-
CASE REPORT Open Access
Resection of rectal cancer resemblingsubmucosal tumor that was
preoperativelydiagnosed with endoscopic ultrasound-guided
biopsyAkimitsu Tanio, Hiroaki Saito* , Keigo Ashida, Shouichi
Urushibara, Manabu Yamamoto, Naruo Tokuyasu,Teruhisa Sakamoto,
Soichiro Honjo, Yoshihiko Maeta and Yoshiyuki Fujiwara
Abstract
Background: Colorectal cancer (CRC) resembling submucosal tumor
(SMT; CRC/SMT) is very rare. Because its biopsyis challenging,
accurate preoperative diagnosis is also very rare.
Case presentation: A 55-year-old woman with a high serum
carcinoembryonic antigen level underwent a computedtomography
colonoscopy, which showed extrinsic rectum compression. A coronal
magnetic resonance image showeda 4-cm low-intensity tumor between
her rectum and sacrum. Endoscopic ultrasound (EUS) showed a
30-mmlow-echoic lesion originating from the rectum. Pathological
examination of specimen obtained with EUS-guided fine-needle
aspiration biopsy (EUS-FNAB) revealed adenocarcinoma.
Immunohistochemical stainingshowed the tumor to be positive for
both CK20 and CDX2 and negative for CK7, indicating that it was
arectal cancer. We performed a laparoscopy-assisted low-anterior
resection with dissection of the regionallymph nodes after eight
chemotherapy cycles. Macroscopically, tumor was completely covered
by normalrectal mucosa, but showed a 2-mm bulge on the mucosa.
Histological examination revealed a moderately
differentiatedadenocarcinoma, mainly located at the subserosal
layer and severely invaded to lymphatic and blood vessels.
Themucosal layer was not exposed to the cancer components, and her
postoperative course was uneventful.
Conclusion: EUS-FNAB was useful in preoperative accurate
diagnosis of this very rare tumor. We also review theliterature and
discuss CRC/SMT.
Keywords: Colorectal cancer, Endoscopic ultrasound-guided fine
needle aspiration biopsy, Submucosal tumor
BackgroundSubmucosal tumor (SMT) usually arises from tissue
inthe wall of digestive tract, and its surface is thereforecovered
with normal mucosa in most cases. In contrast,gastrointestinal (GI)
carcinomas arise from the epithe-lium, and most of their mucosal
surfaces typically con-sist of cancerous tissue. SMT-like growth is
an unusualpresentation for GI carcinomas, especially in
colorectalcancer (CRC). We herein report a rare case of
rectalcancer resembling SMT (CRC/SMT) in which endoscopic
ultrasound-guided fine needle aspiration biopsy (EUS-FNAB) was
useful in accurate preoperative diagnosis. Wealso review the
literature and discuss CRC/SMT.
Case presentationAn asymptomatic 55-year-old woman underwent a
de-tailed GI tract examination, as she was found to havehigh serum
carcinoembryonic antigen (CEA, 26.6 ng/ml)at a local hospital. She
had no event in her past or familyhistory, especially for
colorectal neoplasm or other ma-lignancy. Physical examination and
blood chemicalexamination were within normal ranges except for
highserum CEA level. Computed tomography (CT) colonos-copy revealed
extrinsic rectum compression (Fig. 1a). A
* Correspondence: [email protected] of Surgical
Oncology, Department of Surgery, School of Medicine,Tottori
University Faculty of Medicine, 36-1 Nishi-cho, Yonago
683-8504,Japan
© The Author(s). 2017 Open Access This article is distributed
under the terms of the Creative Commons Attribution
4.0International License
(http://creativecommons.org/licenses/by/4.0/), which permits
unrestricted use, distribution, andreproduction in any medium,
provided you give appropriate credit to the original author(s) and
the source, provide a link tothe Creative Commons license, and
indicate if changes were made.
