-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
1/9
Resistance in gram-negative bacteria:Enterobacteriaceae
David L. Paterson, MD, PhDPittsburgh, Pennsylvania
The emergence and spread of resistance in Enterobacteriaceae are
complicating the treatment of serious nosocomial infections
and threatening to create species resistant to all currently
available agents. Approximately 20% of Klebsiella pneumoniae
infections
and 31% of Enterobacter spp infections in intensive care units
in the United States now involve strains not susceptible to
third-
generation cephalosporins. Such resistance in K pneumoniae to
third-generation cephalosporins is typically caused by the
acqui-
sition of plasmids containing genes that encode for
extended-spectrum b-lactamases (ESBLs), and these plasmids often
carry other
resistance genes as well. ESBL-producing K pneumoniae and
Escherichia coliare now relatively common in healthcare settings
and
often exhibit multidrug resistance. ESBL-producing
Enterobacteriaceae have now emerged in the community as well.
Salmonella
and other Enterobacteriaceae that cause gastroenteritis may also
be ESBL producers, which is of relevance when children require
treatment for invasive infections. Resistance of Enterobacter
spp to third-generation cephalosporins is most typically caused
by
overproduction of AmpC b-lactamases, and treatment with
third-generation cephalosporins may select for
AmpC-overproducing
mutants. Some Enterobacter cloacae strains are now ESBL and AmpC
producers, conferring resistance to both third- and fourth-
generation cephalosporins. Quinolone resistance in
Enterobacteriaceae is usually the result of chromosomal mutations
leading
to alterations in target enzymes or drug accumulation. More
recently, however, plasmid-mediated quinolone resistance has
been reported in K pneumoniae and E coli, associated with
acquisition of the qnr gene. The vast majority of
Enterobacteriaceae,
including ESBL producers, remain susceptible to carbapenems, and
these agents are considered preferred empiric therapy for
serious Enterobacteriaceae infections. Carbapenem resistance,
although rare, appears to be increasing. Particularly
troublesome
is the emergence of KPC-type carbapenemases in New York City.
Better antibiotic stewardship and infection control are needed
to prevent further spread of ESBLs and other forms of resistance
in Enterobacteriaceae throughout the world. (Am J Infect
Control
2006;34:S20-8.)
Gram-negative bacteria of the Enterobacteriaceae
family are important causes of urinary tract infections(UTIs),
bloodstream infections, hospital- and health-
care-associated pneumonias, and various intra-abdom-
inal infections. Within this family, Escherichia coli is
afrequent cause of UTIs, Klebsiella spp and Enterobacterspp are
important causes of pneumonia, and all of
the Enterobacteriaceae have been implicated in blood-
stream infections and in peritonitis, cholangitis, and
other intra-abdominal infections. Additionally, organ-
isms such as Salmonella produce gastroenteritis and
subsequently, in some patients, invasive infection.
Emerging resistance in Enterobacteriaceae is a signifi-
cant problem that requires immediate attention. Re-
sistance related to production of extended-spectrum
b-lactamases (ESBLs) is a particular problem in the
handling of Enterobacteriaceae infections, but othermechanisms
of resistance are also emerging, leading
to multidrug resistance and threatening to create
panresistant species.
OVERVIEW OF RESISTANCE TRENDS
AND OUTCOMES
Third-generation cephalosporins were originally
developed as b-lactams able to overcome resistance
caused by common b-lactamases. When first intro-
duced, third-generation agents like ceftriaxone, cefo-
taxime, and ceftazidime were stable in the presence
of common b-lactamases. However, within a few years,
hospital-acquired gram-negative bacilli like Klebsiella
pneumoniae and others began producing mutated ver-
sions of these b-lactamases that made them resistant
to third-generation cephalosporins and to the mono-
bactam aztreonam. According to the National Nosoco-
mial Infections Surveillance (NNIS) System report, in
2003, 20.6% of all K pneumoniae isolates from patients
in intensive care units (ICUs) in the United States were
nonsusceptible to third-generation cephalosporins.1
This represented a 47% increase compared with resis-
tance rates for 1998 to 2002. Nonsusceptibility to third-
generation cephalosporins was also observed in
31.1%ofEnterobacter spp and 5.8% ofE coliisolated from pa-
tients in ICUs in 2003. Those rates were approximately
the same as for 1998 to 2002. International studies re-
port even higher rates of nonsusceptible K pneumoniaein
hospitals and particularly in ICU settings.2
From the Antibiotic Management Program, University of
PittsburghMedical Center, Pittsburgh, PA.
Reprint requests: David L. Paterson, MD, PhD, Suite 3A, Falk
MedicalBuilding, 3601 5th Avenue, Pittsburgh, Pennsylvania 15213.
E-mail:[email protected].
0196-6553/$32.00
Copyright 2006 by the Association for Professionals in
InfectionControl and Epidemiology, Inc. and Elsevier, Inc.
doi:10.1016/j.ajic.2006.05.238
S20
mailto:[email protected]:[email protected]
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
2/9
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
3/9
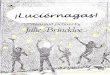
data suggested that an antibiotic MIC of 8 mg/mL was
universally associated with clinical failure and that
high rates of failure were also observed with a MIC of4 mg/mL
(Table 2).14 These results are consistent with
those from a variety of observational studies that
show rates of clinical failure .90%, approximately
67%, and,
30% with MICs of 8, 4, and #2 mg/mL, re-spectively.7,15 Whether
the susceptibility break points
of Enterobacteriaceae for cephalosporins should be
changed is currently under consideration. The 2005
CLSI guidelines recommend that laboratories report
ESBL-producing isolates as resistant to all penicillins,
cephalosporins, and aztreonam irrespective of in vitro
tests results.16 The presence of inadequately identified
ESBL producers has important implications for both
antibiotic therapy and infection control.
