Embed Size (px)
Citation preview

RESPIRATIONSCENTER VEST Århus Universitetshospital - Skejby
Ole Nørregaard
Januar 2013
Respiratory Center West
Respiratory Center East
Respiratory Center South

SKEJBY SYGEHUS

Respirationscenter Vest
har højt specialiseret funktion for • diagnostik, • behandling og • opfølgning af patienter med kronisk respirationsinsufficiens i bredeste forstand, herunder søvnrelaterede sygdomme.

Disposition
• RCV's historiske udvikling (incl. vækst)
• Epidemiologi
• Patofysiologi
• Diagnostik
• Hvornår henvisning til RCV ?
• Behandling – Ventilation
• Non-invasiv
• Invasiv (organisering, hjælperoplæring)

Historie:
• 1952 Polioepidemien
• 1954 Etablering af center på Blegdamshospitalet
• 1978 Flyttes til Rigshospitalet
• 1990 Sundhedsstyrelsens vejledning vedr. visitation og sygehusbehandling af patienter med kronisk respirationsinsufficiens.
• 1991 Respirationscentrene – RCV-RCØ

Historie: • 1991 RCV oprettes som en del af int.afd.N, ÅKH med 1-4 sengepladser • 1998 RCV etableres som selvstændigt afsnit med 4-7
sengepladser og ambulatorium • 2010 Sundhedsstyrelsens specialeudmelding for det
anæstesiologiske speciale definerer området som en højt specialiseret funktion.
• 1.6.11 RCV Skejby åbner med 8 sengepladser og udvidet ambulant funktion.

Afdelingen:
• 8 senge
– Enestuer med plads til hjælper/pårørende
• Søvnambulatorium
• Ambulatorium
• 24 timers
hotline funktion

Personale på RCV:
RCV
4 Overlæger
32 Syge-plejersker
5 SoSu-assistenter
Service-medarbejder
3 Sekretærer
Respirations
teamet –
3 socilal
rådgivere

Samarbejdspartnere Kompleks logistik kræver et bredt samarbejde
• Lægfolk (patienter, pårørende, hjælpere) • Leverandører af teknisk udstyr • Medicotekniske afdelinger • Sociale myndigheder • Patientforeninger • Kliniske afdelinger/praktiserende
læger/speciallæger • Respirationcenter Øst • Udenlandske centre

Patientkategorier: • Neuromuskulære sygdomme • Thoraxdeformiteter • Tetraplegi • Adipositasbetinget hypoventilation
• KOL • Cystisk fibrose
• Børn med syndromer og kroniske lungesygdomme (BPD)
• Søvnudløste respirationsforstyrrelser (SDB) • Søvnforstyrrelser







Duchenne’s muscular dystrophy --- National data
Start of the respiratory centers in Denmark

Patientudvikling (RCV)
0
500
1000
1500
2000
2500
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011

Home mechanical ventilation in Denmark (5 mill inhibitants)

• 240 ventilated via trachesostomy
• 1035 ventilated via mmask
• 81 % ventilated via NIV
• Respiratory Centre West (55% of the population): 20 % of ventilated individuals are children

Age distribution (percent)
0%
20%
40%
60%
80%
100%
ALL
Austria
Belgium
Den
mark
Finlan
dFra
nceG
ermany
Gree
ceIre
land
ItalyN
etherlan
ds
Norw
ayPolan
dPortug
alSp
ainSw
eden
UK
66 years +66 years +
26 – 65 yrs26 – 65 yrs
17 – 25 yrs17 – 25 yrs
16 or less16 or less


