Embed Size (px)
Citation preview

Research Introduction
9.17.13

• Altered metabolism in polycystic kidney
disease
• Telomerase activity in polycystic kidney disease cells

Autosomal dominant polycystic kidney disease • ADPKD is the most common inherited kidney disease.
Incidence 1 in 500 to 1 in 1000 worldwide. 600,000 patients in US
• Third most common single cause of ESRD world wide
and accounts for 5-10% of ESRD in US • ADPKD is caused by mutations of either PKD1 gene
(around 85% of cases) on chromosome 16 or the PKD2 gene (around 15% of cases) on chromosome 4
• There is evidence for a two hit mechanisms( germ line and somatic inactivation of two PKD alleles) explaining the focal development of renal and hepatic cysts
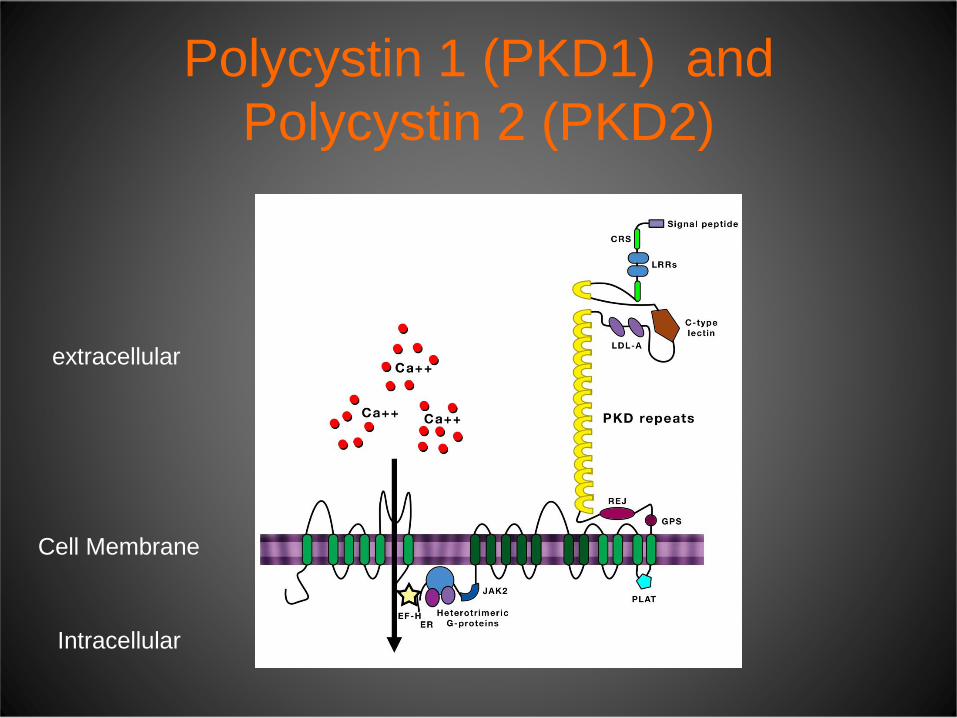
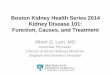
Polycystin 1 (PKD1) and Polycystin 2 (PKD2)
Intracellular
Cell Membrane
extracellular

Polycystins localize to cilia and are activated by mechanosensation
tubular lumen
Normal PKD1 or PKD2 Mutant
x
x x
PC1 PC2 PC1
PC2

Pathways up-regulated or down regulated in polycystic kidney disease

Altered Metabolism and Cancer

Altered Metabolism and Cancer
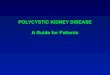
Resting cell Proliferating cells

Metabolism in proliferating cancer cells
Glucose Glutamine
Macro molecules
ATP
Proteins Lipids Nucleotides

Altered metabolism and Cancer

Glutamine metabolism and Cancer

Altered metabolism and Cancer
Do ADPKD cells behave like cancer cells?