Treatment of ESBL producers
The presence of ESBL-producing Enterobacteriaceae
complicates therapy, especially because these orga-
nisms are often multidrug resistant. When isolates from
a patient indicate an ESBL-producing organism, the
first thing to consider is whether the patient has a
true infection. Patients with positive isolates from urine
or perhaps the respiratory tract may be only colonized,
and clearly, there is no indication for treatment in those
situations. Assuming the patient has a serious infection
due to ESBL-producing Enterobacteriaceae, the choice
of empiric therapy is made difficult by the likelihood
of multidrug resistance and the fact that there are no
data from large, randomized, controlled trials designed
to compare one antibiotic therapy with another for in-
fections caused by ESBL-producing organisms. More-
over, for a variety of reasons, it is unlikely that such astudy
will ever be performed. Nonetheless, data from
a number of studies strongly point to carbapenems as
the drugs of choice for empiric treatment of serious in-
fections involving ESBL-producing Enterobacteriaceae.
Subgroup analysis from a randomized, evaluator-
blind trial comparing cefepime with imipenem in
patients with nosocomial pneumonia showed that
100% of patients (10 of 10) receiving imipenem for
pneumonia caused by an ESBL producer experienced
a positive clinical response compared with only 69%
of patients (9 of 13) treated with cefepime.17 Similarly,
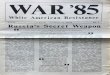
Table 1. Selected b-lactamases of gram-negative bacteria
b-Lactamase Examples Substrates
Inhibition by
clavulanate*
Molecular
class
Broad-spectrum TEM-1, TEM-2, SHV-1 Penicillin G,
aminopenicillins, carboxypenicillins,
piperacillin, narrow-spectrum cephalosporins
111 A
OXA family Substrates of the broad-spectrum group
pluscloxacillin, methicillin, and oxacillin
1
D
Extended-spectrum TEM family, SHV family Substrates of the
broad-spectrum group plus
oxyimino-cephalosporins, and monobactam (aztreonam)
1111 A
CTX-M family Substrates of the expanded-spectrum group plus,
for some enzymes, cefepime
1111 A
OXA family Same as for CTX-M family 1 D
Others (PER-1, PER-2, BES-1,
GES/IBC family, SFO-1, TLA-1,
VEB-1, VEB-2)
Same as for TEM family and SHV family 1111 A
AmpC ACC-1, ACT-1, CFE-1, CMY family,
DHA-2, FOX family, LAT family,
MIR-1, MOX-1, MOX-2
Substrates of expanded-spectrum group plus cephamycins 0 C
Carbapenemase IMP family, VIM family, GIM-1, SPM-1
(metallo-b-enzymes)
Substrates of the expanded-spectrum group plus
cephamycins and carbapenems
0 B
KPC-1, KPC-2, KPC-3 Same as for IMP family, VIM family, GIM-1,
and SPM-1 111 AOXA-23, OXA-24, OXA-25, OXA-26,
OXA-27, OXA-40, OXA-48
Same as for IMP family, VIM family, GIM-1, and SPM-1 1 D
Adapted from N Engl J Mea.10
*1, 111, and 1111 denote relative sensitivity to inhibition.
Table 2. Outcome of cephalosporin treatment of seriousinfections
due to extended-spectrum b-lactamaseproducing organisms
Patients % (n)
MIC (mg/mL)
Experienced failure of
cephalosporin therapy
Died of bacteremia
within 14 days
8 100 (6/6) 33 (2/6)
4 67 (2/3) 0 (0/3)
2 33 (1/3) 0 (0/3)
#1 27 (3/11) 18 (2/11)
Total* 54 (15/28)
MIC, minimum inhibitory concentration.
Adapted from J Clin Microbio.14
*Includes 5 patients with isolates for which MICs were recorded
simply as 0.5 to
4 mg/L.
S22 Vol. 34 No. 5 Supplement 1 Paterson
http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
4/9
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
5/9
Nonetheless, the healthcare community needs to be
aware of the potential problem that CA-ESBL producers
may present in the United States in the future, espe-
cially given what has been observed in the United King-
dom and Canada. It suggests that attention be focused
on potential risk factors for community development
of infection with ESBL-producing bacteria. In a Spanishstudy,
those risk factors included diabetes mellitus, pre-
vious quinolone use, recurrent UTIs, a previous hospi-
tal admission, and older age in male patients.30 An
Israeli study identified risk factors as previous hospital-
ization within the past 3 months, antibiotic treatment
within the past 3 months, age .60 years, male sex,
K pneumoniae infection, previous use of third-genera-
tion cephalosporins, previous use of second-genera-
tion cephalosporins, previous use of quinolones, and
previous use of penicillin.28 Although both studies
identified previous hospitalization as a risk factor, it
should be noted that cases of infection with an ESBL-producing
organism in the community have been
reported in patients without recent hospitalization.