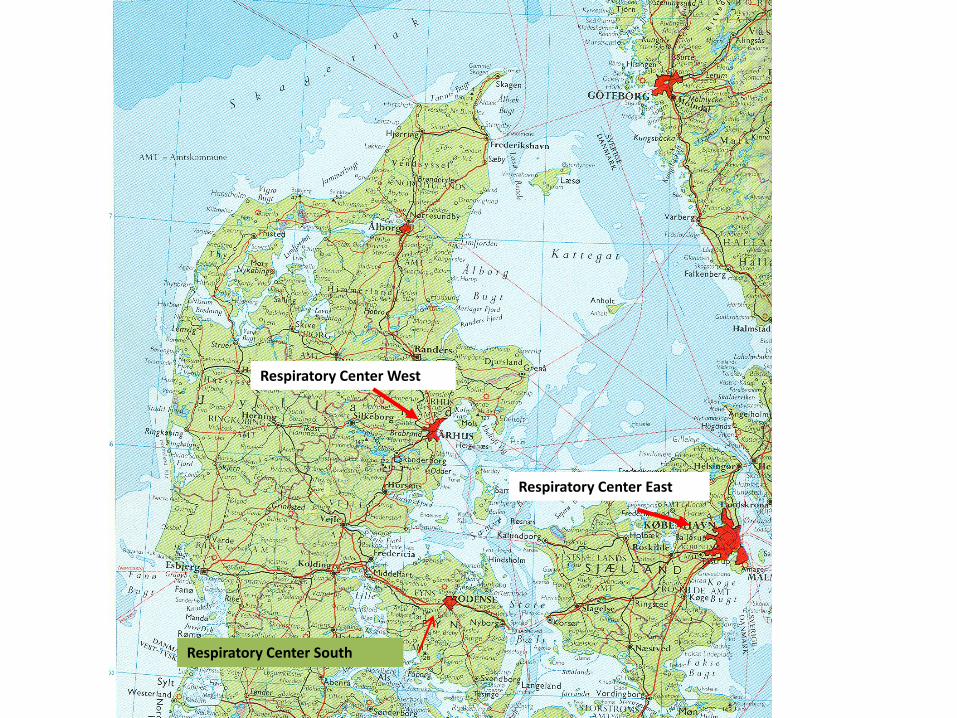
RESPIRATORY PHYSIOLOGY AND PATHOPHYSIOLOGY

Søvnudløste ventilationsændringer
SØVN
RESPIRATORISK KONTROL • Kemoreceptor følsomhed • Cortical input • Respiratoriske motorneuroner
RESPIRATORISK MUSKELFUNKTION •Intercostal •Diafragma •Accesesoriske
LUNGE-MEKANIK • Luftvejsmodstand • FRC • V/Q match




Raw - patophysiology
• Congenital malformations (laryngomalacia, epiglottic anomalies, tonsils, membraneous obstruction, vascular ring etc)
• tumor mediastini
• sekretions, foreign bodies
• age 1-3 years











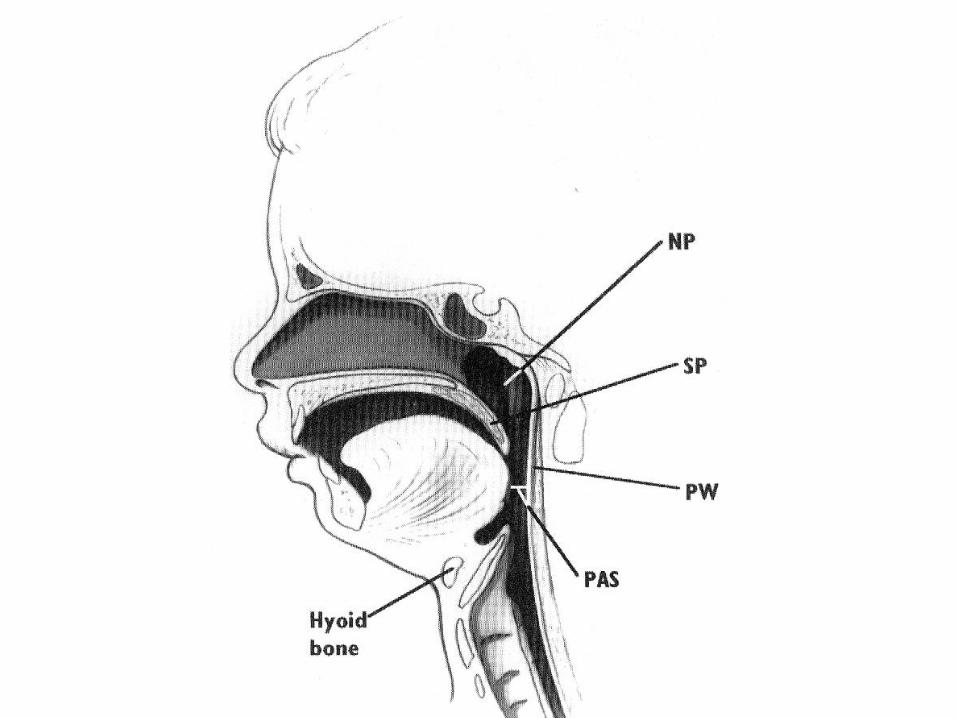
KARAKTERISTIKA
• Små dimensioner => luftvejsmodstand
• adenoide vegetationer & tonsiller
• compliant chest wall => paradoks respiration => energitab(wasted ventilation)
• horisontale costae
• immature muskler
• FRC => vulnerabel for hypoxæmi

KARAKTERISTIKA
• Alveolær ventilation:FRC hos små børn = 5.0:1.0, hos voksne 1.5:1.0
• Apnøer kraftigt REM-associerede
• hypoxæmisk respiratorisk respons svækkede hos små børn
• med alderen ofte aftagende compliance af thorax => øgning af det respiratoriske arbejde
KARAKTERISTIKA
• Neuromuskulær sygdom er oftest associeret med HYPERKAPNISK respirationsinsufficiens (i modsætning til hypoxæmisk)

Pediatric characteristics
• FRC very small (unmodified 15 % of TLC, 40 % modified)
• Modified with
– Expiratory breake
– High respiratory frequency
– Maintanence of muscular tone
• Periodic closure of the airways during tidal breathing





diagnostics
• Pulmonary function tests
• Pulse oxymetry
• cardio-respiratory monitoring (CRM)(flow, thoraco-abdominal movements, SaO2, CO2)
• polysomnography (PSG)(= CRM + sleep stages)
• SYMPTOMS



Cardiorespiratorisk monitorering (CRM)
Airflow
Chest- and abdominal movements
SaO2
tcCO2 EKG

CRM



Why PSG ??
• Document prescence of vulnerable (REM) sleep
• PSG determines diagnosis
• PSG can possibly identify differential diagnosis
• PSG can contribute to prognosis
• Evaluate severity
• Contributes to the evaluation of perioperative risc
• Determines base line for follow-up comparison


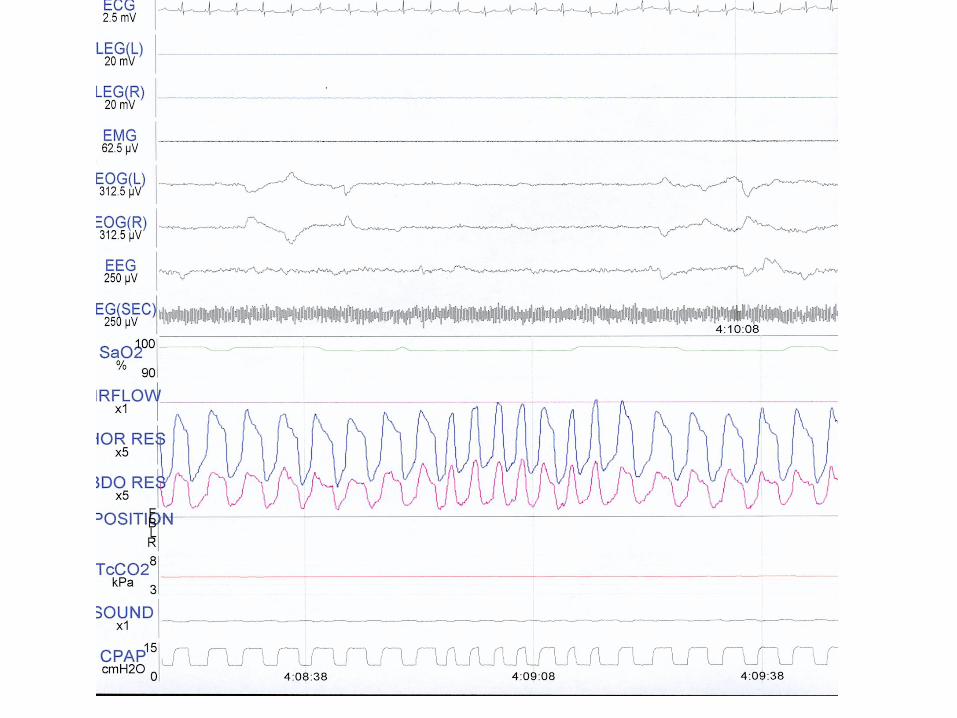
Polysomnografi(PSG)
Airflow
Chest- and abdominal movements
SaO2
tcCO2 EKG
EEG
Leg movements
EOG
EMG



Polysomnografi


HENVISNING TIL RESPIRATIONSCENTER
HVORNÅR ??

Physiological criteria
• Vital capacitet < 15 ml/kg
• PCEF < 2-3 l/sec (180 l/min) (Bach)
• PaCO2 > 6.0 kPa (45 mmHg)
• PaO2 < 9.3 kPa (70 mmHg)
• SaO2 < 97 % (on room air) Chest
1998;113:289S-344S

Indications for NIPPV (neuromuscular, restrictive a.o.)
• Symptoms (fatigue, dyspnea etc.)
• PaCO2 > 45 mmHg (6 kPa)
• Nocturnal desat. < 88% for 5 consecutive minutes
• Pimax < 60 cm H2O or FVC < 50% predicted
Chest, 1999;116:521

Referral of children
• signs and/or symptoms of nocturnal hypoventilation (NH) during the night
• daytime symptoms of NH
• failure to thrive

Referral of children
• IVC < 60 % (=> SBD, < 40% => noct hypovent)
• MIP < 4.0 kPa (=> SDB, < 2.5 => noct hypovent)
• CPF < 270 l/min
• Daytime PaCO2 > 45 mmHg (=> noct hypovent)

TREATMENT

Problems with NIPPV in children with neuromuscular disease
• Impaired ability to trigger in child =>
• child-ventilator dyssynchrony =>
• increased work of breathing
• discomfort, potentially =>
• poor compliance (treatment) (and thus)
• lack of effect
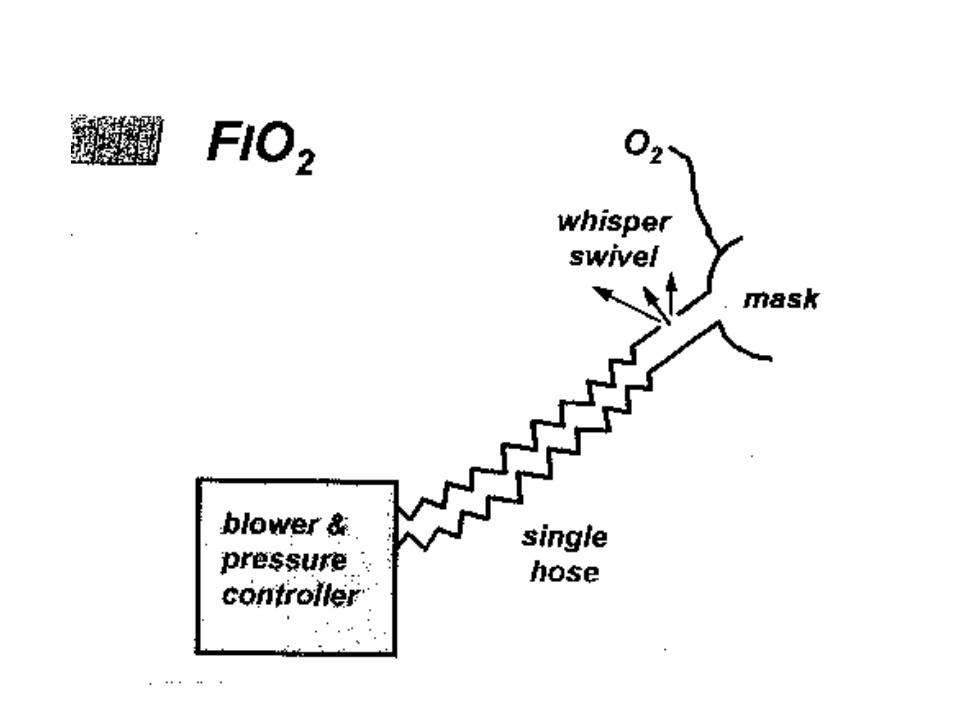


Choose the right interface and put it in the right position


Choose the right ventilator
• Trigger pressure (sensitivity, inspiratory and expiratory)
• Time delay
• Flow rise time
• Durability, noise, simpliticity in setting etc

Is it complicated
• Yes
• No

• Clinical mode
– VE , SaO2 , respiratory rate, patient comfort
• Scientific/invasive mode
– Clinical + Pes, Pga




Thorax
Abdomen
BiPAP
Figure 3

Long term/chronic setting

Simonds, Thorax 1998;53:949

• Method: record review
• N = 14 (DMD, cong myopathy, myoton dyst)
• Age 7.7 yrs (1.5 – 16)
• Treatment: BiPAP (reg tm)
– Settings: ?
– Duration: 30 mos (6 – 84)
– h/day: ?


Results
• Hospitalization:
– 41.7 days/y before treatment -> 10.5 days/y
– Number of hosp stays: 3.8/y - > 0.7/y
– PICU days: 10.2/y -> 2.3/y
• Annual direct cost og health care/patient
– $ 55.129 -> 14.914

• 30 patients aged 12.4 + 4.1 yrs
• IPAP/EPAP: 13.9 (8-19)/4.4 (3-8) cm H2O
• Ventilated for 25.3 (8-60) mos

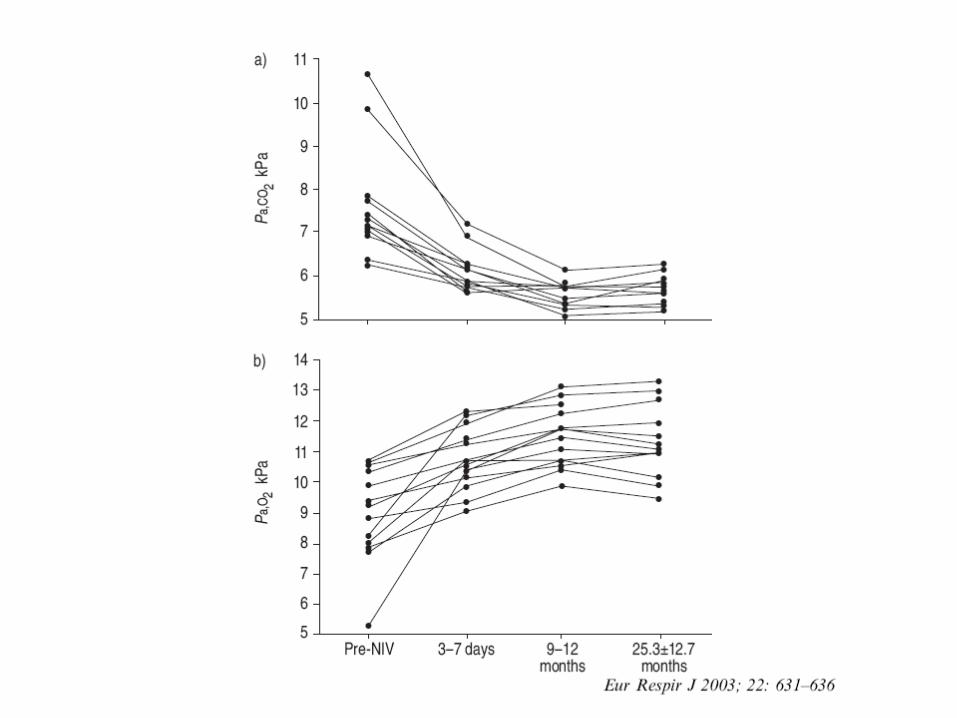




• Questionnaire
• 24 + NIV, 11 no NIV
• Ventilation > 36 mos














Fauroux, ICM 2005
Adverse effects of long term non-invasive ventilation


Retrograde position of maxillar teeth
Figure 5




• Appetite improved in 7 of 12
• Dyspnea disappeared in 8 of 11
• Swallowing improved in 6 of 7

Cough assist/ in-exufflator





INVASIV VENTILATION
WHEN ?

WHEN ?
• NIPPV is insufficient to oxygenate and/or ventilate the ventilator assisted individual (VAI) satisfactorily
• VAI is unable to be weaned
• VAI with no spontaneous respiration
• VAI with (advanced) bulbar insufficiency or other upper airway impairment
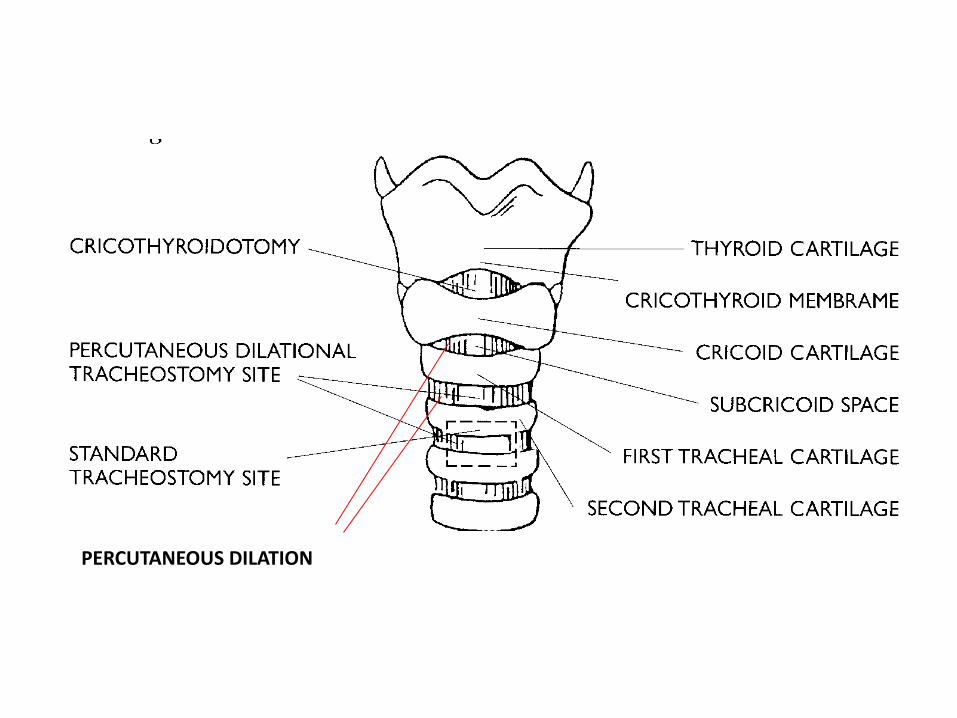
PERCUTANEOUS DILATION

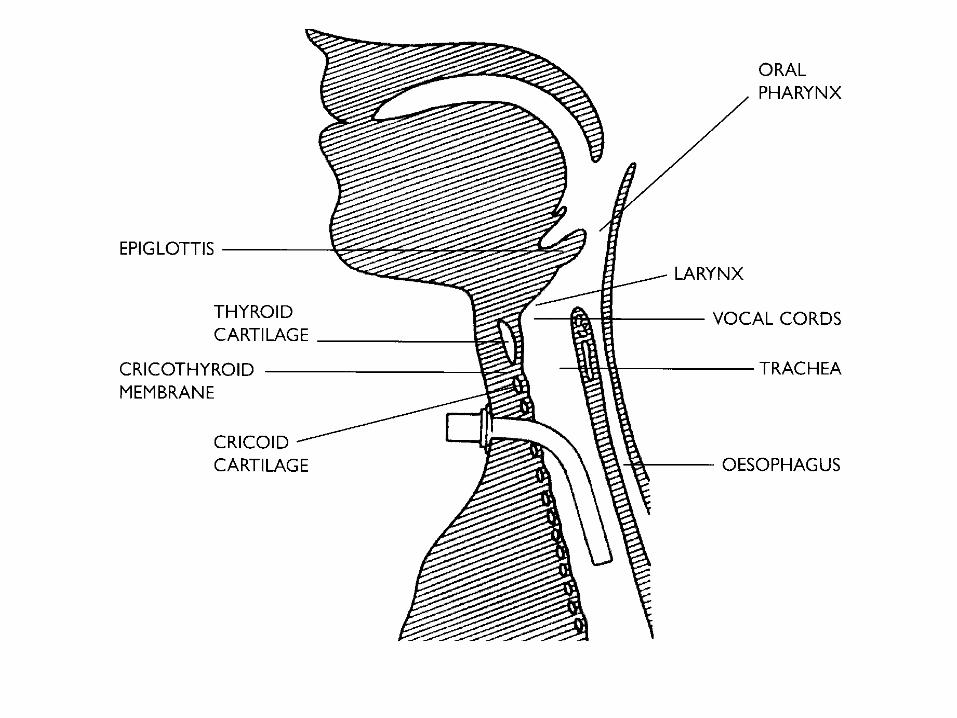
Ventilator – invasive treatment














SUMMARY
• NIV & TIV works in children in the – Acute setting
– Chronic setting
• Perform appropiate diagnosis
• Use appropiate equipment
• Use appropiate ventilator settings
• Adverse effects should be monitored – In particular facial malformation
• Trained staff very important

Referral of children
• signs and/or symptoms of nocturnal hypoventilation (NH) during the night
• daytime symptoms of NH
• failure to thrive

Referral of children
• IVC < 60 % (=> SBD, < 40% => noct hypovent)
• MIP < 4.0 kPa (=> SDB, < 2.5 => noct hypovent)
• CPF < 270 l/min
• Daytime PaCO2 > 45 mmHg (=> noct hypovent)

Mistanke om en evt henvisning til RCV er relevant ?
• Ring
– 78451350/78451340
• Skriv