Embed Size (px)
Citation preview

Preat et al. Diagnostic Pathology 2014, 9:26http://www.diagnosticpathology.org/content/9/1/26
RESEARCH Open Access
Differences in breast carcinomaimmunohistochemical subtypes betweenimmigrant Arab and European womenFanny Preat, Philippe Simon and Jean-Christophe Noel*
Abstract
Background: There is a dearth of information on the clinicopathological differences, including the molecularsubtypes, of breast carcinomas from immigrant Arab women in Europe. Therefore, the aim of our study was toexamine and compare these features in immigrant Arab/Moroccan patients with those of European women.
Methods: Included in this study were 441 cases of breast cancer: 91 Arab/Moroccan women and 350 Europeanwomen. Age, size, grade, node involvement, and immunohistochemical profile (classification into the followingsubtypes: luminal A, luminal B, HER2 +/ER -, and triple negative) were analyzed.
Results: The average age of breast cancer presentation in Arab women is almost a decade earlier than in Europeanwomen (49 versus 60 years old; p = 0.00001). Arab patients also had a higher average tumor size (25 mm versus19 mm; p =0,008) and more grade 3 and less grade 1 tumors (p = 0.02). It should be noted, however, that thisvariability in the size and grade do not appear statistically significant when compared in Arab and Europeanpatients under 50 years old. In contrast, independent of age, the immunohistochemical subtypes were differentbetween the two populations, with a greater number of luminal B subtype and fewer luminal A subtype (p <0.02)in Arab patients.
Conclusions: Arab patients with breast carcinoma have different clinicopathological features from Europeanpatients, mainly the age of cancer presentation. Their immunohistochemical profile is also different, with moreluminal B and less luminal A subtypes, suggesting that there are not only clinicopathological differences but alsodisparities in the expression profiling in these women.
Virtual slide: The virtual slides for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/2104813621113288.
Keywords: Arab, European, Breast carcinoma, Molecular classification, Luminal A, Luminal B, Immunohistochemistry
BackgroundIn Belgium, breast cancer accounts for almost 13% of allcancers and each year 9,400 new cases are observed. Itsincidence is estimated at 146/100,000 [1]. The origin ofthis cancer is likely multifactorial and many factors havebeen implicated, including the woman’s reproductivelifestyle, endogenous hormones, exogenous hormones,adiposity, physical activity, nutrition, alcohol consump-tion, smoking, environmental toxins, and genetic suscep-tibility in inherited syndromes [2]. Breast cancer rates
* Correspondence: [email protected] of Senology, Erasme University Hospital-ULB, Route de Lennik808, B-1070 Bruxelles, Belgium
© 2014 Preat et al.; licensee BioMed Central LtCommons Attribution License (http://creativecreproduction in any medium, provided the orwaiver (http://creativecommons.org/publicdomstated.
also differ by race and ethnicity [3]. It has been sugges-ted that breast cancer in Arab populations has specificmorphological and molecular characteristics, includingpoorly differentiated pathological features and increasedHER2 overexpression [4]. Naturally, Arab populationsare not homogeneous and have genetic diversity [5].However, in a recent publication El Fatemi et al. demon-strated that in a Moroccan Arab population, the luminalB subtype was the most prevalent [6]. These studies,however, were performed on the indigenous population,and there are no data on the Moroccan Arab immigrant
d. This is an Open Access article distributed under the terms of the Creativeommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andiginal work is properly cited. The Creative Commons Public Domain Dedicationain/zero/1.0/) applies to the data made available in this article, unless otherwise

Table 1 Clinicopathological characteristics of the breastcancer patients (all ages combined)
European Arabic/Moroccan P-value
Number 350 91
Mean age (SD) 60 (13) 49 (11) 0.00001
Mean size (SD) 19 (14) 25 (18) 0.008
pT
< 20 mm 216 (62%) 45 (49%) 0.04
≥ 20 mm 134 (38%) 46 (51%)
Tumor grade
G1 69 (20%) 7 (8%) 0.02
G2 169 (48%) 41 (45%) NS
G3 112 (32%) 43 (47%) 0.01
Nodes
N positive 78 (22%) 26 (29%) NS
N Negative 272 (78%) 65 (71%)
Estrogen receptors
Positive (>1%) 301 (86%) 72 (79%) NS
Negative 49 (14%) 19 (21%)
Progesterone receptors
Positive (>1%) 266 (76%) 58 (64%) 0.02
Negative 84 (24%) 33 (36%)
Mean Ki-67 (SD) 20 (14) 27 (20) 0.003
Molecular classification
Luminal A 160 (46%) 21 (23%) 0.001
Luminal B 141 (40%) 51 (56%) 0.02
HER2 17 (5%) 5 (6%) NS
Triple negative 32 (9%) 14 (15%) NS
Preat et al. Diagnostic Pathology 2014, 9:26 Page 2 of 5http://www.diagnosticpathology.org/content/9/1/26
women in Western Europe. Since the Moroccan immi-grant population is the most common at our institution,the aim of this study was to define the morphologicaland immunohistochemical (surrogates to molecular clas-ses) characteristics of breast carcinomas in these immi-grant Moroccan Arab patients and compare them withthe European native population.
