Embed Size (px)
Citation preview
Respiratory Infections and the Infant
Rees Oliver MDAssistant Professor
Department of PediatricsDivision of NeonatologyUniversity of Alabama at
Birmingham
Disclosure statement:
I do speak as a consultant on behalf of MedImmune for the product Synagis.

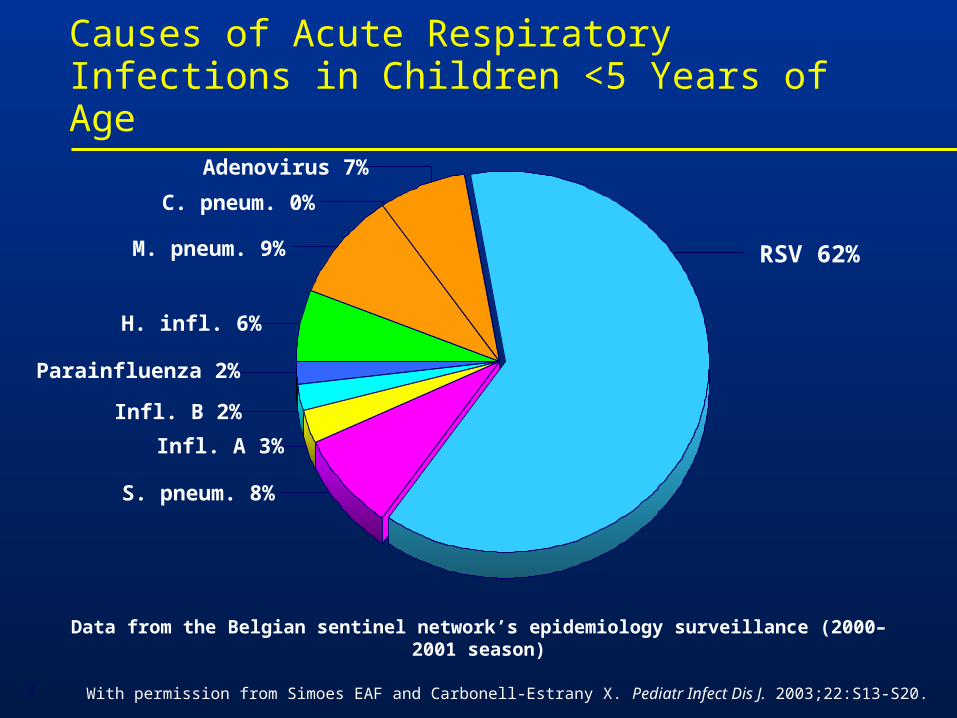
With permission from Simoes EAF and Carbonell-Estrany X. Pediatr Infect Dis J. 2003;22:S13-S20.
Causes of Acute Respiratory Infections in Children <5 Years of Age
Data from the Belgian sentinel network’s epidemiology surveillance (2000–2001 season)
Adenovirus 7%
C. pneum. 0%
M. pneum. 9%
H. infl. 6%
Parainfluenza 2%
Infl. B 2%
Infl. A 3%
S. pneum. 8%
RSV 62%
3
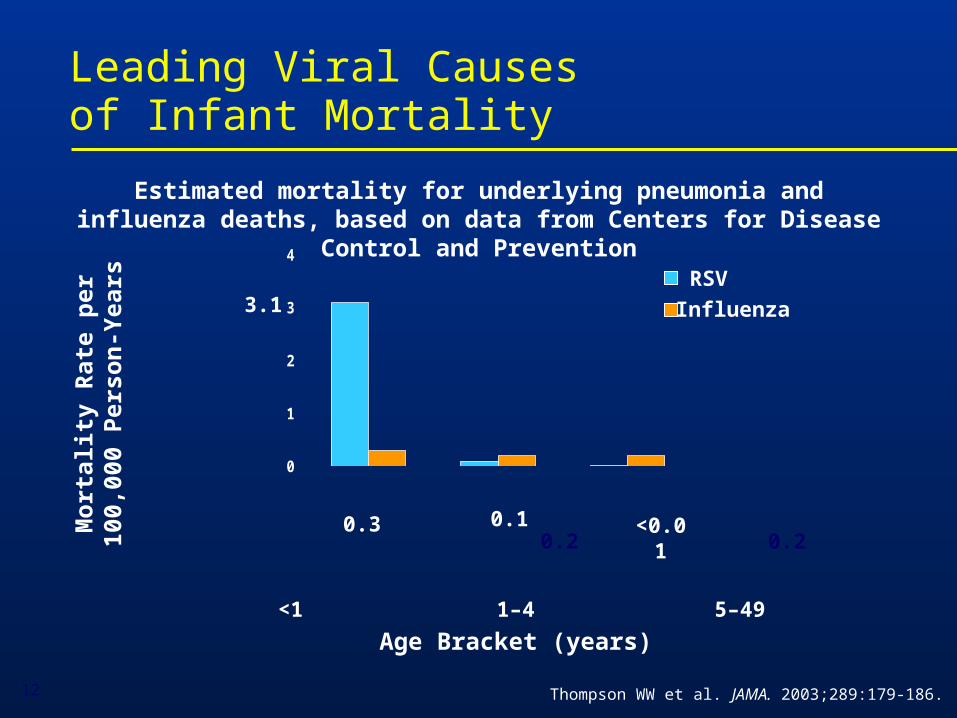
Leading Viral Causesof Infant Mortality