So, cases of true CA-ESBL producers have been docu-
mented. As mentioned previously, ESBL-producing
pathogens may also be involved in gastrointestinal in-
fections acquired in the community. Bacterial species
that have been reported to produce ESBLs leading to
drug-resistant gastroenteritis include Salmonella spp,
Shigella, Vibrio cholerae, and Shiga toxinproducing
E coli.29,32-37 The possible emergence and spread of
Salmonella strains resistant to antibiotics commonly
used as treatment are concerns, because theseinfections can be
invasive. Outside the United States,
TEM-, SHV-, and CTX-M-type ESBLs, as well as AmpC
b-lactamases, have been identified in infection-causing
Salmonella.29,32,38 Within the United States, the mecha-nism
ofSalmonella resistance to third-generation ceph-
alosporins has been linked to production of AmpC
b-lactamases.39-41 In particular, resistance has been as-
sociated with the plasmid-mediated AmpCb-lactamase
known as CMY-2. Salmonella strains resistant to third-
generation cephalosporins are of concern because (1)
ceftriaxone and, secondarily, quinolones are the drugs
of choice for invasive salmonella disease, and (2) quino-
lones are not indicated for use in children. Fortunately,
ceftriaxone-resistant Salmonella are currently rare in
the United States, but they represent an area that bears
further watching.
ANTIBIOTIC RESISTANCE IN ENTEROBACTERSPECIES
Enterobacter spp are significant causes of nosoco-
mial infection and are intrinsically resistant to amino-
penicillins, cefazolin, and cefoxitin due to production
of constitutive chromosomal AmpC b-lactamases.42
Moreover, b-lactam exposure is capable of inducing
expression of AmpCb-lactamases inEnterobacter spp
with consequent resistance to third-generation cepha-
losporinsand mutations may result in permanent
hyperproduction and persistent resistance. Treatment
of Enterobacter infections with third-generation ceph-
alosporins may select for mutant strains associatedwith
hyperproduction of AmpC b-lactamase. The prev-
alence ofEnterobacter spp resistant to third-generation
cephalosporins has increased since the introduction
and common use of these antibiotics. For example, in
1 study, resistance to third-generation cephalosporins
emerged in approximately 20% of patients during
treatment for Enterobacter bacteremia.43 Multidrug-
resistant Enterobacter spp in initial positive blood
cultures were significantly more prevalent (P, .001)
among patients who had previously received third-
generation cephalosporins than among patients who
had previously received other antibiotic treatments,and they
were associated with higher mortality rates.43
In summary, third-generation cephalosporins should
be avoided as treatment forserious infection withEnter-
obacter spp because their use in such situations results
in selection of the small number of AmpC-overproduc-
ing mutants present in any collection ofEnterobacterspp isolates
and because the typical clinical scenario
is characterized by initial response followed by recur-
rence of infection. In contrast, cefepime is compar-
atively stable to AmpC b-lactamases, and therefore
has been regarded as a suitable option for treatment
ofEnterobacter infections.
42
However, ESBL-producingEnterobacter spp, particularly
Enterobacter cloacae,
have been identified in the United States (Table 1),44-46
Europe,47 and Asia.48-50 At our medical center in Pitts-
burgh, approximately 33% of bloodstream isolates havebeen shown
to contain E cloacae that produce ESBL
as well as AmpC b-lactamases.51 The MIC of cefepime
may be within that danger zone of 48 mg/mL, where
cephalosporin activity may be compromised. Hence,
not all resistance to later-generation cephalospo-
rins in E cloacae may be the result of hyperpro-
duction of AmpC b-lactamases, and ESBL-producing
strains of E cloacae may be resistant to fourth- as well
as third-generation cephalosporins. The advent of
ESBLs in AmpC-producing E cloacae is certainly some-
thing to be aware of and is potentially clinically
important.
EMERGING QUINOLONE AND CARBAPENEMRESISTANCE
Quinolone resistance
Quinolones are used widely for the treatment of
serious E coliUTIs and may also be used to treat other
S24 Vol. 34 No. 5 Supplement 1 Paterson
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
6/9
infections caused by other members of the Enterobac-
teriaceae family.52,53 Hence, quinolone resistance in
Enterobacteriaceae may lead to treatment failures
and is a significant concern, as is the recent emergence
of plasmid-mediated resistance to quinolones. Accord-
ing to the 2004 NNIS report, means of 7.3% and 8.2%
ofE coliisolates from US patients in both ICUs and non-ICU areas
of hospitals, respectively, and a mean of
3.6% from US outpatients exhibited quinolone resis-
tance.1 Higher rates of quinolone resistance may be
found in ESBL-producing strains of E coli and K pneu-
moniae. For example, 55.8% of infections in the Uni-
versity of Pennsylvania Health System caused by
ESBL-producing E colior K pneumoniae were fluoroqui-
nolone resistant.21 In Shanghai, China, 86.1% of ESBL-
producing E coliand 45.6% of ESBL-producing K pneu-
moniae were reported to be resistant to levofloxacin.54
We studiedK pneumoniae bacteremia from 12 hospitals
in 7 countries and found that overall, 18% of ESBL-pro-ducing
isolates were ciprofloxacin resistant and60% of
ciprofloxacin-resistant isolates produced ESBLs.55 Prior
receipt of a quinolone has been shown to be an inde-
pendent risk factor for quinolone resistance.21,55
Quinolone resistance in Enterobacteriaceae is usu-
ally due to alterations in target enzymes (DNA gyrase
and/or topoisomerase IV) or to impaired access to the
target enzymes, occurring either because of changes
in porin expression or because of efflux mecha-
nisms.56 Both of these principal means of resistance
are caused by chromosomal mutations. More recently,
plasmid-mediated quinolone resistance has emergedin K pneumoniae
and E coli. The first case of plasmid-
mediated resistance to quinolones in K pneumoniaewas reported in
the United States in 1998 and was
from a strain isolated at the University of Alabama in1994.57
The plasmid, pMG252, confers multidrug resis-
tance and was shown to greatly increase quinolone re-
sistance when transferred to strains of K pneumoniaedeficient in
outer-membrane porins. The gene asso-
ciated with that resistance has been designated qnr.
Quinolone resistance associated with qnr-containing
plasmids has now emerged in E coliand K pneumoniaestrains.58-60
A recent study in the United States re-
ported that 11.1% ofK pneumoniae strains from 6 states
exhibited plasmid-mediated quinolone resistance asso-
ciated with the qnr gene, although none of the E colistrains
examined contained qnr.61 Some of the strains
contained the original pMG252 plasmid, but qnr was
carried on different plasmids for others. The mech-
anism of quinolone resistance associated with qnr-
containing plasmids appears to involve inhibition of
quinolone binding with DNA gyrase.62
The emergence of this new plasmid-mediated
mechanism of quinolone resistance is particularly wor-
risome because it provides a mechanism for the rapid
development and spread of quinolone and multidrug
resistance to important members of the Enterobacteri-
aceae family.
Carbapenem resistance
As mentioned earlier, carbapenems are currentlyconsidered to be
the preferred agents for treatment of
serious infections caused by ESBL-producing Entero-
bacteriaceae. Carbapenems are highly stable tob-lacta-
mase hydrolysis, and porin penetration is facilitated
by their general size and structure. Their susceptibility
to most strains of Enterobacteriaceae makes them
generally useful as treatment for multidrug-resistant
organisms. Carbapenem resistance is currently rare
among Enterobacteriaceae, but some worrisome signs
have appeared in recent years.
The expression of AmpC or class A (TEM- or SHV-
type) ESBLs plus loss of outer-membrane proteinshave been
associated with carbapenem resistance in
K pneumoniae.63-68 Resistance to carbapenems has
also been reported in K pneumoniaeproducing class
B b-lactamases (metallo-b-lactamases) in various coun-
tries outside the United States, including Brazil,69
Greece,70 China,71 and Singapore.72 A metallo-b-lacta-
maseproducing strain ofE cloacae with reduced sus-
ceptibility to carbapenems has also recently been
observed in Greece.73 Standard susceptibility testing
may categorize metallo-b-lactamaseproducing Enter-
obacteriaceae as susceptible to carbapenems, but an
inoculum effect has been observed, suggesting thatthe
susceptibility testing may falsely predict the sus-
ceptibility of particular Enterobacteriaceae to carbape-
nems in the clinical environment.73,74
In the United States, carbapenem resistance has beenobserved in
strains ofK pneumoniaeproducing class A
carbapenemases, namely, KPC-1, KPC-2, and KPC-3.75-82
The genes encoding these enzymes are apparently
obtained via plasmid conjugation; the enzymes are ca-
pable of hydrolyzing and inactivating the carbapenems.
KPC-producing strains have generally been shown to
exhibit multidrug resistance that includes piperacillin/
tazobactam, third- and fourth-generation cephalospo-
rins, fluoroquinolones, and aminoglycosides, as well
as carbapenems.82 KPC-1 expression itself was appar-
ently associated with moderate- to high-level carbape-
nem resistance,75 while loss of outer-membrane
proteins appeared to be a required cofactor for high-
level resistance in KPC-2 and KPC-3producing
strains.76,78 In 96 isolates obtained from 10 New York
hospitals, .80% of the KPC-producing organisms be-
longed to a single ribotype.82 This is worrisome because
it suggests that these isolates are not just being selected
by antibiotic use, but rather are being passed from
person to person as a result of breakdown in infection
Paterson June 2006 S25
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
7/9
control. As with metallo-b-lactamaseproducing Enter-
obacteriaceae, susceptibility testing may falsely indi-
cate the clinical susceptibility of KPC-producing
K pneumoniae due to an inoculum effect.79-81 In vitro
testing suggests that tigecycline and polymyxins
may exhibit the most consistent activity against KPC-
producing strains of K pneumoniae, but this has yet tobe
demonstrated clinically.82 KPC-producing strains of
Enterobacter81 and Salmonella spp83 have also been
identified in the United States.
Strains of clinically important Enterobacteriaceae
have now emerged with broader multidrug resistance
than has ever before been observed. As the list of anti-
biotics with potential activity against these strains
continues to shrink, measures that prevent and slow
the spread of multidrug-resistant Enterobacteriaceae
strains throughout the world must be put into action.
SUMMARY
Enterobacteriaceae are significant causes of serious
infections, and many of the most important members
of this family are becoming increasingly resistant to
currently available antibiotics. This is a troubling trend,
and one that requires vigilance and intensified mea-sures to
control the further spread of resistance by
these important gram-negative pathogens. Although
improvements in antibiotic stewardship and infection
control are discussed in greater detail by others in
this supplement, it should be emphasized that such im-
provements are necessary if the steady rise in ESBL-producing
Enterobacteriaceae and in other forms of
resistance in these species is to be slowed or stopped.
The widespread use of third-generation cephalospo-
rins as the driving force behind the emergence of
ESBL-producing organisms has been shown in many
studies. Because of that risk, third-generation cephalo-
sporins are no longer appropriate as workhorse anti-
biotics in our hospitals, and the restriction of their
use in hospitals and other healthcare facilities has
been shown to reduce the incidence of ESBL-producing
Enterobacteriaceae like K pneumoniae. Quinolones
seem to have replaced third-generation cephalosporins
in hospitals, yet their overuse, particularly in light of
plasmid-mediated quinolone resistance in Enterobac-
teriaceae, may be of concern.
Infection control is the second aspect in restriction
of the emergence and spread of resistant Enterobacte-
riaceae. With regard to ESBL producers, there is ample
evidence of person-to-person spread. Combining re-
ductions in third-generation cephalosporin use with
traditional infection control measuressuch as the
use of gloves, gowns, and hand hygiene in the care
of colonized or infected patientshas been reported
to control the hospital spread of multidrug-resistant
K pneumoniae. Both improvement in antibiotic stew-
ardship and infection control strategies are needed
before it is too latebefore we have to deal with infec-
tions caused by multidrug-resistant Enterobacteriaceae
for which there are no clinically effective drugs.
References
1. National Nosocomial Infections Surveillance (NNIS) System
Report,
data summary from January 1992 through June 2004, issued
October
2004. Am J Infect Control 2004;32:470-85.
2. Paterson DL, Ko WC, Von Gottberg A, et al. International
prospec-
tive study of Klebsiella pneumoniae bacteremia: implications
of
extended-spectrum beta-lactamase production in nosocomial
Infec-
tions. Ann Intern Med 2004;140:26-32.
3. Rupp ME, Fey PD. Extended spectrum beta-lactamase
(ESBL)-produc-
ing Enterobacteriaceae: considerations for diagnosis,
prevention,
and drug treatment. Drugs 2003;63:353-65.
4. Shah AA, Hasan F, Ahmed S, Hameed A. Extended-spectrum
beta-
lactamases (ESBLs): characterization, epidemiology, and
detection.
Crit Rev Microbiol 2004;30:25-32.5. Kollef MH, Sherman G, Ward
S, Fraser VJ. Inadequate antimicrobial
treatment of infections: a risk factor for hospital mortality
among crit-
ically ill patients. Chest 1999;115:462-74.
6. Du B, Long Y, Liu H, et al. Extended-spectrum
beta-lactamase-produc-
ing Escherichia coli and Klebsiella pneumoniae bloodstream
infection:
risk factors and clinical outcome. Intensive Care Med
2002;28:
1718-23.
7. Paterson DL, Ko WC, Von Gottberg A, et al. Antibiotic therapy
for
Klebsiella pneumoniae bacteremia: implications of production of
ex-
tended-spectrum beta-lactamases. Clin Infect Dis
2004;39:31-7.
8. Bradford PA. Extended-spectrum beta-lactamases in the 21st
century:
characterization, epidemiology, and detection of this important
resis-
tance threat. Clin Microbiol Rev 2001;14:933-51, table of
contents.
9. Walther-Rasmussen J, Hoiby N. Cefotaximases (CTX-M-ases), an
ex-
panding family of extended-spectrum beta-lactamases. Can J
Microbiol
2004;50:137-65.
10. Jacoby GA, Munoz-Price LS. The new beta-lactamases. N Engl J
Med
2005;352:380-91.
11. Walsh TR, Toleman MA, Poirel L, Nordmann P.
Metallo-beta-lacta-
mases: the quiet before the storm? Clin Microbiol Rev
2005;18:
306-25.
12. Thomson KS, Moland ES. Cefepime, piperacillin-tazobactam,
and the
inoculum effect in tests with extended-spectrum
beta-lactamase-pro-
ducing Enterobacteriaceae. Antimicrob Agents Chemother
2001;45:
3548-54.
13. Jett BD, Ritchie DJ, Reichley R, Bailey TC, Sahm DF. In
vitro activities
of various beta-lactam antimicrobial agents against clinical
isolates of
Escherichia coliand Klebsiella spp. resistant to oxyimino
cephalosporins.
Antimicrob Agents Chemother 1995;39:1187-90.14. Paterson DL, Ko
WC, Von Gottberg A, et al. Outcome of cephalospo-
rin treatment for serious infections due to apparently
susceptible
organisms producing extended-spectrum beta-lactamases:
implications
for the clinical microbiology laboratory. J Clin Microbiol
2001;39:
2206-12.
15. Wong-Beringer A, Hindler J, Loeloff M, et al. Molecular
correlation
for the treatment outcomes in bloodstream infections caused
by
Escherichia coli and Klebsiella pneumoniae with reduced
susceptibility
to ceftazidime. Clin Infect Dis 2002;34:135-46.
16. Data on file. Performance standards for antimicrobial
susceptibility
testing; fifteenth informational supplement. Wayne, PA: Clinical
and
Laboratory Standards Institute; 2005.
17. Zanetti G, Bally F, Greub G, et al. Cefepime versus
imipenem-cilastatin
for treatment of nosocomial pneumonia in intensive care unit
patients:
S26 Vol. 34 No. 5 Supplement 1 Paterson
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
8/9
a multicenter, evaluator-blind, prospective, randomized study.
Antimi-
crob Agents Chemother 2003;47:3442-7.
18. Alvarez M, Tran JH, Chow N, Jacoby GA. Epidemiology of
conjugative
plasmid-mediated AmpC beta-lactamases in the United States.
Antimi-
crob Agents Chemother 2004;48:533-7.
19. Tracz DM, Boyd DA, Bryden L, et al. Increase in AmpC
promoter
strength due to mutations and deletion of the attenuator in a
clinical
isolate of cefoxitin-resistant Escherichia coli as determined by
RT-PCR.J Antimicrob Chemother 2005;55:768-72.
20. Martinez-Martinez L, Hernandez-Alles S, Alberti S, Tomas JM,
Benedi
VJ, Jacoby GA. In vivo selection of porin-deficient mutants
ofKlebsiella
pneumoniae with increased resistance to cefoxitin and
expanded-spec-
trum-cephalosporins. Antimicrob Agents Chemother
1996;40:342-8.
21. Lautenbach E, Strom BL, Bilker WB, Patel JB, Edelstein PH,
Fishman
NO. Epidemiological investigation of fluoroquinolone resistance
in
infections due to extended-spectrum beta-lactamase-producing
Esche-
richia coli and Klebsiella pneumoniae. Clin Infect Dis
2001;33:1288-94.
22. DiPersio JR, Deshpande LM, Biedenbach DJ, Toleman MA, Walsh
TR,
Jones RN. Evolution and dissemination of extended-spectrum
beta-
lactamase-producing Klebsiella pneumoniae: epidemiology and
molecu-
lar report from the SENTRY Antimicrobial Surveillance
Program
(19972003). Diagn Microbiol Infect Dis 2005;51:1-7.
23. Hyle EP, Lipworth AD, Zaoutis TE, et al. Risk factors for
increasing mul-tidrug resistance among extended-spectrum
beta-lactamase-producing
Escherichia coliand Klebsiella species. Clin Infect Dis
2005;40:1317-24.
24. Pitout JD, Nordmann P, Laupland KB, Poirel L. Emergence of
Entero-
bacteriaceae producing extended-spectrum b-lactamases (ESBLs)
in
the community. J Antimicrob Chemother 2005;56:52-9.
25. Pitout JD, Hanson ND, Church DL, Laupland KB.
Population-based
laboratory surveillance for Escherichia coli-producing
extended-spec-
trum beta-lactamases: importance of community isolates with
blaCTX-M genes. Clin Infect Dis 2004;38:1736-41.
26. Moland ES, Black JA, Hossain A, Hanson ND, Thomson KS,
Pottumar-
thy S. Discovery of CTX-M-like extended-spectrum
beta-lactamases
in Escherichia coli isolates from 5 US States. Antimicrob Agents
Che-
mother 2003;47:2382-3.
27. Paterson DL, Hujer KM, Hujer AM, et al. Extended-spectrum
beta-
lactamases in Klebsiella pneumoniae bloodstream isolates from
7
countries: dominance and widespread prevalence of SHV- and
CTX-
M-type beta-lactamases. Antimicrob Agents Chemother 2003;47:
3554-60.
28. Colodner R, Rock W, Chazan B, et al. Risk factors for the
develop-
ment of extended-spectrum beta-lactamase-producing bacteria
in
nonhospitalized patients. Eur J Clin Microbiol Infect Dis
2004;23:
163-7.
29. Munday CJ, Whitehead GM, Todd NJ, Campbell M, Hawkey PM.
Pre-
dominance and genetic diversity of community- and
hospital-acquired
CTX-M extended-spectrum beta-lactamases in York, UK. J
Antimi-
crob Chemother 2004;54:628-33.
30. Rodriguez-Bano J, Navarro MD, Romero L, et al. Epidemiology
and
clinical features of infections caused by extended-spectrum
beta-lacta-
mase-producing Escherichia coli in nonhospitalized patients. J
ClinMicrobiol 2004;42:1089-94.
31. Woodford N, Ward ME, Kaufmann ME, et al. Community and
hospital
spread of Escherichia coli producing CTX-M extended-spectrum
beta-
lactamases in the UK. J Antimicrob Chemother 2004;54:735-43.
32. Kruger T, Szabo D, Keddy KH, et al. Infections with
nontyphoidal Sal-
monella species producing TEM-63 or a novel TEM enzyme,
TEM-131,
in South Africa. Antimicrob Agents Chemother
2004;48:4263-70.
33. Ishii Y, Kimura S, Alba J, et al. Extended-spectrum
beta-lactamase-
producing Shiga toxin gene (Stx1)-positive Escherichia coli
O26:H11:
a new concern. J Clin Microbiol 2005;43:1072-5.
34. Kim S, Kim J, Kang Y, Park Y, Lee B. Occurrence of
extended-spec-
trum beta-lactamases in members of the genus Shigella in the
Republic
of Korea. J Clin Microbiol 2004;42:5264-9.
35. Petroni A, Corso A, Melano R, et al. Plasmidic
extended-spectrum
beta-lactamases in Vibrio cholerae O1 El Tor isolates in
Argentina.
Antimicrob Agents Chemother 2002;46:1462-8.
36. Radice M, Gonzealez C, Power P, Vidal MC, Gutkind G.
Third-gener-
ation cephalosporin resistance in Shigella sonnei, Argentina.
Emerg
Infect Dis 2001;7:442-3.
37. Vignoli R, Varela G, Mota MI, et al. Enteropathogenic
Escherichia coli
strains carrying genes encoding the PER-2 and TEM-116
extended-spectrum beta-lactamases isolated from children with
diarrhea in
Uruguay. J Clin Microbiol 2005;43:2940-3.
38. Li WC, Huang FY, Liu CP, et al. Ceftriaxone resistance of
nontyphoidal
Salmonella enterica isolates in Northern Taiwan attributable to
produc-
tion of CTX-M-14 and CMY-2 b-lactamases. J Clin Microbiol
2005;43:
3237-43.
39. Carattoli A, Tosini F, Giles WP, et al. Characterization of
plasmids car-
rying CMY-2 from expanded-spectrum cephalosporin-resistant
Salmo-
nella strains isolated in the United States between 1996 and
1998.
Antimicrob Agents Chemother 2002;46:1269-72.
40. Dunne EF, Fey PD, Kludt P, et al. Emergence of domestically
acquired
ceftriaxone-resistant Salmonella infections associated with
AmpC
beta-lactamase. JAM 2000;284:3151-6.
41. Fey PD, Safranek TJ, Rupp ME, et al. Ceftriaxone-resistant
salmonella
infection acquired by a child from cattle. N Engl J Med
2000;342:1242-9.
42. Bouza E, Cercenado E. Klebsiella and Enterobacter:
antibiotic resistance
and treatment implications. Semin Respir Infect
2002;17:215-30.
43. Chow JW, Fine MJ, Shlaes DM, et al. Enterobacter bacteremia:
clinical
features and emergence of antibiotic resistance during therapy.
Ann
Intern Med 1991;115:585-90.
44. Levison ME, Mailapur YV, Pradhan SK, et al. Regional
occurrence of
plasmid-mediated SHV-7, an extended-spectrum beta-lactamase,
in
Enterobacter cloacae in Philadelphia Teaching Hospitals. Clin
Infect
Dis 2002;35:1551-4.
45. Sanders CC, Ehrhardt AF, Moland ES, Thomson KS, Zimmer B,
Roe
DE. BetalasEN: microdilution panel for identifying
beta-lactamases pre-
sent in isolates of Enterobacteriaceae. J Clin Microbiol
2002;40:123-7.
46. DAgata E, Venkataraman L, DeGirolami P, Weigel L, Samore
M,
Tenover F. The molecular and clinical epidemiology of
Enterobacte-
riaceae producing extended-spectrum beta-lactamase in a
tertiary
care hospital. J Infect 1998;36:279-85.
47. Tzelepi E, Giakkoupi P, Sofianou D, Loukova V, Kemeroglou A,
Tsakris
A. Detection of extended-spectrum beta-lactamases in clinical
isolates
of Enterobacter cloacae and Enterobacter aerogenes. J Clin
Microbiol
2000;38:542-6.
48. Park YJ, Park SY, Oh EJ, et al. Occurrence of
extended-spectrum beta-
lactamases among chromosomal AmpC-producing Enterobacter
cloacae,
Citrobacter freundii, and Serratia marcescens in Korea and
investigation of
screening criteria. Diagn Microbiol Infect Dis
2005;51:265-9.
49. Jiang X, Ni Y, Jiang Y, et al. Outbreak of infection caused
by Enterobac-
ter cloacae producing the novel VEB-3 beta-lactamase in China. J
Clin
Microbiol 2005;43:826-31.
50. Pai H, Hong JY, Byeon JH, Kim YK, Lee HJ. High prevalence
ofextended-spectrum beta-lactamase-producing strains among
blood
isolates of Enterobacter spp. collected in a tertiary hospital
during an
8-year period and their antimicrobial susceptibility patterns.
Anti-
microb Agents Chemother 2004;48:3159-61.
51. Szabo D, Bonomo RA, Silveira F, et al. SHV-type
extended-spectrum
beta-lactamase production is associated with reduced cefepime
sus-
ceptibility in Enterobacter cloacae. J Clin Microbiol
2005;43:5058-64.
52. Carson C, Naber KG. Role of fluoroquinolones in the
treatment of
serious bacterial urinary tract infections. Drugs
2004;64:1359-73.
53. Hooper DC. Clinical applications of quinolones. Biochim
Biophys Acta
1998;1400:45-61.
54. Xiong Z, Zhu D, Wang F, Zhang Y, Okamoto R, Inoue M.
Investigation
of extended-spectrum beta-lactamase in Klebsiellae pneumoniae
and
Paterson June 2006 S27
-
7/28/2019 Resist%EAncia Enterobact%E9rias Paterson
9/9
Escherichia coli from China. Diagn Microbiol Infect Dis
2002;44:
195-200.
55. Paterson DL, Mulazimoglu L, Casellas JM, et al. Epidemiology
of cipro-
floxacin resistance and its relationship to extended-spectrum
beta-
lactamase production in Klebsiella pneumoniae isolates
causing
bacteremia. Clin Infect Dis 2000;30:473-8.
56. Hooper DC. Mechanisms of fluoroquinolone resistance. Drug
Resist
Updat 1999;2:38-55.57. Martinez-Martinez L, Pascual A, Jacoby
GA. Quinolone resistance
from a transferable plasmid. Lancet 1998;351:797-9.
58. Wang M, Tran JH, Jacoby GA, Zhang Y, Wang F, Hooper DC.
Plasmid-
mediated quinolone resistance in clinical isolates of
Escherichia coli
from Shanghai, China. Antimicrob Agents Chemother
2003;47:2242-8.
59. Mammeri H, Van De Loo M, Poirel L, Martinez-Martinez L,
Nordmann
P. Emergence of plasmid-mediated quinolone resistance in
Escherichia
coli in Europe. Antimicrob Agents Chemother 2005;49:71-6.
60. Rodriguez-Martinez JM, Pascual A, Garcia I,
Martinez-Martinez L.
Detection of the plasmid-mediated quinolone resistance
determinant
qnr among clinical isolates of Klebsiella pneumoniae producing
AmpC-
type beta-lactamase. J Antimicrob Chemother 2003;52:703-6.
61. Wang M, Sahm DF, Jacoby GA, Hooper DC. Emerging
plasmid-medi-
ated quinolone resistance associated with the qnr gene in
Klebsiella
pneumoniae clinical isolates in the United States. Antimicrob
AgentsChemother 2004;48:1295-9.
62. Tran JH, Jacoby GA. Mechanism of plasmid-mediated
quinolone
resistance. Proc Natl Acad Sci U S A 2002;99:5638-42.
63. Bornet C, Davin-Regli A, Bosi C, Pages JM, Bollet C.
Imipenem resis-
tance of Enterobacter aerogenes mediated by outer membrane
perme-
ability. J Clin Microbiol 2000;38:1048-52.
64. de Champs C, Henquell C, Guelon D, Sirot D, Gazuy N, Sirot
J. Clin-
ical and bacteriological study of nosocomial infections due to
Entero-
bacter aerogenes resistant to imipenem. J Clin Microbiol
1993;31:123-7.
65. Chow JW, Shlaes DM. Imipenem resistance associated with the
loss of
a 40 kDa outer membrane protein in Enterobacter aerogenes. J
Antimi-
crob Chemother 1991;28:499-504.
66. Poirel L, Heritier C, Tolun V, Nordmann P. Emergence of
oxacillinase-
mediated resistance to imipenem in Klebsiella pneumoniae.
Antimicrob
Agents Chemother 2004;48:15-22.
67. Martinez-Martinez L, Pascual A, Hernandez-Alles S, et al.
Roles of
beta-lactamases and porins in activities of carbapenems and
cephalo-
sporins against Klebsiella pneumoniae. Antimicrob Agents
Chemother
1999;43:1669-73.
68. Bradford PA, Urban C, Mariano N, Projan SJ, Rahal JJ, Bush
K. Imi-
penem resistance in Klebsiella pneumoniae is associated with the
com-
bination of ACT-1, a plasmid-mediated AmpC beta-lactamase, and
the
loss of an outer membrane protein. Antimicrob Agents
Chemother
1997;41:563-9.
69. Lincopan N, McCulloch JA, Reinert C, Cassettari VC, Gales
AC,
Mamizuka EM. First isolation of
metallo-beta-lactamase-producing
multiresistant Klebsiella pneumoniae from a patient in Brazil. J
Clin
Microbiol 2005;43:516-9.
70. Giakkoupi P, Xanthaki A, Kanelopoulou M, et al. VIM-1
Metallo-beta-
lactamase-producing Klebsiella pneumoniae strains in Greek
hospitals.
J Clin Microbiol 2003;41:3893-6.
71. Yan JJ, Ko WC, Tsai SH, Wu HM, Wu JJ. Outbreak of infection
with
multidrug-resistant Klebsiella pneumoniae carrying bla(IMP-8) in
a
university medical center in Taiwan. J Clin Microbiol
2001;39:
4433-9.
72. Koh TH, Sng LH, Babini GS, Woodford N, Livermore DM, Hall
LM.Carbapenem-resistant Klebsiella pneumoniae in Singapore
producing
IMP-1 beta-lactamase and lacking an outer membrane protein.
Antimi-
crob Agents Chemother 2001;45:1939-40.
73. Galani I, Souli M, Chryssouli Z, Orlandou K, Giamarellou H.
Charac-
terization of a new integron containing bla(VIM-1) and aac(6
9)-IIc in an
Enterobacter cloacae clinical isolate from Greece. J Antimicrob
Chemo-
ther 2005;55:634-8.
74. Giakkoupi P, Tzouvelekis LS, Daikos GL, et al. Discrepancies
and inter-
pretation problems in susceptibility testing of VIM-1-producing
Klebsi-
ella pneumoniae isolates. J Clin Microbiol 2005;43:494-6.
75. Yigit H, Queenan AM, Anderson GJ, et al. Novel
carbapenem-hydro-
lyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain
of
Klebsiella pneumoniae. Antimicrob Agents Chemother 2001;45:
1151-61.
76. Smith Moland E, Hanson ND, Herrera VL, et al.
Plasmid-mediated, car-bapenem-hydrolysing beta-lactamase, KPC-2, in
Klebsiella pneumoniae
isolates. J Antimicrob Chemother 2003;51:711-4.
77. Bradford PA, Bratu S, Urban C, et al. Emergence of
carbapenem-resis-
tant Klebsiella species possessing the class A
carbapenem-hydrolyzing
KPC-2 and inhibitor-resistant TEM-30 beta-lactamases in New
York
City. Clin Infect Dis 2004;39:55-60.
78. Woodford N, Tierno PM Jr, Young K, et al. Outbreak of
Klebsiella
pneumoniae producing a new carbapenem-hydrolyzing class A
beta-
lactamase, KPC-3, in a New York Medical Center. Antimicrob
Agents Chemother 2004;48:4793-9.
79. Bratu S, Landman D, Haag R, et al. Rapid spread of
carbapenem-resis-
tant Klebsiella pneumoniae in New York City: a new threat to
our
antibiotic armamentarium. Arch Intern Med 2005;165:1430-5.
80. Bratu S, Mooty M, Nichani S, et al. Emergence of
KPC-possessing
Klebsiella pneumoniae in Brooklyn, New York: epidemiology and
re-
commendations for detection. Antimicrob Agents Chemother
2005;
49:3018-20.
81. Bratu S, Landman D, Alam M, Tolentino E, Quale J. Detection
of KPC
carbapenem-hydrolyzing enzymes in Enterobacter spp. from
Brooklyn,
New York. Antimicrob Agents Chemother 2005;49:776-8.
82. Bratu S, Tolaney P, Karumudi U, et al.
Carbapenemase-producing Kleb-
siella pneumoniae in Brooklyn, NY: molecular epidemiology and in
vitro
activity of polymyxin B and other agents. J Antimicrob
Chemother
2005;56:128-32.
83. Miriagou V, Tzouvelekis LS, Rossiter S, Tzelepi E, Angulo
FJ, Whichard
JM. Imipenem resistance in a Salmonella clinical strain due to
plasmid-
mediated class A carbapenemase KPC-2. Antimicrob Agents
Chemo-
ther 2003;47:1297-300.
S28 Vol. 34 No. 5 Supplement 1 Paterson