Materials and methodsBreast carcinoma specimens in formalin-fixed, paraffin-embedded tissue blocks from 441 female patients diag-nosed with invasive carcinoma from january 2008 todecember 2012 were retrieved from the archives of theDepartment of Pathology, Erasme University Hospital.This study was approved by the local ethics committee(Erasme University Hospital, reference number: 2013/027)and included 350 European white women and 91 MoroccanArab patients. The pathological stage and histologicalgrade were defined according to the criteria of the WorldHealth Organization 2012 [7]. The estrogen receptor (ER),progesterone receptor (PR), Ki-67 labeling index, andHER2 expression were evaluated at the time of the ori-ginal diagnosis by immunohistochemistry, as previouslydescribed [8-10]. A clinically positive test for the receptorsis defined as nuclear staining in ≥1% of the tumor cells[8]. HER2 immunoreactivity was performed using the Or-acle HER2 test (clone CB11; Leica Microsystems GmbH,Wetzlar, Germany) according to the manufacturer’s in-structions, as previously described [10]. The scoring wasassessed with the recommendations of the American So-ciety of Clinical Oncology [11]. All of the HER2 scores of2+ and 3+ were analyzed using the fluorescent in situhybridization (FISH) PathVysion HER2 DNA test (Abbottlaboratories, Abbott Park, USA) according to the manu-facturer’s instructions. Signal ratios (HER2/CEP17) of ≥2were classified as amplified. In this study, only 2+ and 3+tumors with a HER2 FISH amplification were consideredas a positive result. A subtype immunohistochemical clas-sification (surrogates to molecular classes) was adopted tocharacterize the tumors, using the following criteria:Luminal A, when either one or both of the ER and PR werepresent, HER2 was negative and Ki-67 <14%; Luminal B,when ER and/or PR were present and either Ki-67 ≥14% orHER2 was positive; HER2 positive, when ER and PR wereabsent and HER2 was positive irrespective of the Ki-67;and Triple negative, when ER and PR were absent andHER2 was negative. The correlation analysis was con-ducted using the χ2 test and Fisher’s exact probably test.For the comparison of the means, the student’s t-test wasused. Results were considered significant when p <0.05.
ResultsThe clinicopathological characteristics of the 441 pa-tients are summarized in the Table 1. Arab/Moroccan
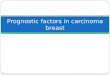
patients were characterized by an average age of pre-sentation for breast cancer almost a decade earlier thanin European individuals (49 versus 60 years old; p =0.00001). In addition, the size of the tumor in these pa-tients was larger (25 mm versus 19 mm; p = 0.008), theincidence of grade 3 tumors more frequent (p = 0.01),the grade 1 less frequent (p = 0.02), the percentage of PRpositive lesions was less (p = 0.02), the mean Ki-67 indexwas higher (27% versus 20%; p = 0.003), the Luminal Atumor was less frequent (p = 0.001), and the Luminal Bwas more frequent (p = 0.02). To ensure these resultswere not biased by the age at the time of the presenta-tion of cancer, we only extracted premenopausal patientsfrom this series. This enabled us able to compare groupswith an almost identical age (43 versus 42 years old). In-terestingly, despite these adjustments, the Arab/Moroccanpatients continued to display less Luminal A tumors (p =0.01) and more Luminal B tumors (p = 0.02) (Table 2)(Figure 1).