Thompson WW et al. JAMA. 2003;289:179-186.
<1 1–4 5–49
Age Bracket (years)
Mo
rtal
ity
Rat
e p
er10
0,00
0 P
erso
n-Y
ears
RSV
Influenza
0
1
2
3
4
Estimated mortality for underlying pneumonia and influenza deaths, based on data from Centers for Disease Control and Prevention
3.1
0.3 0.10.2 0.2
<0.01
12
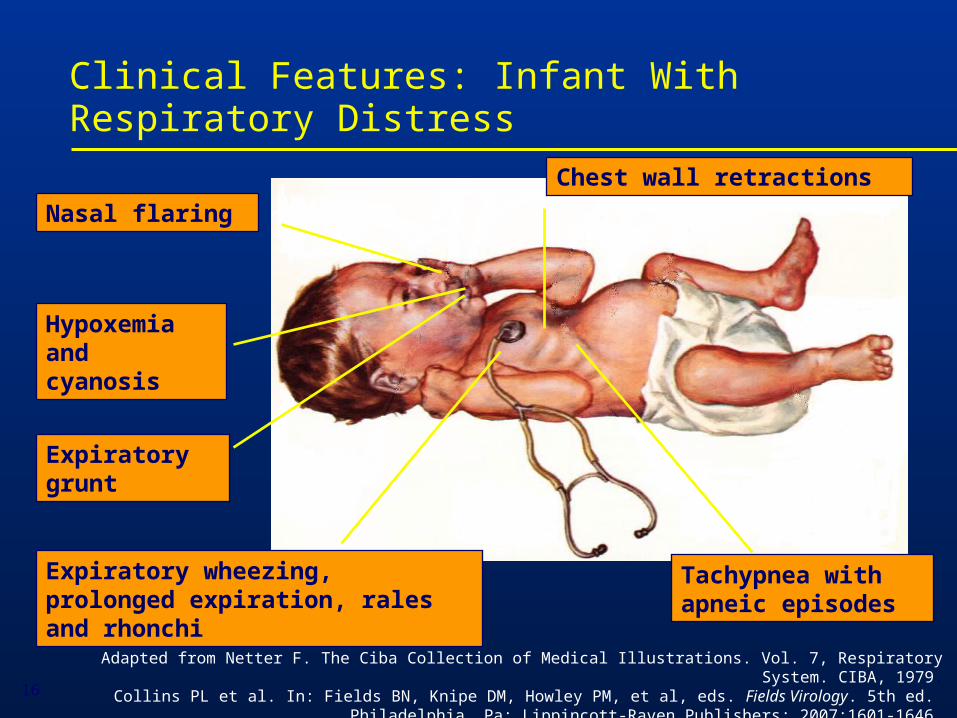
Expiratory wheezing, prolonged expiration, rales and rhonchi
Chest wall retractions
Tachypnea with apneic episodes
Nasal flaring
Hypoxemia and cyanosis
Expiratory grunt
Clinical Features: Infant With Respiratory Distress
Adapted from Netter F. The Ciba Collection of Medical Illustrations. Vol. 7, Respiratory System. CIBA, 1979.Collins PL et al. In: Fields BN, Knipe DM, Howley PM, et al, eds. Fields Virology. 5th ed.