Many of the signaling pathways activated in cancer cells are also active in ADPKD cells

Cells used for studies
1. NHK cells. Primary normal human kidney distal tubular epithelial cells isolated from nephrectomies.
2. ADPKD cells. Primary human ADPKD cells that are mutant for PKD1.
ADPKD cells Isolate cyst lining epithelial cells
PKD-/-
PKD+/-

Upregulation of PKM2 isoform in PKD cells
glutaminase
PKM2
actin
APKD NHK APKD NHK
PKM1

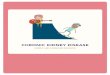
Glutaminase 1 is upregulated in ADPKD cells by cAMP
Forskolin/cAMP APKD APKD APKD NHK NHK NHK
Forskolin/cAMP
anti-glutaminase KGA anti-glutaminase GAC
glutaminase 1 KGA
glutaminase 1 GAC

Inhibition of glutaminase 1 blocks cyst formation by PDK-/- cells in cell culture

Inhibition of glutaminase 1 lowers ATP levels in ADPKD but not NHK cells

Alpha Ketoglutarate- most abundant metabolite in the urine of rat model of PKD
Nephrology 2012

Assess whether cyst formation in PKD-/- mice (knockout) is inhibited in by gls1 inhibitor
BPTES
Pkhd1-Cre; PKDfl/-
BPTES postnatal day 10-24
Vehicle control postnatal day 10-24
Sacrifice day 24

Treatment with BPTES slows cyst growth in PKD1 knockout model

Amino acids and glutaminolysis regulate mTORC1
Glutamine Glutamate Ketoglutarate GLS GDH
Leucine
mTORC1 Cell
proliferation
PS6K PS6
Cell 2012

Glutaminolysis regulates mTORC1
Cell 2012

Sirolimus and kidney growth in Autosomal Dominant Polycystic Kidney Disease
• 18 month randomized control trial
• 100 patients b/w the age group 18-40yrs- sirolimus (target dose 2 mg daily) or standard care
• Sirolimus level b/w 4 and 10 microgram/litre
• Estimated CrCl 70 ml/min • Serial MRI – to measure the
volume of polycystic kidney disease
• At randomization- median kidney volume was 907cm3 (sirolimus) and 1003 (control group)
• Primary outcome- kidney volume at 18 months
• Secondary outcomes –GFR and urine albumin excretion
Results: • Median increase in
sirolimus group was 99 cm3( interquartile range 43-173) Control group 97 cm3( interquartile range 37-181) at 18 months
• GFR did not differ between two groups
• Urinary albumin excretion rate was higher in sirolimus group
NEJM aug 2010

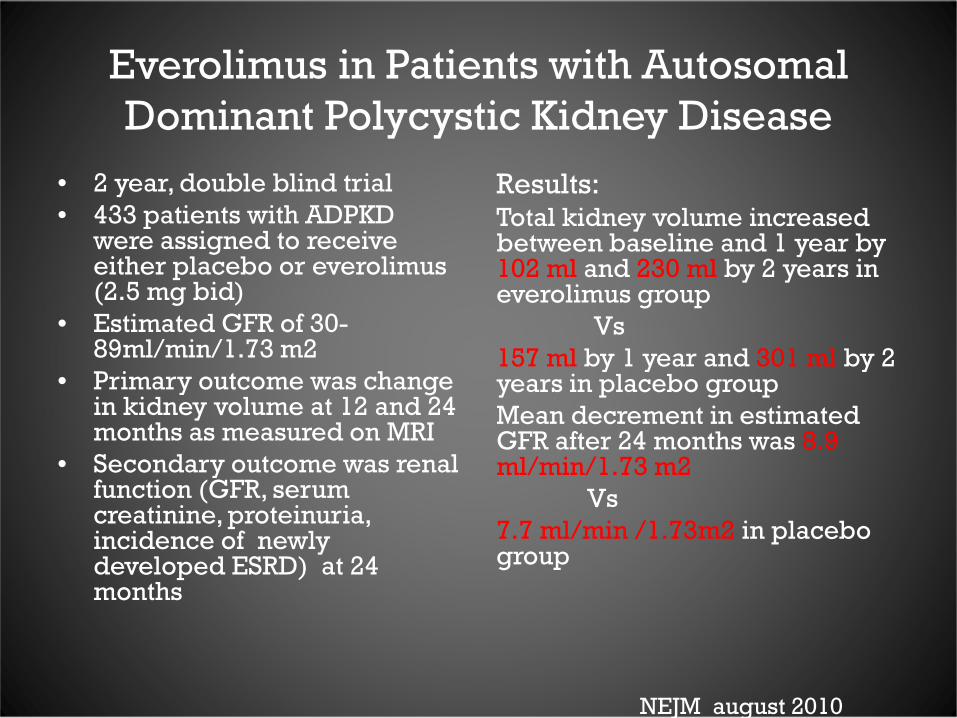
Everolimus in Patients with Autosomal Dominant Polycystic Kidney Disease
• 2 year, double blind trial • 433 patients with ADPKD
were assigned to receive either placebo or everolimus (2.5 mg bid)
• Estimated GFR of 30-89ml/min/1.73 m2
• Primary outcome was change in kidney volume at 12 and 24 months as measured on MRI
• Secondary outcome was renal function (GFR, serum creatinine, proteinuria, incidence of newly developed ESRD) at 24 months
Results: Total kidney volume increased between baseline and 1 year by 102 ml and 230 ml by 2 years in everolimus group Vs 157 ml by 1 year and 301 ml by 2 years in placebo group Mean decrement in estimated GFR after 24 months was 8.9 ml/min/1.73 m2 Vs 7.7 ml/min /1.73m2 in placebo group
NEJM august 2010


Rapamycin may not inhibit mTOR in ADPKD kidneys
Canaud et. al (2010) AJT
• Do polycystic kidney disease cells have up regulated telomerase activity?

TELOMERE and TELOMERASE


TELOMERES • Telomeres are DNA-protein structures that protect
the chromosome ends from degradation and fusion
• Telomere DNA sequence comprises of tandem repeats of the six nucleotide unit sequence TTAGGG. These sequences extend for thousands of bases at chromosome ends, averaging 10 kb in a newborn human’s cord blood.
• Telomere DNA is bound by a specialized group of protective proteins collectively called shelterin

TELOMERASE • Telomerase was first identified in ciliated protozoan “tetrahymena”
• Telomerase is a specialized DNA polymerase that synthesizes new
telomere sequences onto chromosome ends.
• Telomerase is composed of the core telomerase protein TERT, which contains the telomerase reverse transcriptase domain and and an essential RNA component called TERC which provides the template for telomeric sequence synthesis
• Telomerase activity is regulated during development and has a very low
level, almost undetectable in somatic cells. Telomerase is found in found in fetal tissue, germ cells
• Telomerase activity has been found to be up-regulated in most cancer cells thus allowing cancer cells to escape cellular senescence and becoming immortal.

Science 1994
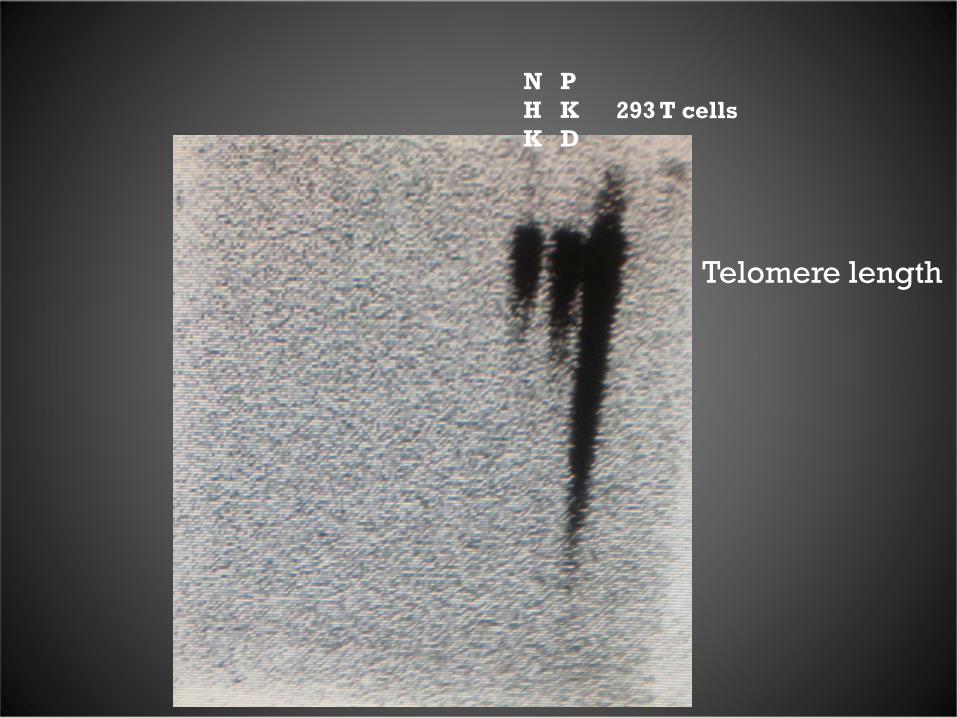
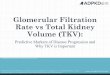
Telomere length
293 T cells PKD
NHK

Thank You!