Table 2 Clinicopathological characteristics in thepremenopausal women
European Arabic/Moroccan P-value
Number 86 56
Mean age (SD) 43 (4) 42 (15) NS
Mean size (SD) 22 (14) 24 (17) NS
pT
< 20 mm 47 (55%) 30 (54%) NS
≥ 20 mm 39 (45%) 26 (46%)
Tumor grade
G1 12 (14%) 1 (2%) 0.02
G2 42 (49%) 27 (48%) NS
G3 32 (37%) 28 (50%) NS
Nodes
N positive 23 (27%) 18 (32%) NS
N Negative 63 (73%) 38 (68%)
Estrogen receptors
Positive (>1%) 71 (83%) 45 (80%) NS
Negative 15 (17%) 11 (20%)
Progesterone receptors
Positive (>1%) 61 (71%) 37 (66%) NS
Negative 25 (29%) 19 (34%)
Mean Ki-67 (SD) 24 (18) 29 (20) 0.04
Molecular classification
Luminal A 35 (41%) 10 (18%) 0.01
Luminal B 36 (42%) 35 (63%) 0.02
HER2 4 (4%) 3 (5%) NS
Triple negative 11 (13%) 8 (14%) NS
Preat et al. Diagnostic Pathology 2014, 9:26 Page 3 of 5http://www.diagnosticpathology.org/content/9/1/26
DiscussionThe study of possible ethnic differences in breast cancerhas mainly occurred in the United States [12]. Recently,new data have been described for Arab populations, butthe true prevalence of breast cancer remains uncertain
Figure 1 Immunohistochemical profile surrogates of the molecular cl
[4,13-17]. For the majority of these studies, which wereperformed only on indigenous populations, some cli-nicopathological features are repeatedly observed: theage of cancer presentation is a decade earlier than inEuropean or US patients, the average size of the lesionsis often greater than 20 mm, and the grade of tumors isoften higher. Interestingly, these data were corroboratedin our study of Arab/Moroccan immigrants. Indeed, inour series, the mean age of presentation of breast cancerwas 49 years old in Moroccan patients and occurred al-most a decade earlier than in European patients (meanage: 60 years old; p = 0.00001) (Table 1). These data aresimilar to those recently published by Chouchane et al.in a review article, in which the mean age of presenta-tion of breast cancer for Arab patients was 48 years old,compared to 63 years old in European women. Theseauthors also observed that two-thirds of the Arab pa-tients with breast cancer are younger than 50 years old[4]. We found similar results with our Arab immigrantpopulation. Indeed, 61% of the Arab patients with cancerwere less than 50 years old, compared to only 24% inthe European population (p = 0.0001) (Table 2). How-ever, these results should be interpreted with caution asthey may simply reflect that the immigrant population ison average younger than the European population andthat the Arab older patients have a different perceptionof breast cancer and therefore do not participate in thescreening program. These challenges and barriers tobreast cancer screening in Arab women have been dem-onstrated in several studies [17-19].The second observation on Arab patients frequently
found in the literature is the presence of larger tumors(mean tumor size greater than 20 mm) and a highergrade (grade 3) at diagnosis [20,21]. We were able toconfirm these findings in the general population used inour study. Indeed, over 50% of the Arab patients hadtumors larger than 20 mm, compared to 38% of theEuropean patients with a tumor greater or equal to 20 mm(p = 0.04). Furthermore, the average tumor size was 25 mm
asses in premenopausal women (in percentage).

Preat et al. Diagnostic Pathology 2014, 9:26 Page 4 of 5http://www.diagnosticpathology.org/content/9/1/26
in the Arab patients, while it was only 19 mm in Europeans(p = 0.008) (Table 1). We also demonstrated that the Arabpatients had an increased incidence in grade 3 tumors (p =0.01) and fewer grade 1 tumors (p = 0.01) than Europeans.However, the data concerning the tumor size and
grade are only statistically significant in the general po-pulation, with all ages combined. Indeed, if we restrictour analysis to the premenopausal women under 50years old, the differences in the tumor size and grade areless obvious (Table 2). This phenomenon is consistentwith recent publications that establish a strong link be-tween age at diagnosis and the size and/or grade of thetumor [7,22]. Molecular subtyping of breast cancer geneexpression has resulted in a better understanding ofbreast carcinoma and several distinctive breast carcin-oma molecular subtypes have been identified [22,23]. Inaddition to this gene expression analysis, immunohisto-chemical surrogates have been used for breast cancerclassification with relatively good reproducibility [24]. Inthe present work, we demonstrated that the luminal sub-type B was the most common in an Arab/Moroccan im-migrant population. This subtype was found in 56% ofthe women in the general population but only in 40% ofthe European women (p = 002) (Table 1). In contrast,the luminal A subtype was significantly more commonin the European (46% than in the Arab patients (23%;p = 0.001). Interestingly, these statistically significant dif-ferences in the incidence of luminal A and B subtypes be-tween the two populations were also seen in patientsunder 50 years old (Table 2). However, no differences wereobserved for the subtypes HER2 and triple negative. Ourresults corroborate the study performed on a native popu-lation in Morocco, where the luminal B subtype was alsothe most common [6]. Deregulation in both genomic and/or proteomic expression of cytokeratin 8/18 and TFAP2C(a member of the AP-2 family) has been shown to regulateexpression of the ER, and the RET proto-oncogene mightcontribute to the high proportion of the luminal B subtypeobserved in Arab women. However, this observationshould be confirmed in future studies [25].