Philadelphia, Pa: Lippincott-Raven Publishers; 2007:1601-1646.16
Signs and Symptoms of Respiratory Distress in Infants
Mild symptoms: moderate tachypnea, rhinorrhea, low-grade fever, and, frequently, otitis media. Recovery occurs after an illness of 7 to 12 days
Severe symptoms: coughing and wheezing followed by dyspnea; severe tachypnea is common; in cases of extreme hypoxemia, respiratory failure occurs
In high-risk infants, respiratory failure severe enough to require airway intubation can occur early in the course of illness
Collins PL et al. In: Fields BN, Knipe DM, Howley PM, et al, eds. Fields Virology. 5th ed. Philadelphia, Pa: Lippincott-Raven Publishers; 2007:1601-1646.
17
Transmission of Viruses
• Viruses can be transmitted by droplets, large particles, and fomites
• Can survive for as long periods of time on nonporous surfaces
• Medical personnel transmit these viruses readily
• Nosocomial infection remains an enormous problem
Blydt-Hansen T, et al. Pediatr Infect Dis J. 1999;18(2):164; Hall CB, et al. J Pediatr. 1980;141:98-102;
Hall CB. Clinical Infectious Diseases; 2000;31:590-6; Cohen B, et al. Pediatric Infectious Disease Journal. 2003;22:494-9
Epidemiology of Viral Processes
• Several of these viruses produce outbreaks each year particularly RSV
• In the case of these outbreaks they can vary in length from region to region, and from season to season and can last for months throughout much of the U.S.
• Year-round epidemics have been reported
Mavunda K, et al. Am J Crit Care Pulm Med. 2000;ATS Abstr # G55:348; Ledbetter JC, et al. Ped ResAPS/SPR/APA. 2002;Abstr #2787; Doraisingham S, Ling ,AE. Ann Acad Med Singapore. 1986;15:9-14
Viral Epidemiology
• During any given season a large portion of the population develops an upper or lower respiratory tract infection (LRTI), Bronchiolitis
• More than half of all children will be infected by their first birthday especially with RSV
• By two years of age essentially all children have been experienced Bronchiolitis
Glezen WP, et al. Am J Dis Child. 1986;140:543-6
Re-infection
• If you look at studies looking at these viruses there are reports that between 6% and 83% of children followed longitudinally have been re-infected each year
• Antibody response is sometimes not sufficient to prevent subsequent re-infection
• Infected lymphocytes and macrophages may suppress secondary immune responses
Feigin RD, Cherry JD, (Eds.). Textbook of Pediatric Infectious Diseases, 4th Ed. 1998. 185.2095; Hall CB, et al. Journal of Infectious Diseases. 163,no.4(1991):693-8;Openshaw, P.J.M. Respiratory Research 3, Suppl 1. (2002):S15
Recent Trends in Hospitalizations
• Up to 126,300 annual hospitalizations among U.S. infants for bronchiolitis or pneumonia may be attributed to RSV alone.