Tanio et al. Surgical Case Reports (2017) 3:84 DOI
10.1186/s40792-017-0362-7
http://crossmark.crossref.org/dialog/?doi=10.1186/s40792-017-0362-7&domain=pdfhttp://orcid.org/0000-0001-7675-0754mailto:[email protected]://creativecommons.org/licenses/by/4.0/
-
coronal magnetic resonance image (MRI) showed a
4-cmlow-intensity tumor between the rectum and sacrum(Fig. 1b); the
patient was referred to our hospital forfurther evaluation of this
tumor. The 18-FDG positronemission tomography (PET) and CT scans
indicated high18-FDG uptake in the primary tumor (SUVmax: 3.34;Fig.
2a), with enlarged para-aortic lymph node (SUVmax:2.58; Fig. 2b)
and anterosuperior segment of right hepaticlobe (SUVmax: 2.74; Fig.
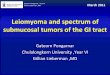
2c). Colonoscopy showed extrin-sic rectum compression, but no
change in her rectal mu-cosa (Fig. 3a). Pathological examination of
rectum biopsyspecimen showed normal rectal mucosa.
Endoscopicultrasound (EUS) showed a 30-mm, low-echoic
lesionoriginating from the rectum (Fig. 3b). Pathological
exam-ination of biopsied specimen obtained with
EUS-guidedfine-needle aspiration biopsy (EUS-FNAB)
revealedadenocarcinoma. Immunohistochemical staining showedthat the
specimen was positive for both cytokeratin 20
(CK20; Fig. 3c) and caudal-type homeobox 2 (CDX2;Fig. 3d) and
negative for cytokeratin-7 (CK7), which indi-cated that it had
originated from rectal cancer. Weplanned to perform low-anterior
resection with dissectionof the regional lymph nodes and an
enlarged para-aorticlymph node under the diagnosis of rectal cancer
and pos-sible metastasis to liver and para-aortic lymph
node,followed by resection of possible liver metastasis
afterpostoperative chemotherapy. Because of a possibilitythat tumor
had invaded to the sacrum, however, weperformed neoadjuvant
chemotherapy with capecita-bine and oxaliplatin. The tumor shrank
by 38% after8 courses of chemotherapy, and we performed
alaparoscopy-assisted low-anterior resection with dis-section of
the regional lymph nodes as planned. Al-though we confirmed direct
invasion of the tumor tohypogastric nerve during the surgery, the
tumor didnot invade to the sacrum. An enlarged para-aortic
lymph
a b
Fig. 1 a CT colonoscopy revealed extrinsic compression of
rectum. b Coronal magnetic resonance imaging (MRI) showed 4-cm
low-intensitytumor between rectum and sacrum
a b
c
Fig. 2 The 8-FDG positron emission tomography (PET) and CT scans
indicate high 18-FDG uptake in (a) the primary tumor (SUVmax:
3.34);(b) enlarged para-aortic lymph node (SUVmax: 2.58); and (c)
anterosuperior segment of right hepatic lobe (SUVmax: 2.74)
Tanio et al. Surgical Case Reports (2017) 3:84 Page 2 of 5
-
node was also removed. Macroscopically, the tumor wascompletely
covered by normal rectal mucosa (Fig. 4a), al-though there was a
2-mm bulge of elevated lesion on themucosa (Fig. 4b).
Histologically, the tumor was composedfrom moderately
differentiated adenocarcinoma (Fig. 5a)and was mainly located at
subserosal region with severe in-vasion to lymphatic and blood
vessels (Fig. 5b). However,the mucosal surface showed no exposure
of the cancercomponent (Fig. 5c). Metastases were found in two
lymphnodes of mesorectum (#251) and in one lymph node alongthe
superior rectal artery (#252), although there was nometastasis in
the para-aortic lymph node dissected. Thepostoperative course was
uneventful. The patient is cur-rently undergoing chemotherapy for
liver metastasis in theoutpatient clinic of our hospital.
DiscussionCarcinomas of the digestive tract arise from the
mucosalepithelium; most of their mucosal surfaces consist
ofcancerous tissues. Although cancer cells then infiltrateboth
horizontally and vertically, the dominant directiondepends on the
nature of the cancer cells. Some intes-tinal cancers dominantly
infiltrate in a vertical directionwithout massive invasion along
the horizontal plane. Asa result, the internal intestinal surfaces
over these tu-mors are mostly covered with normal mucosa,
andtherefore manifest as SMTs. This type of tumor is some-times
called a carcinoma resembling an SMT; and al-though it is extremely
rare, has been reported in theesophagus [1], stomach [2], and colon
and rectum [3, 4].A report that reviewed 70 reported cases of
CRC/SMT
a b
c d
Fig. 3 a Colonoscopy also showed extrinsic compression of
rectum, but no change in rectal mucosa. b Endoscopic ultrasound
(EUS) showed a30-mm low echoic lesion originating from rectum.
Immunohistochemical staining of biopsy specimen obtained by
EUS-FNAB showed that tumorwas positive for both (c) CK20 and (d)
CDX2
a b
Fig. 4 a Macroscopically, the tumor was completely covered by
normal rectal mucosa. b The formalin-fixed resected specimen showed
a 2-mmbulge above the mucosa level
Tanio et al. Surgical Case Reports (2017) 3:84 Page 3 of 5
-
found it to be characterized by small tumor size, highrates of
poorly differentiated adenocarcinoma or mucin-ous adenocarcinoma,
and invasiveness (including highrates of lymph node metastasis and
lymphatic vessel in-vasion) [4].Two points make our case different
from previously
reported CRC/SMT. Firstly, the tumor was completelycovered by
normal rectal mucosa in our case. Most tu-mors reported previously
showed at least faint mucosalchanges, such as erosion and
ulceration, which aremicroscopically consistent with exposure of
carcinomacells. Because most of the cancer on our case was lo-cated
subserosally with no exposure of cancer cells onmucosal surface,
metastatic rectal cancer was consid-ered. In this regard,
immunohistochemical staining ofthe biopsied specimen showed the
tumor was positivefor CK20 and negative for CK7, indicating the
strong
possibility that our patient had primary rectal cancer. Tothe
best of our knowledge, only four cases (including thepresent case)
have been reported of CRC/SMT that werecompletely covered with
normal rectal mucosa (Table 1)[5–7]. Why no cancer cells were
exposed on the mucosallayer remains unclear. Cancer may arise from
ectopicmucosal cells in the rectal wall. Further investigationsare
required to show the detailed mechanism.Secondly, our case clearly
showed that EUS-FNAB is
useful for accurate preoperative diagnosis of CRC/SMT.EUS-FNAB
was recently shown to be useful in accuratepreoperative diagnosis
of gastrointestinal stromal tumor(GIST) [8] and pancreatic cancer
[9]. Previous reportshave shown the difficulty of preoperative
CRC/SMTdiagnosis, because of the difficulty of obtaining
biopsyspecimens. Therefore, EUS-FNAB should be consideredto make
accurate preoperative SMT diagnoses in colon
Fig. 5 a Histologically, the tumor was composed of moderately
differentiated adenocarcinoma. b The carcinoma was mainly located
at subserosaand had severely invaded to lymphatic and blood
vessels. c Adenocarcinoma was observed in the submucosal layer and
the mucosal surfaceshowed no exposure of the cancer component
Table 1 Reported cases of colorectal cancer resembling SMT in
which tumor was completely covered with normal colorectal
mucosa
Case Year Age(years)
Gender Locationa Size(cm)
Endoscopicfindings
Depth ofinvasionb
Histologicdiagnosis ofbiopsy specimen
Histologicdiagnosis ofresected specimenc
Lymphnodemetastasis
Distantmetastasis
Reference
1 2005 57 M Rb 10 None A Unknown Muc Absent Unknown 5
2 2011 82 M S 8 None SS Normal mucosa Muc Absent Absent 6
3 2014 79 M Ra 2.6 Erosion SE Not performed Mod Absent Absent
7
4 2017 55 F RS 4 None SS Normal mucosa Mod Present
Livermetastasis
Our case
aLocation. Ra upper rectum, Rb lower rectum, RS rectosigmoid, S
sigmoid colonbDepth of invasion. A adventitia, SE serosa, SS
subserosacHistologic diagnosis of resected specimen. Mod moderately
differentiated adenocarcinoma, Muc mucinous carcinoma
Tanio et al. Surgical Case Reports (2017) 3:84 Page 4 of 5
-
and rectum. To our knowledge, our case is the first touse
EUS-FNAB for an accurate preoperative diagnosis ofCRC/SMT.
ConclusionWe should keep in mind that colorectal cancer
canpresent with SMT-like growth. Furthermore, EUS-FNABis useful for
preoperative accurate diagnosis of this rarecolorectal cancer.
Received: 3 April 2017 Accepted: 11 July 2017
Authors’ contributionsAT contributed to the drafting of the
manuscript. KA, SU, MY, NT, TS, SH, andYM contributed to the
critical revision of the manuscript. HS and YFcontributed to the
final approval of the manuscript. All authors read andapproved the
final manuscript.
Consent for publicationConsent for publication was obtained from
the patients.
Competing interestsThe authors declare that they have no
competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to
jurisdictional claims in publishedmaps and institutional
affiliations.
Received: 3 April 2017 Accepted: 11 July 2017
References1. Kishino T, Yamaguchi Y, Yamagishi T, Hashimoto T,
Kyomasu Y, Mori H, et al.
Submucosal tumor (SMT)-like esophageal squamous cell carcinoma
withgastric metastasis. Hepatogastroenterology. 2000;47:1581–4.
2. Ohara N, Tominaga O, Uchiyama M, Nakano H. A case of advanced
gastriccancer resembling submucosal tumor of the stomach. Jpn J
Clin Oncol.1997;27:423–6.
3. Shinagawa T, Ishihara S, Nozawa H, Murono K, Nishikawa T,
Otani K, et al.Small colorectal cancers resembling submucosal tumor
with massivesubmucosal invasion and lymph node metastasis: A report
of two cases andreview of the literature. Clin Res Hepatol
Gastroenterol. 2016;41:e19–e23.
4. Nakajima T, Kamano T, Shibasaki K, Watanabe K, Meguro H,
Tomiki Y, et al.Colon carcinoma resembling submucosal tumor: report
of a case andreview of the literature. Int J Gastrointest Cancer.
2005;36:155–61.
5. Kameda K, Matsuda G, Nakashima M, Kubo A, Takekawa Y, Kato K,
et al. Acase of mucoid carcinoma of rectum presented as a
submucosal tumorwhich was discovered by elevated value of CEA. J
Japan Surg Assoc. 2005;66:1985–9.
6. Sato K, Kojima Y, Matsuno Y, Watanabe Y. A case of mucoid
carcinoma ofthe sigmoid colon with features of a submucosal tumor.
J Japanese SocietyGastroenterol. 2011;108:88–94.
7. Shiraiwa S, Taniwaki S, Imamura T, Sou H, Shimokobe T,
Morimitsu Y. A caseof rectal cancer presented as submucosal tumor
without the continuationwith the mucous membrane. J Jpn Surg Assoc.
2014;75:749–53.
8. Mekky MA, Yamao K, Sawaki A, Mizuno N, Hara K, Nafeh MA, et
al.Diagnostic utility of EUS-guided FNA in patients with gastric
submucosaltumors. Gastrointest Endosc. 2010;71:913–9.
9. Duskova J, Krechler T, Dvorak M. Endoscopic ultrasound-guided
fine needleaspiration biopsy of pancreatic lesions. An 8-year
analysis of singleinstitution material focusing on efficacy and
learning progress.Cytopathology. 2016;28:109–15.
Tanio et al. Surgical Case Reports (2017) 3:84 Page 5 of 5
AbstractBackgroundCase presentationConclusion
BackgroundCase presentationDiscussionConclusionReferences