ConclusionsArab immigrant patients with breast carcinoma have dif-ferent clinicopathological features from those of Europeanwomen. In particular, the average age at presentation is al-most a decade earlier than in European women and ap-pears as a key factor that at least partially explains theother variable modifications, including the lesion size andhistological grade. Moreover, independent of age, the im-munohistochemical profile of the molecular classes is dif-ferent, with more luminal B and less luminal A subtypes,suggesting that there are clinicopathological differences,as well as disparities in the expression profiling in thesewomen.
AbbreviationsER: Estrogen receptor; PR: Progesterone receptor; HER2: Human epidermalgrowth factor receptor 2; FISH: Fluorescent in situ hybridization; CEP 17:Chromosome 17 centromere; TFAP2C: Transcription factor AP-2 gamma;AP-2: Activating protein 2; RET: Proto-oncogene tyrosine protein kinasereceptor.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsAll authors analyzed, interpreted, and approved the final manuscript.
FundingThis study has not received funding from a specific grant.
Received: 14 November 2013 Accepted: 21 December 2013Published: 4 February 2014
References1. Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P: Estimates of
the cancer incidence and mortality in Europe in 2006. Ann Oncol 2007,18:581–592.
2. McPherson K, Steel CM, Dixon JM: Breast cancer: epidemiology, riskfactors and genetics. BMJ 2000, 321:624–628.
3. Bernstein L, Teal CR, Joselyn S, Wilson J: Ethnicity-related variation inbreast cancer risk factors. Cancer 2003, 97:222–229.
4. Chouchane L, Boussen H, Satry K: Breast cancer in Arab populations:molecular characteristics and disease management implications. LancetOncol 2013, 14:417–424.
5. Teebi AS, Teebi SA: Genetic diversity among the Arabs. Community Genet2005, 8:21–26.
6. El Fatemi H, Chahbouni S, Jayi S, Moumna K, Melhouf MA, Bannani A,Mesbahi O, Amarti A: Luminal B tumors are the most frequentmolecular subtype in breast cancer of North African women: animmunohistochemical profile study from Morocco. Diagn Pathol 2012,7:170.
7. Lakhani SR, Ellis IO, Schnitt SJ, Hoon Tan P, van de Vijver MJ (Eds): WHOclassification of tumours of the breast. Lyon, France: IARC Press; 2012.
8. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S,Fitzgibbons PL, Francis G, Goldstein NS, Hayes M, Hicks DG, Lester S, Love R,Mangu PB, McShane L, Miller K, Osbome CK, Paik S, Perlmutter J, Rhodes A,Sasano H, Schwartz JN, Sweep F, Taube S, Torlakovic EE, Valenstein P, VialeG, Visscher D, Wheeler T, Williams RB, et al: American Society of ClinicalOncology/College of American Pathologists guideline recommendationsfor immunohistochemical testing of estrogen and progesteronereceptors in breast cancer. J Clin Oncol 2010, 28:2074–2795.
9. Dowsett M, Nielsen TO, A’Hern R, Bartlett J, Coombes C, Cuzick J, Ellis M,Henry NL, Hugh JC, Lively T, McShane L, Paik S, Penault-Llorca F, Prudkin L,Regan M, Salter J, Sotiriou C, Viale G, Zujewski JA, Hayes DF: Assessment ofKi-67 in breast cancer: recommendations from the international KI67 inBreast Cancer working group. J Natl Cancer Inst 2011, 103:1656–1664.
10. Schrohl AS, Pedersen HC, Jensen SS, Nielsen S, Brünner N: Humanepidermal growth factor receptor 2 (HER2) immunoreactivity: specificityof three pharmacodiagnostic antibodies. Histopathology 2011, 59:975–983.
11. Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH,Allred DC, Bartlett J, Bilous M, Fitzgibbons P, Hanna W, Jenkins R, Mangu P,Paik S, Perez EA, Press MF, Spears PA, Vance GH, Viale G, Hayes DF:American Society of Clinical Oncology/College of American Pathologistsguideline recommendations for human epidermal growth factorreceptor 2 testing in breast cancer. J Clin Oncol 2013, 31:3997–4013.
12. Eheman CR, Shaw KM, Ryerson AB, Miller JW, Ajani UA, White MC: Thechanging incidence of in situ and invasive ductal and lobular breastcarcinomas: United States 1999–2004. Cancer Epidemiol Biomarkers Prev2009, 18:1763–1769.
13. El Saghir NS, Khalil MK, Eid T, El Kinge AR, Charafeddine M, Geara F, SeouldM, Shamseddine AL: Trends in epidemiology and management of breastcancer in developing Arab countries: a literature and registry analysis. IntJ Surg 2007, 5:225–233.

Preat et al. Diagnostic Pathology 2014, 9:26 Page 5 of 5http://www.diagnosticpathology.org/content/9/1/26
14. Boulos S, Gadallah M, Neguib S, Essam E, Youssef A, Costa A, Mittra I, MillerAB: Breast screening in the emerging world: high prevalence of breastcancer in Cairo. Breast 2005, 14:340–346.
15. Bujassoum SM, Gehani AA: Epidemiology of breast cancer in Qatar1999–2002. Qatar Med J 2004, 13:43–45.
16. El-Zaemey S, Nagi N, Fritschi L, Heyworth J: Breast cancer among Yemeniwomen using the National Oncology Centre Registry 2004–2010. CancerEpidemiol 2012, 36:249–253.
17. Azaiza F, Cohen M: Health beliefs and rates of breast cancer screeningamong Arab women. J Womens Health 2006, 15:520–530.
18. Mellon S, Gauthier J, Cichon M, Hammad A, Simon MS: Knowledge,attitude and beliefs of Arab-American women regarding inherited cancerrisk. J Genet Couns 2013, 22:268–276.
19. Kawar LN: Barriers to breast cancer screening participation amongJordanian and Palestinian American women. Eur J Oncol Nurs 2012,1:88–94.
20. Missaoui N, Jaidene L, Abdelkrim SB, Abdelkader A, Beizig N, Yaacoub LB,Yaacoubi MT, Hmissa S: Breast cancer in Tunisia: clinical and pathologicalfindings. Asian Pac J Cancer Prev 2011, 12:169–172.
21. Al-Kuraya K, Schraml P, Skeik S, Amr S, Torhost J, Tapia C, Novotny H,Spichtin H, Maurer R, Mislacher M, Simon R, Sauter G: Predominance ofhigh grade pathway in breast cancer development of Middle Eastwomen? Mod Pathol 2005, 18:891–895.
22. Cakir A, Gonul I, Uluoglu O: A comprehensive morphological study forbasal-like breast carcinomas with comparison to nonbasal-like carcin-omas. Diagn Pathol 2012, 7:145.
23. Sorlie T, Perou C, Tibshirani R, Aas T, Geisler S, Johnsen H, Hartie T, Eisen M,van de Rijn M, Jeffrey S, Thorsen T, Quist H, Matese J, Brown P, Botstein D,Eystein Lonning P: Gene expression patterns of breast carcinomadistinguish tumor subclasses with clinical implications. Proc Natl Acad SciU S A 2001, 98:10869–10874.
24. Goldhirsch A, Wood W, Coates AS, Gelber R, Thurslimann B, Senn H:Strategies for subtypes-dealing with diversity of breast cancer: highlightsof the St Gallen International expert consensus on primary therapy ofearly breast cancer 2011. Ann Oncol 2011, 22:1736–1747.
25. Chalabi N, Bernard-Gallon DJ, Bignon Y: Comparative clinical and transcrip-tomal profiles of breast cancer between French and South Mediterraneanpatients show minor bit significative biological differences. CancerGenomics Proteomics 2008, 5:253–261.
doi:10.1186/1746-1596-9-26Cite this article as: Preat et al.: Differences in breast carcinomaimmunohistochemical subtypes between immigrant Arab and Europeanwomen. Diagnostic Pathology 2014 9:26.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit