figure 1 Clinical techniques for harvesting alveolar bone marrow (a) The cancellous bone was drilled at 50 rpm until achieving the desireddiameter and length for the implant site (b) Before dental implant placement bonemarrowwas harvested using a flapless minimally invasivesurgical procedure (c d) Bone marrow scraped from the pilot drill was immediately placed in sterile tubes and transported to the laboratory(e) Confirmation of the initial stability of the dental implant by cone-beam CT (f) Photomicrograph of aBMSCs 7ndash10 days following initialplating revealing a fibroblastic spindle shaped morphology similar to that of stem cells from other cell sources Magnification times400
25 Biometric Preparation and Seeding of nHACPLA Scaf-folds The features of the nHACPLA porous scaffold (All-gens Beijing China) were similar to that of natural bone aporosity of 70ndash90 and a pore size of 300ndash400plusmn150 120583m [18]aBMSCs at passage 3 were seeded into nHACPLA materialsthat had been cut into 10 times 5 times 3mm blocks The nHACPLA+ aBMSCs constructs were then incubated in basic mediumin a 24-well plate for 24 hours at 37∘C After the aBMSCs hadadhered to the nHACPLA the constructs were cultured inbasic medium or osteogenic induction medium for in vitrocharacterization and in vivo implantation
26 MTS Assay 3-(45-Dimethylthiazol-2-yl)-5-(3-carbox-ymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium innersalt (MTS Promega) was used as an indicator of cellviability In preparation aBMSCs at passage 3 were seededonto nHACPLA discs in 96-well culture plates at density of15 times 104 cellscm2 After culture for 24 hours the cells wereserum starved overnight in 120572MEM with 1 FBS and thencultured in basic medium (nHACPLA + aBMSCs group)or osteogenic induction medium (nHACPLA + preinducedaBMSCs group) for another 7 days On days 1 3 5 and7 during this period 20120583L of MTS was added and thesamples were incubated for 2 hours at 37∘C Subsequently
the absorbance of each well was measured at 490 nm usingan ELx800 UV reader (Bio-Tek Instruments Winooski VTUSA)
27 Scanning Electron Microscopy (SEM) aBMSCs were cul-tured on nHACPLA scaffolds in basic medium or osteogenicinduction medium at 1 times 105 cellscm2 for 7 days afterwhich the samples were washed with PBS and fixed in25 glutaraldehyde The samples were then coated withseveral nanometer-thick layers of gold The adhesion andmorphology of the aBMSCs on the surface of the nHACPLAcomposite were observed using a variable-pressure scanningelectron microscope (S-3400N Hitachi Japan) with beamenergies of 6ndash25 kV
28 Osteogenic Gene aBMSCs on nHACPLA scaffolds werecultured in osteogenic induction medium or basic mediumfor 7 days Total RNA was subsequently extracted usingTRIzol (Invitrogen Grand Island NY USA) and first-strandcomplementaryDNA (cDNA)was synthesized using a cDNAsynthesis kit (Promega Madison WI USA) Quantitativereal-time PCR was then performed using human osteocalcin(OCN) Runx2 Osterix and 120573-actin primers and FastSYBR Green MasterMix in a StepOnePlus Real-Time
4 Stem Cells International
PCR System (Applied Biosystems Carlsbad CA USA) Thefollowing primer sets were used Runx2 GenBank Accessionnumber 860 F51015840-CGGAATGCCTCTGCTGTTATGAA-31015840R51015840-AGGATTTGTGAAGACGGTTATGG-31015840 Osterixnumber 121340 F51015840-CTCCTCCTGCGACTGCCCTAAT-31015840 R51015840-AGGTG CGAAGCCTTG CCATACA-31015840 OCNnumber 632 F51015840-GGAGGGCAGCGAGGTAGTGAAG-31015840 R51015840-GATGTGGTCA GCCAACTCGTCA-31015840 actinnumber 60 F51015840-TGCCCATCTA CGAGGGGTATG-31015840 R51015840-TCCTTAAT GTCACGCACGATTTC-31015840 The expressionsof the genes were normalized to the internal control b-actinmRNA levels Data were analyzed using the comparison Ct(2minusΔΔCt)methodThe specificity of single-target amplificationby each primer pair was confirmed bymelting curve analysis
29 Alkaline Phosphatase (ALP) OCN Calcium and Phos-phonium Content Assays aBMSCs on nHACPLA scaffoldswere cultured for 21 days in basic medium or osteogenicinduction medium at 15 times 104cm2 cells per graft Thesupernatants were collected at 3 time points days 7 14 and21 The ALP activity in the medium was assayed using RocheDiagnostics ALP kits on the cobas e602 platform (RocheDiagnosticsMannheimGermany) and calcium content andphosphonium content were assayed using Roche DiagnosticsCaP kits OCN activity was assayed using N-MID osteocal-cin kits based on electrochemiluminescence immunoassaytechniques All data were measured and analyzed on thecobas 8000 platform (Roche Diagnostics)
210 Genetic Stability Assay Reverse transcription PCR wasperformed to examine the gene expression of tumor suppres-sors and protooncogenes For this purpose RNAwas isolatedfrom aBMSCs cultured on flasks at passages 1 and 2 and fromaBMSCs cultured on nHACPLA scaffolds in basic mediumor osteogenic induction medium at passage 3 The primersequences were as follows p53 F51015840-CCTCACCATCAT-CACA CTGG-31015840 R51015840-TTATGGCGGGAGGTAGACTG-31015840c-myc F51015840-CTCCTGGCAAAAGGTCAG AG-31015840 R51015840-GGC-CTTTTCATTGTTTTCCA-31015840 ARF F51015840-TGGGTCCCA-GTCTGCA GTTA-31015840 R51015840-CTGCCCATCATCATGACCT-31015840 GAPDH F51015840-ACAGTCAGCC GCATCTTCTT-31015840 R51015840-ACGACCAAAT CCGTTGACTC-31015840
At the end of culture aBMSCs from three different patientsamples at passage 4 were subjected to karyotyping analysisThese aBMSCs were cultured on nHACPLA scaffolds inosteogenic induction medium followed by treatment with60 ngmL colcemid (Sigma) and harvesting with 025trypsinEDTA The cells were then collected by centrifu-gation and karyotyping analysis was performed using G-banding techniques in a clinical laboratory at the ChinesePLA General Hospital
211 Bone Regeneration in the Mandibular Defect Model Thebone-forming capacity of 20 different aBMSCs populationswas evaluated qualitatively in a New Zealand white rabbitsegmental critical-size mandibular defect model [18 19] Forthis purpose 30 female rabbits were housed in the laboratoryanimal center at the Chinese PLA General Hospital The
rabbits had weights of 250ndash300 kg All surgical proceduresand care followed Chinese PLA General Hospital ReviewBoard approval The rabbits were first intravenously anes-thetized with 2 pentobarbital sodium (30mgkg) The hairon the right of the rabbit mandible was then depilated Underaseptic conditions a 10mm incision was made along theupper edge of the rabbit mandible and the right buccal wasexposed A segmental defect (10 times 5 times 3mm) was prepared inthe alveolar bone of all rabbits using a surgical oscillating sawand sterile saline irrigation nHACPLA blocks withwithout5 times 106 aBMSCs were implanted in the segmental defectand the rabbits were assigned to five groups mandibulardefects were treated with nHACPLA nHACPLA + aBM-SCs or nHACPLA + preinduced aBMSCs (preinduced inosteogenic induction medium for 7 days) or with AB fromthe iliac bone as a positive control or untreated defect as anegative control
After eight weeks the samples were surgically removedand fixed Goldnerrsquos trichrome staining was used to examinebone regeneration at the defects All samples were analyzedby morphometric analysis using the Leica-Q Win 32 imageanalysis system Five sequential sections per implant wereselected and the type of tissue (mature bone-like or osteoid-like) was identified by an independent observer The extentof newly formed bone was indicated by the percentage of thenewly formed bone areas within a section An average valuewas then calculated for each implant and data were averagedacross all implants within each group
212 Assessment of Bone Regeneration byMicro-CT Thebonevolume and trabecular microarchitecture were monitoredusing a Quantum FX micro-CT Imaging System (CaliperUSA) at 70 kV and 114mA A total of 512 binary images wereobtained with a wide field of view (FOV) with scanning at36mm and a 45 120583m voxel size resolution The thresholdswere set at 1300 which was adequate to separate bone andnHAC using discrimination analysis The calculated bonevolume density (bone volumetotal volume) in this area ispresented as the percentage regeneration of the defect
213 Statistical Analysis All data are presented as the meanplusmn standard deviation Statistical analyses of the results wereperformed using SPSS 160 software Studentrsquos 119905-test was usedto study significant differences in the MTS PCR SEM ALPOCN and calcium and phosphonium content results One-way ANOVA and an unpaired 119905-test were used to studysignificant differences in the bone volume density and thepercentage of bone formation area between study groupsThesignificance threshold was set at 119901 lt 005
3 Results
31 Isolation and Characterization of aBMSCs We collectedalveolar bone marrow samples from 52 patients undergoingdental implant surgery Every dental implant was initiallystable (final torque gt 35Ncm) and no complications afterbone marrow collection were reported Postoperative 1- to 3-month cone-beam CT results revealed closely aligned dentalimplants and bone (Figure 1(e))
Stem Cells International 5
(a) (b) (c)
0
0
102
103
104
105 0
0
102
103
104
105
0
0
102
103
104
1050
0
102
103
104
105
0
0
102
103
104
105 0
0
102
103
104
105
CD44962
CD34217
CD90955
CD140866
CD106973
HLA-DR158
(d)
Figure 2 Characterization of human aBMSCs (a) The aBMSCs expressed STRO-1 a mesenchymal stromal cell marker Positive stainingof the cells with Alizarin red (b) or Oil red O (c) demonstrated the osteogenic and adipogenic differentiation potential of the aBMSCsMagnification times400 (d) The aBMSCs were positive for MSC markers including CD44 CD90 and CD106 and negative for hematopoieticand endothelial markers including CD14 CD34 and HLA-DR
The aBMSCs in 37 samples adhered to the culture surfaceand proliferated in vitroThe isolated aBMSCs formed single-cell-derived colonies and most of the cells retained theirfibroblastic spindle shape (Figure 1(f)) The aBMSCs wereexpanded in culture followed by characterization of cellsurfacemarkers by flow cytometry and immunofluorescenceImmunofluorescence analysis demonstrated that the cells
were STRO-1 positive (Figure 2(a)) To evaluate the invitro differentiation potential of the aBMSCs the cells wereinduced to differentiate along osteogenic and adipogeniclineages under specific culture conditions as revealed byAlizarin red (Figure 2(b)) and Oil red O (Figure 2(c))staining Flow cytometry revealed that the cultured cellswere homogenously positive for CD44 CD90 and CD106
6 Stem Cells International
(a) (b) (c)
(d) (e) (f)
20
15
10
05
00
OD
val
ue
1 3 5 7
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(g)
Rela
tive q
uant
ifica
tion
20
15
10
05
00OCN OSX RUNX2
lowast
lowast lowast
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(h)
Figure 3 Proliferation and osteogenic differentiation potential of aBMSCs on nHACPLA (a) SEM analysis showed that nHACPLA wassimilar to natural bone in terms of microstructure (b) After 3 days of culture the aBMSCs adhered to extended and connected with eachother and produced ECM on the nHACPLA surface The aBMSCs (cndashf) were spindle triangle or cube shaped with developed cytoplasmicextensions attached to the scaffold (g) The MTS results demonstrated that the aBMSCs were proliferative on days 1 3 5 and 7 after seedingonto nHACPLA (119899 = 6 mean plusmn SD) (h) Real-time PCR revealed that osteogenic induction for 7 days promoted aBMSC expression of OCNRunx2 and Osterix (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005 Magnification (ab) times100 SE (c) times500 SE (d) times150 k SE (e) times500 k SE (f) times100 k SE
and negative for hematopoietic and endothelial cell surfacemarkers including CD14 CD34 and HLA-DR (Figure 2(d))
32 Biocompatibility between aBMSCs and nHACPLA Theadherence and morphology of aBMSCs on nHACPLA wereobserved by SEM which revealed that the nHACPLAblocks without cells exhibited a hierarchical microstruc-ture (Figure 3(a)) After 3 days of culture the aBMSCsadhered to extended and connected with each other and
produced extracellular matrix (ECM) on the nHACPLAsurface (Figure 3(b)) The aBMSCs were spindle triangle orcube shaped with developed cytoplasmic extensions attachedto the scaffold (Figures 3(c)ndash3(f))
The proliferation of aBMSCs on nHACPLA was evalu-ated using theMTSmethod ondays 1 3 5 and 7 (Figure 3(g))Throughout the 7 days of culture the cell numbers increasedindicating that the nHACPLA had no negative effect onproliferation Compared with cells cultured in basic medium
Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Stem Cells International 3
(a) (b) (c)
(d) (e) (f)
Figure 1 Clinical techniques for harvesting alveolar bone marrow (a) The cancellous bone was drilled at 50 rpm until achieving the desireddiameter and length for the implant site (b) Before dental implant placement bonemarrowwas harvested using a flapless minimally invasivesurgical procedure (c d) Bone marrow scraped from the pilot drill was immediately placed in sterile tubes and transported to the laboratory(e) Confirmation of the initial stability of the dental implant by cone-beam CT (f) Photomicrograph of aBMSCs 7ndash10 days following initialplating revealing a fibroblastic spindle shaped morphology similar to that of stem cells from other cell sources Magnification times400
25 Biometric Preparation and Seeding of nHACPLA Scaf-folds The features of the nHACPLA porous scaffold (All-gens Beijing China) were similar to that of natural bone aporosity of 70ndash90 and a pore size of 300ndash400plusmn150 120583m [18]aBMSCs at passage 3 were seeded into nHACPLA materialsthat had been cut into 10 times 5 times 3mm blocks The nHACPLA+ aBMSCs constructs were then incubated in basic mediumin a 24-well plate for 24 hours at 37∘C After the aBMSCs hadadhered to the nHACPLA the constructs were cultured inbasic medium or osteogenic induction medium for in vitrocharacterization and in vivo implantation
26 MTS Assay 3-(45-Dimethylthiazol-2-yl)-5-(3-carbox-ymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium innersalt (MTS Promega) was used as an indicator of cellviability In preparation aBMSCs at passage 3 were seededonto nHACPLA discs in 96-well culture plates at density of15 times 104 cellscm2 After culture for 24 hours the cells wereserum starved overnight in 120572MEM with 1 FBS and thencultured in basic medium (nHACPLA + aBMSCs group)or osteogenic induction medium (nHACPLA + preinducedaBMSCs group) for another 7 days On days 1 3 5 and7 during this period 20120583L of MTS was added and thesamples were incubated for 2 hours at 37∘C Subsequently
the absorbance of each well was measured at 490 nm usingan ELx800 UV reader (Bio-Tek Instruments Winooski VTUSA)
27 Scanning Electron Microscopy (SEM) aBMSCs were cul-tured on nHACPLA scaffolds in basic medium or osteogenicinduction medium at 1 times 105 cellscm2 for 7 days afterwhich the samples were washed with PBS and fixed in25 glutaraldehyde The samples were then coated withseveral nanometer-thick layers of gold The adhesion andmorphology of the aBMSCs on the surface of the nHACPLAcomposite were observed using a variable-pressure scanningelectron microscope (S-3400N Hitachi Japan) with beamenergies of 6ndash25 kV
28 Osteogenic Gene aBMSCs on nHACPLA scaffolds werecultured in osteogenic induction medium or basic mediumfor 7 days Total RNA was subsequently extracted usingTRIzol (Invitrogen Grand Island NY USA) and first-strandcomplementaryDNA (cDNA)was synthesized using a cDNAsynthesis kit (Promega Madison WI USA) Quantitativereal-time PCR was then performed using human osteocalcin(OCN) Runx2 Osterix and 120573-actin primers and FastSYBR Green MasterMix in a StepOnePlus Real-Time
4 Stem Cells International
PCR System (Applied Biosystems Carlsbad CA USA) Thefollowing primer sets were used Runx2 GenBank Accessionnumber 860 F51015840-CGGAATGCCTCTGCTGTTATGAA-31015840R51015840-AGGATTTGTGAAGACGGTTATGG-31015840 Osterixnumber 121340 F51015840-CTCCTCCTGCGACTGCCCTAAT-31015840 R51015840-AGGTG CGAAGCCTTG CCATACA-31015840 OCNnumber 632 F51015840-GGAGGGCAGCGAGGTAGTGAAG-31015840 R51015840-GATGTGGTCA GCCAACTCGTCA-31015840 actinnumber 60 F51015840-TGCCCATCTA CGAGGGGTATG-31015840 R51015840-TCCTTAAT GTCACGCACGATTTC-31015840 The expressionsof the genes were normalized to the internal control b-actinmRNA levels Data were analyzed using the comparison Ct(2minusΔΔCt)methodThe specificity of single-target amplificationby each primer pair was confirmed bymelting curve analysis
29 Alkaline Phosphatase (ALP) OCN Calcium and Phos-phonium Content Assays aBMSCs on nHACPLA scaffoldswere cultured for 21 days in basic medium or osteogenicinduction medium at 15 times 104cm2 cells per graft Thesupernatants were collected at 3 time points days 7 14 and21 The ALP activity in the medium was assayed using RocheDiagnostics ALP kits on the cobas e602 platform (RocheDiagnosticsMannheimGermany) and calcium content andphosphonium content were assayed using Roche DiagnosticsCaP kits OCN activity was assayed using N-MID osteocal-cin kits based on electrochemiluminescence immunoassaytechniques All data were measured and analyzed on thecobas 8000 platform (Roche Diagnostics)
210 Genetic Stability Assay Reverse transcription PCR wasperformed to examine the gene expression of tumor suppres-sors and protooncogenes For this purpose RNAwas isolatedfrom aBMSCs cultured on flasks at passages 1 and 2 and fromaBMSCs cultured on nHACPLA scaffolds in basic mediumor osteogenic induction medium at passage 3 The primersequences were as follows p53 F51015840-CCTCACCATCAT-CACA CTGG-31015840 R51015840-TTATGGCGGGAGGTAGACTG-31015840c-myc F51015840-CTCCTGGCAAAAGGTCAG AG-31015840 R51015840-GGC-CTTTTCATTGTTTTCCA-31015840 ARF F51015840-TGGGTCCCA-GTCTGCA GTTA-31015840 R51015840-CTGCCCATCATCATGACCT-31015840 GAPDH F51015840-ACAGTCAGCC GCATCTTCTT-31015840 R51015840-ACGACCAAAT CCGTTGACTC-31015840
At the end of culture aBMSCs from three different patientsamples at passage 4 were subjected to karyotyping analysisThese aBMSCs were cultured on nHACPLA scaffolds inosteogenic induction medium followed by treatment with60 ngmL colcemid (Sigma) and harvesting with 025trypsinEDTA The cells were then collected by centrifu-gation and karyotyping analysis was performed using G-banding techniques in a clinical laboratory at the ChinesePLA General Hospital
211 Bone Regeneration in the Mandibular Defect Model Thebone-forming capacity of 20 different aBMSCs populationswas evaluated qualitatively in a New Zealand white rabbitsegmental critical-size mandibular defect model [18 19] Forthis purpose 30 female rabbits were housed in the laboratoryanimal center at the Chinese PLA General Hospital The
rabbits had weights of 250ndash300 kg All surgical proceduresand care followed Chinese PLA General Hospital ReviewBoard approval The rabbits were first intravenously anes-thetized with 2 pentobarbital sodium (30mgkg) The hairon the right of the rabbit mandible was then depilated Underaseptic conditions a 10mm incision was made along theupper edge of the rabbit mandible and the right buccal wasexposed A segmental defect (10 times 5 times 3mm) was prepared inthe alveolar bone of all rabbits using a surgical oscillating sawand sterile saline irrigation nHACPLA blocks withwithout5 times 106 aBMSCs were implanted in the segmental defectand the rabbits were assigned to five groups mandibulardefects were treated with nHACPLA nHACPLA + aBM-SCs or nHACPLA + preinduced aBMSCs (preinduced inosteogenic induction medium for 7 days) or with AB fromthe iliac bone as a positive control or untreated defect as anegative control
After eight weeks the samples were surgically removedand fixed Goldnerrsquos trichrome staining was used to examinebone regeneration at the defects All samples were analyzedby morphometric analysis using the Leica-Q Win 32 imageanalysis system Five sequential sections per implant wereselected and the type of tissue (mature bone-like or osteoid-like) was identified by an independent observer The extentof newly formed bone was indicated by the percentage of thenewly formed bone areas within a section An average valuewas then calculated for each implant and data were averagedacross all implants within each group
212 Assessment of Bone Regeneration byMicro-CT Thebonevolume and trabecular microarchitecture were monitoredusing a Quantum FX micro-CT Imaging System (CaliperUSA) at 70 kV and 114mA A total of 512 binary images wereobtained with a wide field of view (FOV) with scanning at36mm and a 45 120583m voxel size resolution The thresholdswere set at 1300 which was adequate to separate bone andnHAC using discrimination analysis The calculated bonevolume density (bone volumetotal volume) in this area ispresented as the percentage regeneration of the defect
213 Statistical Analysis All data are presented as the meanplusmn standard deviation Statistical analyses of the results wereperformed using SPSS 160 software Studentrsquos 119905-test was usedto study significant differences in the MTS PCR SEM ALPOCN and calcium and phosphonium content results One-way ANOVA and an unpaired 119905-test were used to studysignificant differences in the bone volume density and thepercentage of bone formation area between study groupsThesignificance threshold was set at 119901 lt 005
3 Results
31 Isolation and Characterization of aBMSCs We collectedalveolar bone marrow samples from 52 patients undergoingdental implant surgery Every dental implant was initiallystable (final torque gt 35Ncm) and no complications afterbone marrow collection were reported Postoperative 1- to 3-month cone-beam CT results revealed closely aligned dentalimplants and bone (Figure 1(e))
Stem Cells International 5
(a) (b) (c)
0
0
102
103
104
105 0
0
102
103
104
105
0
0
102
103
104
1050
0
102
103
104
105
0
0
102
103
104
105 0
0
102
103
104
105
CD44962
CD34217
CD90955
CD140866
CD106973
HLA-DR158
(d)
Figure 2 Characterization of human aBMSCs (a) The aBMSCs expressed STRO-1 a mesenchymal stromal cell marker Positive stainingof the cells with Alizarin red (b) or Oil red O (c) demonstrated the osteogenic and adipogenic differentiation potential of the aBMSCsMagnification times400 (d) The aBMSCs were positive for MSC markers including CD44 CD90 and CD106 and negative for hematopoieticand endothelial markers including CD14 CD34 and HLA-DR
The aBMSCs in 37 samples adhered to the culture surfaceand proliferated in vitroThe isolated aBMSCs formed single-cell-derived colonies and most of the cells retained theirfibroblastic spindle shape (Figure 1(f)) The aBMSCs wereexpanded in culture followed by characterization of cellsurfacemarkers by flow cytometry and immunofluorescenceImmunofluorescence analysis demonstrated that the cells
were STRO-1 positive (Figure 2(a)) To evaluate the invitro differentiation potential of the aBMSCs the cells wereinduced to differentiate along osteogenic and adipogeniclineages under specific culture conditions as revealed byAlizarin red (Figure 2(b)) and Oil red O (Figure 2(c))staining Flow cytometry revealed that the cultured cellswere homogenously positive for CD44 CD90 and CD106
6 Stem Cells International
(a) (b) (c)
(d) (e) (f)
20
15
10
05
00
OD
val
ue
1 3 5 7
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(g)
Rela
tive q
uant
ifica
tion
20
15
10
05
00OCN OSX RUNX2
lowast
lowast lowast
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(h)
Figure 3 Proliferation and osteogenic differentiation potential of aBMSCs on nHACPLA (a) SEM analysis showed that nHACPLA wassimilar to natural bone in terms of microstructure (b) After 3 days of culture the aBMSCs adhered to extended and connected with eachother and produced ECM on the nHACPLA surface The aBMSCs (cndashf) were spindle triangle or cube shaped with developed cytoplasmicextensions attached to the scaffold (g) The MTS results demonstrated that the aBMSCs were proliferative on days 1 3 5 and 7 after seedingonto nHACPLA (119899 = 6 mean plusmn SD) (h) Real-time PCR revealed that osteogenic induction for 7 days promoted aBMSC expression of OCNRunx2 and Osterix (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005 Magnification (ab) times100 SE (c) times500 SE (d) times150 k SE (e) times500 k SE (f) times100 k SE
and negative for hematopoietic and endothelial cell surfacemarkers including CD14 CD34 and HLA-DR (Figure 2(d))
32 Biocompatibility between aBMSCs and nHACPLA Theadherence and morphology of aBMSCs on nHACPLA wereobserved by SEM which revealed that the nHACPLAblocks without cells exhibited a hierarchical microstruc-ture (Figure 3(a)) After 3 days of culture the aBMSCsadhered to extended and connected with each other and
produced extracellular matrix (ECM) on the nHACPLAsurface (Figure 3(b)) The aBMSCs were spindle triangle orcube shaped with developed cytoplasmic extensions attachedto the scaffold (Figures 3(c)ndash3(f))
The proliferation of aBMSCs on nHACPLA was evalu-ated using theMTSmethod ondays 1 3 5 and 7 (Figure 3(g))Throughout the 7 days of culture the cell numbers increasedindicating that the nHACPLA had no negative effect onproliferation Compared with cells cultured in basic medium
Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

4 Stem Cells International
PCR System (Applied Biosystems Carlsbad CA USA) Thefollowing primer sets were used Runx2 GenBank Accessionnumber 860 F51015840-CGGAATGCCTCTGCTGTTATGAA-31015840R51015840-AGGATTTGTGAAGACGGTTATGG-31015840 Osterixnumber 121340 F51015840-CTCCTCCTGCGACTGCCCTAAT-31015840 R51015840-AGGTG CGAAGCCTTG CCATACA-31015840 OCNnumber 632 F51015840-GGAGGGCAGCGAGGTAGTGAAG-31015840 R51015840-GATGTGGTCA GCCAACTCGTCA-31015840 actinnumber 60 F51015840-TGCCCATCTA CGAGGGGTATG-31015840 R51015840-TCCTTAAT GTCACGCACGATTTC-31015840 The expressionsof the genes were normalized to the internal control b-actinmRNA levels Data were analyzed using the comparison Ct(2minusΔΔCt)methodThe specificity of single-target amplificationby each primer pair was confirmed bymelting curve analysis
29 Alkaline Phosphatase (ALP) OCN Calcium and Phos-phonium Content Assays aBMSCs on nHACPLA scaffoldswere cultured for 21 days in basic medium or osteogenicinduction medium at 15 times 104cm2 cells per graft Thesupernatants were collected at 3 time points days 7 14 and21 The ALP activity in the medium was assayed using RocheDiagnostics ALP kits on the cobas e602 platform (RocheDiagnosticsMannheimGermany) and calcium content andphosphonium content were assayed using Roche DiagnosticsCaP kits OCN activity was assayed using N-MID osteocal-cin kits based on electrochemiluminescence immunoassaytechniques All data were measured and analyzed on thecobas 8000 platform (Roche Diagnostics)
210 Genetic Stability Assay Reverse transcription PCR wasperformed to examine the gene expression of tumor suppres-sors and protooncogenes For this purpose RNAwas isolatedfrom aBMSCs cultured on flasks at passages 1 and 2 and fromaBMSCs cultured on nHACPLA scaffolds in basic mediumor osteogenic induction medium at passage 3 The primersequences were as follows p53 F51015840-CCTCACCATCAT-CACA CTGG-31015840 R51015840-TTATGGCGGGAGGTAGACTG-31015840c-myc F51015840-CTCCTGGCAAAAGGTCAG AG-31015840 R51015840-GGC-CTTTTCATTGTTTTCCA-31015840 ARF F51015840-TGGGTCCCA-GTCTGCA GTTA-31015840 R51015840-CTGCCCATCATCATGACCT-31015840 GAPDH F51015840-ACAGTCAGCC GCATCTTCTT-31015840 R51015840-ACGACCAAAT CCGTTGACTC-31015840
At the end of culture aBMSCs from three different patientsamples at passage 4 were subjected to karyotyping analysisThese aBMSCs were cultured on nHACPLA scaffolds inosteogenic induction medium followed by treatment with60 ngmL colcemid (Sigma) and harvesting with 025trypsinEDTA The cells were then collected by centrifu-gation and karyotyping analysis was performed using G-banding techniques in a clinical laboratory at the ChinesePLA General Hospital
211 Bone Regeneration in the Mandibular Defect Model Thebone-forming capacity of 20 different aBMSCs populationswas evaluated qualitatively in a New Zealand white rabbitsegmental critical-size mandibular defect model [18 19] Forthis purpose 30 female rabbits were housed in the laboratoryanimal center at the Chinese PLA General Hospital The
rabbits had weights of 250ndash300 kg All surgical proceduresand care followed Chinese PLA General Hospital ReviewBoard approval The rabbits were first intravenously anes-thetized with 2 pentobarbital sodium (30mgkg) The hairon the right of the rabbit mandible was then depilated Underaseptic conditions a 10mm incision was made along theupper edge of the rabbit mandible and the right buccal wasexposed A segmental defect (10 times 5 times 3mm) was prepared inthe alveolar bone of all rabbits using a surgical oscillating sawand sterile saline irrigation nHACPLA blocks withwithout5 times 106 aBMSCs were implanted in the segmental defectand the rabbits were assigned to five groups mandibulardefects were treated with nHACPLA nHACPLA + aBM-SCs or nHACPLA + preinduced aBMSCs (preinduced inosteogenic induction medium for 7 days) or with AB fromthe iliac bone as a positive control or untreated defect as anegative control
After eight weeks the samples were surgically removedand fixed Goldnerrsquos trichrome staining was used to examinebone regeneration at the defects All samples were analyzedby morphometric analysis using the Leica-Q Win 32 imageanalysis system Five sequential sections per implant wereselected and the type of tissue (mature bone-like or osteoid-like) was identified by an independent observer The extentof newly formed bone was indicated by the percentage of thenewly formed bone areas within a section An average valuewas then calculated for each implant and data were averagedacross all implants within each group
212 Assessment of Bone Regeneration byMicro-CT Thebonevolume and trabecular microarchitecture were monitoredusing a Quantum FX micro-CT Imaging System (CaliperUSA) at 70 kV and 114mA A total of 512 binary images wereobtained with a wide field of view (FOV) with scanning at36mm and a 45 120583m voxel size resolution The thresholdswere set at 1300 which was adequate to separate bone andnHAC using discrimination analysis The calculated bonevolume density (bone volumetotal volume) in this area ispresented as the percentage regeneration of the defect
213 Statistical Analysis All data are presented as the meanplusmn standard deviation Statistical analyses of the results wereperformed using SPSS 160 software Studentrsquos 119905-test was usedto study significant differences in the MTS PCR SEM ALPOCN and calcium and phosphonium content results One-way ANOVA and an unpaired 119905-test were used to studysignificant differences in the bone volume density and thepercentage of bone formation area between study groupsThesignificance threshold was set at 119901 lt 005
3 Results
31 Isolation and Characterization of aBMSCs We collectedalveolar bone marrow samples from 52 patients undergoingdental implant surgery Every dental implant was initiallystable (final torque gt 35Ncm) and no complications afterbone marrow collection were reported Postoperative 1- to 3-month cone-beam CT results revealed closely aligned dentalimplants and bone (Figure 1(e))
Stem Cells International 5
(a) (b) (c)
0
0
102
103
104
105 0
0
102
103
104
105
0
0
102
103
104
1050
0
102
103
104
105
0
0
102
103
104
105 0
0
102
103
104
105
CD44962
CD34217
CD90955
CD140866
CD106973
HLA-DR158
(d)
Figure 2 Characterization of human aBMSCs (a) The aBMSCs expressed STRO-1 a mesenchymal stromal cell marker Positive stainingof the cells with Alizarin red (b) or Oil red O (c) demonstrated the osteogenic and adipogenic differentiation potential of the aBMSCsMagnification times400 (d) The aBMSCs were positive for MSC markers including CD44 CD90 and CD106 and negative for hematopoieticand endothelial markers including CD14 CD34 and HLA-DR
The aBMSCs in 37 samples adhered to the culture surfaceand proliferated in vitroThe isolated aBMSCs formed single-cell-derived colonies and most of the cells retained theirfibroblastic spindle shape (Figure 1(f)) The aBMSCs wereexpanded in culture followed by characterization of cellsurfacemarkers by flow cytometry and immunofluorescenceImmunofluorescence analysis demonstrated that the cells
were STRO-1 positive (Figure 2(a)) To evaluate the invitro differentiation potential of the aBMSCs the cells wereinduced to differentiate along osteogenic and adipogeniclineages under specific culture conditions as revealed byAlizarin red (Figure 2(b)) and Oil red O (Figure 2(c))staining Flow cytometry revealed that the cultured cellswere homogenously positive for CD44 CD90 and CD106
6 Stem Cells International
(a) (b) (c)
(d) (e) (f)
20
15
10
05
00
OD
val
ue
1 3 5 7
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(g)
Rela
tive q
uant
ifica
tion
20
15
10
05
00OCN OSX RUNX2
lowast
lowast lowast
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(h)
Figure 3 Proliferation and osteogenic differentiation potential of aBMSCs on nHACPLA (a) SEM analysis showed that nHACPLA wassimilar to natural bone in terms of microstructure (b) After 3 days of culture the aBMSCs adhered to extended and connected with eachother and produced ECM on the nHACPLA surface The aBMSCs (cndashf) were spindle triangle or cube shaped with developed cytoplasmicextensions attached to the scaffold (g) The MTS results demonstrated that the aBMSCs were proliferative on days 1 3 5 and 7 after seedingonto nHACPLA (119899 = 6 mean plusmn SD) (h) Real-time PCR revealed that osteogenic induction for 7 days promoted aBMSC expression of OCNRunx2 and Osterix (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005 Magnification (ab) times100 SE (c) times500 SE (d) times150 k SE (e) times500 k SE (f) times100 k SE
and negative for hematopoietic and endothelial cell surfacemarkers including CD14 CD34 and HLA-DR (Figure 2(d))
32 Biocompatibility between aBMSCs and nHACPLA Theadherence and morphology of aBMSCs on nHACPLA wereobserved by SEM which revealed that the nHACPLAblocks without cells exhibited a hierarchical microstruc-ture (Figure 3(a)) After 3 days of culture the aBMSCsadhered to extended and connected with each other and
produced extracellular matrix (ECM) on the nHACPLAsurface (Figure 3(b)) The aBMSCs were spindle triangle orcube shaped with developed cytoplasmic extensions attachedto the scaffold (Figures 3(c)ndash3(f))
The proliferation of aBMSCs on nHACPLA was evalu-ated using theMTSmethod ondays 1 3 5 and 7 (Figure 3(g))Throughout the 7 days of culture the cell numbers increasedindicating that the nHACPLA had no negative effect onproliferation Compared with cells cultured in basic medium
Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Stem Cells International 5
(a) (b) (c)
0
0
102
103
104
105 0
0
102
103
104
105
0
0
102
103
104
1050
0
102
103
104
105
0
0
102
103
104
105 0
0
102
103
104
105
CD44962
CD34217
CD90955
CD140866
CD106973
HLA-DR158
(d)
Figure 2 Characterization of human aBMSCs (a) The aBMSCs expressed STRO-1 a mesenchymal stromal cell marker Positive stainingof the cells with Alizarin red (b) or Oil red O (c) demonstrated the osteogenic and adipogenic differentiation potential of the aBMSCsMagnification times400 (d) The aBMSCs were positive for MSC markers including CD44 CD90 and CD106 and negative for hematopoieticand endothelial markers including CD14 CD34 and HLA-DR
The aBMSCs in 37 samples adhered to the culture surfaceand proliferated in vitroThe isolated aBMSCs formed single-cell-derived colonies and most of the cells retained theirfibroblastic spindle shape (Figure 1(f)) The aBMSCs wereexpanded in culture followed by characterization of cellsurfacemarkers by flow cytometry and immunofluorescenceImmunofluorescence analysis demonstrated that the cells
were STRO-1 positive (Figure 2(a)) To evaluate the invitro differentiation potential of the aBMSCs the cells wereinduced to differentiate along osteogenic and adipogeniclineages under specific culture conditions as revealed byAlizarin red (Figure 2(b)) and Oil red O (Figure 2(c))staining Flow cytometry revealed that the cultured cellswere homogenously positive for CD44 CD90 and CD106
6 Stem Cells International
(a) (b) (c)
(d) (e) (f)
20
15
10
05
00
OD
val
ue
1 3 5 7
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(g)
Rela
tive q
uant
ifica
tion
20
15
10
05
00OCN OSX RUNX2
lowast
lowast lowast
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(h)
Figure 3 Proliferation and osteogenic differentiation potential of aBMSCs on nHACPLA (a) SEM analysis showed that nHACPLA wassimilar to natural bone in terms of microstructure (b) After 3 days of culture the aBMSCs adhered to extended and connected with eachother and produced ECM on the nHACPLA surface The aBMSCs (cndashf) were spindle triangle or cube shaped with developed cytoplasmicextensions attached to the scaffold (g) The MTS results demonstrated that the aBMSCs were proliferative on days 1 3 5 and 7 after seedingonto nHACPLA (119899 = 6 mean plusmn SD) (h) Real-time PCR revealed that osteogenic induction for 7 days promoted aBMSC expression of OCNRunx2 and Osterix (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005 Magnification (ab) times100 SE (c) times500 SE (d) times150 k SE (e) times500 k SE (f) times100 k SE
and negative for hematopoietic and endothelial cell surfacemarkers including CD14 CD34 and HLA-DR (Figure 2(d))
32 Biocompatibility between aBMSCs and nHACPLA Theadherence and morphology of aBMSCs on nHACPLA wereobserved by SEM which revealed that the nHACPLAblocks without cells exhibited a hierarchical microstruc-ture (Figure 3(a)) After 3 days of culture the aBMSCsadhered to extended and connected with each other and
produced extracellular matrix (ECM) on the nHACPLAsurface (Figure 3(b)) The aBMSCs were spindle triangle orcube shaped with developed cytoplasmic extensions attachedto the scaffold (Figures 3(c)ndash3(f))
The proliferation of aBMSCs on nHACPLA was evalu-ated using theMTSmethod ondays 1 3 5 and 7 (Figure 3(g))Throughout the 7 days of culture the cell numbers increasedindicating that the nHACPLA had no negative effect onproliferation Compared with cells cultured in basic medium
Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

6 Stem Cells International
(a) (b) (c)
(d) (e) (f)
20
15
10
05
00
OD
val
ue
1 3 5 7
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(g)
Rela
tive q
uant
ifica
tion
20
15
10
05
00OCN OSX RUNX2
lowast
lowast lowast
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(h)
Figure 3 Proliferation and osteogenic differentiation potential of aBMSCs on nHACPLA (a) SEM analysis showed that nHACPLA wassimilar to natural bone in terms of microstructure (b) After 3 days of culture the aBMSCs adhered to extended and connected with eachother and produced ECM on the nHACPLA surface The aBMSCs (cndashf) were spindle triangle or cube shaped with developed cytoplasmicextensions attached to the scaffold (g) The MTS results demonstrated that the aBMSCs were proliferative on days 1 3 5 and 7 after seedingonto nHACPLA (119899 = 6 mean plusmn SD) (h) Real-time PCR revealed that osteogenic induction for 7 days promoted aBMSC expression of OCNRunx2 and Osterix (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005 Magnification (ab) times100 SE (c) times500 SE (d) times150 k SE (e) times500 k SE (f) times100 k SE
and negative for hematopoietic and endothelial cell surfacemarkers including CD14 CD34 and HLA-DR (Figure 2(d))
32 Biocompatibility between aBMSCs and nHACPLA Theadherence and morphology of aBMSCs on nHACPLA wereobserved by SEM which revealed that the nHACPLAblocks without cells exhibited a hierarchical microstruc-ture (Figure 3(a)) After 3 days of culture the aBMSCsadhered to extended and connected with each other and
produced extracellular matrix (ECM) on the nHACPLAsurface (Figure 3(b)) The aBMSCs were spindle triangle orcube shaped with developed cytoplasmic extensions attachedto the scaffold (Figures 3(c)ndash3(f))
The proliferation of aBMSCs on nHACPLA was evalu-ated using theMTSmethod ondays 1 3 5 and 7 (Figure 3(g))Throughout the 7 days of culture the cell numbers increasedindicating that the nHACPLA had no negative effect onproliferation Compared with cells cultured in basic medium
Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Stem Cells International 7
ALP
(mm
olL
)
7 14 21
Times (day)
lowast
lowast
0
5
10
15
nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
(a)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
0
1
2
3
OCN
(mm
olL
)
lowast
lowast
(b)
0
1
2
3
4
Ca (m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
lowastlowast
(c)
0
5
10
15
P(m
mol
L)
7 14 21
Times (day)nHACPLA + aBMSCsnHACPLA + preinduced aBMSCs
lowast
(d)
Figure 4 Effect of osteogenic induction on the ALP activity (a) OCN content (b) calcium content (c) and phosphonium content (d) ofaBMSCs cultured on nHACPLA (119899 = 6 mean plusmn SD) lowastCompared with nHACPLA + aBMSCs Differences are significant at 119901 lt 005
(nHACPLA + aBMSCs group) the number of aBMSCson nHACPLA decreased in the nHACPLA + preinducedaBMSCs group but the difference was not significant (119901 gt005)
33 Osteogenic Capability of aBMSCs on nHACPLA To con-firm their osteogenic potential aBMSCs on nHACPLAwerecultured in basic medium or osteogenic induction mediumfor 7 days followed by the evaluation of osteogenesis-related genes by quantitative real-time PCR The PCR resultsdemonstrated that osteogenic inductive treatment promotedexpression of the osteogenesis-related genes OCN Runx2and Osterix in the BMSCs (Figure 3(h))
To investigate the osteogenic capability of aBMSCs onnHACPLA the ALP activity calcium and phosphoniumcontent and OCN content in the culture supernatant wereassayed at days 7 14 and 21 The aBMSCs and nHACPLAconstructs were cultured in basic medium or osteogenic
induction medium for this purpose During the 28 daysof culture the ALP activity and OCN and phosphoniumcontent in both groups increased with culture time but thecalcium content decreased However the ALP activity andOCN and phosphonium content were significantly higherin the nHACPLA + preinduced aBMSCs group than innHACPLA + aBMSCs group at day 21 (Figure 4) Althoughthe calcium content in both groups declined the contentin the nHACPLA + preinduced aBMSCs group was alwayssignificantly lower
34 Genetic Stability Assessment To evaluate transforma-tional alterations in gene expression the levels of the tumorsuppressor genes p53 and ARF and the protooncogene c-mycwere measured (119899 = 6) However no significant changeswere observed over time or upon osteogenic induction(Figure 5(a))
8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

8 Stem Cells International
ARF
c-myc
GAPDH
p53
Passage 1 Passage 2 Passage 3 Induced
(a)
1 2 3 4 5
6 7 8 9 10 11 12 X
13 14 15 16 17 18
19 20 21 22 Y
(b)
Figure 5 Genetic stability evaluation (a) The expression levels of p53 ARF and c-myc in aBMSCs were unchanged over time and underosteogenic induction (The term ldquoinducedrdquo denotes aBMSCs at passage 3 that were cultured on nHACPLA scaffolds in osteogenic inductionmedium) (b) aBMSCs at passage 4 that were cultured on nHACPLA in osteogenic induction medium exhibited a normal karyotype
After culture on nHACPLA scaffolds in osteogenicinductionmedium for 21 days aBMSCs at passage 4 exhibiteda normal diploid karyotype (119899 = 6) Chromosome structuralabnormalities such as inversion deletion translocation andrings were not observed by karyotyping analysis of G-banding (Figure 5(b))
35 Bone Regeneration in a Mandibular Defect Model In thecritical-size mandibular defect rabbit model the mandiblewas harvested for histological analyses at 8 weeks In thenHACPLA and the nHACPLA + aBMSCs groups themandibular defects were filled with abundant red-stainedosteoid tissue and some green-stained newly formed bone(Figures 6(a) and 6(b)) and many osteoclasts were observedin the newly formed osteoid tissue Meanwhile the defects inthe nHACPLA + preinduced aBMSCs group were filled witha large amount of mature thickened bone (Figure 6(c)) andosteoblasts lined the surface of the newly formed bone In theAB group there were areas of autogenous grafted bone as wellas areas of new bone regeneration (Figure 6(d)) In differentmaturation stages the autologous bone and newly formedbone exhibited different trabecular arrangements Little boneregeneration was observed in the untreated defect groupwhich served as the negative control
A total of 68 slides from the different groups werequantified by morphological analysis The extent of newlyformed mature bone and osteoid tissue was indicated by thepercentage of total bone formation area within the sectionthis percentage was averaged across all slides within eachgroup The percentages of the osteoid tissue formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs and AB groups were 235 plusmn 33 156 plusmn12 79 plusmn 19 and 92 plusmn 11 respectively The percentages ofmature bone formation area in the nHACPLA nHACPLA+aBMSCs nHACPLA + preinduced aBMSCs and AB groups
were 32 plusmn 12 192 plusmn 13 412 plusmn 24 and 432 plusmn 27respectively The percentages of total bone formation areain the nHACPLA nHACPLA + aBMSCs nHACPLA +preinduced aBMSCs andABgroupswere 267plusmn45 348plusmn25491 plusmn 43 and 522 plusmn 38 respectively
Histomorphometric measurements revealed significantdifferences in bone formation (Figure 7(F)) The nHACPLAgroup had the lowest percentage of total bone formation areaof the five implanted groups and differed significantly fromthe other groups (119901 lt 005) Total bone formation in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) The maximal percentage of total bone formationarea was observed in the AB group However there were nosignificant differences between the nHACPLA + preinducedaBMSCs and the AB groups (119901 gt 005)
Regeneration of the mandibular defects was evaluatedusingmicro-CT In the 3-dimensional volume reconstructionof the images the bone defect in the untreated defectgroup was unfilled (Figure 7(A)) For defects filled withan nHACPLA scaffold new bone formation in the openscaffold pores with incomplete healing of the defect wasobserved (Figure 7(B)) For defects filled with nHACPLA +aBMSCs the defect surface was healed with a thin corticalshell bridge (Figure 7(C)) For defects filled with nHACPLA+ preinduced aBMSCs the defect surface was also completelyhealed with a thick cortical shell bridge (Figure 7(D)) In theAB group the defects healedwell and the iliac graft block andmandibular bone could not be distinguished (Figure 7(E))
To quantify newbone formation the bone volumedensityin the defect is presented as the percentage regeneration ofthe defect The bone volume densities in the nHACPLAnHACPLA + aBMSCs nHACPLA + preinduced aBMSCsand AB groups and the untreated defect group were 251 plusmn
Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Stem Cells International 9
OS
OSNB
20120583m
(a)
NB
OS
NB
20120583m
(b)
NB
NB
20120583m
(c)
NB OS
AB
20120583m
(d)
Figure 6 Bone regeneration in a rabbit critical-size mandibular defect model stained with Goldnerrsquos trichrome (a) The defects in thenHACPLA group were filled with abundant red-stained osteoid tissue and some green-stained newly formed bone (b) The defects in thenHACPLA + aBMSCs group were filled with more newly formed trabeculae (c)The defects in the nHACPLA + preinduced aBMSCs groupwere filled with a large amount of mature thickened bone (d)TheAB group exhibited areas of newly formed bone osteoid tissue osteoblasticseams and residual bone graft Magnification times400 NB new mature bone AB autogenous bone OS osteoid tissue
45 332 plusmn 34 478 plusmn 42 554 plusmn 39 and 585 plusmn 38respectively (Figure 7(G)) The bone volume density in thenHACPLA+ aBMSCs groupwas significantly higher than inthe nHACPLA group (119901 lt 005) but significantly lower thanin the nHACPLA + preinduced aBMSCs and the AB groups(119901 lt 005) There were no significant differences between thenHACPLA + preinduced aBMSCs and the AB groups (119901 gt005) indicating that new bone formation was significantlyimproved by the nHACPLA + preinduced aBMSCs
4 Discussion
As a promising alternative approach for the treatment ofbone defects bone tissue engineering creates a bone graftingmaterial with osteogenic osteoinductive and osteoconduc-tive properties These events are also essential for optimalbone healingwhen a combination of BMSCs and biomaterialsis to be used to treat periodontal bone defects In vitrostudies of BMSCs often involve cells derived from the tibiaof animals including mice and rats When human skeletalprogenitor cells are studied most bone grafting proceduresperformed for craniofacial applications use cells derived fromthe mesodermal lineage (eg the fibula iliac crest andribs) Recently several scholars have described the isolationof BMSCs from the marrow of maxillofacial bones anddemonstrated that these cells share the basic characteristics ofMSCs [10 16] In the same individuals maxillofacial-derivedBMSCs were found to have greater osteogenic potentialsthan iliac crest-derived BMSCs [20] In previous studies
we also found that osteogenic differentiation capacity ofalveolar BMSCswas higher than that of femoral BMSCs in themiddle-aged and old group [21] These reports indicate theBMSCs from maxillofacial bones with some characteristicsthat may be beneficial for treating maxillofacial bone defectsNevertheless inmost published studies alveolar BMSCs havenot been used in critical-size mandibular bone defect model
In this study we describe a convenient and minimallyinvasive process for craniofacial BMSC isolation and furtherdemonstrate that a combination of aBMSCs after osteogenicinduction and nHACPLA could effectively restoremandibu-lar defects It would be an advantage to use aBMSCs via thisprocess thereby reducing donor-site morbidity and residualpain related to bone harvesting from for example the iliaccrest
At the histological level defect repair in the craniofacialskeleton is indistinguishable from appendicular bone repairboth defect sites are vascularized following trauma bothbecome populated by osteoblast progenitor cells and bothundergo bony matrix remodeling within a similar timeframe However cellular and molecular analyses belie thishistological equivalency In particular Hox expression statusas well as embryonic origin has an influence on the fate ofskeletal progenitor cells in the regenerative context Leuchtet al found that initially mandibular skeletal progenitorcells are Hox negative but that they adopt a Hoxa11-positiveprofile when transplanted into a tibial defect Converselytibial skeletal progenitor cells are Hox positive and maintainthis Hox status even when transplanted into a Hox-negative
10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

10 Stem Cells International
(a) (e)(c) (d)(b)
A E
(A) (B)
(F) (G)
(C) (D) (E)
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
Unt
reat
ed g
roup
HAC
PLA
HAC
PLA
+aB
MSC
HAC
PLA
+pr
eind
uced
aBM
SC
Auto
geno
us b
one
0
20
40
60
80
Bone
vol
ume d
ensit
y (
)
lowast
lowast
lowast
0
20
40
60
Bone
form
atio
n ar
ea (
)
OsteoidNew mature bonesTotal bone
998771
998771998771
998771998771998771
998771998771998771
lowast
lowastlowast
lowastlowastlowast
lowastlowastlowast
998779
998779998779
998779998779998779 998779
998779998779
Figure 7 Micro-CT images of the mandibular defects at 8 weeks after implantation (A a) The critical-size bone defect in the untreatedgroup was unfilled (B b) For defects filled with an nHACPLA scaffold new bone formation in the open scaffold pores with incompletehealing on the surface of the defect was observed (C c) The defect surface was healed with a thin cortical shell bridge in the nHACPLA +aBMSCs group (D d) The defect surface was completely healed with a thick cortical shell bridge in the nHACPLA + preinduced aBMSCsgroup (E e) In the AB group the defect healed well and the iliac graft block and mandibular bone could not be distinguished (The redboxes represent the defect area in the mandible and the blue arrow indicates an incomplete cortical shell) (F) The percentages of osteoidtissue formation mature bone formation and total bone formation were determined by histomorphometric measurements Differences aresignificant at 119901 lt 005 Groups with the same symbol (lowast 998771 998779) were not significantly different (G) The bone volume density in micro-CT ispresented as the percentage regeneration of the defect Differences are significant at 119901 lt 005
mandibular defect [15]This mismatch between the Hox geneexpression statuses of host and donor cells is correlated with adisruption in bone regeneration such that the grafted cells failto differentiate into osteoblasts [22]When iliac crest-derivedBMSCs are placed in a mandibular defect these mesoderm-derived progenitor cells differentiate into chondrocytes [23]
Conversely craniofacial bone-derived BMSCs can integrateinto and contribute to bony regeneration in a mandibulardefect
In the present study we isolated and characterized aBM-SCs which fulfill the criteria of the International Societyfor Cellular Therapy including fibroblast-like morphology
Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Stem Cells International 11
expression of surfacemarkers and a capacity formultilineagedifferentiation [24] Although the maintenance of stemnessis difficult to achieve in ex vivo culture this profile suggeststhat cells collected from alveolar bone resemble immaturemesenchymal cells We also determined that the aBMSCswere STRO-1 positive STRO-1 which recognizes only clono-genic and highly osteogenic progenitors is expressed bystromal elements in the bone marrow [25] Additionally weevaluated the osteogenic potential of the aBMSCs Runx2andOsterix are essential transcription factors for osteoblasticdifferentiation and skeletal morphogenesis and OCN is amajor noncollagenous protein specific to bone and the mostrecently identified osteogenic expression marker
The cellular state under 2D and 3D cell culture condi-tions may vary considerably [26] Accordingly the prolif-eration and osteogenic capabilities of the aBMSCs on the3D porous nHACPLA scaffold were further evaluated ThenHACPLA scaffold was formed from new mineralized col-lagen consisting of a combination of collagen fibrils and PLAattached to nanohydroxyapatite by a self-assembly methodThe microstructure of this composite was a mineralizedcollagen fiber bundle similar to the hierarchical structure ofnatural bone [27] We have previously demonstrated that thiscomposite has good biocompatibility and osteoconductivitysuggesting its potential for hard tissue repair [18] The resultsof the current study further confirmed that nHACPLA pro-vides a suitable environment for aBMSC adhesion prolifera-tion and differentiationThe upregulation of both osteogenicgene expression and protein expression suggests that theosteogenic potential of aBMSCs on nHACPLAwas activatedby the osteogenic induction medium
In this study a localized mandibular defect model wasused to characterize the osteogenic differentiation of thenHACPLA + aBMSCs construct in vivo Micro-CT andhistomorphometric analyses further confirmed the capabilityof this method to repair bone defects In the rabbit mandiblea defect diameter greater than 5mm has been reported to bea critical size that prevents spontaneous healing [19] In thepresent study after 8 weeks of implantation histological anal-ysis demonstrated that the untreated group exhibited no boneformation and that the nHACPLAgroup had abundant engi-neered osteoid tissue and some newly formed bone Theseresults indicated that a critical-size defect was successfullyestablished and that nHACPLA can be used as a potentialscaffold for mandibular bone regeneration Furthermore thenHACPLA + aBMSCs group had significantly greater boneformation than the nHACPLA group didThese results onceagain confirmed that the structure and composition of thenHACPLA had good biocompatibility and promoted cellproliferation and osteogenic differentiation The ECM andother factors in the bone defect environment played a key rolein this osteogenic differentiation of the aBMSCs Specificallyfor defects filled with nHACPLA + preinduced aBMSCsa large amount of mature thickened bone was observed inthe morphometric analysis and the defect surface exhibitedcomplete healing with a thick cortical shell bridge in CTimages These results demonstrated that the nHACPLA +aBMSCs preinduced in osteogenic induction medium didindeed exhibit enhanced initial bone formation in vivoThese
results also indicated that factors from defects are insufficientto stimulate aBMSCs to undergo osteogenic differentia-tion To achieve improved therapeutic effects regulating thedegree of aBMSCsrsquo osteogenic differentiation is desirableTheselected inducermay include osteoblasts that have undergoneosteogenic preinduction in vitro Osteoblast-secreted factorscan promote the proliferation and osteogenic differentiationof BMSCs via the VEGFheme-oxygenase-1 pathway [28]To verify that the tissue-engineered bone generated fromnHACPLA + preinduced aBMSCs is a valid alternative forthe reconstruction of mandibular bone defects a positive-control gold-standard fresh autogenous iliac bone graft wasalso tested in this study Quantitative histomorphometric andmicro-CT analyses demonstrated that the tissue-engineeredbone was similar to that derived from the gold-standardmethod
The effects of the nHACPLA + preinduced aBMSCsmethod on bone defect repair are similar to those of theautologous bone method but with less trauma Thereforethe method presented here needs to be considered carefullyfor clinical applications Cone-beam CT also confirmed thatthe method does not affect the osseointegration of dentalimplants From a purely technical perspective aBMSC collec-tion offers advantages over collection fromother sites becausethe cells are passed through the mucous membrane withoutdamaging the skin which avoids the need for general anes-thesia and effectively reduces patient discomfort Moreoverthe cells can be easily obtained during routine dental surgerysuch as dental implant surgery wisdom tooth extractionand tooth crown-lengthening measures The selection ofsurgical methods depends on the surgeonrsquos familiarity withthe anatomic region but most maxillofacial surgeons anddentists feel confident about extracting bone marrow fromalveolar bones
It is noteworthy that although complete absence ofteratoma formation was observed in this study it is onlya speculation whether some aBMSCs still survive in vivoor are killed in xenogeneic hosts Several studies havesuggested that the stem cells could suppress immuneresponses through immune-privileged immunosuppressiveor tolerance-inducing methods [29 30] Others have sug-gested that the functional improvements after implantationof xenogeneic stem cells are only caused by paracrine effectsrather than by engraftment [31] Thus further studies aboutimmune mechanisms will be necessary to correctly interpretthe results of animal models and for future translation intoclinical practice
Another safety consideration for tissue engineeringstrategies is genetic stability in ex vivo cell culture Inthe present study aBMSCs were expanded passaged andosteogenically induced Following long-term cell culture theresults of karyotyping tumor suppressor and protooncogeneanalyses were unchanged These results are in agreementwith those of Poloni et al who observed that humanadipocytes dedifferentiated into endothelial cells and didnot undergo transformational changes [32] Our results thusdemonstrated that genetic instability does not occur amongaBMSCs cultured on nHACPLA in osteogenic inductionmedium
12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

12 Stem Cells International
5 Conclusion
The key parameter of bone reconstruction in bone tissueengineering is the selection of favorable seed cells bio-materials and an osteogenic inducer changes in any ofthese three factors will affect osteogenesis The present studyovercame the difficulties of isolating human craniofacialBMSCs and demonstrated the bone regeneration potentialof an innovative seed cell type namely aBMSCs withoutviral gene deliveryThese findings also demonstrated that thismethod of applying nHACPLA + aBMSCs with osteogenicpreinduction is a valid alternative for the correction ofmandibular bone defects This study is an important stepin the clinical application of human craniofacial BMSCsalthough additional studies will be necessary to determinethe effects of immunity on human autologous aBMSCs afterpreinduction in vitro
Competing Interests
No competing financial interests exist
Authorsrsquo Contributions
XingWang and Helin Xing contributed equally to this paper
Acknowledgments
This study was supported by National Natural Science Foun-dation of China (81271180) the National Natural ScienceDirector Foundation of China (81150019) Beijing NaturalScience Foundation (7164297) and the Open Research FundProgram of the State Key Laboratory of Low-DimensionalQuantum Physics (20120908) The authors are also gratefulto the staff and faculty of Institute of Stomatology ChinesePeople Liberation Army General Hospital
References
[1] S Marthy and M Richter ldquoHuman immunodeficiency virusactivity in rib allograftsrdquo Journal of Oral and MaxillofacialSurgery vol 56 no 4 pp 474ndash476 1998
[2] J-W Jang J-H Yun K-I Lee et al ldquoOsteoinductive activityof biphasic calcium phosphate with different rhBMP-2 dosesin ratsrdquo Oral Surgery Oral Medicine Oral Pathology and OralRadiology vol 113 no 4 pp 480ndash487 2012
[3] M F Pittenger A M Mackay S C Beck et al ldquoMultilineagepotential of adult human mesenchymal stem cellsrdquo Science vol284 no 5411 pp 143ndash147 1999
[4] G Ren L Zhang X Zhao et al ldquoMesenchymal stem cell-mediated immunosuppression occurs via concerted action ofchemokines and nitric oxiderdquo Cell Stem Cell vol 2 no 2 pp141ndash150 2008
[5] G Ciapetti L Ambrosio GMarletta N Baldini and A GiuntildquoHuman bone marrow stromal cells in vitro expansion anddifferentiation for bone engineeringrdquo Biomaterials vol 27 no36 pp 6150ndash6160 2006
[6] W-K Min J-S Bae B-C Park et al ldquoProliferation andosteoblastic differentiation of bone marrow stem cells compar-ison of vertebral body and iliac crestrdquo European Spine Journalvol 19 no 10 pp 1753ndash1760 2010
[7] D Kaigler G Pagni C H Park et al ldquoStem cell therapyfor craniofacial bone regeneration a randomized controlledfeasibility trialrdquo Cell Transplantation vol 22 no 5 pp 767ndash7772013
[8] G J Meijer J D de Bruijn R Koole and C A van BlitterswijkldquoCell based bone tissue engineering in jaw defectsrdquo Biomateri-als vol 29 no 21 pp 3053ndash3061 2008
[9] D R Reissmann B Dietze M Vogeler R Schmelzeisen andG Heydecke ldquoImpact of donor site for bone graft harvestingfor dental implants on health-related and oral health-relatedquality of liferdquo Clinical Oral Implants Research vol 24 no 6pp 698ndash705 2013
[10] S Mason S A Tarle W Osibin Y Kinfu and D KaiglerldquoStandardization and safety of alveolar bone-derived stem cellisolationrdquo Journal of Dental Research vol 93 no 1 pp 55ndash612014
[11] E J Mackie Y A Ahmed L Tatarczuch K-S Chen and MMirams ldquoEndochondral ossification how cartilage is convertedinto bone in the developing skeletonrdquo International Journal ofBiochemistry and Cell Biology vol 40 no 1 pp 46ndash62 2008
[12] Y Chai X Jiang Y Ito et al ldquoFate of the mammalian cranialneural crest during tooth and mandibular morphogenesisrdquoDevelopment vol 127 no 8 pp 1671ndash1679 2000
[13] I T Jackson G Helden and R Marx ldquoSkull bone grafts inmaxillofacial and craniofacial surgeryrdquo Journal of Oral andMaxillofacial Surgery vol 44 no 12 pp 949ndash955 1986
[14] P D Sawin V C Traynelis and A H Menezes ldquoA comparativeanalysis of fusion rates and donor-site morbidity for autogeneicrib and iliac crest bone grafts in posterior cervical fusionsrdquoJournal of Neurosurgery vol 88 no 2 pp 255ndash265 1998
[15] P Leucht J-B Kim R Amasha AW James S Girod and J AHelms ldquoEmbryonic origin andHox status determine progenitorcell fate during adult bone regenerationrdquoDevelopment vol 135no 17 pp 2845ndash2854 2008
[16] TMatsubara K Suardita M Ishii et al ldquoAlveolar bonemarrowas a cell source for regenerative medicine differences betweenalveolar and iliac bone marrow stromal cellsrdquo Journal of Boneand Mineral Research vol 20 no 3 pp 399ndash409 2005
[17] L L E L L Xu X Wu et al ldquoThe interactions between rat-adipose-derived stromal cells recombinant human bone mor-phogenetic protein-2 and beta-tricalcium phosphate play animportant role in bone tissue engineeringrdquo Tissue EngineeringPart A vol 16 no 9 pp 2927ndash2940 2010
[18] H-C Liu D-S Wang F Su et al ldquoReconstruction ofalveolar bone defects using bone morphogenetic protein 2mediated rabbit dental pulp stem cells seeded on nano-hydroxyapatitecollagen poly(l-lactide)rdquo Tissue Engineering Avol 17 no 19-20 pp 2417ndash2433 2011
[19] V Thomaidis K Kazakos D N Lyras et al ldquoComparativestudy of 5 different membranes for guided bone regeneration ofrabbit mandibular defects beyond critical sizerdquoMedical ScienceMonitor vol 14 no 4 pp BR67ndashBR73 2008
[20] S O Akintoye T Lam S Shi J Brahim M T Collins andP G Robey ldquoSkeletal site-specific characterization of orofacialand iliac crest human bone marrow stromal cells in sameindividualsrdquo Bone vol 38 no 6 pp 758ndash768 2006
Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Stem Cells International 13
[21] X Wang X Zou J Zhao et al ldquoSite-specific characteristics ofbone marrow mesenchymal stromal cells modify the effect ofaging on the skeletonrdquo Rejuvenation Research 2016
[22] S Creuzet G Couly C Vincent and N M Le DouarinldquoNegative effect of Hox gene expression on the development ofthe neural crest-derived facial skeletonrdquo Development vol 129no 18 pp 4301ndash4313 2002
[23] A DrsquoAddona and H Nowzari ldquoIntramembranous autogenousosseous transplants in aesthetic treatment of alveolar atrophyrdquoPeriodontology 2000 vol 27 no 1 pp 148ndash161 2001
[24] M Dominici K Le Blanc I Mueller et al ldquoMinimal crite-ria for defining multipotent mesenchymal stromal cells TheInternational Society for Cellular Therapy position statementrdquoCytotherapy vol 8 no 4 pp 315ndash317 2006
[25] P J Simmons and B Torok-Storb ldquoIdentification of stromalcell precursors in human bone marrow by a novel monoclonalantibody STRO-1rdquo Blood vol 78 no 1 pp 55ndash62 1991
[26] P-C Tseng T-H Young T-M Wang H-W Peng S-M Houand M-L Yen ldquoSpontaneous osteogenesis of MSCs culturedon 3Dmicrocarriers through alteration of cytoskeletal tensionrdquoBiomaterials vol 33 no 2 pp 556ndash564 2012
[27] S Liao K Tamura Y Zhu et al ldquoHuman neutrophils reactionto the biodegraded nano-hydroxyapatitecollagen and nano-hydroxyapatitecollagenpoly(L-lactic acid) compositesrdquo Jour-nal of Biomedical Materials Research A vol 76 no 4 pp 820ndash825 2006
[28] L-F Zhang J Qi G Zuo et al ldquoOsteoblast-secreted factorspromote proliferation and osteogenic differentiation of bonemarrow stromal cells via VEGFheme-oxygenase-1 pathwayrdquoPLoS ONE vol 9 no 6 Article ID e99946 2014
[29] L LiM L Baroja AMajumdar et al ldquoHuman embryonic stemcells possess immune-privileged propertiesrdquo STEMCELLS vol22 no 4 pp 448ndash456 2004
[30] C A Koch P Geraldes and J L Platt ldquoImmunosuppression byembryonic stem cellsrdquo Stem Cells vol 26 no 1 pp 89ndash98 2008
[31] R Dressel ldquoEffects of histocompatibility and host immuneresponses on the tumorigenicity of pluripotent stem cellsrdquoSeminars in Immunopathology vol 33 no 6 pp 573ndash591 2011
[32] A Poloni G Maurizi S Anastasi et al ldquoPlasticity of humandedifferentiated adipocytes toward endothelial cellsrdquo Experi-mental Hematology vol 43 no 2 pp 137ndash146 2015
Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology

Submit your manuscripts athttpwwwhindawicom
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation httpwwwhindawicom
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttpwwwhindawicom
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
Microbiology