• Bronchiolitis hospitalizations 1980-1996
– 1.65 million hospitalizations
– 7 million inpatient days
– 57% were in children <6 mo
– 81% were in children <1 yo
– 239% increase in bronchiolitis hospitalizations in children less than six months of age
Shay DK, et al. J Infect Dis. 2001;183:16-22; Institute of Medicine. In: New Vaccine Development: Establishing Priorities. Vol I. Wash DC Nat Aca Press 1986: 397-409; Shay DK, et al. JAMA. 1999;282:1440-9
Leader S, Kohlhase K. Pediatr Infect Dis J. 2002;21:629-32
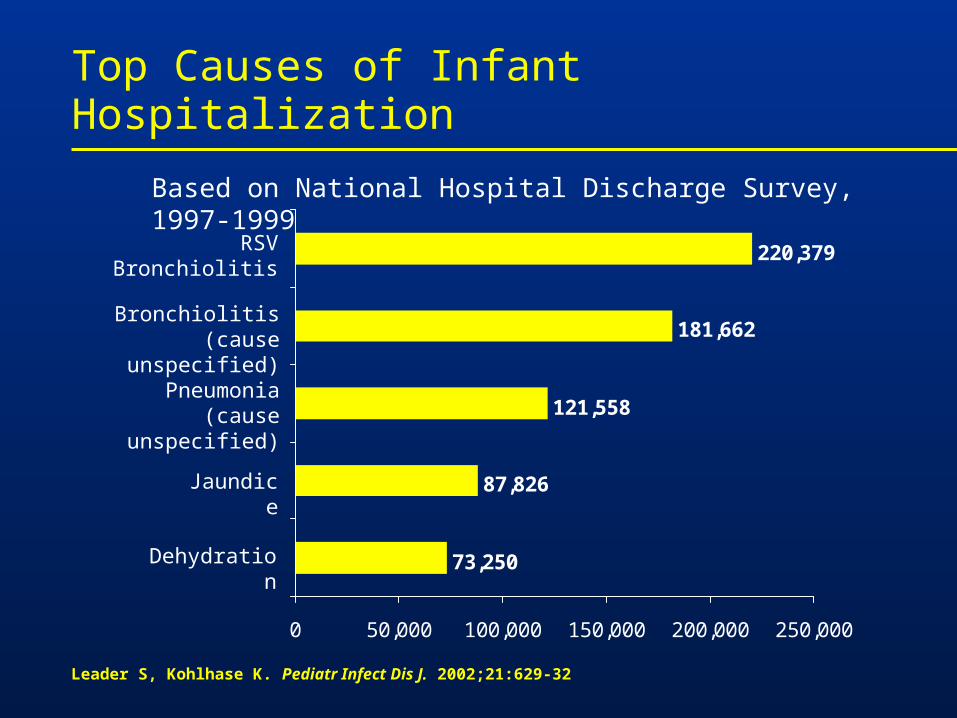
Top Causes of Infant Hospitalization
73,250
87,826
121,558
181,662
220,379
0 50,000 100,000 150,000 200,000 250,000
Dehydration
Jaundice
Pneumonia(cause unspecified)
Bronchiolitis(cause unspecified)
RSV Bronchiolitis
Based on National Hospital Discharge Survey, 1997-1999
• Several prospective studies have shown that even RSV bronchiolitis is associated with recurrent wheezing during subsequent years
• Recurrent wheezing tends to diminish by early adolescence (age 13)
• Conclusion: RSV bronchiolitis appears to be linked to recurrent childhood wheezing through early adolescence
Sigurs N, et al. Am J Crit Care Med. 2000;161:1501-7Taussig LM, et al. Am J Epidemiol. 1989;129:1219-31Stein RT, et al. The Lancet. 1999;354:541-5
Children at Highest Risk for Severe Respiratory Distress as an Infant
Adapted from a presentation by L Weisman, MD: 1st International Congress RSV, 2002
Premature birth
Chronic Lung Disease
Congenital Heart disease
Neuromuscular disease
Immune deficiency
• Altered airway anatomy• Absence of maternal antibody
• Bronchial hyper-responsiveness• Reduced lung capacity
• Pulmonary vascular hyper-responsiveness• Pulmonary hypertension• Increased pulmonary blood flow
• Decreased respiratory muscle strength and endurance
• Decreased host defenses• Impaired capacity to eliminate virus
Problems in Premature Infants
•Respiratory: Airway alteration, respiratory distress/failure, apnea, air leaks, CLD/BPD
•Cardiovascular: Patent ductus arteriosus
•CNS: Intraventricular hemorrhage, periventricular leukomalacia, seizures
•Renal: Electrolyte imbalance, acid-base disturbances, renal failure
•Ophthalmologic: Retinopathy of prematurity, strabismus, myopia
•Gastrointestinal-nutritional: Feeding intolerance, necrotizing enterocolitis, inguinal hernias, failure to thrive
•Immunologic: Poor defense to infection
Boyce TG, et al. J Pediatr. 2000;137:865-70; Law BJ, et al. Paediatr Child Health. 1998;3:402-4; Imaizumi S, Agarwal S, Pereira GR, et al. APS/SPR/APA – 2001 convention 4-28-2001. Abstract
Prematurity: Increased Disease Severity
• Several studies have confirmed the high-risk status of premature infants
• Among premature infants hospitalized with RSV and other viral pathogens:
– 28-34% were admitted to the ICU
– 7-22% required mechanical ventilation
Premature Infants are at High-Risk
Altered lung development
• Altered airway anatomy
• Reduced lung function through early childhood
Immature immune system
• Impaired humoral and cellular immunity
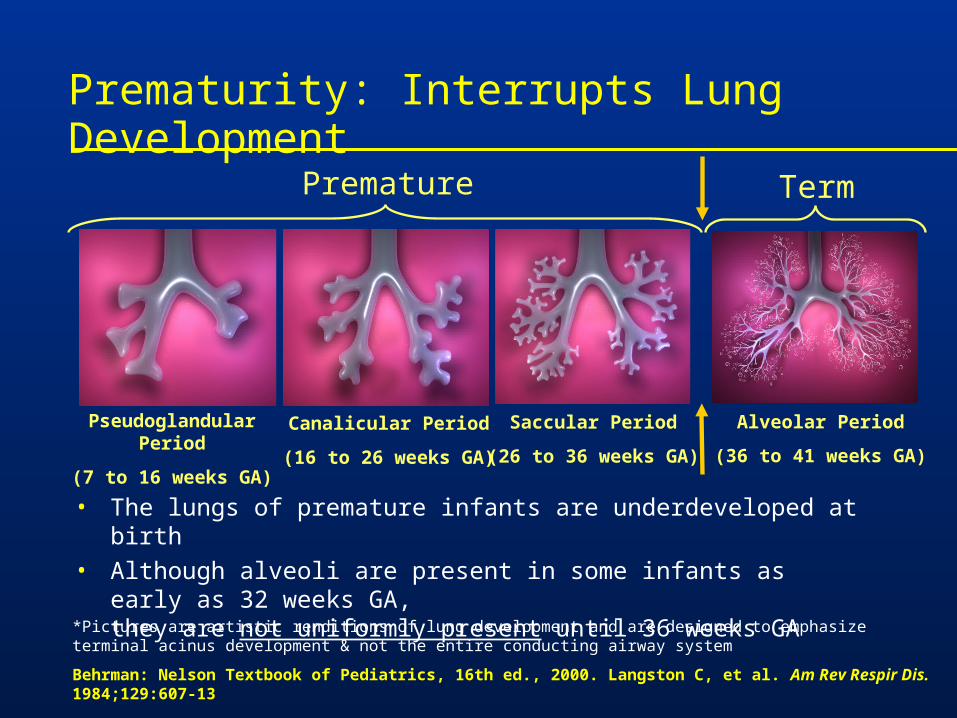
*Pictures are artistic renditions of lung development and are designed to emphasize terminal acinus development & not the entire conducting airway system
Behrman: Nelson Textbook of Pediatrics, 16th ed., 2000. Langston C, et al. Am Rev Respir Dis. 1984;129:607-13
Pseudoglandular Period
(7 to 16 weeks GA)
Canalicular Period
(16 to 26 weeks GA)
Saccular Period
(26 to 36 weeks GA)
Alveolar Period
(36 to 41 weeks GA)
Premature Term
• The lungs of premature infants are underdeveloped at birth
• Although alveoli are present in some infants as early as 32 weeks GA, they are not uniformly present until 36 weeks GA
Prematurity: Interrupts Lung Development
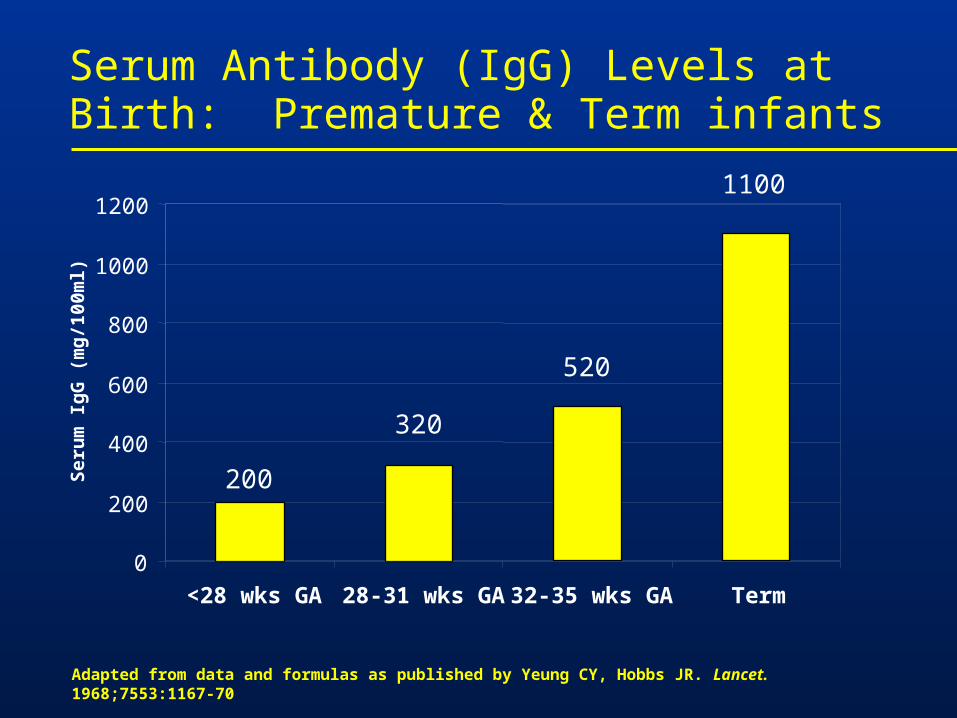
Adapted from data and formulas as published by Yeung CY, Hobbs JR. Lancet. 1968;7553:1167-70
Serum Antibody (IgG) Levels at Birth: Premature & Term infants
200
320
520
1100
0
200
400
600
800
1000
1200
<28 wks GA 28-31 wks GA 32-35 wks GA Term
Ser
um
Ig
G (
mg
/100
ml)
Summary: Risk of Severe Disease in Premature Infants
• Hospitalization rates demonstrate that premature infants up to 36 wks GA are potentially high risk for severe respiratory distress
• Premature infants, even those without a history of ventilation or oxygen use, are high risk due to
– Altered airway anatomy-significant obstruction seen throughout early childhood
– Immature immunity-impaired cellular and humoral immunity
Congenital Heart Disease
• Increased morbidity and mortality. Statistics among children hospitalized:
– 25-33% admission to PICU
– 11-24% mechanical ventilation
– 3.4% fatality rate
• CHD patients with associated pulmonary hypertension are at highest risk for complications.
Navas L, et al. J Pediatr. 1992;121:348-54; Altman CA, et al. Pediatr Cardiol. 2000;21:433-8;Moler FW, et al. Crit Care Med. 1992;20:1406-13; MacDonald NE, et al. N Engl J Med. 1982;307:397-400; Khongphatthanayothin A, et al. Crit Care Med. 1999;27:1974-81
Risk Factors in CHD Patients
• Compromised cardiorespiratory status at baseline
• Altered pulmonary mechanics may contribute to disease severity
• Pulmonary hypertension may exacerbate the adverse effects of respiratory disease
• Inability to properly compensate for intercurrent disease
Navas L, et al. J Pediatr. 1992;121:348-54
Chronic Lung Disease: Increased Risk of Severe Respiratory Distress
• Studies have confirmed the high-risk status of children with Chronic Lung Disease (CLD)
• Among CLD children hospitalized viral processes:
– 32% were admitted to the ICU
– 17% required mechanical ventilation
– 3.5% died within two weeks
Therapeutic Options for Bronchiolitis
• Prevention
– Limit exposure– Avoid daycare
– Excellent hand washing
– Passive immunoprophylaxis:Synagis® (palivizumab)
• Supportive care
• Overcoming airway obstruction and inflammation
Prophylaxis: Reserved for the Highest Risk Children
• RSV immunoprophylaxis is the only available safe and effective method for preventing severe RSV disease
• Prophylaxis is reserved for high risk infants and children
– Premature infants <36 wks GA are at a significantly elevated risk of severe RSV disease
– Children with chronic lung disease, congenital heart disease, immunodeficiencies, and other high-risk conditions
The IMpact-RSV Study Group. Pediatrics. 1998;102(3):531-7; Boyce TG, et.al. J. Pediatr. 2000;137:865-70;Imaizumi S, et al. Abstract # 2311:APS/SPR/APA-2001;Law BJ, et al. CAAC 1998 (abstract #MN-9);Meissner HC, et al. Pediatr Infect Dis J. 1999;18:223
IMpact-RSV Clinical Trial: Study Design
Multicenter, randomized, placebo-controlled trial
Infants 35 weeks gestational age (GA) or with bronchopulmonary dysplasia (BPD) were randomized (N=1502) to receive 5 injections of Synagis® (palivizumab) (15 mg/kg) or equivalent volume of placebo every 30 days
The IMpact-RSV Study Group. Pediatrics. 1998;102:531-537.Please see full prescribing information for Synagis® (palivizumab).
65
IMPACT-RSV TRIAL
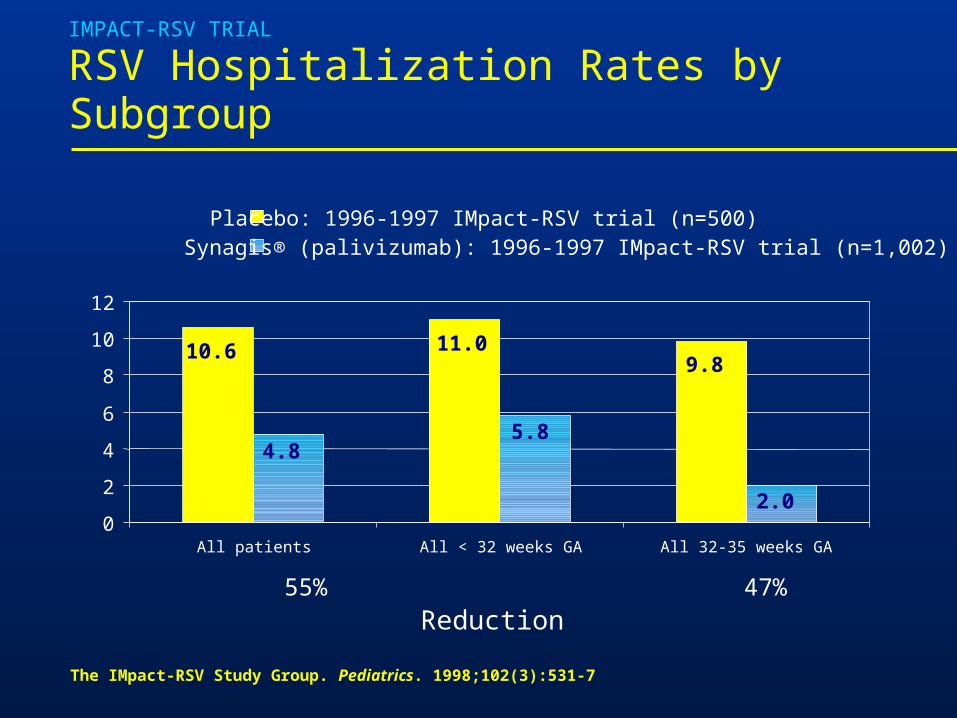
RSV Hospitalization Rates by Subgroup
10.6 11.09.8
4.85.8
2.00
2
4
6
8
10
12
All patients All < 32 weeks GA All 32-35 weeks GA
Placebo: 1996-1997 IMpact-RSV trial (n=500)Synagis® (palivizumab): 1996-1997 IMpact-RSV trial (n=1,002)
55% 47% 80%
Reduction
The IMpact-RSV Study Group. Pediatrics. 1998;102(3):531-7
Summary
• There is significant viral pathogens, some producing annual epidemics and others that are common to our communities
• Bronchiolitis is a major threat to the health of all infants and can lead to hospitalization and death
• The threat of these viruses is greatest in high-risk groups, such as infants born prematurely and children with CLD or CHD
• Treatment options are limited